The GINA report was updated in 2022 following the routine biennial review of the literature by the GINA Science Committee. Full details of the changes can be found in the tracked version archived on the GINA website.
ADULTS, ADOLESCENTS AND CHILDREN 6 YEARS AND OLDER
Definition, description, and diagnosis of asthma
The diagnosis of asthma is based on the history of characteristic symptom patterns and evidence of variable expiratory airflow limitation. Box 1-3 (p.27) describes how to confirm the diagnosis of asthma in a patient who is already being treated with a controller.
Assessment of asthma
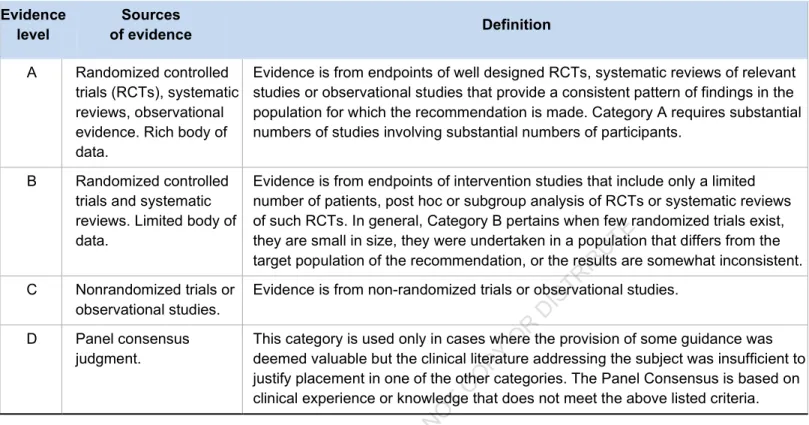
Many studies describe discrepancies between the patient's and the healthcare provider's assessment of the patient's level of asthma control. For clinical trials, describe the patient population according to their level of asthma control and treatment, e.g.
Treating asthma to control symptoms and minimize risk
Relievers were divided into low-dose ICS-formoterol as needed (the preferred reliever, but not if the maintenance controller contains a different ICS-LABA) or SABA as needed. Low-dose ICS-LABA with SABA as needed (Evidence A), OR Medium-dose ICS with SABA as needed (Evidence A), OR.
Medicines containing ICS should be taken daily or, in mild asthma, an alternative is to take a low dose of ICS-formoterol as needed to relieve symptoms. In children aged 6 to 11 years, there have been no studies using the ICS-formoterol only as needed.
Two large double-blind studies in mild asthma showed as-needed budesonide-formoterol was noninferior for severe exacerbations compared with regular ICS.188,189. In two open-label, randomized controlled trials representing how patients with mild asthma would use ICS-formoterol as needed in real life, budesonide-formoterol as needed was superior to maintenance ICS in reducing the risk of exacerbations severe190,191 (Evidence A). In all four studies, the as-needed ICS-formoterol strategy was associated with a significantly lower mean ICS dose than low-dose ICS maintenance.
The greater reduction in severe exacerbations with as-needed ICS formoterol compared with daily ICS among patients previously taking SABA alone; with no significant difference for patients with well-controlled asthma on ICS or LTRA at baseline.190,213. Alternative Step 2 treatment for adults and adolescents: daily low-dose ICS plus as-needed SABA (Track 2) For regular daily low-dose ICS plus as-needed SABA in patients with mild asthma, the burden of symptoms is low, so the most important consideration was to reduce the risk of serious exacerbations. Low-dose ICS taken when SABA is used (in combination or separate inhalers) is another option if the necessary ICS formoterol is not available, and the patient is unlikely to take regular ICS.
No comparison between regular and as-needed ICS-formoterol has been studied in patients eligible for Step 2 treatment.
Another screening option for children is to receive low-dose ICS whenever a SABA is taken, based on the results of two studies with separate ICS and SABA inhalers in patients aged between 5 years and 17 or 18 years.221,223 Interviews with parents showed that those whose children were randomized to as-needed ICS+SABA felt more in control of their child's asthma than those whose children were randomized to physician-based adjustment.223. Another option is daily LTRA, which is generally less effective than ICS.240 The FDA warning for montelukast (above) also applies to its use in children.241 Another option for adults and adolescents is to increase the ICS to the average dose146 (see Box 3-6, p. 63), but at the group level this is less effective than adding a LABA265,266 (Evidence A).
Other less effective options are treatment with low-dose ICS and either LTRA267 (evidence A) or low-dose extended-release theophylline 268 (evidence B). In children, after checking inhaler technique and adherence and treating modifiable risk factors, there are three preferred options at the population level: increase ICS to an intermediate dose (see Box 3-6, p. 63),269 (evidence A) or switch to combination therapy with a low-dose ICS-LABA (evidence A),270 both with a reliever SABA as needed, or switching to maintenance and reliever therapy with a very low-dose ICS-formoterol (evidence B).271 In a large study of children aged 4 up to 11 years, with a history of exacerbation in the previous year, the ICS-LABA combination was noninferior to the same dose of ICS alone in severe exacerbations, with no difference in symptom control or reliever use.272 In children, one study of maintenance versus reliever treatment with very low-dose budesonide -formoterol (100/6 delivered dose, 80/4.5 mcg delivered dose for maintenance and reliever) showed a large reduction in exacerbations compared to the same dose of budesonide-formoterol with a SABA reliever or compared to a higher dose of ICS.271. Individual children's responses vary, so other controller options above should be tried before considering treatment in step 4.273.
In children, there is little evidence for the addition of LTRA to low-dose ICS.267 The FDA warning about montelukast (above) also applies to its use in children.241.
Alternative step 4 treatment for adults and adolescents: medium or high dose ICS-LABA with SABA as needed (track 2). Long-acting muscarinic antagonists (LAMA) may be considered as add-on therapy in a separate inhaler for patients ≥6 years of age (tiotropium), or in a combined ("triple") inhaler for patients ≥18 years of age (beclometasone-formoterol - glycopyrronium; fluticasone furoate- vilanterol umeclidinium; mometasone indacaterol glycopyrronium) if asthma remains persistently uncontrolled despite medium or high dose ICS-LABA. Adding LAMA to a medium or high dose of ICS-LABA modestly improved lung function, evidence A) but with no difference in symptoms.
In some studies, adding LAMA to ICS-LABA modestly reduced exacerbations compared to some moderate or high doses of ICS-LABA. However, for patients who experience exacerbations despite a low dose of ICS-LABA, the ICS dose should be increased to at least medium, or treatment switched to maintenance and reliever therapy with ICS-formoterol, before considering to add a LAMA. For children whose asthma is not adequately controlled on a low maintenance dose of ICS-LABA with SABA as needed, treatment can be increased to a medium dose of ICS-LABA272 (Evidence B).
Other controller options include escalation to high-dose pediatric ICS-LABA (Box 3-6B, p.63), but side effects must be considered.
Adjunctive treatment with bronchial thermoplasty: may be considered for some adult patients with severe asthma199,306 (Evidence B). Patients with suspected or confirmed occupational asthma should be referred for expert assessment and advice if possible. Electronic inhaler monitoring has also been used in clinical practice to identify poor adherence in patients with difficult-to-treat asthma.156,157.
For patients with asthma and For symptoms suggestive of reflux, an empiric trial of antireflux medication, such as a proton pump inhibitor or motility agent, may be considered, as in the general population. Chronic rhinosinusitis is associated with more severe asthma, especially in patients with nasal polyps.493 Diagnosis. For patients with persistent symptoms and/or exacerbations despite high-dose ICS, the clinical or inflammatory phenotype should be evaluated, as this may guide the choice of additional treatment.
Patients with severe asthma often feel alone and misunderstood, as their experience is so different from that of most people with asthma.557. Consider adjunctive type 2 biologic therapy for patients with exacerbations or poor symptom control on high-dose ICS-LABA who have evidence of type 2* inflammation. Results: 305,593 in RCTs in patients with severe asthma with severe exacerbations in the last year anti-TSLP led to 30-70%.
Management of worsening asthma and exacerbations
Patients at increased risk of asthma-related death should be identified and flagged for more frequent review. Patients with severe exacerbations should be advised to contact their doctor immediately or, The written asthma action plan should be reviewed to see if it met the patient's needs.
Where possible, the patient should be given systemic corticosteroids within 1 hour of presentation.650652 The use of systemic corticosteroids is particularly important in the emergency department if:. Sedation should be strictly avoided during asthma exacerbations due to the respiratory depressant effect of anxiolytic and hypnotic drugs. Overall, these risk factors should be considered by clinicians when making admission/discharge decisions for patients with asthma managed in the acute care setting.
In patients with features of COPD, high-dose ICS should be avoided because of the risk of pneumonia.723,724.
CHILDREN 5 YEARS AND YOUNGER
Diagnosis and management of asthma in children 5 years and younger
Many young children wheeze with viral infections and it can be difficult to decide when a child should receive controller treatment. The frequency and severity of wheezing episodes and the temporal pattern of symptoms (only with viral colds or also in response to other triggers) should be taken into account. Response should be evaluated by symptom control (day and night), and the frequency of wheezing episodes and exacerbations.
Episodes of wheezing in young children should be treated first with inhaled short-acting beta2 agonists (SABAs), regardless of whether a diagnosis of asthma has been made. In young children, as in older patients, symptom control and future risk should be monitored (Evidence D). Asthma action plans should be provided for families/caregivers of all children with asthma, including those aged 5 and under (Exhibit D).
The child should be monitored closely and the dose should be adjusted according to clinical improvement and side effects.
Primary prevention of asthma
Several environmental factors, both biological and sociological, may be important in the development of asthma. Evidence supporting a role for environmental risk factors in the development of asthma includes a focus on: diet, allergens (both inhaled and ingested), pollutants (particularly environmental tobacco smoke), microbes, and psychosocial factors. FACTORS ASSOCIATED WITH INCREASED OR REDUCED RISK OF ASTHMA IN CHILDREN Maternal and infant nutrition.
Although the risk of parent-reported asthma with infrequent wheezing was reduced after 6 years, there was no impact on physician-diagnosed asthma or lung function.847 The long-term effect of palivizumab on asthma prevention thus remains uncertain. The social environment that children are exposed to can also contribute to the development and severity of asthma. Maternal stress during pregnancy852 or during the first years of the child's life853 has been associated with an increased risk of developing asthma in the child.
Identification and correction of vitamin D insufficiency in women with asthma who are pregnant or planning pregnancy may reduce the risk of wheezing episodes early in life.
TRANSLATION INTO CLINICAL PRACTICE
Implementing asthma management strategies into health systems
