If weight loss of 5-10% is not achieved within 6 months, the next step is the same basic treatment combined with medication. Keeping records has been shown to be one of the most successful behavioral techniques for weight loss and maintenance. A change in treatment regimen should be considered if weight loss is less than 5% in the first 6 months.
While short-term weight loss depends on calorie restriction, maintenance of weight loss largely depends on the level of physical activity. Some studies have shown that intentional weight loss reduces mortality, while unintentional weight loss is associated with an increased risk of mortality. Weight loss with adjustable gastric bands is associated with an incidence of gallstones no different from that of the normal population.
In addition, smoking, weight change (weight gain and loss can be more harmful than stable weight), and unintentional weight loss can confound health risk assessment. A combination of a moderate energy-deficit diet, increased physical activity, and behavioral modification leads to moderate weight loss of 0.4–0.9 kg/week or 8–10%. This weight loss is associated with an improvement in obesity-related comorbidities and an overall reduction in medication requirements.
Weight loss in the elderly can therefore exacerbate age-related loss of muscle mass and further impair physical function.
Stakeholders and management options
The SCAMOP (Screening and Counseling for Physical Activity and Mobility in the Elderly) study included 619 patients aged 75–83 years with a BMI between 20 and 53 kg/m2. A meta-analysis of 43 studies in older adults rejected the hypothesis that interventions to increase physical activity do not affect activity in older adults. Several modulating factors have been identified that can be used to increase physical activity in the elderly.
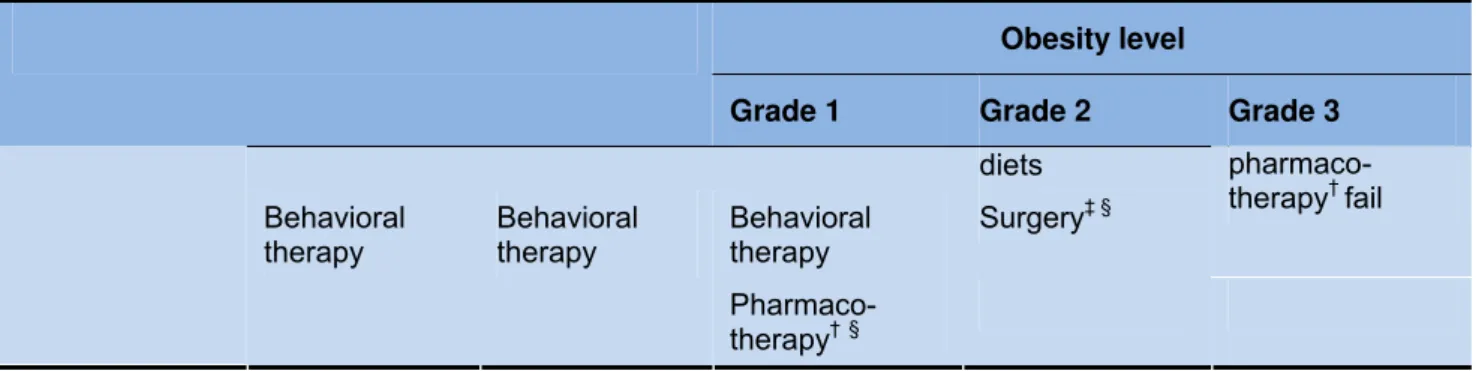
Only physical activity should be targeted and should not be accompanied by health education. Only in patients with obesity-related diseases who are unable to achieve adequate weight loss with available conventional lifestyle modifications and have no absolute contraindications to drug therapy. Only in patients with obesity-related diseases who are unable to lose weight with available conventional therapy and have no absolute contraindications to surgery.
Although there is no evidence for surgery in patients with BMI 30-35 and no complications, exceptions are possible when there is significant comorbidity. There is evidence for surgery in patients with BMI 35-40 and comorbidities; according to experts, the cut-off is likely to be lowered to 30 over the next few years.
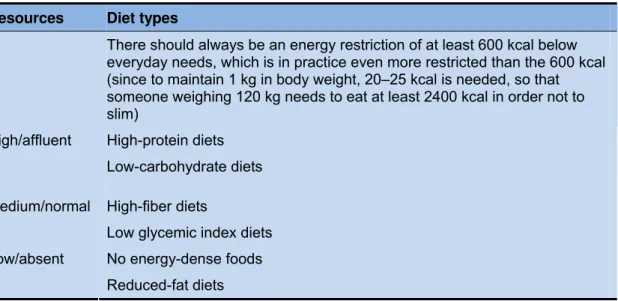
Management options relative to available resources
There should always be an energy restriction of at least 600 kcal below daily needs, which in practice is even more limited than the 600 kcal (since to maintain 1 kg of body weight, 20-25 kcal are needed, so someone who weighs 120 kg must eat at least 2400 kcal in order not to lose weight). Of course, it is difficult to first emphasize energy restriction or reduction before discussing in detail the changes in macronutrients and dietary composition.
Obesity
- Nutrition and diet
- Pharmacotherapy
- Lifestyle changes
- Surgery
Lowering the glycemic load of the diet can be an effective method of losing weight. In randomized trials, substituting protein for carbohydrates in calorie-restricted diets has been found to lead to more weight loss. Nevertheless, weight loss medications can help patients adhere to lifestyle advice, and can lead to clinically significant and meaningful improvement in symptoms, risk factors, and quality of life.
Combination with lifestyle modification resulted in more weight loss at 12 months (combination: 12.1 kg; sibutramine alone 5.0 kg; lifestyle intervention alone 6.7 kg). Patients who had the greatest initial weight loss and were most physically active were most likely to successfully maintain the weight loss. In patients with essential hypertension, treatment with a weight loss diet or orlistat treatment reduced body weight and blood pressure.
The drug is a triacylglycerol lipase inhibitor and causes a 30% reduction in dietary fat absorption in the intestinal lumen. It is available over the counter in lower doses in the United States (60 mg, three times a day). It has been shown to result in about 2% more weight loss compared to placebo over a period of 4-24 months.
In the United States, Roux-en-Y gastric bypass (open or laparoscopic) is the most commonly used operation. Combined procedures are sometimes performed as staged operations, with a restriction followed by a Roux-en-Y procedure after initial weight loss has facilitated surgery and reduced operative risk. Recent research on LAGB with the Swedish Adjustable Gastric Band (SAGB) shows that it is effective in achieving a mean sustained weight loss of > 50% at 8 years postoperatively with an acceptably low morbidity rate.
In obese people, bariatric surgery can be risky, but the risk of not losing weight may well be greater than the risks of the surgery. A 2005 Cochrane Review suggests a typical weight loss of 20–50 kg lb) with various bariatric procedures compared with modest weight gain in medically treated patients. In general, weight loss with malabsorptive procedures tends to be greater than weight loss with purely restrictive procedures.
There appears to be little additional benefit of the intragastric balloon in relation to weight loss. However, recent research has shown that abdominal liposuction does not significantly improve the metabolic abnormalities associated with obesity and that reduction of adipose tissue mass alone does not achieve the metabolic benefits of weight loss.
Obesity and the Elderly
Aging is associated with marked changes in body composition and metabolism (Villareal et al. 2005, Zamboni et al. 2005, Kennedy et al. 2004). Changes in the gonadal axis and other hormones that occur with normal aging appear to be exaggerated in the presence of abdominal obesity and insulin resistance (Kennedy et al. 2004). Waist circumference, which is highly correlated with total fat and intra-abdominal fat, could be a better parameter for predicting the adverse health effects of obesity in the elderly (Han et al. 2011).
Many confounding factors also contribute to an underestimation of the health risks of obesity in the elderly (Zamboni et al. 2005). The underlying disease (reverse cause), physical activity and cardiorespiratory fitness (a lean unfit person may have a higher mortality than an obese fit person and the obese unfit person a higher mortality than the lean fit), fat distribution (unknown in many studies) and height of the follow-up (since there is no association between obesity and mortality with a shorter duration) also plays a role (Zamboni et al. 2005). Both high fitness and high BMI independently reduced mortality in the US Veterans study (McAuley et al. 2010, Ades & Savage 2010).
Sarcopenic obesity is a unique weight status in the elderly: a combination of an unhealthy excess of body fat with a detrimental loss of muscle and lean mass, including bone (Zamboni et al. The focus of treatment should be on a reduction of intra-abdominal fat while maintaining muscle mass and strength (Kennedy et al. 2004). The mean age of subjects ranged from 34 to 54 years in a meta-analysis of pharmacotherapy (Li et al. 2005).
Moreover, orlistat has a weight loss independent beneficial effect on dyslipidaemia (Hollander et al. 1998, Muls et al. 2001). One study had a slightly but significantly higher mortality with no difference in postoperative morbidity (Sosa et al. 2004). The addition of leucine to a mixed nutrient meal in older subjects resulted in a 56% increase in muscle protein synthesis (Rieu et al. 2006).
It completely prevented the loss of upper extremity lean mass and partially prevented the loss of lower extremity lean mass (Frimel et al. 2008). Improvements in endurance, muscle strength, plasma triglycerides and LDL cholesterol and diastolic blood pressure occurred with the diet plus exercise, but not in the diet alone group (Shah et al. 2009). Lifestyle intervention improved pancreatic β-cell and α-cell function, increased insulin clearance and doubled insulin sensitivity (Villareal et al. 2008).
The only negative effect consisted of an increase in bone turnover and a 2-3% decrease in thigh bone mass after 1 year (Villareal et al. 2008). Eight years later, they re-analyzed their data and obtained the death certificates of the deceased participants (Shea et al. 2010).