The results of the qualitative reviews were assessed using the GRADE confidence in the evidence from reviews of qualitative research (GRADE-CERQual)7 approach. Low-quality evidence indicates that confidence in the effect estimate is limited and the true effect may be substantially different from the estimate of the effect.
Immediate support to initiate and establish breastfeeding
This included the following considerations: (i) the quality of evidence on outcomes relevant to decision-making; (ii) balance of benefits and harms; (iii) values and preferences regarding the recommended intervention in different settings and for different stakeholders, including at-risk populations; (iv) acceptability of the intervention among key stakeholders; (v) resource implications for program managers; (vi) equity; and (vii) the feasibility of implementing the intervention.
Feeding practices and additional needs of infants
Creating an enabling environment
This guideline examines each of the practices in the Ten Steps to Successful Breastfeeding to gather evidence and considerations to inform practice. The scope of the guideline is limited to specific practices that can be implemented in facilities offering maternity and newborn services to protect, promote and support breastfeeding.
Immediate support to initiate and establish breastfeeding
This guideline applies to women who give birth in hospitals, 1 maternity wards 2 or other establishments providing maternity and newborn services, and their babies. Babies born at home or in the community and babies with medical reasons not to breastfeed temporarily or permanently (37) are not taken into account in this guideline.
Feeding practices and additional needs of infants
Should hospitals and facilities providing maternity and neonatal care (P) have a written breastfeeding policy that is routinely communicated to staff (I), compared to institutions without a written breastfeeding policy (C), to increase rates of early breastfeeding initiations ( O). Should mothers giving birth in hospitals or facilities providing maternity and newborn care (P) be provided with a link to continued breastfeeding support after discharge from the institution (I), rather than not providing a link to continued breastfeeding support after discharge (C ), in order to increase rates of exclusive breastfeeding after 1 month (O).
Infant outcomes
Maternal outcomes
Facilities providing maternity and newborn services and staff outcomes
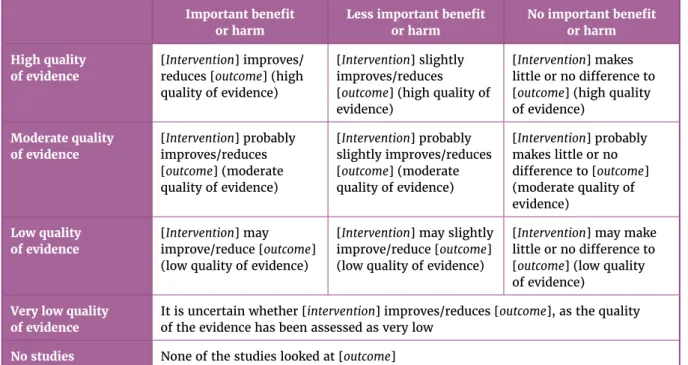
In presenting the summary of evidence from systematic reviews for each of the interventions, standardized statements of effects were used for different combinations of the magnitude of the effect and the quality of evidence (assessed using the Grading of Recommendations Assessment, Development and Evaluation [GRADE] ( 38)). It is uncertain whether [intervention] improves/reduces [outcome], as the quality of the evidence was rated as very low.
Immediate support to initiate and establish breastfeeding
The comparative intervention is that mothers and infants are housed separately for all or part of the time, and the primary place of care for the infant is the facility nursery during the hospital stay. Demand, responsive or baby-led feeding places no restrictions on the frequency or length of the babies' feeds, or the use of one or both breasts at a feed, and mothers are advised to breastfeed when the baby shows signs of hunger , or as often as the baby wants.
Feeding practices and additional needs of infants
Demand feeding (or responsive feeding or baby feeding) involves recognizing and responding to the infant's display of hunger and food cues and readiness to eat, as part of a nurturing relationship between mother and infant. Prenatal breastfeeding education differs from breastfeeding support in that breastfeeding support is given postnatally to the individual mother according to her needs.
Feasibility
The information on these two issues was common to all interventions and is presented below.
Equity and human rights
A search of the published literature was conducted to inform feasibility and equity and human rights issues. A search of the published literature was conducted to inform the resource implications, feasibility and equity and human rights issues of each of the interventions.
Early skin-to-skin contact
The overall quality of evidence for early skin-to-skin contact on the critical outcomes is moderate. Several problems with resource implications for the early skin-to-skin contact have been identified. i) the time with mothers; (ii) staff capacity;.
Early initiation of breastfeeding
Early and uninterrupted skin-to-skin contact between mothers and babies should be facilitated and encouraged as soon as possible after birth (recommended, moderate-quality evidence).
Showing mothers how to breastfeed
They also found that learning how to express breast milk (hand expression or mechanical pumping) was helpful and allowed them to have someone else feed the baby when they were unable (low confidence in the evidence). No studies were found specifically on the acceptability among health workers to show mothers how to express breast milk.
Rooming-in
Issues identified with resource implications for teaching mothers how to breastfeed and express breast milk include staff time, staff capacity, staff knowledge and training, and cost of optional equipment (eg, manual or electronic pumps) (62 -66). Mothers should be counseled on how to express breast milk as a means of maintaining breastfeeding in the event that they are temporarily separated from their infants (recommended, very low quality evidence).
Demand feeding
The review of the literature on the acceptability of on-demand feeding among healthcare professionals identified seven studies conducted in six countries (Australia, Canada, China, India, Ireland and the United States). Some healthcare professionals were uncomfortable with the promotion of on-demand feeding (particularly against the continued practice of more experienced staff to plan feedings), while others saw on-demand feeding as standard care, except in specialized units such as the neonatal intensive care unit where strict documentation of nutrition is required (low confidence in evidence) (see Appendix 5).
Rationale for immediate support to initiate and establish breastfeeding
All mothers should be supported to start breastfeeding as soon as possible after birth, after birth (recommended, high quality evidence). Mothers should receive practical support to enable them to initiate and establish breastfeeding and to manage common breastfeeding difficulties (moderate-quality recommended evidence).
Remarks
Mothers should be supported to implement responsive feeding as part of care (recommended, very low quality evidence). Mothers of infants admitted to the NICU should be carefully supported to allow skin-to-skin contact with their infants, recognize their infants' behavioral cues, and express breast milk effectively soon after birth.
Early additional foods or fluids
Details of the systematic reviews can be found in Appendix 2 and summary tables of findings can be found in Appendix 3. Potential resource implications of not providing early complementary foods or fluids include continued implementation of the International Code of Marketing of Breast-Substitutes milk (26) adopted by the 34th session of the WHA.
Avoidance of pacifiers or dummies
The PICO question and critical outcomes can be found in Appendix 1. The details of the systematic reviews can be found in Annex 2. The summary of findings tables can be found in Appendix 3. Balance of benefits and harms. The review of literature on the values and preferences of mothers towards pacifier use identified five studies conducted in five countries (Australia, Brazil, Egypt, New Zealand and Sweden).
Avoidance of feeding bottles and teats
The review of literature on the values and preferences of mothers regarding the avoidance of feeding bottles and teats identified three studies conducted in three countries (Australia, Sweden and the United Kingdom). The review of literature on the acceptability of avoiding feeding bottles and teats among healthcare professionals identified 10 studies conducted in 5 countries (Canada, Germany, India, the United Kingdom and the United States).
Rationale for feeding practices and additional needs of infants
Breastfeeding policy at facilities providing maternity and newborn
Training of health workers
Antenatal breastfeeding education for mothers
Some studies have shown that healthcare professionals are uncertain about addressing the issue of bottle feeding. While some studies reported that health professionals felt confident in counseling women about breastfeeding and breastfeeding problems, others reported that health professionals felt insecure and ineffective in their counseling.
Discharge planning and linkage to continuing support
Studies cited that health workers describe gaps and lack of communication between health care providers in the continuum of care after women leave hospital (moderate confidence in the evidence) (see Annex 5). As part of the protection, promotion and support of breastfeeding, discharge from facilities providing maternity and newborn services should be planned and coordinated so that parents and their babies have access to ongoing support and appropriate care (recommended, low-quality evidence).
Rationale for creating an enabling environment
Regional advisors from WHO regions also participated in the guideline development group meetings. The list of members of the guideline development group and their areas of expertise is presented in Annex 7.
Quality of evidence
A recommendation that is "recommended" is one for which the guideline development group is convinced that the desirable consequences clearly outweigh the undesirable consequences. A recommendation that is "recommended only in specific contexts" is one in which the balance between the benefits and harms of implementing the recommendation may be different for certain situations.
Balance of benefits and harms
The draft recommendations were discussed by the steering group, in consultation with the guideline development group, in a meeting held on 7–11 November 2016 in Florence, Italy. The following domains were prepared by the steering group and discussed during the guideline development group meeting for each of the key PICO questions.
Values and preferences
The recommendations in this category will specify the contexts in which these recommendations can be used. A systematic review and GRADE evidence profiles for each of the critical outcomes were used to develop the recommendations.
Acceptability
The implication for policymakers is that the recommendation can be adopted as a policy, quality standard or performance indicator in most situations.
Resource implications
Question in population,
- Immediate support to initiate and establish breastfeeding
- Feeding practices and additional needs of infants
- Creating an enabling environment
Duration of exclusive breastfeeding (in months) Neonatal, infant or child mortality (all causes) Initiation of lactation. Duration of exclusive breastfeeding (in months) Duration of any breastfeeding (in months) Neonatal, infant or child deaths (all causes).
Breastfeeding policy of facilities providing maternity and newborn services
Should health facility staff (P) be trained on breastfeeding and supportive feeding practices (I), compared to not trained (C), in order to increase the rate of early initiation of breastfeeding (O). Quality of skills of health facility staff in improving practices of mothers in optimal infant feeding Attitudes about infant feeding.
Antenatal breastfeeding education for mothers
Discharge planning and linkage to continuing support
Systematic review details
The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). Guideline: protection, promotion and support of breastfeeding in settings providing maternity and newborn services *Risk in the intervention group (and 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and 95 %CI).
WHO steering group
WHO guideline development group
External resource persons
Systematic reviews and authors
Cochrane Pregnancy and Childbirth Group
St Luke’s International University in Tokyo (Cochrane Pregnancy and
Cochrane Neonatal Review Group
Independent reviewers
Peer-reviewers
Note: The names and affiliations of peer reviewers are provided here as an acknowledgment and in no way indicate that they endorse the recommendations in this guideline. The recognition of the peer reviewers does not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
WHO Secretariat
WHO regional and country offices