Tese, requisito parcial para obtenção do título de Doutor, apresentada no Programa de Pós-Graduação em Ciências Médicas da Universidade do Estado do Rio de Janeiro. Análise da sobrevida e fatores de risco para óbito em pacientes adultos com bronquiectasias não fibrose cística acompanhados em clínica especializada. Tese (Doutorado em Ciências Médicas) - Faculdade de Ciências Médicas, Universidade do Estado do Rio de Janeiro, Rio de Janeiro, 2022.
Analysis of survival and risk factors for death in adult patients with noncystic fibrosis bronchiectasis followed up in a specialized outpatient clinic. To assess quality of life (QoL) and identify risk factors associated with mortality in patients with non-cystic fibrosis bronchiectasis (NCFB), the present thesis conducted a single-center, cohort study comprising 120 patients with NCFB followed regularly from January 2017 to June 2020. As conclusions, patients have with NCFB reduced quality of life, and several factors can contribute unfavorably to the clinical development, some of which can be identified early and treated preventively.
Termo de Consentimento Livre e Esclarecido por Tomografia Computadorizada de Alta Resolução Fator de Necrose Tumoral (Fator de Necrose Tumoral) Universidade do Estado do Rio de Janeiro. APÊNDICE H - Artigo na Publicação 1: Acompanhamento de 1 ano de uma coorte de pacientes com bronquiectasia sem fibrose cística…….
Publicação artigo 2: Mortality and comorbidities in patients with bronchiectasis over a 3-year follow-up
Nesta tese será apresentada a evolução da sobrevida de um grupo de pacientes com bronquiectasias que realizam acompanhamento ambulatorial em uma instituição terciária durante 3 anos. A ausência de patógenos em amostras de escarro de pacientes com bronquiectasias é um indicador de doença mais leve32. Um estudo aponta que um dos principais patógenos responsáveis pela colonização de pacientes com bronquiectasias foi o P.
A hemoptise em pacientes com bronquiectasias é intermitente e geralmente ocorre em pequenas quantidades (estrias de sangue) em 26% a 51% dos casos, mas às vezes pode ser relevante (hemoptise maciça)82, 97 e requer atenção médica imediata. A exacerbação ocorre frequentemente em pacientes com bronquiectasias e está associada ao rápido declínio da função pulmonar13, pior QV99, aumento da mortalidade22, 20. Onen et al101 descobriram que a vacinação contra influenza e pneumococos se correlaciona com melhor sobrevida em pacientes com bronquiectasias.
O manejo convencional de pacientes com bronquiectasias é baseado em critérios utilizados em indivíduos com FC e DPOC67. Os principais recursos para o tratamento de pacientes com bronquiectasias estão publicados em diretrizes internacionais29 e recentemente em consenso nacional45. Os principais componentes do instrumento que ficaram comprometidos em pacientes com bronquiectasias foram dor/desconforto e ansiedade/depressão16.
Alzeer e cols.108 relataram taxa de mortalidade de 34% em pacientes com bronquiectasias internados com insuficiência respiratória em unidade de terapia intensiva (UTI).
Follow-up of a cohort of patients with noncystic fibrosis bronchiectasis for 1 year
Non-cystic fibrosis bronchiectasis (NCFB) is an irreversible disease characterized by bronchial dilatation1,2 resulting from the destruction of the elastic and muscular components of its walls3. Bronchiectasis is a disease characterized by high morbidity and mortality12,13, so studies are needed to better understand the development of the disease and improve patient care. The Research Ethics Committee of the Pedro Ernesto University Hospital in Brazil approved the study (No.
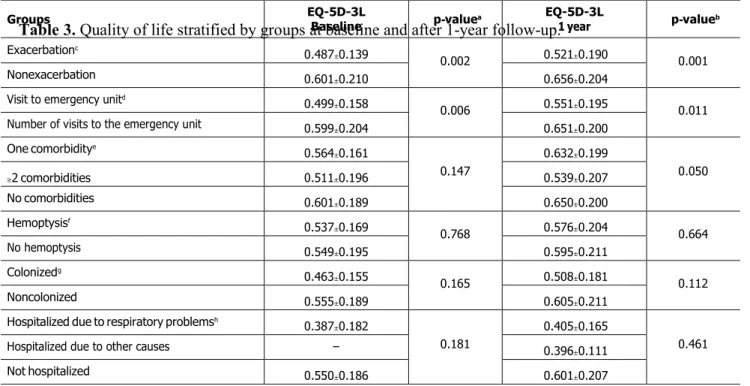
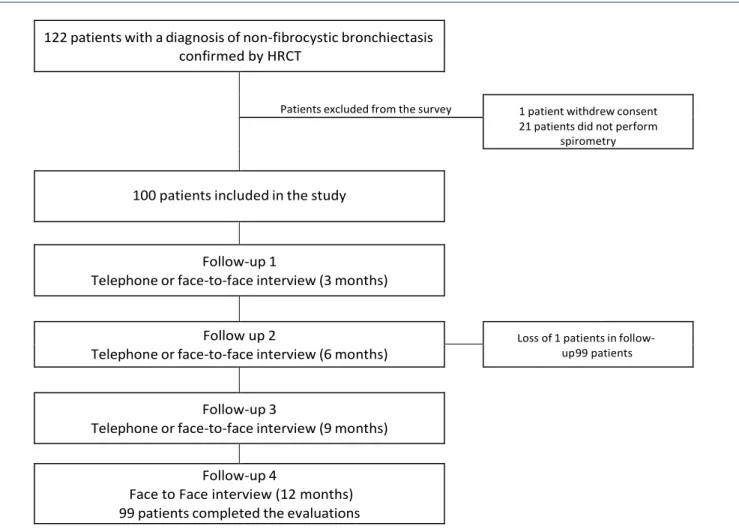
The quality of life questionnaire is an instrument consisting of the EQ-5D-3L questionnaire and the Visual Analogue Scale (VAS)11. The survey was registered on the website of the EuroQol Research Foundation and an authorization to apply the self-completed version of the EQ-5D-3L questionnaire and the face-to-face version of the EQ-5D-3L to reading or writing patients. difficulties were met. Of the 122 patients recruited, 1 patient withdrew the consent form, 21 were excluded because they did not meet all eligibility criteria, and 1 patient was lost to follow-up.
Etiological dominance was associated with the consequences of pulmonary tuberculosis in 53% of cases. The results show that these variables contribute to the deterioration of the quality of life of these individuals. Currently, despite technological advances and guideline development, there are still difficulties and a lack of consensus in some approaches related to bronchiectasis.
Of the admitted patients, 65% had hemoptysis due to active pulmonary tuberculosis or its sequelae, and 9.3% of cases were due to bronchiectasis. In this study, 17 of 31 patients who reported small amounts of hemoptysis (<100 ml/24 hours) or blood streaks had previous pulmonary tuberculosis. We identified 79 patients with comorbidities concurrent with bronchiectasis, with half of the subjects presenting with multiple comorbidities.
The recent consensus stated that cardiovascular disorders, COPD, diabetes, gastroesophageal reflux disease (GERD), psychological diseases and pulmonary hypertension are more likely to coexist with bronchiectasis and that such comorbidities contribute to morbidity and mortality, and worsening of the quality of life 25. Another limitation of the study was the recruitment of volunteers from a single center specialized in bronchiectasis, representing a subgroup of patients who regularly attended medical appointments. However, one of the strengths of the article was its prospective design, with careful monitoring and determination that quality of life should be incorporated as one of the indicators of therapeutic management.
Mortality and comorbidities in patients with bronchiectasis over a 3-year follow- up
Introduction
Therefore, this study aimed to identify risk factors for mortality in patients with NCFB during outpatient follow-up at a tertiary institution.
Methods
The Mann-Whitney U test was used to compare basic demographic and clinical data for continuous numerical variables, and Chi-square tests were used for categorical nominal variables to evaluate frequency independence between these variables and death. To estimate the risk of progression to death, person-years (pY) at risk were calculated based on the number of follow-up years with bronchiectasis for each patient. The effects of various risk factors on death were assessed using adjusted hazard ratios and their associated 95% confidence intervals, which were estimated using Cox proportional hazards multiple regression models.
In addition to disease types, all clinical or phenotypic characteristics at least suggestively associated with outcome were introduced as confounders ( P ≤ 0.1) to eliminate any potential bias introduced by convenience sampling. Whenever necessary, continuous numerical variables were categorized using the round integer closest to either the median or percentiles of 0.33 and 0.66, respectively. In addition, the prevalence rates and 95% confidence interval of patients with bronchiectasis were estimated according to asymptotic standard errors calculated from the gamma distribution.
RESULTS
Both groups had a higher incidence of bronchiectasis related to pulmonary tuberculosis (38.5% in GS and 56.1% in GD). All (100%) patients in the GD group and patients in the GS group were diagnosed with lung involvement in 2 or more lobes by chest HRCT, with no significant difference between the 2 groups. The most common disease in the GD group was systemic arterial hypertension in 61.5% of patients, followed by chronic obstructive pulmonary disease (COPD) (38.5%) and diabetes mellitus (30.8%).
Four (30.8%) patients visited the emergency clinic at least once in the past year due to deterioration. In addition, 32.7% of patients in the GS group showed no discharge, 25.2% had mucoid discharge, 35.8% had purulent discharge, and 6.5% had mucopurulent sputum. In addition, more than half of the patients in both groups were vaccinated against influenza (GS, 81.3%;.
Less than 8% of the study population was enrolled in a routine respiratory physiotherapy program (GS, 7.5%; GD, 7.7%). Comparison of spirometry results between the two groups showed statistically significant differences in forced expiratory volume in 1 second (FEV1) (P = 0.023), forced vital capacity (FVC) (P = 0.025) and FEV1/FVC ratio (P = 0.024). Analyzed using the Mann-Whitney U test for continuous variables and the chi-square test for categorical variables.
According to the International Classification of Diseases, the causes of death during the study period were acute myocardial infarction, cerebrovascular disease, liver fibrosis and cirrhosis, gastrointestinal bleeding, septicemia, human immunodeficiency virus disease, COPD, and laryngeal and breast cancer. Variables significantly associated with an increased risk of death were female gender, active smoker, diabetes, COPD, emergency room visits, use of oral antibiotics due to exacerbation, secretion color change, exacerbation, FEV1, FVC, lack of respiratory physiotherapy, lack of respiratory physiotherapy. of pneumococcal vaccination, mobility domain (EQ-5D-3L), and visual analog scale scores.
Discussion
The presence of comorbidities has been identified as a risk factor for increased mortality in patients with BNFC [6,17]; however, it was not considered a predictor of increased mortality in this study. Exacerbation was also identified as a risk factor for death in patients with bronchiectasis in this cohort. This finding supports a cross-sectional study conducted in Korea with 19,851 participants with and without bronchiectasis, which reported poorer QoL and mobility problems in patients with bronchiectasis [20].
In conclusion, this study identified potential factors associated with the risk of mortality in patients with bronchiectasis and emphasized that some of these factors are modifiable and therefore can be addressed through a preventive approach. Factors associated with bronchiectasis in patients with uncontrolled asthma; the NOPES score: a study in 398 patients. Severe obstructive disease: similarities and differences between smokers and non-smokers patients with COPD and/or bronchiectasis.
An analysis of the etiology, causative pathogens, imaging patterns, and treatment of Japanese patients with bronchiectasis.
HOSPITAL UNIVERSITÁRIO PEDRO ERNESTO/ UERJ
PEDRO ERNESTO/ UERJ
HOSPITAL UNIVERSITÁRIO PEDRO ERNESTO/ UERJ
ANEXO B - Instrumento de Qualidade de Vida (Versão em Papel EQ-5D-3L) HOSPITAL UNIVERSITÁRIO PEDRO ERNESTO/HUPE UNIVERSIDADE DO ESTADO DO RIO DE JANEIRO/UERJ. O instrumento consiste em um sistema descritivo com cinco dimensões: mobilidade, autocuidado, atividades habituais, dor/desconforto e ansiedade/depressão, com três níveis de resposta para cada dimensão e avaliação do estado de saúde atual do indivíduo por meio de termômetro (analógico visual escala/EQ-EAV). Considere o seu estado de saúde atual e marque com uma cruz (por exemplo, ), as caixas de cada um dos grupos seguintes, indicando qual das afirmações melhor descreve o seu estado de saúde atual.
SISTEMA DECRITIVO EQ-5D-3L
ESCALA ANALÓGICA VISUAL (EAV)
O MELHOR estado de saúde imaginável
O PIOR estado de saúde imaginável
Teve alteração da cor da secreção/escarro?
Apresentou diariamente, no período de doze meses por três meses consecutivos, tosse com secreção purulenta, mucoide ou mucopurulenta?
Você participa de algum programa de reabilitação respiratória?
Você faz uso de oxigenoterapia?
Algum médico ou outro profissional de saúde disse que você tem
Você tem ou teve problemas respiratórios ou do pulmão
Você já fez as seguintes vacinas?
Andar mais devagar que uma pessoa da mesma idade no avião por falta de ar ou por parar para respirar. Quantas vezes em um período de 90 dias você precisou procurar um pronto-socorro ou atendimento que não estava previamente agendado por problemas relacionados a bronquiectasias.
Publicação 2: Mortality and comorbidities in patients with bronchiectasis over a 3-year follow-up