1
Volume 30 - Número 2 - Abril / Junho, 2011
ASTM CODENT GAEDOW 30(2):37-80 ISSN 0101-7772
Revista GED02 Abril2011.indd 1
Revista GED02 Abril2011.indd 1 5/19/11 6:28:30 PM5/19/11 6:28:30 PM
*PMC com 18% de ICMS
*PMC com 18% de ICMS
Apresentação
20mg c/ 7 comp 14,22
20mg c/ 14 comp 23,77
20mg c/ 28 comp
31,88 55,02 103,58
45,50
Genéricos
1Pantozol
1Neo Química* (Nycomed)*
G G G G G
N N N N N
P
Apresentação
40mg c/ 7 comp 23,52
40mg c/ 14 comp 42,96
40mg c/ 28 comp
53,41 97,83 182,55
81,17
Genéricos
1Pantozol
1Neo Química* (Nycomed)*
G G G G G
N N N N N
P
Referência Bibliográfi ca: 1. Revista ABC Farma, Fevereiro 2011.
Pantoprazol.
Comprimidos gastrorresistentes 20 mg e 40 mg. Embalagens com 7, 14, 28 e 280 comprimidos revestidos. Indicações: pantoprazol 20 mg: lesões gastrintestinais leves, gastrites ou gastroduodenites agudas ou crônicas e dispepsias não ulcerosas;refl uxo gastroesofágico sem esofagites leves e manutenção de pacientes com esofagite de refl uxo cicatrizada; pantoprazol 40 mg: tratamento da úlcera péptica duodenal, úlcera péptica gástrica e das esofagites de refl uxo moderada ou severa. Contraindicações:
hipersensibilidade aos componentes da fórmula.
Não deve ser administrado em gestantes, lactante; pacientes com disfunção hepática ou renal de moderada a grave em uso de terapia combinada para erradicação do Helicobacter pylori. Não há experiência clínica com o uso em crianças. Precauções e Advertências: não é indicado o uso de 40 mg em distúrbios gastrintestinais leves.
Antes de se iniciar o tratamento, excluir a possibilidade de úlcera gástrica maligna e doenças malignas do esôfago. O diagnóstico de esofagite por refl uxo deve ser confi rmado por endoscopia. Monitorar as enzimas hepáticas em pacientes com insufi ciência hepática grave. Não se recomenda o tratamento por mais de 16 semanas.
Interações Medicamentosas:
pode alterar a absorção dos fármacos cuja biodisponibilidade seja dependente do pH do suco gástrico (cetoconazol)
e, também daqueles que são ingeridos pouco tempo antes do pantoprazol. Reações Adversas: cefaléia, dor abdominal, diarreia, constipação ou fl atulência e reações alérgicas como prurido e exantema. Náuseas, vertigem ou visão turva, edema periférico, febre, início de depressão ou mialgia foram raramente observados. Posologia: de 20 mg a 40 mg por dia. Cicatrização da úlcera péptica gastroduodenal e da esofagite de refl uxo: 40 mg por dia, antes, durante ou após o café da manhã. Pacientes idosos ou com isufi ciência renal: até 40 mg ao dia. Redução severa da função hepática: 20 mg. MS 1.5537.0012. VENDA SOB PRESCRIÇÃO MÉDICA. Março/2011.O GENÉRICO DE CONFIANÇA O ENÉ
O GENÉRICO DE CONFIANÇA
pantoprazol
QUÍMICA DA QUALIDADE:
A COMBINAÇÃO DA CONFIANÇA COM PREÇO ACESSÍVEL
SAC
S S
Anuncio PANTOPRAZOL Rev GED.indd 1
Anuncio PANTOPRAZOL Rev GED indd 1 3/15/11 3:34:43 PM3/15/11 3:34:43 PM
Revista GED02 Abril2011.indd 2
Revista GED02 Abril2011.indd 2 5/19/11 6:28:31 PM5/19/11 6:28:31 PM
Anuncio PANTOPRAZOL Rev GED.indd 1 3/15/11 3:34:43 PMPM
Gastroenterologia Endoscopia Digestiva
A Revista GED – Gastrenterologia Endoscopia Digestiva é o órgão ofi cial de circulação trimestral da SOBED (Sociedade Brasileira de Endoscopia Digestiva), da FBG (Federação Brasileira de Gastroenterologia), da SBH (Sociedade Brasileira de Hepatologia), do CBCD (Colégio Brasileiro de Cirurgia Digestiva) e da SBMD (Sociedade Brasileira de Motilidade Digestiva). Fundada pelo Capítulo de São Paulo da SOBED em 1982, durante a gestão do Prof. Dr. Arnaldo José Ganc. Registrado na Lei de Imprensa em 19/11/1981, sob o no
1.870, Lv. A, no 5o Registro de Títulos e Documentos de São Paulo.
Indexada nas seguintes bases de dados
LILACS, SCOPUS, EMBASE/EXCERPTA MÉDICA, LATINDEX e ADSAÚDE
Editor Chefe
Paulo Roberto Arruda Alves (SP)
Editores Responsáveis
José Murilo Robilotta Zeitune (SP) – Gastroenterologia Nelson Adami Andreollo (SP) – Cirurgia Digestiva Paulo Roberto Arruda Alves (SP) – Endoscopia Digestiva
Rimon Sobhi Azzam (SP) – Motilidade Digestiva Aécio Flávio Meirellez Souza (SP) – Hepatologia
Editores Associados
Arnaldo J. Ganc (SP) Jaime Natan Eisig (SP) Eduardo Luiz Rachid Cançado (SP)
Marcelo Averbach (SP) Sânzio S. Amaral (SP)
Conselho Editorial – Brasil
Admar Borges da Costa Jr. (PE), Ana Maria Pittella (RJ), Antonio Frederico N. Magalhães (SP), Artur Parada (SP), Bruno Zilberstein (SP), Claudio Coy (SP), Deborah Crespo (PA), Decio Chinzon (SP), Edmundo Pessoa Lopes (PE), Edna Strauss (SP), Edson Pedro da Silva (SC), Everson Artifon (SP), Flair Carrilho (SP), Flavio Quilici (SP), Henrique Coelho (RJ), Hugo Cheinquer (RS), Ismael Maguilnik (RS), João Carlos Andreolli (SP), João Galizzi Filho (MG), José Galvão Alves (RJ), Julio Cesar U. Coelho (PR), Lix A.R. Oliveira (SP), Lorete M.S. Kotze (PR), Lúcia Câmara Castro Oliveira (RJ), Luiz Gonzaga Vaz Coelho (MG), Luiz Pimenta Modena (SP), Luiz Roberto Lopes (SP), Márcio M. Tolentino (SP), Marcus Túlio Haddad (RJ), Mario Pessoa (SP), Martha Pedroso (SP), Maurício Fernando de Almeida Barros (SP), Orlando J.M. Torres (MA), Paulo Bittencourt (BA), Paulo R. Ott Fontes (RS), Paulo Roberto Savassi Rocha (MG), Paulo Sakai (SP), Ramiro Mascarenhas (BA), Raymundo Paraná (BA), Ricardo A. Refi netti (RJ), Roberto Dantas (SP), Sérgio Gabriel Barros (RS), Tomas Navarro
Rodriguez (SP), Venâncio A.F. Alves (SP), Vera Lúcia Andrade (MG), Walton Albuquerque (MG)
Editores Internacionais
Daniel Sifrim (Bélgica), Dirk J. Gouma (Holanda), Helena Cortez Pinto (Portugal), Jorge Daruich (Argentina)
Secretaria
Coordenadora: Fátima Lombardi dos Santos Av. Brigadeiro Faria Lima, 2.391, conj. 102 – 01452-000
São Paulo, SP
Tel.: (11) 3813-1610 – Fax: (11) 3032-1460 E-mail: [email protected]
Tiragem: 7.000 exemplares Periodicidade: trimestral
Circulação: nacional para todos os associados da SOBED, FBG, SBH, CBCD e SBMD Números anteriores e separatas: [email protected]
Editoração Eletrônica, Distribuição, Impressão e Publicidade
E-mail: [email protected] Tel.: (11) 3186-5600
Revista GED02 Abril2011.indd 3
Revista GED02 Abril2011.indd 3 5/19/11 6:28:34 PM5/19/11 6:28:34 PM
Índice
ÍNDICE ISSN 0101-7772
EUS-guided biliary drainage: a Latin American experience
Drenagem biliar eco-guiada:
experiência latino-americana
EVE R SON L. A. ARTI FON, FLAVIO FE R R E I RA, AN DR E
BOR DI N I, CAROLI NA RABE LLO, JONAS TAK ADA, PAU LO SAK AI
37
Análise de colonoscopias realizadas em centro de referência de Florianópolis para identificar fatores preditivos da presença de pólipos adenomatosos
Analysis of colonoscopies held in Florianopolis reference center to identify predictive factors associated with presence of adenomatous polyps DAN I E LA WALE N DOWS KY, LUCIANO SAPOR ITI,
TH IAGO MAMÔR U SAK AE
42
Doença do refluxo gastroesofágico:
o papel do Alginato
Gastroesophageal reflux disease: the role of Alginat
RICAR DO C. BAR BUTI
49
Colite Pseudomembranosa Pseudomembranous colitis
ALDO ROSADA CR U Z, ANTON IO BU E NO JÚN IOR, CH U ENLAY PAE S LE M E
80
A RTIGO O RIGINAL
A RTIGO DE R EVISÃO
I MAGEM EM F OCO
Osteodistrofia Hepática Hepatic Osteodystrophy
ALE XAN DR E KHODR FU RTADO, ALLANDE OLIVE I RA SANTOS, JOSÉ MU R I LO ROBI LOTTA ZE ITU N E, ELZA COTR I M SOAR E S
Rastreamento e Vigilância do Câncer Colorretal: Guidelines Mundiais
Tracking and surveillance of colorectal: guidelines world
ROS EAN E VALE R IA BICALHO FE R R E I RA AS S I S
Avanços no tratamento da bactéria Helicobacter pylori (HP)
Advances in the treatment of bacteria Helicobacter pylori (HP)
MOYSÉS MI NCI S, RICAR DO MI NCI S, RODR IGO MI NCI S
52
62
75
Revista GED02 Abril2011.indd 4
Revista GED02 Abril2011.indd 4 5/19/11 6:28:39 PM5/19/11 6:28:39 PM
Contraindicações: Hipersensibilidade conhecida à trimebutina ou a qualquer componente da fórmula.
Interações Medicamentosas: Não existem relatos a respeito de interações medicamentosas com Digedrat.
JIMENEZ
Cerca de 50% dos pacientes que procuram atendimento gastroenterológico sofrem
de problemas funcionais:
a SII é o mais frequente deles.
6Digedrat - maleato de trimebutina cápsula gelatinosa 200mg. Indicações: síndrome do intestino irritável, dispepsia e íleo pós-operatório. Contraindicações: hipersensibilidade conhecida à trimebutina ou a qualquer componente da fórmula. Precauções e Advertências: pode ser prescrito sem restrições, exceto durante os três primeiros meses de gravidez. Só deve ser usado na gravidez sob prescrição médica. Nenhum ajuste de dose é necessário para pacientes idosos. Interações medicamentosas: não existem relatos a respeito de interações medicamentosas de trimebutina na forma oral com alimentos. Nenhuma interferência significativa foi observada quanto aos parâmetros bioquímicos, exceto diminuição da contagem de eritrócitos. Relato de leucopenia também pode ocorrer. Pacientes que estiverem fazendo tratamento com Digedrat devem evitar o uso simultâneo de bebidas alcoólicas. Não existem relatos a respeito de interações medicamentosas com Digedrat. Reações adversas: os efeitos adversos relatados são raros, e incluem vermelhidão cutânea (< 2% dos pacientes), sonolência (0,08%) e, muito raramente, alguns casos de dor de cabeça, boca seca, constipação, diarreia, vômitos, fraqueza e tonturas (menos de 0,01% de incidência para cada efeito colateral). Posologia: deve ser administrado por via oral. Adultos: 1 cápsula, duas a três vezes ao dia, preferencialmente antes das refeições. A duração do tratamento deve ser determinada pelo médico. A dose oral máxima diária recomendada é de 600mg. Crianças: só deve ser administrado a crianças com mais de 12 anos de idade. Registro no MS: 1.0181.0477.
VENDA SOB PRESCRIÇÃO MÉDICA. AO PERSISTIREM OS SINTOMAS, O MÉDICO DEVERÁ SER CONSULTADO. SAC 0800 7717017. Material destinado a profissionais de saúde habilitados a prescrever ou dispensar medicamentos.
Referências bibliográficas: 1.DELVAUX M & WINGATE D. Trimebutine: Mecanism of action, effects on gastrointestinal function and clinical results. J Int. Med. Res., 25(5): 225-46;
1997. 2.TANAKA M. Gastric ulcer, motility and trimebutine. J Gastroenterol., 33(6): 916-7; 1998. 3. Micromedex: Drugdex Evaluations Trimebutine. Acesso em 28 Agosto 2006.
4. RAMON JF. et al. Pharmacological Properties of Trimebutine and N-monodesmethyltrimebutine. JPET, 289(3): 1391-97; 1980. 5. POYNARD T. et al. Meta-analysis of smooth muscle relaxants in the treatment of irritable bowel syndrome. Aliment Pharmacol Ther., 15(3): 355-61; 2001. 6. GRUNDMANN O, et al. Irritable bowel syndrome: epidemiology, diagnosis and treatment: an update for health-care practitioners. J Gastroenterol. Hepatol; 25: 691-9.7. Bula do produto Digedrat (maleato de trimebutina). MS - 1.0181.0477.
MÚLTIPLA AÇÃO NA SII EM APENAS UMA CÁPSULA
1,2Posologia:
72 a 3 cápsulas ao dia, preferencialmente antes das refeições.
Rapidez no alívio da dor;
3Ação moduladora na constipação e diarreia;
2,4Melhora global dos sintomas.
5Apresentações:
7cápsulas de 200 mg com 20, 30 e 60 unidades.
Revista GED02 Abril2011.indd 5
Revista GED02 Abril2011.indd 5 5/19/11 6:28:39 PM5/19/11 6:28:39 PM
S
OCIEDADEB
RASILEIRA DEE
NDOSCOPIAD
IGESTIVA(SOBED)
Diretoria Executiva (2010-2012): Presidente: Sérgio Luiz Bizinelli (PR) • Vice-Presidente: Flávio Hayato Ejima (DF) • 1o Secretário: Jimi Izaques Bifi Scarparo (SP) • 2º Secretário: Afonso Celso da Silva Paredes (RJ) • 1o Tesoureiro: Thiago Festa Secchi (SP) • Sede: Rua Peixoto Gomide, 515 – cj. 14 – 01409-001 – São Paulo, SP – Tel./fax: (11) 3148-8200 e 3148-8201 - E-mail: [email protected] – Site: sobed.org.br
F
EDERAÇÃOB
RASILEIRADEG
ASTROENTEROLOGIA(FBG)
Diretoria (2010-2012): Presidente: José Galvão Alves (RJ) • Vice-Presidente: José Roberto de Almeida (PE)
• Secretário Geral: Sender Jankiel Mizsputen (SP) • 1o Secretário: Adávio de Oliveira e Silva (SP) • Diretor Financeiro:
Rubens Basile (RJ) • Coordenador do FAPEGE: Maria do Carmo Friche Passos (MG) • Presidente Eleito (2012-2014):
José Roberto de Almeida (PE) • Sede: Av. Brig. Faria Lima, 2.391, 10º andar – cj. 102 – 01452-000 – São Paulo, SP – Tel.: (11) 3813-1610 / 3813-1690. Fax: (11) 3032-1460 - E-mail: [email protected] – Site: www.fbg.org.br
S
OCIEDADEB
RASILEIRA DEH
EPATOLOGIA(SBH)
Diretoria 2009-2011: Presidente: Raymundo Paraná Filho • 1º Vice-Presidente: Mário Guimarães Pessoa • Secretário Geral: Paulo Lisboa Bittencourt • Secretária Adjunta: Celina Maria Lacet • 1º Tesoureiro: Delvone Freire Gil Almeida
• Presidente Eleito 2011-2013: Henrique Sérgio M. Coelho • Sede: Av. Brig. Faria Lima, 2.391, 10º andar – cj.
102 – 01452-000 – São Paulo, SP – Tel.: (11) 3812-3253 - E-mail: [email protected] – Site: www.
sbhepatologia.org.br
Diretoria - Gestão 2010-2011: Presidente: Eponina M. O. Lemme • Vice-Presidente: Sânzio Santos Amaral • Secretário Geral:
Rosana Bihari Schechter • 1o Secretário: Luciana Dias Moretzsohn • 1o Tesoureiro: Luiz João Abrahão Junior • Sede: Av.
Brigadeiro Faria Lima, 2391, Conj. 102, Jardim Paulistano – 01452-000 – São Paulo, SP – Fone: (11) 3518-9117 – E-mail:
[email protected] – Site: www.sbmd.org.br
S
OCIEDADEB
RASILEIRA DEM
OTILIDADED
IGESTIVA(SBMD) C
OLÉGIOB
RASILEIRO DEC
IRURGIAD
IGESTIVA(CBCD)
Diretoria - Gestão 2011-2012: Presidente: Cleber Dario Pinto Kruel • Vice-Presidente: Luis Augusto Carneiro D’Albuquerque
• 1o Secretário: Cláudio José Caldas Bresciani • 2o Secretário: Nicolau Gregori Czezcko • 1o Tesoureiro: Bruno Zilberstein
• Presidente Eleito (2013-2014) Ivan Cecconello • Sede: Av. Brig. Luiz Antonio, 278 – salas 10 e 11 – 01318-901 – São Paulo, SP – Tels.: (11) 3289-0741 / 3266-6201 / Fone/Fax: (11) 3288-8174 – E-mail: [email protected] – Site: www.cbcd.org.br
Diretoria das Sociedades
Revista GED02 Abril2011.indd 6
Revista GED02 Abril2011.indd 6 5/19/11 6:28:40 PM5/19/11 6:28:40 PM
A GED, órgão ofi cial da Sociedade Brasileira de Endoscopia Digestiva – SOBED, da Federação Brasileira de Gastroenterologia – FBG, da Sociedade Brasileira de Hepatologia – SBH, do Colégio Brasileiro de Cirurgia Digestiva – CBCD e da Sociedade Brasileira de Motilidade Digestiva – SBMD, tem por objetivo a divulgação de trabalhos que contribuam para o progresso da Gastroenterologia, da Endoscopia Digestiva, da Hepatologia, da Cirurgia Digestiva e da Motilidade Digestiva.
São publicáveis as colaborações que, enviadas à Secretaria da GED (Av. Brig. Faria Lima, 2.391 – 10o andar – cj. 102 –1452- 000 – São Paulo, SP, email [email protected]), forem aceitas pelo Conselho Editorial e não tenham sido previamente publicadas e nem o venham a ser, simultaneamente, em outros periódicos.
Serão aceitos artigos escritos na língua portuguesa. A critério do Conselho Editorial, poderão ser considerados manuscritos em língua inglesa e castelhana.
A GED adota as regras da Uniform Requirements for Manuscripts Submitted to Biomedical Journals emitidas pelo International Committee for Medical Journal Editors, disponível na Internet (http:// www.icmje.org).
C
ONTEÚDO DAGED
Editoriais
Destinam-se à apresentação de temas de natureza polêmica, atual e de impacto, nos quais os editores da GED percebam a necessidade de manifestar de forma sintética a visão destes editores, abordando ou não artigos publicados na GED. Serão escritos pelos editores e/ou membros do Conselho Editorial ou, mediante convite, por outros especialistas.
Artigos Originais
De pesquisa clínica e/ou experimental, devem apresentar a aprovação da pesquisa pelo Conselho de Ética do hospital, serviço ou instituição onde o trabalho foi realizado. Devem ser estruturados com os seguintes itens: Resumo (e Unitermos), Introdução, Métodos, Resultados, Discussão, Conclusões e Referências Bibliográfi cas (acompanhado de unitermos).
Introdução – Em que se apresenta a justifi cativa para o estudo, com referências relacionadas ao assunto e o objetivo do artigo.
Métodos – Em que se apresentam: a) descrição da amostra utilizada; b) mencionar se há consentimento informado;
c) identifi cação dos métodos, aparelhos e procedimentos utilizados, de modo a permitir a reprodução dos resultados pelos leitores; d) breve descrição e referências de métodos publicados mas não conhecidos amplamente; e) descrição de métodos novos ou modifi cados; f) se for o caso, referir a análise estatística utilizada, bem como os programas empregados.
Resultados – Em que serão apresentados os resultados em
sequência lógica, em forma de texto, tabelas e ilustrações;
recomenda-se evitar repetição excessiva de dados em tabelas ou ilustrações e no texto. No texto, números menores que 10 serão grafados por extenso; de 10 em diante, serão expressos em algarismos arábicos.
Discussão – Em que serão enfatizados: a) os aspectos originais e importantes do artigo, evitando repetir dados já apresentados anteriormente; b) a importância e as limitações dos achados, confrontando com dados da literatura;
c) a ligação das conclusões com os objetivos do estudo;
d) as conclusões decorrentes do estudo.
Referências – As referências bibliográfi cas devem ser numeradas na ordem em que são citadas primeiramente no texto. Elas devem seguir as regras do Uniform Requirements for Manuscripts Submitted to Biomedical Journals – http://www.icmje.org. Alguns exemplos mais comuns são apresentados a seguir.
Exemplos:
1. Artigo padrão em periódico (devem ser listados todos os autores; se houver mais de seis, citar os seis primeiros, seguidos por et al.): Alper CA, Kruskal MS, Marcus- Bagle Y, Craven DE, Katz AJ, Brint SJ, et al.. Genetic prediction of response to hepatitis B vaccine. N Engl J Med. 1989;321:708-12.
2. Autor institucional: NHI Consensus Development Panel on Helicobacter pylori in Peptic Ulcer Disease.
Helicobacter pylori in peptic ulcer disease. JAMA.
1994;272:65- 9.
3. Livro com autor(es) responsável(is) por todo o conteúdo: With TK. Bile pigments. New York: Academic Press, 1968.
4. Livro com editor(es) como autor(es): Magrath I, editor. The non-Hodgkin’s limphomas. 2nd ed. London: Arnold, 1997.
5. Capítulo de livro: Warshaw AL, Rattner DW. Residual common duct stones and disorders of duodenal ampullae.`In: Ellis H, editor. Maingot’s abdominal operations. New York: Lange Publishers, 1990:1471-2 Os títulos dos periódicos devem ser abreviados de acordo com o Index Medicus (List of Journals Indexed). Se o periódico não constar dessa lista, grafar o nome por extenso.
Tabelas – As tabelas devem possuir um título sucinto, com itens explicativos dispostos em seu pé. Devem ser numerados sequencialmente com algarismos arábicos.
Figuras – Serão aceitas fi guras em preto e branco. Figuras coloridas poderão ser publicadas quando forem essenciais para o conteúdo científi co do trabalho; nesses casos, o ônus de sua publicação caberá aos autores.
Informações aos Autores
Modifi cado em outubro de 2007
Revista GED02 Abril2011.indd 7
Revista GED02 Abril2011.indd 7 5/19/11 6:28:40 PM5/19/11 6:28:40 PM
Artigos de Revisão
Somente serão aceitos quando, a convite dos editores da publicação, fi zerem parte da linha de pesquisa do autor, comprovada pela presença de artigos originais na bibliografi a e citados no texto.
Relato de Caso
Devem ser objetivos e precisos, contendo os seguintes itens:
1) Resumo (e Unitermos) e Summary (e keywords); 2) Introdução; 3) Relato objetivo; 4) Discussão; 5) Conclusões; 6) Referências bibliográfi cas.
Cartas ao Editor
Cartas endereçadas ao(s) editor(es) serão consideradas para publicação se promoverem discussão intelectual sobre determinado artigo de publicação recente. Devem conter título informativo e não mais que 500 palavras. Se aceita, uma cópia será enviada ao autor do trabalho que suscitou a discussão, com convite para submeter uma réplica que será publicada junto com a carta.
Confl ito de interesses
Conforme determinação da Agência Nacional de Vigilância Sanitária (RDC 102/2000) e do Conselho Nacional de Saúde (196/96) o(s) autor(es) deve(rão) tornar explícito, por meio de formulário próprio (Divulgação de potencial confl ito de interesses), qualquer potencial confl ito de interesse relacionado ao artigo submetido. A presente exigência visa informar sobre relações profi ssionais e/ou fi nanceiras (como patrocínios e participação societária) com agentes fi nanceiros relacionados aos produtos farmacêuticos ou equipamentos envolvidos no artigo, os quais podem teoricamente infl uenciar as interpretações deste. A existência ou não de confl ito de interesses declarado estará ao fi nal de todos os artigos publicados.
Bioética de experimentos com seres humanos Experimentos envolvendo seres humanos devem seguir reso- lução específi ca do Conselho Nacional de Saúde (196/96), dispo- nível na Internet (http://conselho.saúde.gov.br//docs/Resolu- ções/Reso/96de96.doc), incluindo a assinatura de um termo de consentimento informado e a proteção da privacidade dos voluntários.
Bioética de experimentos com animais
Experimentos envolvendo animais devem seguir resoluções específi cas (Lei 6.638, de 8/5/1979, e Decreto 24.645, de 10/7/1934).
Ensaios clínicos
Artigos que contêm resultados de ensaios clínicos deverão possibilitar todas as informações necessárias à sua adequada avaliação, conforme previamente estabelecido. Os autores deverão refeir-se ao “CONSORT” (www.consort.statement.org).
Revisão pelos pares
Todos os artigos submetidos serão avaliados por dois revisores, os quais emitirão parecer fundamentado que servirá para o(s) editor(es) decidir(em) sobre sua aceitação. Os critérios de avaliação incluem originalidade, contribuição para corpo de conhecimento da área, adequação metodológica, clareza e atualidade. Os artigos aceitos para publicação poderão sofrer revisões editoriais para facilitar sua clareza e entendimento sem alterar seu conteúdo.
Direitos autorais
Todas as declarações contidas nos artigos serão da inteira responsabilidade dos autores. Aceito o artigo, a GED passa a deter os direitos autorais do material. Assim, todos os autores dos artigos submetidos à GED devem encaminhar um Termo de Transferência de Direitos Autorais. O autor responsável pela correspondência receberá 20 separatas impressas do artigo e o arquivo correspondente em formato pdf.
C
OMO ENVIAR O ARTIGOO(s) autor(es) deve(m) encaminhar:
• Carta de apresentação assinada por todos os autores ou pelo primeiro autor em nome dos demais, contendo: 1) informação à respeito de submissão prévia ou dupla ou submissão de qualquer parte do artigo atual; 2) uma declaração de relações, fi nanceiras ou não, que possam levar a confl ito de interesses; 3) uma declaração de que o artigo foi lido e aprovado por todos os coautores e que os critérios necessários para a declaração de autoria (consultar Uniform Requirements for Manuscripts Submitted to Biomedical Journals) foram alcançados por todos os autores e que cada autor afi rma que os dados do manuscrito são verdadeiros; 4) nome, endereço, telefone e e-mail do autor para correspondência; ele será o responsável pela comunicação com os outros autores a respeito de revisões e provas gráfi cas.
• Termo de Divulgação de Potencial Confl ito de Interesses.
• Termo de Transferência de Direitos Autorais.
• Três cópias do artigo, digitado em espaço duplo, impressas em papel tamanho carta em somente um dos lados, com margens de 2,5cm e espaço 1,5, numerando as páginas no canto superior direito;
as legendas das fi guras, as fi guras propriamente ditas e as tabelas devem vir ao fi nal, anexadas a cada cópia; assinalar no texto os locais adequados para inserção de fi guras e tabelas.
• Três conjuntos de fi guras em cópia fotográfi ca brilhante.
• Um CD contendo somente um arquivo do texto, correspondente ao artigo, e os arquivos correspondentes a fotos ou fi guras.
Como preparar o CD
• CD formatado compatível com IBM/PC;
• Usar editor de texto Microsoft Word para Windows;
• O arquivo de texto deve conter somente o texto, da página-título até as referências, e as tabelas;
• As fi guras não devem ser incluídas no mesmo arquivo do texto;
• Colocar no CD a última versão do artigo, idêntica à versão impressa;
• Etiquetar o CD informando o programa e a versão utilizados, bem como o nome do arquivo.
A submissão do artigo pelo correio eletrônico (e-mail) possibilita maior agilidade no procedimento de revisão. Para isso, será necessário o envio dos arquivos contendo o texto e as fi guras para o e-mail da GED ([email protected]).
Mensagem aos editores com identifi cação dos autores deve ser enviada, acompanhada dos endereços convencional e eletrônico e de informações sobre o formato utilizado. O artigo deverá ser enviado em anexo, como attachment, no formato Word para Windows. As fi guras deverão estar nos formatos jpg ou tif.
INFORMAÇÕESAOS AUTORES
Revista GED02 Abril2011.indd 8
Revista GED02 Abril2011.indd 8 5/19/11 6:28:40 PM5/19/11 6:28:40 PM
Revista GED02 Abril2011.indd 9
Revista GED02 Abril2011.indd 9 5/19/11 6:28:44 PM5/19/11 6:28:44 PM
Anuncio PRAZOl 2011-E.indd 1
A 5/18/11 4:22:08 PM
GED is the official journal of the Brazilian Society of Digestive Endoscopy – SOBED, the Brazilian Federation of Gastroenterology – FBG, the Brazilian Society of Hepatology – SBH, the Brazilian College of Digestive Surgery – CBCD, and of the Brazilian Society of Digestive Motility – SBMD, and the purpose of the journal is to publish papers that may contribute towards the progress of Gastroenterology, Digestive Endoscopy, Hepatology, Digestive Surgery and Digestive Motility. Papers sent to the GED Secretariat (Av.
Brig. Faria Lima, 2.391 – 10o andar – cj. 102 –1452-000 – São Paulo, SP, Brazil, e-mail [email protected]), which are accepted by the Editorial Board, and which have not been previously or will not be concomitantly published in other journals may be published.
Papers drafted in the Portuguese language will be accepted. At the discretion of the Editorial Board, papers in the Spanish and in the English language may also be accepted.
GED adopts the Uniform Requirements for Manuscripts Submitted to Biomedical Journals of the International Committee for Medical Journal Editors, available in the Internet (http://www.icmje.org).
GED C
ONTENTSEditorials
Intended to present polemic, current, and impacting topics whenever GED editors feel the need to present their view in a synthetic manner, whether or not such topics are presented in GEDpublished papers. Editorials are written by the editors and/or by Editorial Board members, or by invited specialists.
Original Articles
Clinical and/or experimental research papers should present the approval of the research given by the Ethics Committee of the hospital, clinic, or institution were the study was carried out. The following items must be included:
Summary (and keywords), Introduction, Methods, Results, Conclusions, References, and Summary and Keywords.
Introduction – Presents the justification for the study, with references related to the topic and the objective of the paper.
Methods – Presenting: a) description of the sample used; b) mention whether or not an informed consent has been obtained; c) identification of methods, devices, and procedures used in order to permit reproduction of the results by the readers; d) brief description and references to methods that have been published but that are not broadly know; e) description of new methods or of
modified methods; f) mention the statistical analysis or the software used, as the case may be.
Results – Presenting results in a logical sequence, in text format with tables and illustrations; authors should avoid excessive information repetition in the tables and illustrations and in the text. In the text, numbers below ten will be written in full, whereas numbers 10 and beyond will be written in Arabic numbers.
Discussion – Emphasis will be given to: a) original and major aspects of the paper, without repetition of the aspects previously presented; b) relevance and limitations of the fi ndings, comparing them to information in the literature; c) connection of the conclusions to the objectives of the study;
d) conclusions arising out of the study.
References – Bibliographic references should appear in the order in which they are fi rst quoted in the text. They should follow the Uniform Requirements for Manuscripts Submitted to Biomedical Journals – http://www. icmje.org. Some of the more usual example are presented.
Examples:
1. Standard paper in journals (all authors must be listed;
if they are more than six, list the fi rst six followed by et al.): Alper CA, Kruskal MS, Marcus-Bagle Y, Craven DE, Katz AJ, Brint SJ, et al.. Genetic prediction of response to hepati tis B vaccine. N Engl J Med. 1989;321:708-12.
2. Autor institucional: NHI Consensus Development Panel on Helicobacter pylori in Peptic Ulcer Disease. Helicobacter pylori in peptic ulcer disease. JAMA. 1994;272:65- 9.
3. Book with author(s) responsible for the full text With TK.
Bile pigments: New York: Academic Press, 1968.
4. Book with editor(s) as author(s): Magrath I, editor. The non-Hodgkin’s limphomas. 2nd ed. London: Arnold, 1997.
5. Chapter of a book: Warshaw AL, Rattner DW. Residual common duct stones and disorders of duodenal ampullae. In: Ellis H, editor. Maingot’s abdominal operations. New York: Lange Publishers, 1990:1471-2.
The titles of journal should be abbreviated according to the Index Medicus (List of Journals Indexed). If the journal is not included in such list, write the name in full.
Tables – Tables should have a summarized title, with explanatory comments at the foot of the table. They should be sequentially numbered with Arabic numbers.
Figures – Black and white fi gures will be accepted. Color fi gures may be published when they are essential for the scientifi c contents of the paper; in such case, the cost of publishing colored fi gures will be covered by the authors.
Informations to Authors
Revista GED02 Abril2011.indd 10
Revista GED02 Abril2011.indd 10 5/19/11 6:28:45 PM5/19/11 6:28:45 PM
Economia 4
Melhor relação custo-benefício entre os IBPs
1-4Ação rápida
5Prazol® apresenta pico médio plasmático entre 1,5 e 2,2 horas emjejum5
A
Ação bactericida
6O lansoprazol possui ação bactericida na eliminação do H. pylori6
Efe ei ito prolongado
5As cápsulas gelatinosas de
A Prazol®
têm grânulos de liberação retardada5
*Fonte: Revista ABC Farma PMC I8% - Maio/2011 Apresentações: 30mg 14 cáp. / 15mg 28 cáp.
R$
*4
Uma empresa do Grupo sanofi -aventis
Anuncio PRAZOl 2011-E.indd 1
Anuncio PRAZOl 2011-E indd 1 5/18/11 4:22:08 PM5/18/11 4:22:08 PM
Revista GED02 Abril2011.indd 11
Revista GED02 Abril2011.indd 11 5/19/11 6:28:48 PM5/19/11 6:28:48 PM
AF A
Revision Articles
Will be accepted only when the editors have invited the author to write such articles, when they are part of the research line of the author as evidenced by the presence of original articles in the bibliography and in the quotations in the text.
Case Report
Should be objective and precise, with the following items:
1) Summary (and keywords); 2) Introduction; 3) Objective Report; 4) Discussion; 5) Conclusions; 6) Bibliography.
Letters to the Editor
Letters sent to the editor(s) will be considered for publication if they carry an intellectual discussion regarding a recently published article. They should have an informative title and not more than 500 words. If accepted, a copy will be sent to the author of the paper that raised the discussion, with an invitation to submit a reply to be published together with the letter.
Confl ict of interests
As determined by the Sanitary Surveillance Agency (RDC 102/2000) and by the National Health Council (196/96) author(s) should inform explicitly in the adequate form (Disclosure of potential confl ict of interests) about any potential confl ict of interests related to the paper submitted. This requirement is intended to inform about professional and/or fi nancial relations (with sponsorships and corporate interests) with fi nancial agents related to medical drugs or equipment involved in the paper, which may theoretically infl uence the interpretation of the paper. The existence or non-existence of a declared confl ict of interests shall be included at the end of all articles published.
Bioethics of experiments involving human beings Experiments involving human beings shall follow the specifi c resolution of the National Health Council available in the Internet address (http://conselho.saúde.gov.br//docs/Resoluções/Reso/
96de96.doc), including the signature of an informed consent and the protection to volunteer privacy.
Bioethics of experiments involving animals
Experiments involving animals shall follow specifi c resolutions (Law 6,638, of May 8, 1979, and Decree 24,645, of July 10, 1934).
Clinical Assays
Article containing results of clinical assays should disclose all information required for their proper evaluation, as previously established. Authors shall refer to the “CONSORT” (www.
consort. statement.org).
Review by peers
All articles submitted shall be evaluated by two analysts, who shall issue a fundamented opinion to be used by the editors to decide whether or not the paper will be accepted.
Evaluation criteria include originality, contribution to the body of knowledge in the area, methodological adequacy, clarity, and contemporaneity. Articles accepted for publication may have editorial revisions to improve clarity and understanding without changing its contents.
Copyrights
All statements contained in the articles will be under the full
responsibility of the authors. After and article is accepted, GED becomes the owner of copyrights of the material. Thus, all authors of the articles submitted to GED should also send a Deed of Copyright Assignment. The author incharge of receiving letters from the readers will receive 20 printed copies of the article and the corresponding pdf fi le.
H
OW TO SENDA PAPERThe author(s) should send:
• A letter of submission signed by all authors or by the fi rst author to appear in the list on behalf of all authors, containing:
1) information regarding a prior or double submission of any part of the paper being submitted; 2) a declaration of relations, fi nancial or otherwise, that could lead to a confl ict of interests;
3) a declaration that the article has been read and approved by all coauthors and that the criteria to claim authorship (see Uniform Requirements for Manuscripts Submitted to Biomedical Journals) have been met by all authors and that each author represents that the information in the manuscript is true; 4) name, address, telephone number, and e-mail of the author who will receive letters; this author will be responsible to communicate revisions and print proofs to the other authors.
• Deed of Disclosure of a Potential Confl ict of Interests.
• Deed of Copyright Assignment.
• Three copies of the paper typed in double space, printed in letter-sized paper only on the front (without printing on the back), margins of 2.5 cm and 1.5 space, with pages numbered in the upper right corner; fi gure legends, fi gures, and tables should be placed at the end, attached to each copy; indicate in the text the place to insert fi gures and tables.
• Three sets of fi gures in shiny photographic copies.
• A CD containing the text fi le only, with the paper text, and the fi les containing photographs or fi gures.
How to prepare the CD
• Formatted CD compatible with IBM/PC;
• Use Microsoft Word for Windows text software;
• The text fi le to contain only the text, from the title page to the references, and the tables;
• Figures are not to be included in the text fi le;
• Place in the CD the lest version of the paper, identical to the printed version submitted;
• Label the CD informing the software and the version used, and the fi led name.
Submission of a paper by e-mail allows for greater effi ciency of the revision procedures. For that purpose, the text and the fi gures fi les shall be sent to the GED e-mail ([email protected]).
Messages to the editors with identifi cation of the authors should be sent together with conventional and electronic addresses, and together with information about the format used. The paper shall be sent as an attachment, as a Word for Windows fi le.
Figures shall be in the jpg or tif formats.
INFORMATIONSTO AUTHORS
Revista GED02 Abril2011.indd 12
Revista GED02 Abril2011.indd 12 5/19/11 6:28:50 PM5/19/11 6:28:50 PM
AF An Ultraproct 21 5x28 CV 11 04 11 indd 1 4/11/11 4:36:41 PM Revista GED02 Abril2011.indd 13
Revista GED02 Abril2011.indd 13 5/19/11 6:28:52 PM5/19/11 6:28:52 PM
Patrick
Pavilhão Vermelho - Rua M, 52 Visite nosso estande
Máximo conforto para atender às exigências da sua profi ssão.
Visite nosso novo site
www.
maxiconfort
.com.brSolado Á exível
e anti-derrapante Tecnologia de amortecimento
interno
Os produtos Maxi Confort estão à venda nas lojas da PONTAL calçados, localizadas nos melhores
enderecos. Informacoes no site www.pontal.com.br
Sistema de absorção
de transpiração Produzido com as melhores matérias- primas do mercado
Revista GED02 Abril2011.indd Sec2:14
Revista GED02 Abril2011.indd Sec2:14 5/19/11 6:28:53 PM5/19/11 6:28:53 PM
37
S
UMMARYOur team was the fi rstly to perform an EUS biliary and pancreatic drainage in Latin america. When distal biliary obstruction (pancreatic and papillary lesions) occurs, EUS-guided fi stulization between the common bile duct and duodenal bulb is an effi cient and feasible strategy on achieving resolution of jaundice with low morbidity and mortality rates under experienced hands. EUS-guided hepaticogastrostomy and coledochoduodenostomy are advanced procedures on biliary and pancreatic endoscopy and together make up the echo-guided biliary drainage.
Hepaticogastrostomy is indicated in cases of hilar obstruction, while the procedure of choice is coledochoduodenostomy in distal lesions. Both procedures must be done only after unsucessfull ERCP. The indication of these procedures must be made under a multidisciplinary view while sharing information with the patient or legal guardian. This study was conducted from june 2007 until march 2010.
Keywords: Endoscopic ultrasound, palliation, biliary.
R
ESUMONossa equipe foi a primeira a realizar drenagem pancreático- biliar na América Latina. Na ocasião de obstrução distal (massas em cabeça de pâncreas e papila duodenal maior), a fi stulização eco-guiada entre o colédoco médio e o bulbo duodenal é uma estratégia factível no alívio da icterícia e com baixa morbimortalidade em equipes experientes.
A hepaticogastrostomia e coledocoduodenostomia eco- guiadas são procedimentos avançados na endoscopia
bilio-pancreática e compõe em conjunto a drenagem biliar eco-guiada. A hepaticogastrostomia é indicada nos casos de obstrução hilar, enquanto a coledocoduodenostomia é procedimento de escolha nas lesões distais. Convém lembrar que a drenagem biliar eco-guiada deve ser a segunda opção depois da falha da colangiografia endoscópica retrógrada. A indicação destes procedimentos deve ter alcance multidisciplinar e compartilhar a informação com o paciente ou responsável legal. Este estudo foi realizado entre junho de 2007 até março de 2010.
Unitermos: Ultrassom Endoscópico, Biliar, Paliação.
I
NTRODUCTIONEndoscopic transpapillary biliary drainage is the procedure of choice for biliary decompression in patients with unresectable pancreatic cancer associated to obstructive jaundice1,2,3,4. However, ERCP failure can occur in 3 to 10% of cases1,2,4, even in experienced hands. This failure is related to operator inexperience, anatomic variation, tumor extension, prior surgery or incomplete drainage1,2,3,4. The alternatives for biliary drainage in unsuccessful ERCP cases include precut sphincterotomy when a pathologic lesion is suspected, second-attempted ERCP, percutaneous transhepatic drainage (PTBD) or surgery1,3,5. However, PTBD has a complication rate of up to 30%, including biliary fi stula, peritonitis, empyema, hematoma and liver abscesses1,6. Futhermore, if subsequent internal drainage cannot be achieved, the patients would have to accept long-term external biliary drainage which can be uncomfortable and is non physiological, with signifi cant
Artigo Original
EUS-guided biliary drainage: a Latin American experience
Drenagem biliar eco-guiada: experiência latino-americana
EVERSON L. A. ARTIFON1, FLAVIO FERREIRA2, ANDRE BORDINI2, CAROLINA RABELLO2, JONAS TAKADA3, PAULO SAKAI4 GI ENDOSCOPY SERVICE,UNIVERSITYOF SÃO PAULO (USP),SÃO PAULO, BRAZIL.
1. Livre-docente da Universidade de São Paulo (USP); Coordenador do Setor de Endoscopia Biliopancreatica (CPRE) do Serviço de Endoscopia do HCFMUSP; Chefe do Serviço de Endoscopia do Hospital Ana Costa - HAC, Santos. 2. Alunos de Iniciação Cientifi ca (IC) da FMUSP. 3. Pos-graduando (Nível Doutorado) do Departamento de Cirurgia da FMUSP. 4. Livre-docente da Universidade de São Paulo (USP), Professor Associado da FMUSP, Diretor do Serviço de Endoscopia do HCFMUSP. Endereço para correspondência: Everson Luiz A. Artifon - Rua Guimarães Passos, 260 - Apto. 121 – Vila Mariana – São Paulo – SP - CEP 04107-030 - e-mail: [email protected] Recebido em: 31/8/2010. Aprovação em: 15/9/2010.
GED gastroenterol. endosc.dig. 2011: 30(2):37-41
30(2):37-41
Revista GED02 Abril2011.indd Sec1:37
Revista GED02 Abril2011.indd Sec1:37 5/19/11 6:28:54 PM5/19/11 6:28:54 PM
impairment of quality of life 1. Surgery offers long-term patency but is associated with increased morbidity and mortality6. Recently, EUS-guided biliary drainage has been shown in several reports as an alternative treatment for the management of patients with malignant obstructive jaundice, with acceptable success and complication rates7,8. These techniques include EUS-guided transpapillary rendezvous technique, EUS-guided choledochoduodenostomy and EUS- guided hepaticogastrostomy.
EUS-guided biliary drainage has many advantages over PTBD1,3,4. The proximity of the transducer to the bile duct during EUS is the major advantage4. Even in patients who have undergone total gastrectomy or partial gastrectomy with a Billroth II reconstruction, EUS can reveal the etiology of extrahepatic cholestasis, situations in that ERCP may not be possible1,3,4,5,9. Other advantages include puncture of the biliary tree with color-Doppler information to avoid vascular injury, the lack of ascites in the interventional fi eld and the lack of an external tube, improving the quality of life of the patients1,10.
The main risk of EUS-guided biliary drainage is bile leakage, especially if stent insertion is unsuccessful1. Burmester et al reported the failure of stent placement in 1 of their 4 patients, causing bile peritonitis3. They also reported that only local
peritonitis developed, which did not contribute to the death of the patient. Some investigators recommend the transhepatic approach to decrease the risk of biliary peritonitis in case of stent failure3. Other complications include pneumoperitoneum and minor bleeding1,2,5.
The EUS-guided biliary drainage is being evaluated under research protocols in Sao Paulo University Medical School, aiming at standardizing the procedural technique, with emphasis to improve technical success rates and safety profi le of the procedure. Our experience is shown in Table 1.
E
US-
GUIDED BILIARY RENDEZVOUSEUS rendezvous to obtain bile duct access for conventional ERCP was fi rst reported in 2004, by Mallery et al11. This technique is used solely to puncture the obstructed bile duct and pass a guide wire antegrade through the native papilla to allow subsequent ERCP.
EUS-guided biliary rendezvous can be done through a transduodenal route to the common bile duct or through a transgastric route to the intrahepatic ducts.
Technical successs rate is about 80%12. Complications are uncommon, but duodenal perforation and fl uid leaks have been described12.
EUS-GUIDEDBILIARYDRAINAGE: A LATIN AMERICANEXPERIENCE
GED gastroenterol. endosc.dig. 2011: 30(2):37-41
30(2):37-41
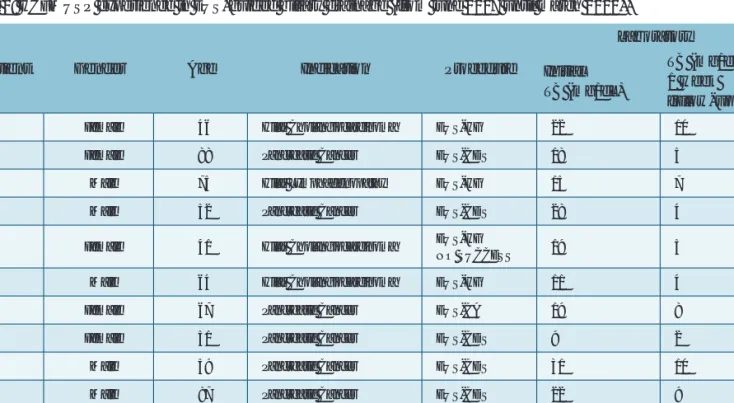
Table 1: HCFMUSP experience in EUS-guided biliary drainage (from june 2007 until march 2010).
Patient Gender Age Indication Procedure
Laboratory Initial
TB (mg/dL)
TB (mg/dL) 1 week follow-up
1 Female 46 Hilar Cholangiocarcinoma EUS-HG 22 10
2 Female 88 Pancreatic Cancer EUS-CDS 18 5
3 Male 75 Hilar Lymphadenopathy EUS-HG 15 7
4 Male 52 Pancreatic Cancer EUS-CDS 28 4
5 Female 41 Hilar Cholangiocarcinoma EUS-HG
NO SUCCESS 19 5
6 Male 64 Hilar Cholangiocarcinoma EUS-HG 11 4
7 Female 67 Pancreatic Cancer EUS-CA 19 8
8 Female 51 Pancreatic Cancer EUS-CDS 9 2
9 Male 59 Pancreatic Cancer EUS-CDS 31 10
10 Male 87 Pancreatic Cancer EUS-CDS 22 9
11 Male 81 Pancreatic Cancer EUS-CDS 16 5
12 Female 95 Pancreatic Cancer EUS-CDS 12 4
Variables presented. TB: Total Bilirubin; EUS-CDS: EUS-guided choledocoduodenostomy; EUS-HG: EUS-guided hepatogastrostomy; EUS-CA: EUS-guided choledocoantrostomy.
38
Revista GED02 Abril2011.indd Sec1:38
Revista GED02 Abril2011.indd Sec1:38 5/19/11 6:28:55 PM5/19/11 6:28:55 PM
39 Advantages of this procedure include achievement of biliary
drainage at a single session by using conventional ERCP techniques, and possibly fewer complications than other EUS transluminal drainage approaches. However, a limitation of this technique is that it can be attempted only in patients in whom the papilla is endoscopically accessible.
E
US-G
UIDEDC
HOLEDOCHODUODENOSTOMY Giovannini et al performed a choledochoduodenal fi stula under EUS guidance in a patient with pancreatic cancer using a needle knife followed by transduodenal stenting13. Since then, many studies described this procedure, with high success rates (92%) and low rate of procedure-related complications (19%)7.EUS-guided choledochoduodenostomy (EUS-CDS) has to be done after failure of ERCP and must be performed by an experienced endoscopist. Prophylactic antibiotics are administered prior to the procedure.
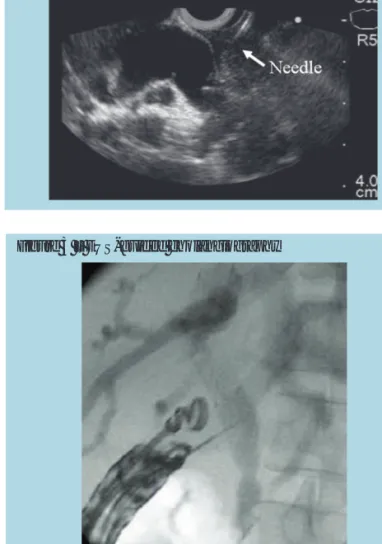
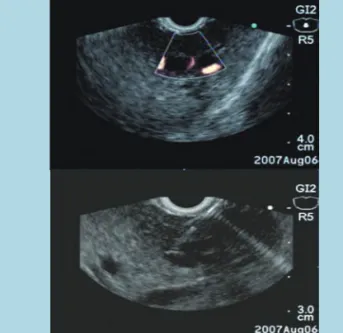
The CBD is visualized using a linear echoendoscope positioned in the duodenal bulb. Color doppler US is used to identify regional vascular anatomy. The dilated bile duct is punctured with a 19 gauge FNA needle. The puncture position is choosen based on EUS evaluation, above the tumor and distal to the duodenal bulb (Figures 1 and 2).
To confi rm successful biliary access, bile can be aspirated and iodine contrast injected under fl uoroscopy to demonstrate biliary opacifi cation (Figure 3).
A 0.035-inch guidewire is introduced through the EUS needle, using fl uoroscopy, and attempts to pass the wire through the papilla to the duodenum are made. When this maneuver has
no success, the needle is withdrawn and a wire-guided needle knife is used to perform a puncture in the duodenal wall.
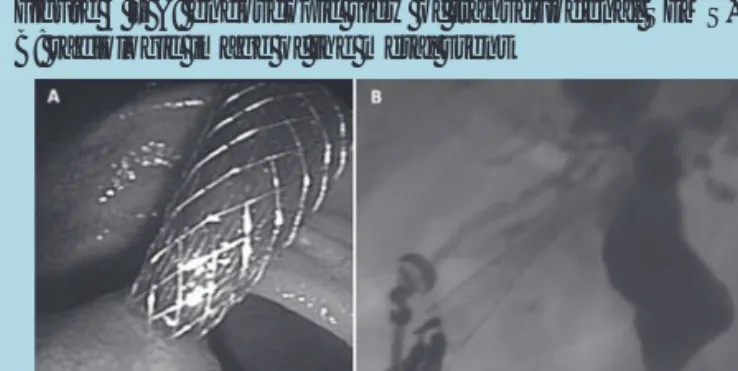
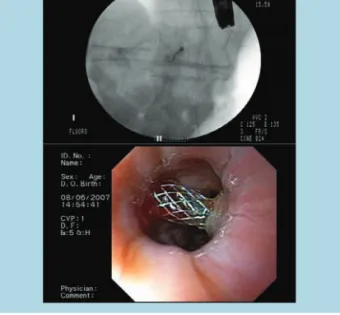
A partially covered self-expandable metallic stent (C SEMS) is passed over the guide, through the choledochoduodenal fi stula, without any dilatation procedure (Figure 4).
Duodenal bulb invasion is a limitation of EUS-guided choledocoduodenostomy, because it can diffi cult the CBD visualization and the tumoral growth can obstruct the stent. In these cases, EUS-guided hepaticogastrostomy can be done,
E. L. A. ARTIFON, F. FERREIRA, A. BORDINI, C. RABELLO, J. TAKADA, P. SAKAI
GED gastroenterol. endosc.dig. 2011: 30(2):37-41
Figure 1 – EUS linear image demonstrating CDB dilatation
Figure 2 – EUS linear image demonstrating CBD puncture
Figure 3 – EUS-guided cholangiography
Figure 4 – A: endoscopic view of transduodenal SEMS, B: radiologic image of the metal stent
30(2):37-41
Revista GED02 Abril2011.indd Sec1:39
Revista GED02 Abril2011.indd Sec1:39 5/19/11 6:28:55 PM5/19/11 6:28:55 PM
but dilation of the left biliary system is not always present, what can diffi cult the procedure. In some patients, visualization of the CBD from the antrum can allow an alternative of a choledochoantrostomy (Figure 5).
This modifi cation of the EUS-guided biliary drainage has been fi rst performed by our group in a case of unresectable pancreatic cancer with biliary obstruction and extensive duodenal invasion. It seems to be technically easier to perform and more physiological than a hepaticogastrostomy. This case has already been submitted for publication.
E
US-G
UIDEDH
EPATICOGASTROSTOMY Giovannini et al., in 2003, described the fi rst EUS-guided hepaticogastrostomy, in a patient with proximal metastatic biliary obstruction14. Other authors have also reported successful outcomes of this technique in which an anastomosis is created between the dilated left intrahepatic biliary system and the cardia or the lesser curve of the stomach15,16. Artifon et al. and Bories et al., in 2007, described the successful use of partially covered metallic stent in EUS-guided hepaticogastrostomy2. This modifi cation seems to reduce complication rates. This procedure has technical success rate of 90% to 100% and clinical success rate of 75% to 100%. Complications are rare, and include stent migration, bile leaks and cholangitis8. A fatal complication has been described by Martins et al., in 2010, after migration of the hepaticogastrostomy stent17.The procedure is performed using a linear array EUS, placed against the cardia or lesser curve of the stomach.
EUS is performed to evaluate for a dilated left intrahepatic biliary system. Vascular anatomy is shown by the power or
color Doppler. Then, a dilated peripheral branch of the left intrahepatic system, that is closest to the EUS transducer, is accessed by using a 19 gauge needle (Figure 6).
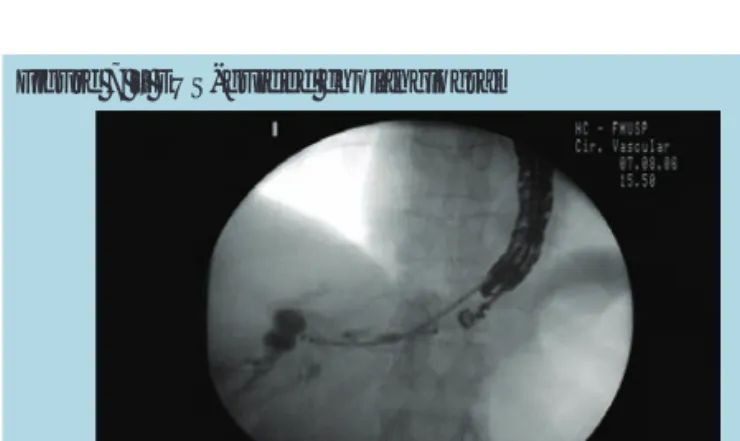
To confi rm successful biliary access, bile can be aspirated and iodine contrast injected under fl uoroscopy to demonstrate biliary opacifi cation (Figure 7).
A 0.035-inch guidewire is introduced through the EUS needle, using fl uoroscopy, and attempts to pass the wire through the native papilla to the duodenum are made. When this maneuver has no success, the needle is withdrawn and a wire-guided needle knife is used to perform the fi stula between the left intrahepatic branch and the stomach. A partially covered self-expandable metallic stent (PC-SEMS) is passed over the guide, through the hepatogastric fi stula, without any dilatation procedure (Figure 8).
Figure 7 – EUS-guided cholangiogram
EUS-GUIDEDBILIARYDRAINAGE: A LATIN AMERICANEXPERIENCE
30(2):37-41
GED gastroenterol. endosc.dig. 2011: 30(2):37-41
Figure 5 – A: endoscopic view of the PC-SEMS (*) and the duodenal SEMS (**) in the antrum/B: radiologic image of the choledocoantrostomy metal stent (*) and the duodenal metal stent (**)
Figure 6 – A: EUS image demonstrating dilated left biliary branch/B: EUS image demonstrating puncture of a left biliary branch (intrahepatic approach)
40
Revista GED02 Abril2011.indd Sec1:40
Revista GED02 Abril2011.indd Sec1:40 5/19/11 6:28:59 PM5/19/11 6:28:59 PM
A L
ATINA
MERICANE
XPERIENCE 41EUS-guided biliary drainage has been done in Sao Paulo Medical School since early 2007, in strict study protocols.
We present here our experience in a single tertiary referral Institution from june 2007 until march 2010. Nowadays, clinical studies in EUS-guided biliary drainage, approved by ethical committees, are in progress, with remarkable results.
We recommend that this method should be made by very experienced endosonographers and in defi ned protocols.
Final results will be shown in future publications. However, our current experience at a public Institution is demonstrated in Table 1.
The short follow-up (1 week) seen in Table 1 is only to demonstrate the immediate improvement jaundice. However, several patients of our protocols already have months of monitoring. Complications, life quality and survival are aims of these studies.
We had just one drainage failure in the EUS-guided hepatogastrostomy group. This patient was sent to PTBD. We would inform the readers that the above cases demonstrated only the patients performed in a protocol at University of Sao Paulo and it was not included the total of patients made by the endosonographer with expertise in the technique (ELAA) in a private Institution in which the procedure is made as well from 2006.
C
ONCLUSIONEUS-guided biliary drainage is an effective and minimally invasive option for malignant biliary obstruction, after ERCP
failure. It is feasible, but it is technically challenging and requires experienced endosonographer, profi cient in ERCP.
Standardization of the procedural technique and development of new specifi c devices are important to improve success and safety rates. EUS biliary drainage is suitable in those patients with advanced pancreatic cancer, presenting diffi cult cannulation or duodenal invasion of the second portion. Finally, clinical trials comparing the different types of EUS-guided biliary drainage and the PTBD and surgery are imperative.
R
EFERENCESAng TL, Teo EK, Fock KM. EUS-guided transduodenal biliary drainage in 1.
unresectable pancreatic cancer with obstructive jaundice. JOP. 2007 Jul 9;8(4):438-43.
Artifon EL, Chaves DM, Ishioka S, Souza TF, Matuguma SE, Sakai P. Echoguided 2.
hepatico-gastrostomy: a case report. Clinics (Sao Paulo). 2007 Dec;62(6):799- 802.
Burmester E, Niehaus J, Leineweber T, Huetteroth T. EUS-cholangio-drainage of 3.
the bile duct: report of 4 cases. Gastrointest Endosc. 2003 Feb;57(2):246-51.
Kahaleh M, Hernandez AJ, Tokar J, Adams RB, Shami VM, Yeaton P.
4.
Interventional EUS-guided cholangiography: evaluation of a technique in evolution. Gastrointest Endosc. 2006 Jul;64(1):52-9.
Wiersema MJ, Sandusky D, Carr R, Wiersema LM, Erdel WC, Frederick PK.
5.
Endosonography-guided cholangiopancreatography. Gastrointest Endosc.
1996 Feb;43(2 Pt 1):102-6.
Irisawa A, Hikichi T, Shibukawa G, Takagi T, et al. Pancreatobiliary drainage using 6.
the EUS-FNA technique: EUS-BD and EUS-PD. J Hepatobiliary Pancreat Surg.
2009;16(5):598-604.
Itoi T, Yamao K; EUS 2008 Working Group. EUS 2008 Working Group document:
7.
evaluation of EUS-guided choledochoduodenostomy (with video). Gastrointest Endosc. 2009 Feb;69(2 Suppl):S8-12.
Savides TJ, Varadarajulu S, Palazzo L; EUS 2008 Working Group. EUS 2008 8.
Working Group document: evaluation of EUS-guided hepaticogastrostomy.
Gastrointest Endosc. 2009 Feb;69(2 Suppl):S3-7.
Ashida R, Chang KJ. Interventional EUS for the treatment of pancreatic cancer.
9.
J Hepatobiliary Pancreat Surg. 2009;16(5):592-7.
Yamao K, Sawaki A, Takahashi K, Imaoka H, Ashida R, Mizuno N. EUS-guided 10.
choledochoduodenostomy for palliative biliary drainage in case of papillary obstruction: report of 2 cases. Gastrointest Endosc. 2006 Oct;64(4):663-7.
Mallery S, Matlock J, Freeman ML. EUS-guided rendezvous drainage of 11.
obstructed biliary and pancreatic ducts: report of 6 cases. Gastrointest Endosc 2004; 59: 100–107.
Kim YS, Gupta K, Mallery S, Li R, Kinney T, Freeman ML. Endoscopic ultrasound 12.
rendezvous for bile duct access using a transduodenal approach: cumulative experience at a single center. A case series. Endoscopy. 2010 Jun;42(6):496- 502.
Giovannini M, Moutardier V, Pesenti C, Bories E, Lelong B, Delpero JR.
13.
Endoscopic ultrasound-guided bilioduodenal anastomosis: a new technique for biliary drainage. Endoscopy. 2001 Oct;33(10):898-900.
Giovannini M, Dotti M, Bories E, Moutardier V, Pesenti C, Danisi C, Delpero JR.
14.
Hepaticogastrostomy by echo-endoscopy as a palliative treatment in a patient with metastatic biliary obstruction. Endoscopy. 2003 Dec;35(12):1076-8.
Bories E, Pesenti C, Caillol F, Lopes C, Giovannini M. Transgastric endoscopic 15.
ultrasonography-guided biliary drainage: results of a pilot study. Endoscopy.
2007 Apr;39(4):287-91.
Will U, Thieme A, Fueldner F, Gerlach R, Wanzar I, Meyer F. Treatment of biliary 16.
obstruction in selected patients by endoscopic ultrasonography (EUS)-guided transluminal biliary drainage. Endoscopy. 2007 Apr;39(4):292-5.
Martins FP, Rossini LG, Ferrari AP. Migration of a covered metallic stent following 17.
endoscopic ultrasound-guided hepaticogastrostomy: fatal complication.
Endoscopy. 2010;42 Suppl 2:E126-7.
Figure 8 – A: radiologic image of the PC-SEMS/
B: endoscopic view of the metallic stent in the cardia
30(2):37-41
GED gastroenterol. endosc.dig. 2011: 30(2):37-41
E. L. A. ARTIFON, F. FERREIRA, A. BORDINI, C. RABELLO, J. TAKADA, P. SAKAI
Revista GED02 Abril2011.indd Sec1:41
Revista GED02 Abril2011.indd Sec1:41 5/19/11 6:29:12 PM5/19/11 6:29:12 PM