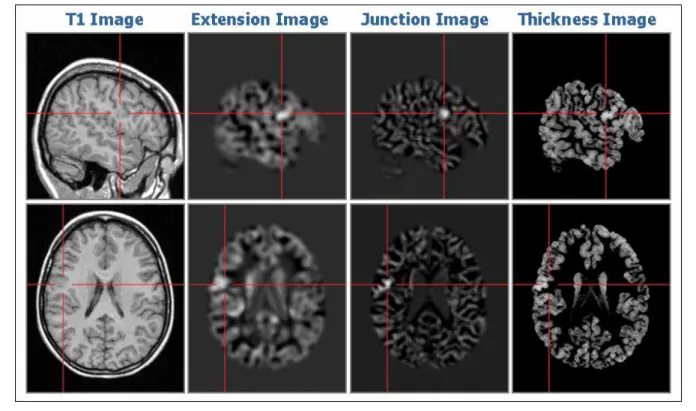
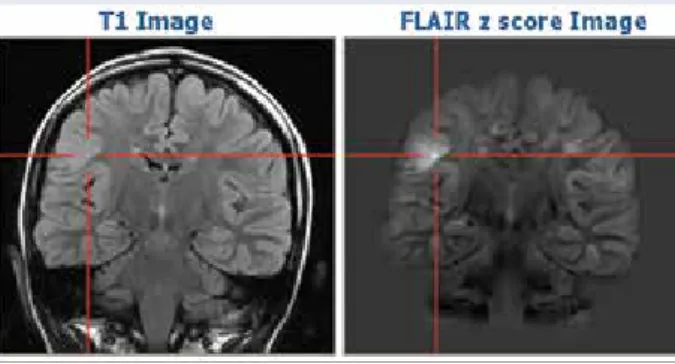
An overview of the different approaches can be found in the review by Bernasconi and colleagues in 2011 [21]. In our sample patient, quantitative FLAIR analysis revealed a subtle hyperintensity at the site of the suspected dysplasia that had been overlooked in the original FLAIR images (Figure 2). The remaining inner part of the brain can then be represented three-dimensionally by volume rendering (Figure 4).
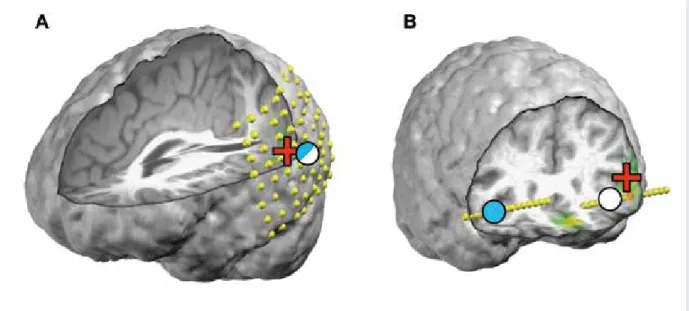
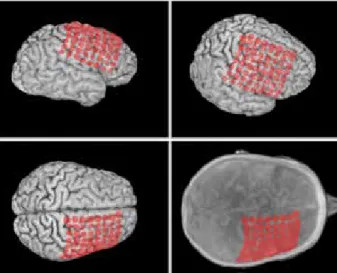
Planar MR slices often present problems with respect to electrode localization due to the convexity of the cortical surface. 3-dimensional rendering of the cortical surface requires computer removal of the skull in the MRI data. Invasive EEG monitoring confirmed the onset of habitual seizures over and in the vicinity of the suspected dysplastic lesion.
Clinical Application of Language and Memory fMRI in Epilepsy
In patients with medically refractory TLE, anterior temporal lobe resection (ATLR) is an effective and safe treatment option, leading to seizure freedom in up to 60–70% of these patients [ 5 , 6 ]. After temporal lobe surgery of the language-dominant hemisphere, a decline in verbal memory can more often be observed [27], while TL surgery in the non-dominant hemisphere is more likely to result in visual-spatial memory decline [28]. Material-specific lateralization of memory encoding in the medial temporal lobe: blocked versus event-related design.
Use of preoperative functional MRI to predict verbal amnesia after temporal lobe epilepsy surgery.
Nuclear Medicine Imaging in Epilepsy
- SPECT Perfusion Studies in Ictal and Interictal State
- FDG PET Imaging in Epilepsy
- Research PET Tracers
- Serotonin system
- Dopamine system
- Glutamate / NMDA system
- Nicotinic cholinergic system
- Adenosine system (A 1 adenosine receptor) Adenosine is different from regular transmitters: it
- Opioid system
- Markers of inflammation
- Technological developments: PET/MRI
Today, FDG PET remains a routinely used examination in the presurgical evaluation of drug-resistant focal epilepsies [11]. FDG PET has a generally established role in the presurgical evaluation of various types of epilepsy for diagnostic and prognostic evaluation [17–19]. Thus, one of the most promising applications of PET in the study of epilepsy is imaging the distribution of these molecular targets in the interictal state.
In a study of 20 patients with intractable partial epilepsy of neocortical origin and non-localizing MRI, a focal reduction of FMZ cortical binding in the lobe of seizure onset was found in 85% of patients [26]. Absorption was also reduced in the putamen, bilaterally in patients with generalized seizures and unilaterally, ipsilateral to hippocampal sclerosis, in patients with focal seizures. Compared to controls, [18F]-Fallypride binding potential in the epileptogenic temporal lobe was significantly reduced in all patients.
Although hippocampal FDG uptake (-8%) and hippocampal MR volume (-35%) were significantly reduced, no significant reduction in [18F]-Fallypride binding potential was found in the hippocampal region. In patients with autosomal dominant nocturnal frontal lobe epilepsy (ADNFLE) and an established nicotinic receptor mutation (in the α4 subunit) they showed reduced binding in the right putamen (increased extracellular dopamine levels or down-regulation of receptors) [56]. Defective dopamine uptake has been observed in the midbrain in patients with juvenile myoclonic epilepsy [57, 58] and in the putamen only in patients with generalized tonic-clonic seizures [57].
A PET study using [18F]-CPFPX in a patient with glioma also revealed increased adenosine A1 receptor density in the immediate vicinity of the tumor. In the first case, including unilateral hippocampal sclerosis, there was a reduction of the hippocampal [18F]-CPFPX signal on the sclerotic side. Thus, this study confirmed changes in opioid receptor availability in the hours following seizures, suggesting an important role of the opioid system in seizure control.
These techniques are most useful in the evaluation of patients with drug-resistant focal seizures who are potential candidates for epilepsy surgery.
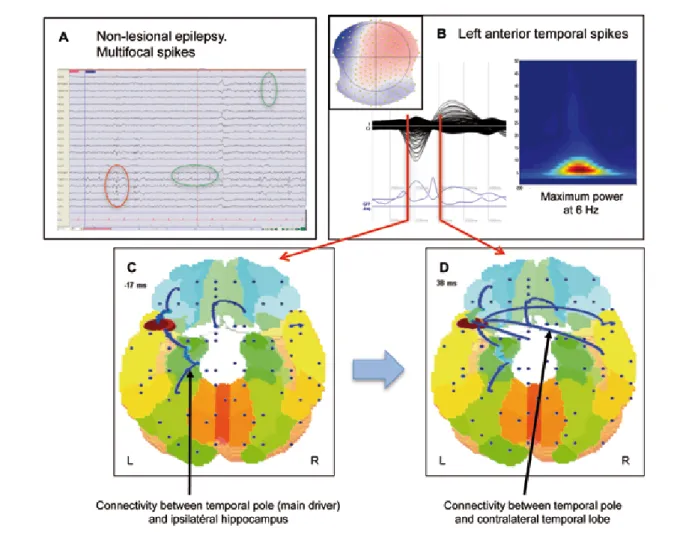
Electric and Magnetic Source Imaging of Epileptic Activity
In addition, EEG and magnetoencephalography (MEG) can be used to image functional brain activity with millisecond resolution. Electromagnetic source imaging should be part of the presurgical evaluation of all patients considering epilepsy surgery. Why is it actually difficult to localize the neural generators of EEG signals recorded on the surface of the head (this inverse problem).
After all, EEG produces squiggly lines (at least for the uninitiated), not pictures of the brain. Moreover, dipole localization is artificial in the "center of mass" of the region it represents. At the EEG and Epilepsy Unit of Geneva University Hospitals, we systematically perform high-density EEG recordings as part of the non-invasive evaluation of adult and pediatric patients being considered for epilepsy surgery.
A distributed inverse solution (Local AUtoRegressive Average, LAURA; [21]) is used to locate the source of the surface tension field. Findings of a positive association between the inclusion of the ESI or MSI result in the resection and seizure freedom ([37]; see also suggest that the results of ESI or MSI should be taken into account when determining strategy for resective surgery. In in this case, consideration of the electroclinical pattern and other imaging tools strongly suggests that the peak recorded for ESI is not representative of seizure onset and the epileptogenic zone.
However, ESI and MSI still lie on the fringes of the curriculum of clinical neurophysiology residents or EEG technicians. Identification of the epileptogenic tuber in patients with tuberous sclerosis: a comparison of high-resolution EEG and MEG.
Neuroimaging of Temporal Lobe Epilepsy: Lesions and Networks
Postfach 1084
Epilepsie-Preise
Epilepsie-Liga-Mitteilungen
Sie absolvierten das erste Jahr Ihres Medizinstudiums in Zürich, zogen dann nach Freiburg und schlossen Ihr Studium schliesslich 1974 in Lausanne mit einem Doktorat ab. Ab 1985 übernahmen Sie auch einen kleineren Bereich für Neurorehabilitation in Lavigny, wiederum vorwiegend als Kooperationsprojekt mit der Abteilung für Neurologie des CHUV. Anschließend spezialisierte sie sich auf Neurologie und arbeitete am Universitätsspital Zürich bei Professor G.
Dumermuth an der Universitäts-Kinderklinik Zürich und bei Professor Scollo-Lavizzari am Universitätsspital Basel. Fernando Lopes da Silva wurde in Portugal geboren und studierte Medizin in Lissabon. Anschließend arbeitete er in London auf dem Gebiet der Physiologie und anschließend in Utrecht auf dem Gebiet der Neurophysiologie. Mise au concours – Soutien de la Recherche Förderung der wissenschaftlichen Forschung auf dem Gebiet der Epilepsie (surtout sous forme d'aide initial) par la Ligue Suisse contre l'Epilepsie (Ligue contre l'Epilepsie).
La Ligue contre l'épilepsie soutient des projets scientifiques dans le domaine de l'épileptologie avec un montant total de. La Ligue suisse contre l'épilepsie (Ligue contre l'épilepsie) décerne un prix d'une valeur de . Le jury qui décerne le prix est composé de trois membres du comité directeur de la Ligue contre l'épilepsie.
Le prix est toujours décerné l'année suivante dans le cadre de l'assemblée annuelle ou générale de la Ligue contre l'épilepsie. Les candidatures doivent parvenir au secrétariat de la Ligue contre l'épilepsie (Seefeldstrasse 84, CarPostal Zurich).
Informations de la Ligue contre l’Epilepsie
Au nom de l'ensemble du comité de pilotage, des différentes commissions, du personnel du secrétariat général et, bien sûr, de nos membres, je tiens à vous remercier pour l'engagement exceptionnel et inlassable dont vous faites preuve depuis des décennies dans - l'accompagnement des personnes atteintes d'épilepsie et de la Ligue suisse contre l'épilepsie. C'est d'abord en votre qualité de chef de service puis, à partir de 1990, de directeur médical de l'établissement Lavigny, que vous avez été membre du comité exécutif de la Ligue à partir de mars 1982, avant de quitter également ce dernier comme les différents comités, à la fin 2011, ainsi que votre démission des postes de direction alors confiés au Dr. méd. Vous avez passé la première année de vos études à Zurich avant de vous rendre d'abord à Fribourg puis de compléter votre formation universitaire en obtenant votre doctorat à Lausanne en 1974.
Mais parce que la psychothérapie n'était pas « ta tasse de thé », tu as choisi de dé-. Lors de votre formation spécialisée avancée à Zurich, Fribourg, Rome et Lausanne, notre ancien président, Paul André Despland, a été votre mentor à Lausanne. Pendant les années que vous avez passées à Lavigny, vous avez toujours assuré une collaboration étroite avec le service de neurologie du CHUV (y compris en tant que médecin assistant), vous avez contribué à une trentaine de publications et rédigé un mémoire pour le Master d'éducation.
À partir de 1985, vous avez également pris en charge un petit service de neuroréhabilitation à Lavigny, également en grande partie un projet collaboratif avec le service de neurologie du CHUV. Bien qu'intégré dans cette structure, le service d'épilepsie est indépendant d'un point de vue médical, ce qui garantit la poursuite de la mission historique de l'établissement Lavigny pour l'avenir. Comment ne pas mentionner également que depuis de nombreuses années, dans le cadre de leur formation en neurologie et épileptologie sur le territoire suisse, vous avez guidé un grand nombre de confrères qui, grâce à votre expérience, tant professionnelle qu'humaine, sont devenus de meilleurs médecins.
Là aussi, tous ceux qui travaillaient avec vous voyaient en vous un partenaire solide et fiable, et vous étiez un acteur clé très apprécié du Centre commun de l'épilepsie de Genève et de Lausanne, lorsque vous, avec tout le personnel concerné, suiviez les patients avant et après après le traitement résecteur. chirurgie ou stimulation cérébrale profonde de l'hippocampe. Concernant ce dernier, vous faites donc partie de "l'avant-garde" - non seulement parmi les épileptologues suisses, mais aussi à l'échelle internationale.
Kongresskalender
Kongress der Deutschen Gesellschaft für Neurologie
Konzeption | Design | Reinzeichnung screenblue Büro für Design | Birgit Depping Gazellekamp 99, D-22529 Hamburg bd@screenblue.de, www.screenblue.de Beleuchtung | Beschäftigt. 67. Jahrestagung der American Epilepsy Society Informationen: American Epilepsy Society, 342 North Main Street, West Hartford, CT USA, Tel.

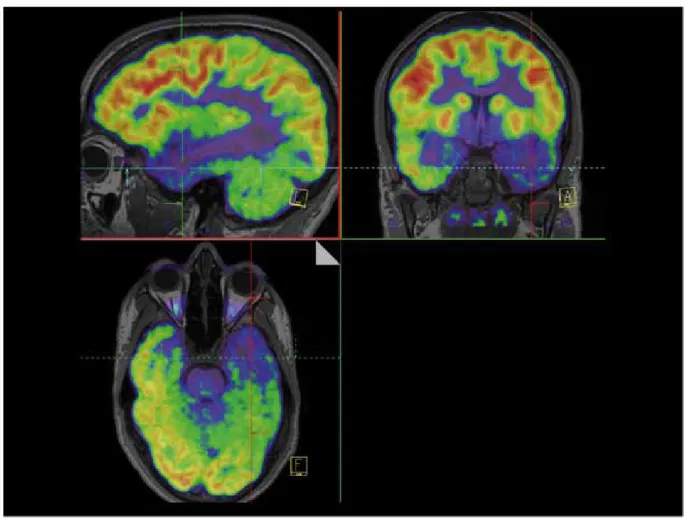
![Figure 3: [ 18 F]-FDG PET and [ 18 F]-MPPF PET in a patient with a temporo-limbic epilepsy and normal MRI: the images show a slight decrease in FDG uptake and a clear and severe MPPF binding reduction located within the left temporal region](https://thumb-eu.123doks.com/thumbv2/pubpdfco/325747.41430/31.892.90.794.85.600/figure-patient-temporo-epilepsy-decrease-binding-reduction-temporal.webp)