The program was aimed at the economic empowerment of the participants through a special curriculum —"Build your life"— and in the field of health through another curriculum —"Protect your life"—. Contrary to our expectations, we did not find that any of the interventions reduced fertility. All girls in class IV in these schools were invited to participate in the project, and we initially interviewed 3,483 girls.
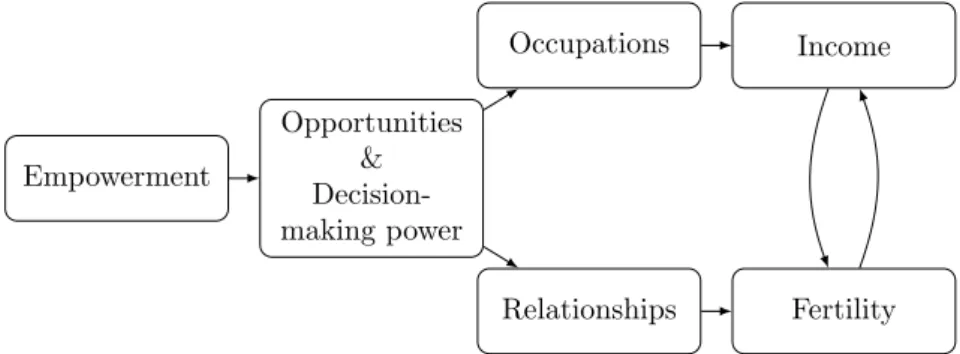
The goal of the interventions was to empower girls by expanding their opportunities and strengthening their decision-making power in the economic and reproductive health fields. To strengthen the external validity and scalability of the programs, they were implemented by local teachers in schools. Participants attended an average of 6.88 sessions in health treatment and 6.65 sessions in economic treatment.
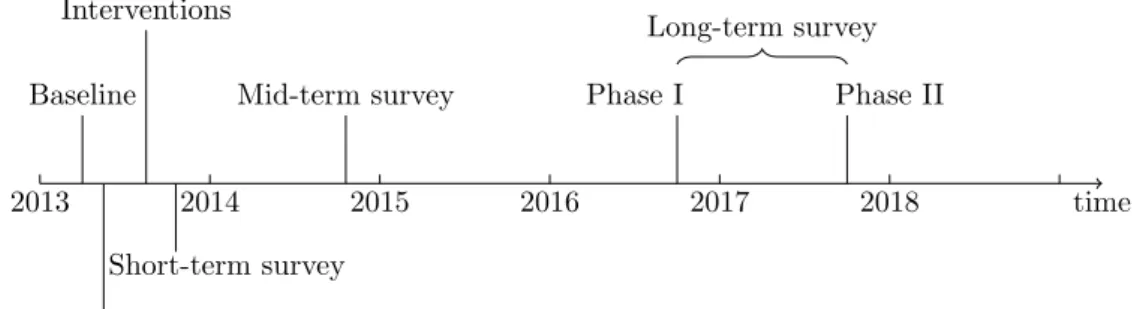
The baseline survey was conducted in the spring of 2013, and the interventions were introduced in August and September 2013. As the vast majority of girls were expected to drop out of school, we interviewed them by phone.
Empirical approach
In the second phase, we sent teams of enumerators to meet the subjects in person for a face-to-face interview and to take pregnancy, syphilis and malaria tests. By the end of 2016, we had managed to interview 88 percent of the baseline sample on the phone and 72 percent in person. To further reduce the attrition rate, we organized a second phase in autumn 2017 to find and meet the participants we missed in 2016.
We interviewed 394 participants in this second phase, bringing the follow-up rate to face-to-face interviews to 83 percent. As we show in Appendix A, attrition rates across surveys do not differ significantly by treatment arm. Xij is a vector of covariates predetermined by the baseline determined at the individual or school level.
According to our first hypothesis about the direct effect of the programs, we expect β1 to be positive for economic outcomes and β2 to be positive for health outcomes. If β1 is also positive for health outcomes and β2 is positive for economic outcomes, then this would be evidence in favor of the second hypothesis, namely the indirect effect of treatment.
Results
Main results
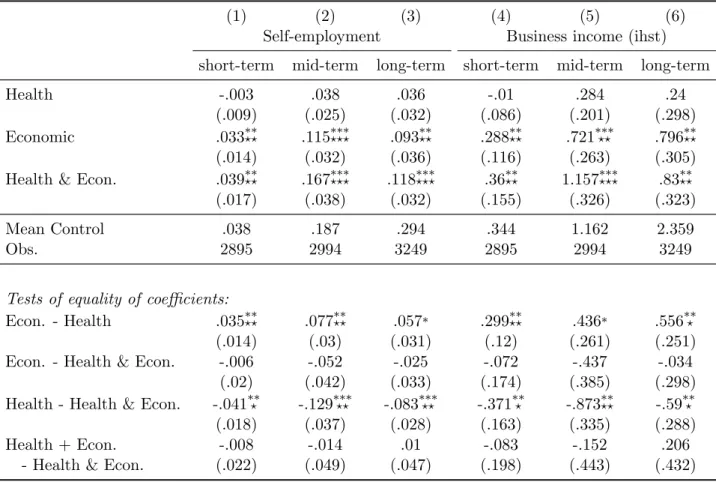
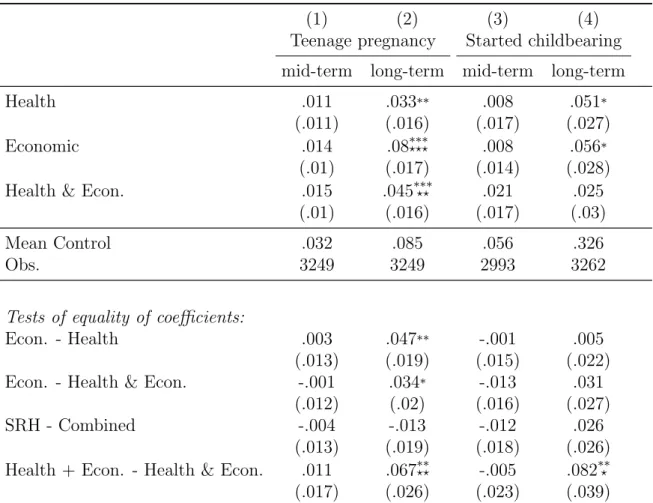
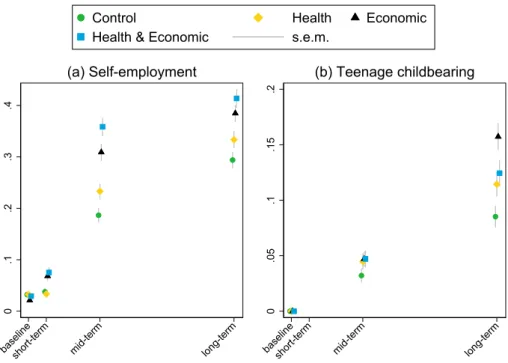
We note that the economic empowerment program has had a tremendous impact on business creation and revenue. Interestingly, the strongest treatment effect on teenage pregnancy comes from the economic empowerment program, where a long-term study shows almost a doubling compared to the control group. In summary, we find evidence for a direct effect of the health intervention on fertility, as well as an indirect effect on fertility from the economic empowerment arm.
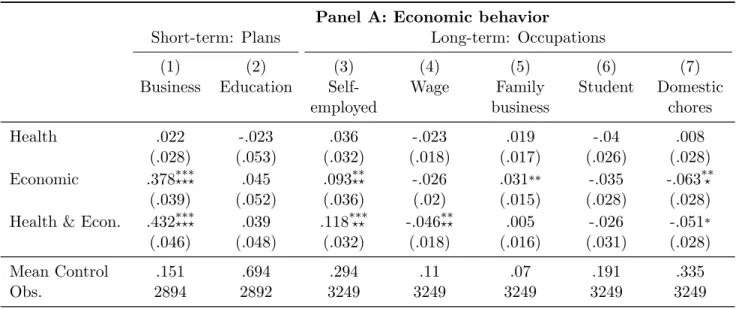
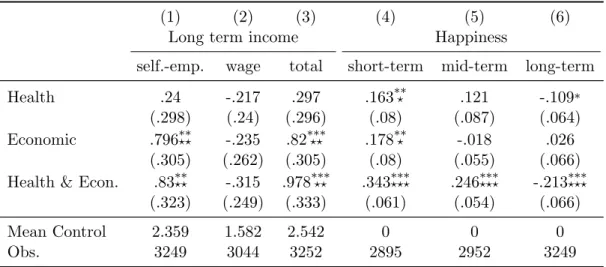
The table shows OLS treatment effect estimates (“Health,” “Economic,” and “Health & Econ.”), tests of equality of effects between branches (“Econ.. Health & Econ.” and “Health - Health & Econ.”), and a test of complementarity between the Health and Economic empowerment programs (“Health + Econ.- Health & Econ.”). Statistically significant differences between scores and zero are indicated by ∗ p <0.1,∗∗p <0.05,∗ ∗ ∗p <0.01 when p-values are uncorrected and z. The table shows OLS treatment effect estimates (“Health”, “Economic” and “Health .. amp; Econ.”), tests of equality of effects between arms (“Econ.
Economy." and “Health - Health & Economy.”), and a test of complementarity between the Health and Economic empowerment programs (“Health + Economy.- Health & Economy.”). Statistically significant differences between the estimates and zero are indicated by ∗p <0.1, ∗∗p <0.05,∗ ∗ ∗p <0.01 when the p-values are uncorrected and by.
Mechanisms
While only the impact of the economic program goes in the same direction, its coefficient is not statistically different from zero. It is noted that the health program, alone or combined, also leads to a decrease in acceptance of wife beating, but without effect from the economic program. 6. We do not find general treatment effects on willingness to compete.7. 6 These short-term effects are consistent with the findings of Dhar et al. 2020), in our case they nevertheless dissipate over time and disappear in the long run.
Given the changes we see in short-term opportunity and decision-making power, we can expect the programs to impact economic and health behavior in the medium and long term. The economic program, alone or in combination, has led to a substantial increase in the proportion of participants who want to become entrepreneurs and later become entrepreneurs: an increase of ten percentage points compared to a control group average of 29 percent. We see that the girls at age 25 express a desire to get married and have their first child at age 26, which is consistent with what we found at baseline, six months earlier, and we find no treatment effect on these aspirations.
Importantly, the health program, alone or combined, leads to a significant increase in medium-term stable relationships. Healthy relationships are between two people who are honest and straightforward with each other.” The fact that we do find a medium-term effect on stable relationships, while the effect on having children occurs later, as shown in Table 3, suggests that the relationship causes the pregnancy rather than the other way around. In the long term, 75.4 percent of girls have a stable relationship and the positive treatment effect has virtually disappeared.
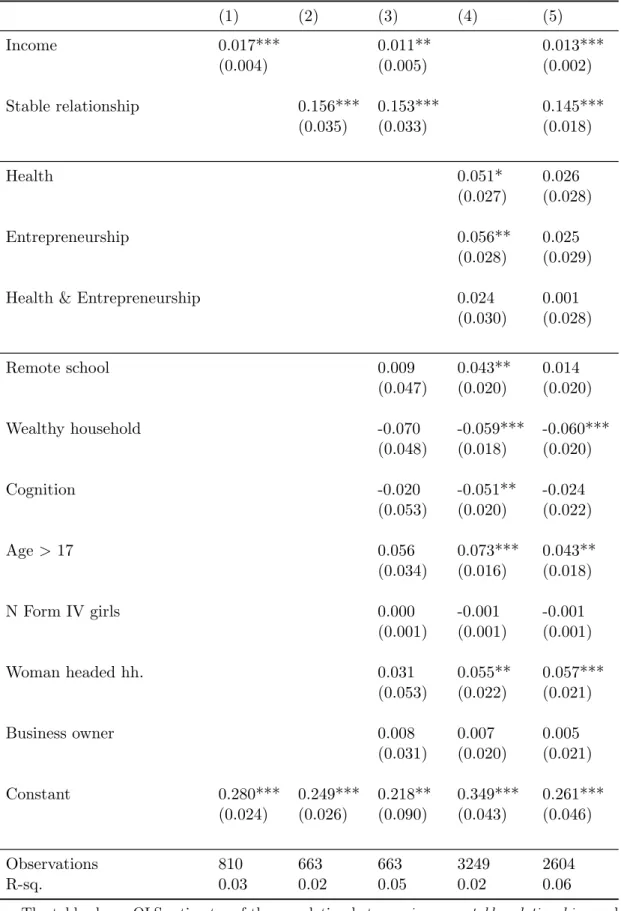
We have observed that there is a causal effect of the economic empowerment program on income, and a causal effect of the health program on stable relationships. We note that the economic and health empowerment coefficients are reduced and lose their statistical significance when we introduce income and stable correlation into the model. Considering only those who do not have a child yet, 44 percent would be happy to have one, 37 percent think their parents would be happy, and 45 percent say they would get more respect.9.
In the group that already has a child, 24 percent would be happy to have another child next year, 26 percent think their parents would be happy, and 32 percent say they would get more respect. Among those who are in a steady relationship and earn their own income, 54 percent would be happy to have a child in the coming year. The table shows OLS estimates of the correlation between having an income, stable relationships, childbearing, and whether the respondent would be happy to have a child, whether she thinks her parents would be happy, and whether she thinks people would treat her with more respect.
Well-being
The table shows the OLS estimates of the treatment effects ("Health," "Economic," and . "Health and the Economy."). Second, happiness levels adjust to a new reference level after a positive shock and return to normal in the long run (Galiani et al., 2018). However, this theory of hedonic adaptations is not a sufficient explanation as happiness levels not only converge but are significantly lower among those assigned to the health intervention.
Third, the health program creates aspirations that are not fulfilled when girls leave school, leading to frustration (Genicot and Ray. In particular, we know that the health program led to an increase in girls' sense of self-control in the short term, but from our data we also see that this positive effect completely disappears in the long term. Therefore, aspirations can be an important motivator for change (Dalton et al.; Bernard et al., 2019), there is a risk of "overshooting" so that aspirations actually become harmful and La Ferrara (2019).
This interpretation is also supported by the fact that we observe very strong negative correlations, at the individual level, between happiness in the long term and in the past.
Conclusion
More power to the pill: The impact of contraceptive freedom on women's life cycle labor supply. An Economic Analysis of Fertility, in: Roberts, G.B. Ed.), Demographic and economic changes in developed countries. The half-life of happiness: Hedonic adaptation to the subjective well-being of poor slum dwellers for meeting basic housing needs.
Can they explain the negative fertility-income relationship?, in: Shoven, J.B. Ed.), Demography and the Economy.
Attrition
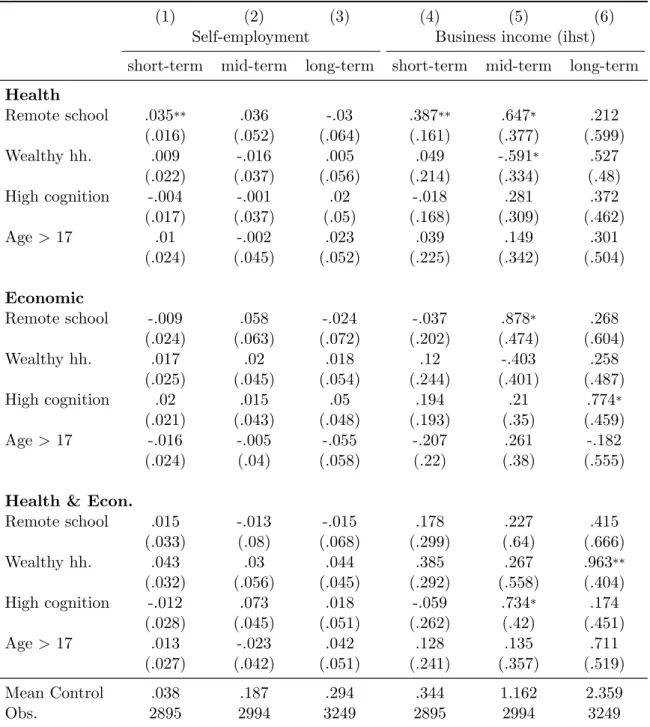
Heterogeneity analysis
Self-employment Business income (ihst) short-term medium-term long-term Health short-term medium-term. The table shows OLS estimates of the interaction between treatment assignment and the baseline variable of interest. Short Term: Plans Stable Relationship Number of Condoms Unwanted Marriage First Child Medium Long Term Partners Use Sex Health.
Multiple hypothesis testing
To illustrate, in Table 2 we first group the 18 p-values corresponding to columns (1) to (6) (first group of results) and the rows "Health", "Economic" and. Health and Economics." (our first question), and we apply the procedure of Benjamini and Hochberg (1995) to these 18 p-values. We then group the six p-values corresponding to columns (1) through (6) and the row "Health + Econ. third question) and adjust these six p-values.
Then we collect the 18 p-values corresponding to the columns (1) to (6) and the rows “Econ.
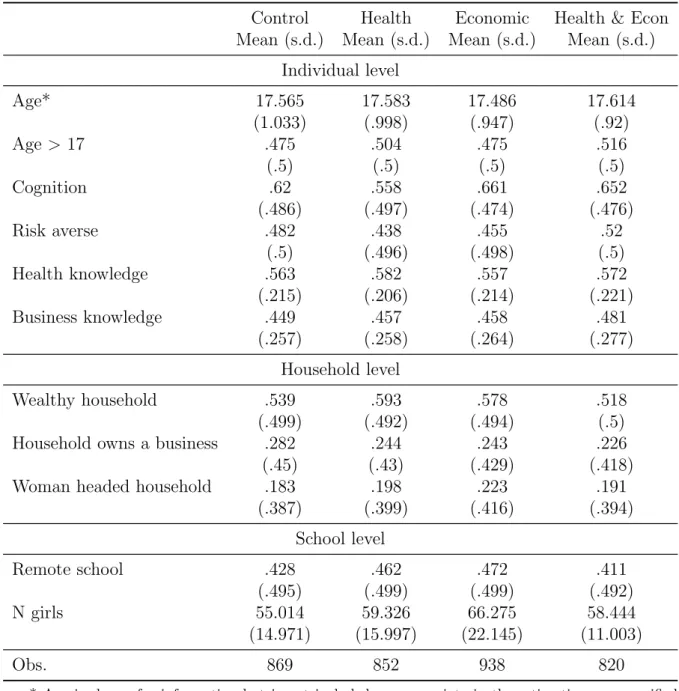
Variables
Map of the study sites
Curriculum
Pre-analysis plans