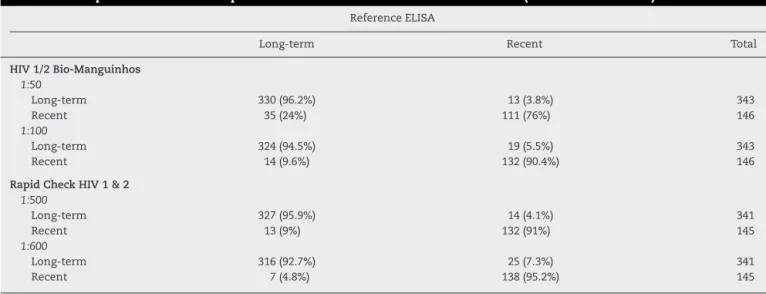
Evaluation of rapid tests for human immunodeficiency virus as a tool to detect recent seroconversion
Texto
Imagem
Documentos relacionados
OBJETIVO Atendendo à diversidade de fontes de variabilidade na atividade muscular, do elevado número de variáveis associadas à atividade muscular e do registo de
Medidas educativas quanto à necessidade de treino específico também são importantes entre indivíduos que praticam a dança sem intuito profissional, visto que força
FIELD EVALUATION OF THE WHOLE BLOOD IMMUNOCHROMATOGRAPHIC TEST FOR RAPID BANCROFTIAN FILARIASIS DIAGNOSIS IN THE NORTHEAST OF BRAZIL.. Cynthia BRAGA(1), Maria Inês DOURADO(2),
Objective: The main objective of this study is to evaluate the comparability of the results of rapid tests (RT) used for the HIV diagnosis in relation to conventional molecular
To assess the prevalence of primary resistance of human immunodeficiency virus type 1 (HIV-1) to antiretrovirals, 84 patients chronically infected with HIV without prior
The analysis of genetic data for human immunodeficiency virus type 1 (HIV-1) and human T-cell lymphotropic virus type 1 (HTLV-1) is essential to improve treatment and public
A rapid method for simultaneous detection of phenotypic resistance to inhibitors of protease and reverse tran- scriptase in recombinant human immunodeficiency virus type 1 isolates
With the Auger Engineering Radio Array (AERA) of the Pierre Auger Observatory, we have observed the radio emission from 561 extensive air showers with zenith angles between 60 ◦ and
