w w w . r b o . o r g . b r
Original
Article
Results
evaluation
of
the
use
of
intra-articular
sodium
hyaluronate
in
the
post-operative
knee
arthroscopy
夽
,
夽夽
Ayrton
de
Paula
Pereira
Junior
a,
Ricardo
Pozzi
Fasolin
a,
Felipe
Ayusso
Correa
Sossa
a,
Ozorio
de
Almeida
Lira
Neto
b,
Marcelo
Schmidt
Navarro
c,
Antonio
Milani
a,b,∗ aDepartamentodeOrtopedia,HospitalIfor,SãoBernardodoCampo,SP,BrazilbDepartamentodeOrtopediaeTraumatologia,UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil cDisciplinadeOrtopedia,FaculdadedeMedicinadoABC,SantoAndré,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received3September2012 Accepted7December2012
Keywords: Arthroscopy Knee
Hyaluronicacid Viscosuplementation
a
b
s
t
r
a
c
t
Objective:to evaluate the efficacy of hyaluronic acid in the post-operative of knee arthroscopy.
Methods:wehaveevaluated49patientsundergoingarthroscopicprocedurewiththeuseof intra-articularhyaluronicacid(Group1)and49patientsundergoingarthroscopicprocedure withouttheuseofhyaluronicacid(Group2).PatientswereevaluatedbasedontheVisual AnalogueScale,householdanalgesia,assessmentoftheRangeofMotionwithagoniometer, andtheLysholmquestionnaire.
Results:therewerenosubstantialadverseeffectsoneithergroup.
Conclusion: theuseofhyaluronicacidinthepost-operativeofkneearthroscopyisjustified due/becauseitleadstoadecreaseinpainintheearlystage,enablingfasterrecoveryofthe patient.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Avaliac¸ão
dos
resultados
do
uso
do
hialuronato
de
sódio
intra-articular
no
pós-operatório
da
artroscopia
do
joelho
Palavras-chave: Artroscopia Joelho
Ácidohialurônico Viscossuplementac¸ão
r
e
s
u
m
o
Objetivo:avaliaraeficáciadousodoácidohialurôniconopós-operatóriodeartroscopiade joelho.
Métodos:foramavaliados49pacientessubmetidosaoprocedimentoartroscópico associ-ado aousodoácidohialurônico intra-articular(GrupoI) e49 pacientessubmetidosao procedimentoartroscópicosemusodoácido hialurônico(GrupoII).Ospacientesforam avaliadoscombasenaEscalaVisualAnalógicadedor(EVA),analgesiadomiciliar,amplitude domovimentodojoelhocomgoniômetroenoquestionárioLysholm.
Resultados: nãoocorreramefeitosadversossignificativosemnenhumdosdoisgrupos.
夽
Pleasecitethisarticleas:dePaulaPereiraJuniorA,FasolinRP,SossaFAC,deAlmeidaLiraNetoO,NavarroMS,MilaniA.Avaliac¸ãodos resultadosdousodohialuronatodesódiointra-articularnopós-operatóriodaartroscopiadojoelho.RevBrasOrtop.2014;49:37–43.
夽夽
StudyconductedattheHospitalIfor,SãoBernardodoCampo,SP,Brazil.
∗ Correspondingauthor.
E-mail:pilot@osite.com.br(A.Milani).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Conclusão:ousodoácidohialurôniconopós-operatóriodeartroscopiadejoelhoéjustificado porlevaraumadiminuic¸ãodadornafaseinicialepossibilitarumarecuperac¸ãomaisrápida dopaciente.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Theuseofintra-articularmedicationintheimmediate post-operativeperiodintheareaofarthroscopickneesurgeriesis controversial,withprospectsfornewbehaviorsandroutines, andwithauthorsforandagainsttheuseofhyaluronicacid post-operatively.1,2
A knee arthroscopy is a medicalprocedure moreusual inthe UnitedStates ofAmerica (USA), and iseffective for symptomreliefinpatientswithintra-articularloosebodies, chondralinjuryandmeniscalpathology.2
Theperformanceofhumanjointsisstrictlyrelatedtothe viscoelasticpropertiesofsynovialfluid,whichdeterminesthe strengthtransmission,lubricationandprotectionofarticular cartilage.Thisviscoelasticitydependsontheconcentrationof hyaluronicacidinthesinovialfluid.3
Other actions of hyaluronic acid would be an anti-inflammatoryeffect(decreasedgeneexpressionofcytokines, prostaglandinproduction,andintra-articularconcentrationof metalloproteinases)andanalgesic(inhibitionofnociceptors), stabilization ofcartilaginous matrix,chondrocyte prolifera-tion,increasedproductionoftypeIIcollagenanditsdecreased degradation.4–6
Someauthorsbelievethatexogenoushyaluronicacidalso stimulates the production of endogenous hyaluronic acid, whichwouldexplainitslong-termeffect.7Withrespecttothe
analgesiceffectofintra-articularhyaluronicacid,itisbelieved that,initially,itwouldbesmallerthantheintra-articular cor-ticosteroidinjection,butwithpersistenceforlongerperiods.8
Anothersourceofdebateisthediscussionregardingthe numberofdosesofhyaluronicacidtobeeffective,butthere wasnodifferenceinthecomparisonbetweenthreeandsix dosesatweeklyintervals.9
Some authors claim that, during an arthroscopic knee surgery,adecreaseinintra-articularhyaluronicacid concen-trationmay occur and,as immediatetherapy, recommend intra-articular applications of sodium hyaluronate 20mg after surgery, and subsequently four injections at weekly intervals.10
Theaimofthisstudywastocomparetheresultsoftheuse ofintra-articularsodiumhyaluronateinagroupofpatients undergoingarthroscopicsurgeryduetomeniscallesions ver-susresultsobservedinagroupofpatientsnottreatedbythis complementarytherapy.
Materials
and
methods
Ninety-eight patients with meniscal lesions were studied. ThesepatientsweretreatedfromMarchtoNovember2005by arthroscopicsurgerywithpartialmeniscectomyofthemedial meniscus,alwaysbythesamesurgicalteam.
Their agesrangedfrom 18to65 years(mean:34 years). Sixty-five(63%)weremenand33(37%),women.
Theparticipantswererandomlydividedintotwogroups of49.Thefirstgroupwastreatedwithintra-articularsodium hyaluronate20mg(Polireumim, TRBPharma) inthe imme-diatepost-operativeperiodand,subsequently,withaweekly applicationforfourconsecutiveweeks.Inthesecondgroup, thistreatmentwasnotdone.Thesurgeonwasunawareofthe grouptowhicheachpatientbelonged,havingbeeninformed onlyafterskinsuture,atthetimeofcompletion(ornot)ofthe infiltration(Table1).
Allpatientswererehabilitatedaccordingtothesame pro-tocol,withevaluationsafterthree,eight,15,30and60days, andwereinstructedtoreturntosportpracticeafter60daysof surgery.
Allpatientsunderwentthesamesurgicaltechnique,with theuseofonlytwoinfrapatellarportals(medialandlateral) and,onaverage,withjointinfusion(6Lofsaline0.9%),using aninfusionpumpatameanpressureof50mmHg.All ran-domizedpatientsshowednosignificantchangesincartilage and,inthis study,onlycasesofOuterbridgegradeIand II chondropathy(Table1)wereincluded.
Allpatientswereanesthetizedbysubarachnoidblockwith bupivacaine0.5%associatedwithglucose12.5to15mg, with-outopioids.Apneumatictourniquetwasalsoused,withan averagetimeof35min.
Afterhospitaldischarge(mean:12haftertheintervention), bothgroupsweretreatedwithcephalexin500mgPO6/6hfor sevendaysand,incaseofpain,dipyrone50dropstothelimit of6/6h.Theuseofanalgesicswascontrolledinaform,in whichthepatienthadtocheckthedateandtimeofuseuntil theeighthday.
InGroup1,afterskinsuturetheinfiltrationsweremadein thelateralsuprapatellararea,(onceaweekforfour consec-utiveweeks).Besidesthecontrolontheformwiththedate andtimeofuseofanalgesics,patientsunderwentVAS.Inall reviews,therangeofmotionofthekneewasalsomeasured witha goniometer;theLysholm questionnairewasapplied inthepreoperatoryonthe dayofsurgeryandonthe 15th, 30thand60thdayspost-operatively.Allevaluationswere per-formedbythe sameexaminerwho didnotknowatwhich groupthepatientbelonged.
Toavoidbiasintheresultsbecause ofthepainof infil-tration,theassessmentsinthe8th,15thand30thdayswere alwaysmadebeforethisprocedure.
Inthestatisticalanalysis,analysisofvariancewithtwo fac-torsand repeatedmeasuresonthetimefactorwere made, assuming a first-order autoregressive correlation matrix betweentimepoints.11Aftertheanalysis,Tukeymultiple
com-parisonsweremade12toseebetweenwhichgroupsortime
pointsoccurreddifferencesinscales.
Table1–Characterizationofsample.
Variables n=98 Group1=49 Group2=49
Age(years)–mean(SD) 34(12.1) 36(11.3) 33(12.1)
Minimum–maximum 18–65 20–65 18–61
Gender–n(%)
Female 33(37) 15(30.6) 18(36.7)
Male 65(63) 34(69.4) 31(63.3)
Operatedsite–n(%)
Right 58(59.2) 26(53) 32(65.3)
Left 40(40.8) 23(47) 17(34.7)
Chondrallesiona–n(%)
Withoutlesion 43(43.9) 22(44.9) 21(42.9)
GradeI 31(31.6) 14(28.6) 17(34.7)
GradeII 24(24.5) 13(26.5) 11(22.4)
a Outerbridge.
Results
ConsideringtheassessmentsbyVAS,theresultssuggestmore rapidreductionofpaininGroup1versusGroup2.Theanalysis showedthatthemeanbehaviorofVASwasstatistically differ-entbetweengroupsovertheevaluationtimepoints(p<0.001) (Fig.1).
Incomparingthedifferentevaluationtimepoints,thedata
inTable2showthatbothgroupshadameanreductioninVAS
withstatisticalsignificanceatallevaluationtimepoints,when comparedto the previous timepoint (p<0.001),but inthe eighthand15thdays,Group1showed,onaverage,statistically lowerVASversusGroup2(p<0.001andp<0.001)andinother timepoints,therewasnostatisticallysignificantdifferencein VASbetweengroups(p>0.05)(Table2).
Withrespecttotheneedforuseofhomeanalgesia,there was no statistical difference between the groups until the eighthday.
Withregardtoassessmentsmadewiththegoniometer,it wasobservedthatafter15daystheGroup1hadgreaterrange ofmotionversusGroup2.After30days,thisdifferencecould stillbeobserved,toalesserextent,butwithoutstatistical sig-nificance.Intheassessmentmadeonthe60thday,theresults weresimilarinbothgroups.
0 1 2 3 4 5 6 7 8
0 10 20 30 40 50 60 70
Dia
VAS
Groups 1 Groups 2
Fig.1–Graphicalrepresentationofthemeanprofilesand respectivestandarderrorsofVAS,accordingtogroups.
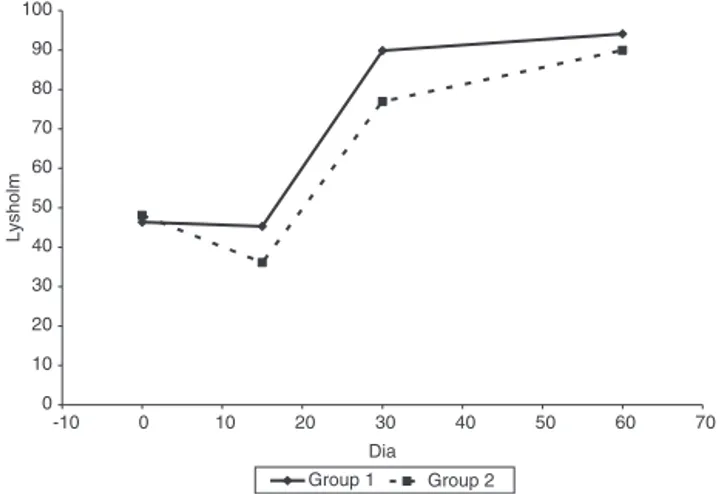
IntheevaluationwiththeLysholmquestionnaire (excel-lent:patientsbetween95and100points,good:94–84;regular: 83–65,andpoorscore:<64),wenotedinthepreoperativethat theGroups1and2hadanaverageof46and48points, respec-tively,classifiedthenaspoor(Table3).
Table 3shows that inboth Groups(1 and 2), themean
Lysholmscoredecreasedstatisticallyfromthepreoperatoryto 15dayspost-operatively(p=0.003andp<0.001,respectively), with“poor”ratinginbothgroups.However,intheevaluation ofthequestions,wefoundthatthelargestdifferencebetween groupswasobservedintheitems “pain”and “swelling”,in whichtheGroup1hadbetterresultsversusGroup2.Inother questions,theresultsweresimilarbetweengroups.
Inthe30thdaytheresultsshowedthegreateststatistical differencebetweengroups.Group1averaged90points, clas-sifiedasgood,andGroup2averaged77points,classifiedas regular. Weperceived agreater difference inthe questions about claudication,instability, swelling and squatting, and noticedthat,justasthatinthe15thday,theswellingwasalso animportantfactor.
Atthelastevaluationperiod,60daysafterthesurgery,the twogroupsdifferedstatistically,with94pointsinGroup1and 90pointsinGroup2,bothclassifiedasgood.Inthisevaluation, werealizedthatthetwogroupsdifferedprimarilyintheitem “climbing stairs”,but withoutstatisticaldifferencebetween values.
IntheallocationoftheresultsoftheLysholmetal. ques-tionnaireonagraph,earlierimprovementoffunctioninGroup 1versusGroup2wasnotedinallassessments(p<0.001)(Fig.2). Inthisstudy,somecomplicationsoccurred:eightpatients inGroup1reportedaneedforanalgesiaafterinfiltration.Insix ofthesecases,twopatientsrequiredonlyonedoseofdipyrone 50drops,andintwoofthem,twodaysofdipyrone50drops 8/8hwererequired.
Noneofthepatientshadpost-operativeinfections,joint stiffness,orscarchanges.
Discussion
Table2–ResultofmultiplecomparisonsofVASamonggroupsandtimepoints.
Group/timepoint Comparison Meanestimated
difference
Standarderror tvalue gL p
Group1 3days–8days 3.86 0.10 38.60 384 <0.001
3days–15days 5.20 0.13 41.05 384 <0.001
3days–30days 6.22 0.14 44.25 384 <0.001
3days–60days 7.02 0.15 47.27 384 <0.001
8days–15days 1.35 0.10 13.48 384 <0.001
8days–30days 2.37 0.13 18.67 384 <0.001
8days–60days 3.16 0.14 22.49 384 <0.001
15days–30days 1.02 0.10 10.21 384 <0.001
15days–60days 1.82 0.13 14.33 384 <0.001
30days–60days 0.80 0.10 7.97 384 <0.001
Group2 3days–8days 2.27 0.10 22.67 384 <0.001
3days–15days 4.33 0.13 34.12 384 <0.001
3days–30days 6.37 0.14 45.26 384 <0.001
3days–60days 7.06 0.15 47.55 384 <0.001
8days–15days 2.06 0.10 20.63 384 <0.001
8days–30days 4.10 0.13 32.35 384 <0.001
8days–60days 4.80 0.14 34.09 384 <0.001
15days–30days 2.04 0.10 20.42 384 <0.001
15days–60days 2.73 0.13 21.57 384 <0.001
30days–60days 0.69 0.10 6.94 384 <0.001
3days Group1–Group2 −0.10 0.16 −0.64 384 >0.999
8days Group1–Group2 −1.69 0.16 −10.59 384 <0.001
15days Group1–Group2 −0.98 0.16 −6.12 384 <0.001
30days Group1–Group2 0.04 0.16 0.26 384 >0.999
60days Group1–Group2 −0.06 0.16 −0.38 384 >0.999
matrixandispresentinhighconcentrationsincartilageand synovialfluid.10
Some authors claimthat sodium hyaluronate, which is a defined fraction of hyaluronic acid, has analgesic and anti-inflammatoryproperties,contributestothe normaliza-tion of fluidity or viscoelasticity of the synovial fluid and totheactivation oftissueregenerationintheaffected car-tilage, and restores the functional balance of the joint. Therefore, they recommend its use for the treatment of osteoarthritis.4,13,14
Somestudieshavereportedthat,inadditiontorelieving painandimprovingfunction,theuseofhyaluronicacidcould
alterthecourseofosteoarthrosisandimprove qualitatively and quantitativelythearticularcartilage.Theseindications are based on studies of imaging such as X-ray and MRI, in which therewas an increase incartilage volume and a decrease injoint space afterthe treatment versus placebo. Thesebenefitsarealsobasedonthebestqualityofthematrix andonahigherdensityofchondrocytesinbiopsystudiesafter theimplementationoftreatment.4
Inanimalstudies,Plaasetal.15concludedthathyaluronic
acid suppresses synovialhyperplasia and the development ofperiarticularfibrosis,andprotectagainstcartilageerosion, andalsoactstorelievepainintheshortterm(dilutionofjoint
Table3–ResultofmultiplecomparisonsofLysholmquestionnaireamonggroupsandtimepoints.
Group/timepoint Comparison Meanestimated
difference
Standarderror tvalue gL p
Group1 Pre–15days 1.10 0.28 3.92 288 0.003
Pre–30days −43.47 0.33 −133.55 288 <0.001
Pre–60days −47.76 0.34 −140.79 288 <0.001
15days–30days −44.57 0.28 −158.49 288 <0.001
15days–60days −48.86 0.33 −150.11 288 <0.001
30days–60days −4.29 0.28 −15.24 288 <0.001
Group2 Pre–15days 12.02 0.28 42.74 288 <0.001
Pre–30days −28.88 0.33 −88.72 288 <0.001
Pre–60days −41.84 0.34 −123.34 288 <0.001
15days–30days −40.90 0.28 −145.43 288 <0.001
15days–60days −53.86 0.33 −165.47 288 <0.001
30days–60days −12.96 0.28 −46.08 288 <0.001
Pre Group1–Group2 −1.73 0.35 −5.01 288 <0.001
15days Group1–Group2 9.18 0.35 26.54 288 <0.001
30days Group1–Group2 12.86 0.35 37.16 288 <0.001
0 10 20 30 40 50 60 70 80 90 100
-10 0 10 20 30 40 50 60 70
Dia
Lysholm
Group 1 Group 2
Fig.2–Graphicalrepresentationofthemeanprofilesand respectivestandarderrorsofLysholmquestionnaire, accordingtogroups.
fluid)andinthelongterm(blockingofpainreceptors),and improvethegaitpatternoftheosteoarthrosisknee.
Currently,theuseofintra-articularhyaluronicacidisalso widelydiscussedbecauseofthedifferentformulations,with differentmolecular weightsand theresultsofsome meta-analyses.Thesestudiesalsodifferintheparameterusedand furtherincreasethediscussionastotheeffectivenessofits use.16
Huanget al.,13inarandomized,double-blind,
multicen-terstudy,evaluatedinonesampleofthe Asianpopulation theuseofintra-articularhyaluronicacidversusplacebo.These authorsfoundstatisticallysignificantimprovementin reduc-ingthepainandinthekneefunction,especiallyafterthefifth weekoftreatment.Thesebenefitshaveremainedeffectivefor upto25weeks.Inthesubjectiveevaluation,favorableresults withitsusealsowerenoted.Regardingtheconsumptionof acetaminophenandthevolumeofjointfluid,therewasno statisticallysignificantdifferenceforanygroup.11
Theseresultsare consistentwiththe study by Navarro-Sarabiaetal.,17inwhichtherewasastatisticallysignificant
difference in favor of hyaluronic acid in the categories of painrelief,improvedfunctionandoverallimprovementofthe patientversusplacebo.
Bannuruetal.,14inameta-analysiscomparativeoftheuse
ofintra-articularhyaluronic acidversus placebo, concluded thathyaluronicacidiseffectiveasearlyasthefourthweek oftreatment, with peak effectiveness at eight weeks, and remainingbeneficialforupto24weeks.Theseauthors eval-uatedtheeffectivenessforpainrelief,improvedfunctionand decreasedjointstiffness.
Leeetal.18believethattheanalgesiceffectofhyaluronic
acid in the first five weeksis equal tothat ofplacebo. In their prospective and randomized study, the authors con-cludedthattheuse ofcetorolac associatedwithhyaluronic acidshowedmorerapidanalgesiaversusmonotherapywith hyaluronic acid. In the fifth week this analgesia achieved equalintensityinbothgroups(hyaluronicacidwith cetoro-lac×hyaluronicacidalone).
Butit isworthbearinginmindthattheaforementioned studies evaluate the hyaluronic acid in the treatment of
osteoarthrosis;hence,itisinterestingtoquotethem,because they discuss the efficacy ofhyaluronicacid as ameans of improvingfunctionandpain.
Regardingtheuseofhyaluronicacidinthepost-operative ofarthroscopy,ForsterandStraw19comparedpainand
func-tion in activities of daily living in patients with isolated arthroscopy versus arthroscopy associated with hyaluronic acid.Theseauthorsconcludedthattherewasimprovement offunctionwiththeuseofHA,butwithoutdifferenceinthe categoryofpain.
Heybeli et al.1 compared pain and function in patients
with 40–65yearsold with mildtomoderate osteoarthrosis and whounderwent arthroscopywithand withoutthe use ofhyaluronicacid(HA)post-operatively.Therewasno statis-ticallysignificant differencewithrespecttopain,but there wasimprovementinfunctioninpatientswhousedHA.Inour study,weobservedthesameresultwithrespecttofunction improvement,mainlyuntilthe30thday,bothbytheLysholm questionnaireandbythegoniometermensuration.However, withregardtopain,untilthethirddaytheresultsconfirmthe literature,withnodifferencewiththeuseofthemedication inquestion;thereafter,patientstreatedwithhyaluronicacid hadlesspainversuscontrolgroup,andthisanalgesiaachieved equalintensityinthe30thday-evaluationandfromthenon.
Hempfling10 also contrasted isolated arthroscopy versus
arthroscopyassociatedwithHAinthe itemsofnightpain, pain when walking, and ability to walk 100 meters with-out pain. A clear symptomatic improvement occurred in bothgroups,comparedwithpreoperativevalues;butinthe group using HA this improvement lasted longer. In our study, therewas alsosignificant improvementin pain and function versus preoperative assessments, but this differ-ence wasobservedintheinitialevaluations.Afterthe60th day,animportantdifferencebetweentheratingsofGroups 1 and 2 was not observed, which can be justified by the lack ofassessmentof patientsover a longer period, when maybe we could observe results equivalent to the litera-ture.
In2007,Ulucayet al.20comparedtheuse ofthreetypes
of HA in women40–60 years old with mild osteoarthrosis and degenerative meniscal lesion,after arthroscopy. These authors concluded that HA is effective therapy for these patients.
Alsoin2008,Atay etal.21 comparedthe effectofHAof
high and lowmolecular weight versus placebo interms of pain,stiffnessandfunctionalabilityatsixand12monthsafter arthroscopicdebridementinpatientswithmildtomoderate osteoarthrosis. Aftersix months,there was nostatistically significantdifference,butthisoccurredafter12months.The authorsconcludedthattheuseofHAresultsbeneficialand improves the effectivenessof treatment, regardless of the substance’shighorlowmolecularweight.Inourstudy,pain improvement wasobserved untilthe 15th day, withbetter rangeofmotionandfunctionalcapacityuntilthe30thday. There was nostatistical differencefor theitems evaluated fromthe60thday.
Waddell andBert,2 inasystematicreviewconductedin
decreasepainandimprovethefunctionofasignificant num-berofpatientspost-operatively.Inourstudy,theimprovement ofpain,function,andrangeofmotioninpatientswhowere treatedwithHAinfiltrationwasobserved.Theimprovement ofpainisobserved intheinitialstage, especiallyuntilthe 15thday;ontheotherhand,thefunctionandrangeofmotion improvedafterthisperiod.Webelieveinadirectrelationwith thiseffect:withlesspain,thepatientcanachieveafaster reha-bilitation,withmorequality,besidesafasterreturntohis/her dailyfunctions.
When interpreting more deeply the Lysholm question-naire,ourresultsdemonstrated,intheinitialevaluation,that although both groups were classified as poor, the superi-ority of the patients in Group 1 was justifiedby the best assessmentsin relation topain and swelling.This finding corroboratestheresultsofVASandcanbeexplainedbythe analgesic and anti-inflammatory effect of hyaluronic acid.
4,13,14
Inthe30thdayevaluation,wefoundthegreatestdifference betweenGroups1and2:90and77points,respectively.The maindifferencesareintheitem“swelling”,againbecausethe anti-inflammatoryeffectofHA.Asof“claudication”, “instabil-ity”and“squatting”,webelievethat,bythistime,withamore effectivetherapy and because ofalower intensity ofpain, itispossiblethatthepatientbesubmittedtomoreintense demands and achieve an earlier gain ofmuscle mass and proprioception.Thiswouldfacilitatetheactivitiesabove eval-uated.Fromthe 30th,the painwassimilarinbothgroups, andintheassessmentofthe60thdaybothgroupswere clas-sifiedasgood,withstatisticalsuperiorityinGroup1versus Group2(94×90,respectively).Thissuperioritywasduetothe
improvedabilitytoclimbstairsbyGroupHApatients,likely duetothebettermusclereservesacquired inthe initial60 days.
Conclusion
Giventhesubjective parametersevaluated, webelievethat theuseofintra-articularinfiltrationsofsodiumhyaluronate 20mgin proceduresof arthroscopicsurgery ofthe knee is fullyjustified,asthispracticeleadstoadecreaseinpainin theinitialphase,enablesfasterpatientrecoveryand gener-atesafasterreturnandbetterqualitytotheactivitiesofdaily living.
Ourstudyhassomelimitations:theshortperiodof eval-uation ofpatients (wewere unable toverify the effects of hyaluronicacidinthemediumandlongterm),andalsothe factofthesubjectivityoftheevaluationofpatients’function. Thisimpliesthatperhapsanisokineticevaluationwithcybex couldbetterdemonstrateamuscledifferencesbetweenthe twogroupsofindividuals.Webelievethatthis isthemain causeofimprovementofthefunctiononthe60thday. Unfor-tunately,wecould notproceedwiththis optionforlackof money.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HeybeliN,DoralMN,AtayOA,LeblebiciogluG,UzumcugilA.
Intra-articularsodiumhyaluronateinjectionsafter
arthroscopicdebridementforosteoarthritisoftheknee:a
prospective,randomized,controlledstudy.ActaOrthop
TraumatolTurc.2008;42(4):221–7.
2.WaddellDD,BertJM.Theuseofhyaluronanafterarthroscopic
surgeryoftheknee.Arthroscopy.2010;26(1):105–11.
3.CarulliC,MatassiF,CivininiR,MorfiniM,TaniM,Innocenti
M.Intra-articularinjectionsofhyaluronicacidinduce
positiveclinicaleffectsinkneesofpatientsaffectedby
haemophilicarthropathy.Knee.2013;20(1):36–9.
4.RezendeMU,CamposGC.Viscossuplementac¸ão.RevBras
Ortop.2012;47(2):160–4.
5.ConrozierT,JeroschJ,BeksP,KemperF,Euller-ZieglerL,
BailleulF,etal.Prospective,multi-centre,randomized
evaluationofthesafetyandefficacyoffivedosingregimens
ofviscosupplementationwithhylanG-F20inpatientswith
symptomatictibio-femoralosteoarthritis:apilotstudy.Arch
OrthopTraumaSurg.2009;129(3):417–23.
6.PavelkaK,UebelhartD.Efficacyevaluationofhighlypurified
intra-articularhyaluronicacid(Sinovial®)hylanG-F20
(Synvisc®)inthetreatmentofsymptomaticknee
osteoarthritis.Adouble-blind,controlled,randomized,
parallel-groupnon-inferioritystudy.OsteoarthritisCartil.
2011;19(11):1294–300.
7.BaggaH,BurkhardtD,SambrookP,MarchL.Longtermeffects
ofintraarticularhyaluronanonsynovialfluidinosteoarthritis
oftheknee.JRheumatol.2006;33(5):946–50.
8.ClarkeS,LockV,DuddyJ,SharifM,NewmanJH,KirwanJR.
Intra-articularhylanG-F(Synvisc®)inthemanagementof
patellofemoralosteoarthritisoftheknee(POAK).Knee.
2005;12(1):57–62.
9.PetrellaR,PetrellaM.Aprospective,randomized,
double-blind,placebocontrolledstudytoevaluatethe
efficacyofintraarticularhyaluronicacidforosteoarthritisof
theknee.JRheumatol.2006;33(5):951–6.
10.HempflingH.Intra-articularhyaluronicacidafterknee
arthroscopy:atwo-yearstudy.KneeSurgSportsTraumatol
Arthrosc.2007;15(5):537–46.
11.SingerJM,AndradeDF.Analysisoflongitudinaldata.In:Sen
PK,RaoCR,editors.Handbookofstatistics:
bio-environmentalandpublichealthstatistics.Amsterdam:
NorthHolland;2000.p.115–60.
12.NeterJ,KutnerMH,NachtsheimCJ,WassermanW.Applied
linearstatisticalmodels.4thed.Illinois:RichardD.Irwing;
1996.
13.HuangTL,ChangCC,LeeCH,ChenSC,LaiCH,TsaiCL.
Intra-articularinjectionsofsodiumhyaluronate(Hyalgan®)in
osteoarthritisoftheknee.Arandomized,controlled,
double-blind,multicentertrialintheAsianpopulation.BMC
MusculoskeletDisord.2011;12:221–8.
14.BannuruRR,NatovNS,DasiUR,SchmidCH,McAlindonTE.
Therapeutictrajectoryfollowingintra-articularhyaluronic
acidinjectioninkneeosteoarthritis–meta-analysis.
OsteoarthritisCartil.2011;19(6):611–9.
15.PlaasA,LiJ,RiescoJ,DasR,SandyJD,HarrisonA.
Intraarticularinjectionofhyaluronanpreventscartilage
erosion,periarticularfibrosis,andmechanicalallodyniaand
normalizesstancetimeinmurinekneeosteoarthritis.
ArthritisResTher.2011;13(2):R46.
16.CurranMP.Hyaluronicacid(Supartz®).Areviewofitsusein
osteoarthritisoftheknee.DrugsAging.2010;27(11):925–41.
17.Navarro-SarabiaF,CoronelP,CollantesE,NavarroFJ,DeLa
SernaAR,NaranjoA,etal.A40-monthmulticentre,
andcarry-overeffectofrepeatedintra-articularinjectionsof
hyaluronicacidinkneeosteoarthritis:theAMELIAproject.
AnnRheumDis.2011;70(11):1957–62.
18.LeeSC,RhaDW,ChangWH.Rapidanalgesiconsetof
intra-articularhyaluronicacidwithketorolacinosteoarthritis
oftheknee.JBackMusculoskeletRehabil.2011;24(1):31–8.
19.ForsterMC,StrawR.Aprospectiverandomizedtrial
comparingintra-articularHyalganinjectionandarthroscopic
washoutforkneeosteoarthritis.Knee.2003;10(3):291–3.
20.UlucayC,AltintasF,UgutmenE,BeksacB.Theuseof
arthroscopicdebridementandviscosupplementationinknee
osteoarthritis.ActaOrthopTraumatolTurc.2007;41(5):
337–42.
21.AtayT,AslanA,BaydarML,CeylanB,BaykalB,KirdemirV.
Theefficacyoflow-andhigh-molecular-weighthyaluronic
acidapplicationsafterarthroscopicdebridementinpatients
withosteoarthritisoftheknee.ActaOrthopTraumatolTurc.