www.elsevier.es/ai
Allergologia
et
immunopathologia
SociedadEspa˜noladeInmunolog´ıaCl´ınica, Alergolog´ıayAsmaPedi´atrica
ORIGINAL
ARTICLE
Short
and
extended
provocation
tests
have
similar
negative
predictive
value
in
non-immediate
hypersensitivity
to
beta-lactams
in
children
F.S.
Regateiro
a,b,
I.
Rezende
c,
N.
Pinto
d,
C.
Abreu
c,
P.
Carreiro-Martins
d,e,
E.R.
Gomes
c,∗aServic¸odeImunoalergologia,CentroHospitalarUniversitáriodeCoimbra,Coimbra,Portugal bInstitutodeImunologia,FaculdadedeMedicina,UniversidadedeCoimbra,Coimbra,Portugal cServic¸odeImunoalergologia,CentroHospitalardoPorto,Porto,Portugal
dHospitaldeDonaEstefânia,CentroHospitalardeLisboaCentral,EPE,Lisbon,Portugal
eNovaMedicalSchool,CEDOC,IntegratedPathophysiologicalMechanismsResearchGroup,Lisbon,Portugal
Received11November2018;accepted4January2019 Availableonline23March2019
KEYWORDS Beta-lactams; Children; Drugprovocation test; Durationofdrug provocation; Negativepredictive value; Non-immediate hypersensitivity Abstract
Introductionandobjectives: Drugprovocationtests (DPTs) arethegold-standard method to diagnosenon-immediatehypersensitivityreactions(NIHSR)tobeta-lactam antibiotics(BL)in children.Ouraimwastocomparethenegativepredictivevalue(NPV)ofone-day(short)DPT versus3---7days(extended)DPTforthediagnosisofNIHSRtoBLinpaediatricage.Asecondary aimwastocompareconfidenceondrugre-exposureaftershortandextendednegativeDPTs.
Methods:TheoccurrenceofHSRondrugre-exposureanddrugrefusalafternegativediagnostic DPTswereevaluatedinchildren/adolescentswithahistoryofNIHSRtoBLusingaquestionnaire performedsixmonthstotenyearsafterDPT.Patientsweredividedintotwogroupsaccording totheprotocolperformed:shortDPTvs.extendedDPT.
Results:Weenrolled212childrenandadolescents(86females,126males,meanageatDPT 5.52years,p25=3years,p75=7.25years):69testedwithshortDPT,and143withextended DPT.TheNPVofbothtypesofDPTtogetherwas95.2%.TheNPVofshortDPTwas97.5%andthe NPVofextendedDPTwas93.8%(p=0.419).AfternegativeDPT,beta-lactamswererefusedby carersin14.75%ofthechildrenrequiringsubsequenttreatment,6.98%intheshortDPTgroup and18.99%intheextendedDPTgroup(p=0.074).
Abbreviations: NIHSR,non-immediatehypersensitivityreactions;BL,beta-lactamantibiotics;Amox/clav,amoxicillinandclavulanate; DPT,drugprovocationtest;HSR,hypersensitivityreaction;NPV,negativepredictivevalue;CHP,CentroHospitalardoPorto;HDE,Hospital D.Estefânia.
∗Correspondingauthor.
E-mailaddress:[email protected](E.R.Gomes).
https://doi.org/10.1016/j.aller.2019.01.004
Conclusions:Inourpaediatricsample,prolongingdrugadministrationdidnotincreasetheNPV ofdiagnosticDPTforNIHSRtoBLorreducedrugrefusal.Altogether,thedataherereported suggestthat,howeverintuitive,prolongingDPTisnotbeneficialintheparametersanalysed. ©2019SEICAP.PublishedbyElsevierEspa˜na,S.L.U.Allrightsreserved.
Introduction
Around10%of peopleavoid sometype ofmedication due tofearofallergicreactions.1 Suspicionofdrugallergyhas
agreatimpactinclinicalpractice.2However,onlyasmall
percentageofpatients areconfirmedtohave drugHSRin subsequentwork-up.Thisover-diagnosingisparticularly fre-quentamongchildren1,3---8andallergy‘‘mislabelling’’often
persistsintoadulthood.
In children, beta-lactam antibiotics (BL) are the most commonmedications suspected of being involved in drug HSRandcanmediateall‘GellandCoombs’typesofHSR.9
MostsuspectedHSRtoBLinchildrenaremildnon-immediate skin eruptions occurring in the context of treatment for infection.10,11 Viralinfections arethemostcommoncause
ofmaculopapularor urticarialeruptionsinchildren, lead-ing to frequent misdiagnosis of HSR to concurrent BL treatment.4,6,12
Itisgenerallyagreedthatdrugprovocationtests(DPT) with the culprit antibiotic are the ‘‘gold standard’’ for thediagnosisofnon-immediateHSRtoBL.13,14Clinical
his-torycriteriacannotaccuratelypredictBLallergy15whereas
blood allergy tests16 and other allergy in vivotests, such
asintradermal testingor patchtesting,have low sensitiv-ityin this clinical context7,8,10,12,17,18 andmay be difficult
toimplementinyoung children.Recentevidencesuggests that, after a careful clinical history, non-immediate mild cutaneouseruptionsin children shouldbe investigatedby ‘‘up-front’’DPTwith the culpritdrug,12,19---22 and such an
approachhasbeenincludedinsomeguidelines.23
The negative predictive value (NPV) of DPTs for non-immediateHRS toBL hasbeen reportedto beas high as 90---98%4,8,24withsomevariationattributabletodifferences
inthepopulationstestedandDPTprotocols.However,some patients do have HSR after negative DPT, and no current methodcan further identifywhich patients are at risk of HSRonre-exposure.SomeDPTmodificationswereproposed toimproveaccuracy,including:
1. Extended DPT protocols,17,24---27 as it has been argued
thatone-day(‘‘short’’)DPTprotocolsmightprovidean exposurethatistoosmalltoelicitafullnon-immediate HSR. It is alsowell knownthat, after a negative DPT, some patients, carers or attending physicians remain reluctant touse or prescribe thepreviously suspected medication.28Extendedprotocolswereproposedtoalso
increase patients/physicians’ confidence insubsequent useofthedrug.29
2. RetestingafterafirstnegativeDPTwiththeculpritdrug. However, recentevidence suggeststhat retesting adds littlediagnosticbenefit.30,31
DatadirectlycomparingshortDPTversusextendedDPT protocolsinthecontextofnon-immediateHSRinchildrenis scarce.TheprimaryaimofthisstudyistocomparetheNPV ofone-day(short)DPTversus3---7days(extended)DPT pro-tocolsforthediagnosisofnon-immediatecutaneousHSRto BLinpaediatricage.Asecondaryaimistocomparethe fre-quencyofdruguse(re-exposure)aftershortandextended negativeDPTs. We didnot intendto compare the perfor-manceofthetwoprotocolsintermsofdiagnosticsensitivity.
Methods
We retrospectively collected data from 212 children and adolescents with a negative diagnostic DPT performed between2007and2015aspartoftheinvestigationof non-immediatecutaneousHSRtoBLintwoHospitalsinPortugal (CentroHospitalardoPorto,CHP,inPorto,andHospitalDona Estefânia,HDE,inLisbon),andcompletedtelephone ques-tionnairestothecarersofthepatientsbetween 2015and 2017.
Drugprovocationtests
Allpatientstestedhadpreviouscutaneous,non-severe, non-immediate HSR toBL (defined asreactions that occurred morethan 1hourafter thepreviousdose intakeandwith characteristic manifestations of non-immediate hypersen-sitivity).Afterinformedconsentbytheparents/carers,the patientsweretested‘‘up-front’’(i.e.,withoutpreviousskin testing)usingoneoftwoDPTprotocolswiththeculpritdrug (diagnosticDPT):
1. ‘‘short’’ DPT--- one-day administration of an age- and weight-adjusted dose of the suspected drug according to ENDA guidelines (total dose was calculated taking into consideration the daily doses and administration intervals recommended to treat the infection present whenthesuspectedHSRoccurred).ThewholeDPT pro-tocolwasusuallyperformedinday-hospitalandthetotal dosewasdividedin2---4administrationswithintervalsof 30---60min,followedbyavigilanceperiodofatleast3h beforemedicaldischarge.Nofurtherdoseswere admin-isteredathome;
2. ‘‘extended’’ DPT --- the first day was identical to the ‘‘short’’DPTprotocolbutantibioticadministration con-tinued at home on the following days using standard doses‘‘aspertreatment’’untilthenumberofdosesthat reportedlytriggeredthereactionwasachieved.
The assignment toshort or extended DPT in CHP was chronological: from2007to2012 allchildren weretested withshortDPTsandafter2012allweretestedwithextended DPT.InHDE,theassignmenttoshortorextendedDPTwas random.
All patients included in this study had negative DPTs. DPTs were considered negativewhen nosymptoms devel-opedduring DPT or in the seven daysafter the last drug administration.AfteranegativeDPT,patients’parentsand carerswereexplainedtheresultandlimitationsoftheDPT andwereinstructedthatBLcouldbesafelyusedin subse-quentbacterialinfections.Awrittenreportwasprovidedto thepatientandtheassistantphysician.DrugHS‘‘labelling’’ and the Hospital’s informatics limitations to beta-lactam prescriptionwereremoved.
Re-exposurequestionnaire
Six monthstoten yearsafter negativeDPT, the carersof patients were contacted by telephone to obtain informa-tionregardingsubsequentuseofbeta-lactams.Astandard questionnairewiththefollowingquestionswascompleted:
1. AfterthenegativeDPT,wasthepatientadministeredthe testedbeta-lactamantibioticeveragain?
2. Iftheanswer toquestion 1waspositive, didthechild havemanifestationsofHSR?Ifso,whatwerethe mani-festations?
3. Ifthe answer toquestion 1 wasnegative (patientwas nevertreatedwithBLagain),whatwasthereason?Were BLnotneeded?Werethepatient/carer/attending physi-cianafraidofusingthesuspecteddrug?
Statisticalanalysis
NPV were calculated and compared using chi-square test using STATA (StataCorp. 2017. Stata Statistical Software: Release15.CollegeStation,TX,USA:StataCorpLLC).The distributionofothervariablesbetweenthetwogroupswere comparedusingStudent’st-test,Fisher-exact-testand chi-square test where appropriate. The level of significance consideredwas˛=0.05.
Ethicsandconsent
Thisstudywasapprovedbyaninstitutionalethics commit-teeandthedatabasewasregisteredinthePortugueseData ProtectionAuthority.Children’sparentsortheentitled care-giverssignedaninformedconsentforthestudy.
Results
Atotalof 212 patientswere included: 151in CHP and61 in HDE, 86 females, 126 males,average age at DPT 5.52 years(median four years, p25---p75: 3---7.25 years). Sixty-nine(32.5%)patientswere testedwithshortDPTand143 (67.5%) with extended DPT. No significant differences in age,sex,typeofreactionorDPTantibioticwereobserved betweenthegroups(Table1).
ShortandextendedDPTshavesimilarnegative predictivevalue
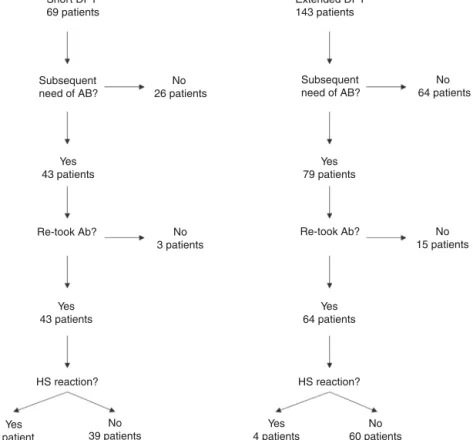
Onehundredandfourofthe212patients(49.1%)were re-exposedtobeta-lactamsmonthstoyearsafterthenegative DPT(Fig.1):40/69(58%)intheshortDPTgroupand64/143
Table1 Shortvs.extendedDPTsamplecharacteristics.
Total ShortDPT ExtendedDPT p-value
Numberofpatients 212 69(32.5%) 143(67.5%) ---Femalesex 86(40.1%) 29(42.0%) 57(39.9%) NSp=0.76 AgeatDPT,years Mean 5.52 5.53 NS p=0.48 Median(p25---p75) 4(3---7.25) 4(3---8) HSRsymptoms Mucocutaneous 199a 92.0% 66 94.2% 133 90.9% NS p=0.55 Mucocutaneous+digestive 8 3.75% 2 2.9% 6 4.2%
Serumsickness-likedisease 3 1.4% 0 0% 3 2.1%
Others,ill-defined 2 0.95% 1 1.45% 1 0.7% DPTantibiotic Amoxicillin 102 48.1% 37 53.6% 65 48.6% NS p=0.23 Amox/clav 92 43.4% 26 37.7% 66 43.1% Cefuroxime 11 5.2% 4 5.8% 7 4.2% Cefaclor 5 2.4% 1 1.45% 4 3.5% Cefatrizine 2 0.9% 1 1.45% 1 0.7%
a Mucocutaneousincludesmaculopapularexanthemawithmucousangioedema(n=3),maculopapularexanthemawithoutangioedema (191),skinerythemas(4)andurticariphormexanthema(1).
DPT:drugprovocationtest;HSR:hypersensitivityreaction;MPE:maculopapularexanthema;Amox/clav:amoxicillinandclavulanate; NS:non-significant.
Short DPT 69 patients Extended DPT 143 patients Subsequent need of AB? Subsequent need of AB? No 26 patients No 64 patients Yes 43 patients Yes 1 patient Yes 43 patients Yes 64 patients HS reaction? HS reaction? Yes 79 patients Yes 4 patients
Re-took Ab? Re-took Ab? No
15 patients No 60 patients No 3 patients No 39 patients
Figure1 Patientdistributioninthetwostudygroupsandquestionnaireresults.DPT:drugprovocationtest;AB:antibiotic;HS: hypersensitivity.
(44.8%)intheextendedDPTgroup(p=0.071).Manyfactors mayhavecontributedtothefrequencyofsubsequent antibi-otic use, e.g., time interval between DPT and telephone interview,rateofinfections,ageofthepatient,among oth-ers.Carer/assistantphysicianrefusalofsubsequentusewill be analysed below. Among the patients re-exposedto BL afternegativeDPT,5/104patientsreportedasuspectedHSR onre-exposure(NPVwas95.2%,when both DPTprotocols wereanalysedtogether).
On re-exposure, only 1/40 patients in the short DPT groupdeveloped a suspected HSR (NPV: 97.5%) compared to4/64patientsintheextendedDPTgroup(NPV:93.75%),
p=0.419(Table2).AllfivepatientswhodevelopedHSRon re-exposure had maculopapular exanthema (MPE) on the HSRindexandagainpresentedMPEonre-exposure.Allfive weremale,average ageat DPTwasfiveyearsand theBL involvedwereamoxicillin/clavulanateinthreepatientsand amoxicillinintwo.
RateofdrugrefusalafternegativeDPTwassmaller intheshortDPTprotocol
Wethenfocusedonthosepatientswho,afternegativeDPT, requiredBLforsubsequentinfectionsbutrefusedthe treat-mentduetofearofHSR.Thedecisiontorefusetreatment mighthavebeentakenbythepatient,carersorprescribing physicians.
DespitepreviousnegativeDPT,antibiotictreatmentwas refusedin18outof122patientsthatrequiredBL(14.75%). Age was higher in those refusing the drug (6.44 years of
age vs. 4.47 years, p=0.021). No significant differences wereobservedbetweenpatientswhorefusedthedrugand thosere-exposedintermsoftypeofinitialHSR (mucocuta-neousreactionin16/18vs.98/104,respectively,p=0.335). Themostfrequentculpritdruginpatientswhorefused re-exposure wasamoxicillin/clavulanate (11patients, 61.1%) andamoxicillinintheremainingsevenpatients(38.9%).In patientswhowerere-exposed(104patients),thesuspected BL were amoxicillin/clavulanate in 40 patients (38.5%), amoxicillin in 57 (54.8%), cefuroxime in five (4.8%) and cefaclor in two (1.9%). Amoxicillin/clavulanate was more frequentinthoserefusingretreatment(p=0.072).
IntheshortDPTgroup,refusaloccurredinthreeoutof 43(6.98%)ofthepatientsthatweresubsequentlyprescribed BLantibiotics,whereasintheextendedDPTgroup,refusal occurredin15outof79patients(18.99%),p=0.074.
Discussion
Inthisstudyweaimedtodeterminewhetherprolongingthe expositiontotheantibioticimprovedthenegative predic-tivevalueofDPTsforthediagnosisofmildnon-immediate HSR to beta-lactams in children. This is a relevant ques-tionbecauseseveralalterationstotheDPTprotocolshave been suggestedandimplementedbutfew datahavebeen published directly comparingthe twomethods toconfirm additional benefits. We evaluated both the recurrence of HSRsymptomsonre-exposure,anddrugrefusalafter nega-tiveone-dayDPTsversuslongerDPTs.
Table2 NegativepredictivevalueoftheDPTandantibioticrefusalafternegativeDPT.
Total ShortProtocol ExtendedProtocol p-value
HSRonre-exposure Negativepredictive value 5/104 95.2% 1/40 97.5% 4/64 93.75% NS p=0.419 Antibioticrefusal afternegativeDPT 18/122 14.75% 3/43 6.98% 15/79 18.99% NS p=0.074 HSR:hypersensitivityreaction;DPT:drugprovocationtest;NS:non-significant.
Table3 Summaryofcurrentstudyandpreviouslyreportedfindings. Agegroup Numberof
patients
Drugstested TypeofHSR Duration ofDPT Re-exposure rate NPVfor beta-lactams Refusalrate after negative DPT Regateiroetal. (presentstudy)
Children 212 Beta-lactams Non-immediate Both 1day 3---7days 49% 58% 45% 95.2% 97.5% 93.8% 14.8% 7% 19% Ponvertetal.4 Children 141 Beta-lactams Immediateand
non-immediate 5---7days 66% 97.9% ---Misirlioglu etal.24 Children 108a Beta-lactams andother drugs Immediateand non-immediate 1---6days 51%b 93.3%a 31%b
Demolyetal.34 Adults 457 Betalactams Immediateand
non-immediate
1day 25.8% 94.1%
---Watonetal.33 Adults 100a Beta-lactams
andother drugs
Immediateand non-immediate
1day 17%a 100%a 25.3%c
a Onlyincludingthedataconcerningbeta-lactams. b Dataconcerningalltypesofantibiotics.
c Foralldrugstested(betalactamsandnon-betalactams).
Our results confirm the high NPVof diagnostic DPTs in non-immediateHSRtobeta-lactamsinchildren(95.2%,both DPT protocols together). Similar values were reported in otherstudies(Table3)despitedifferencesinmethodologies, typeofHSRandpopulationsenrolled.Whencomparingthe NPVofshortversusextendedDPTs,wefoundnodifferences between protocols, although there were more suspected falsenegativesintheextendedgroup(NPVshortDPT97.6% vs. NPV extended DPT 93.8%). Such a small differenceis likelyclinicallyirrelevant.
RefusalofthesuspecteddrugafternegativeDPTremains asignificantissue.Inourstudy,atotalof14.75%ofpatients were refused BL after a negative DPT. In our sample, extended protocolsdid not increase confidence in subse-quent use and, in fact, drug refusal was higher in the extendedDPTgroup.The reasonsfor thisareunclearand werenotexploredinourstudy.Wemayspeculatethat psy-chologicalfactors,suchasa‘‘backfireeffect’’,32mayhave
playedarole.Wenotedthatrefusalwasmorefrequentin childrentested withamoxicillin/clavulanateandwe spec-ulatethatperhapssomenon-allergicsideeffectsoflonger treatmentswithamoxicillin/clavulanate,suchasdigestive symptoms,mayhaveinfluencedsubsequentdecisiontouse thisantibiotic.
Altogether,ourresults showednobenefitinprolonging administrationtotest non-immediateHSRtobeta-lactams in children in the parameters analysed. Previously pub-lishedliteraturearguedforthesafetyofextendedDPTsand reportedthatsomepatientsdevelopedHSRsymptomsonly afterseveraldaysof drugadministrationduring extended DPTs (in adults).25---27 It is however unclear whetherthese
patientswouldhave developedthesedelayed symptomsif ashortDPThadbeen performed.Datadirectlycomparing sensitivity,NPVandre-exposureconfidenceofshortversus extendedDPTsprotocolsisgenerallylackingandourstudy addressesthelattertwoquestions.
Ourstudyincludedalargenumberofchildrenwith simi-larcharacteristicsinbothgroups(e.g.,age,typeofHSRor suspectedantibiotic).BothDPTprotocolswereperformed inthetwohospitalstomitigatedifferencesinprocedures, personal recommendations or regional differences.In our study,a large number of patients (104/212, 49.1%) were re-exposedtotheculpritdrugsubsequenttonegativeDPT. A wide variationon re-exposure rates has been reported (Table3)andthereasonsforavoidancehavebeenexplored elsewhere.33 The high percentage of re-exposure in our
studymay,atleastinpart,beexplainedbythelongperiod betweentheDPTandthe questionnairein somepatients,
andtheyoungageofthepatients(e.g.,childrenhavemore frequentinfectionsprovidingmorepossibilitiesofantibiotic prescription, parents are possibly more abiding to physi-cians’prescriptionsthanadultindividualsdecidingontheir ownhealth).
Weareawareofsomelimitationsinourstudy.Weused aquestionnaire toevaluatere-exposureand drugrefusal. SomecarerswereinterviewedseveralyearsafterDPTand re-exposure, and this might introduce some recall bias. Although we tried to confirm that patients reporting HSR onre-exposurewereindeeddescribing HSRsymptoms, no additionalallergologicalworkupwasperformedtoconfirm truesensitisation.Ithasbeensuggestedthat,aswithindex event, some subsequent HSR reports on re-exposure are not‘‘real’’HSR4,24andthismighthaveunderestimatedthe
NPVinourstudy(however,atanexpectedrateinthetwo protocols).Thepresenceofnon-allergicside-effects,likely arisingmorefrequentlyduringextendedDPT,wasnot eval-uatedinour studyand thismight influence willingness to usethesamedrugbesidesfearoftheHSR.Thehypothetical influencesofthetimeintervalsbetweenHSRandDPTand alsobetweenDPTandre-exposurewerenotanalysed. How-ever,theseputativeeffectsaremitigatedbythefactthat, analysingapaediatricpopulation(averageageatDPT=5.52 years),theseintervalswereneververylong.
In conclusion, we did not find additional benefits in prolonging DPT both in terms of NPV and confidence for antibioticuse.Howeverintuitive,anymodificationsofDPT protocols should be adequately compared with previous standardpracticeforsensitivity,specificity,predictive val-ues,side-effectsand,importantly,patients/carersadhesion totheDPTresult.Giventheloweventrate ofHSRon re-exposureafternegativeDPT,studiesinlargepopulationsare required todetermine the optimal length of DPT. Finally, thediagnosticperformanceofDPTsisalwayslimitedbythe incompletemimickingofall‘‘real-life’’conditions:DPTsare usuallyperformedin‘‘controlled’’settings,whereassome HSRsymptomsmayonlyariseinthepresenceofco-factors occurring in ‘‘real-life’’ situations, e.g. during infection, afterphysicalexercise,orNSAIDsintake.Otherissuesunder investigation,such asthedevelopmentof drugresistance or drug sensitisation during diagnostic procedures, might alsocontributetodetermine therisk/benefitofprolonged exposition.
Funding
The authorsdeclare thatnofunding wasreceivedfor the presentstudy.
Conflicts
of
interest
Theauthorsdeclarethattheyhavenoconflictsofinterest.
Acknowledgements
The authorsthank Dr.Gearoid McMahonfor the insightful commentsonthemanuscript.
References
1.Gomes ER, Demoly P. Epidemiology of hypersensitivity drug reactions.CurrOpinAllergyClinImmunol.2005;5:309---16. 2.Sastre J, Manso L, Sanchez-García S, Fernández-Nieto M.
Medicalandeconomic impactofmisdiagnosisofdrug hyper-sensitivity in hospitalized patients. J Allergy Clin Immunol. 2012;129:566---7.
3.RebeloGomesE,FonsecaJ,AraujoL, DemolyP.Drugallergy claimsinchildren:fromself-reportingtoconfirmeddiagnosis. ClinExpAllergy.2008;38:191---8.
4.PonvertC,WeilenmannC,WassenbergJ,WaleckiP,Bourgeois ML,DeBlicJ,etal.Allergytobetalactamantibioticsin chil-dren:aprospectivefollow-upstudyinretreatedchildrenafter negativeresponsesinskinand challengetests. AllergyEurJ AllergyClinImmunol.2007;62:42---6.
5.RubioM,BousquetP-J,GomesE,Romanoa,DemolyP.Results ofdrughypersensitivityevaluationsinalargegroupofchildren andadults.ClinExpAllergy.2012;42:123---30.
6.Atanaskovic-MarkovicM,GaetaF,MedjoB,Gavrovic-Jankulovic M,CirkovicVelickovicT,TmusicV,etal.Non-immediate hyper-sensitivityreactionstobeta-lactamantibioticsinchildren---our 10-yearexperienceinallergywork-up.PediatrAllergyImmunol. 2016;27:533---8.
7.PonvertC,PerrinY,Bados-AlbieroA,LeBourgeoisM,KarilaC, DelacourtC,etal.Allergytobetalactamantibioticsinchildren: resultsofa20-year studybasedon clinicalhistory, skinand challengetests.PediatrAllergyImmunol.2011;22:411---8. 8.ZamboninoMA,CorzoJL,Mu˜nozC,RequenaG,ArizaA,
May-orgaC,etal.Diagnosticevaluationofhypersensitivityreactions to beta-lactamantibiotics in a largepopulation of children. PediatrAllergyImmunol.2014;25:80---7.
9.PichlerWJ,AdamJ,DaubnerB,GentinettaT,KellerM,YerlyD. Drughypersensitivity reactions:pathomechanism andclinical symptoms.MedClinNorthAm.2010;94:645---64.
10.GomesER,BrockowK,KuyucuS,SarettaF,MoriF,Blanca-Lopez N,etal.Drughypersensitivityinchildren:reportfromthe pedi-atrictaskforceoftheEAACIDrugAllergyInterestGroup.Allergy EurJAllergyClinImmunol.2016;71:149---61.
11.Caubet J, Pichler WJ, Eigenmann PA. Educational case series: mechanisms of drug allergy. Pediatr Allergy Immu. 2011;22:559---67.
12.CaubetJC,KaiserL,LemaîtreB,FellayB,GervaixA,Eigenmann PA.Theroleofpenicillin inbenignskinrashesinchildhood: aprospectivestudybasedondrugrechallenge.JAllergyClin Immunol.2011;127:218---22.
13.AbererW, BircherA, Romano A,Blanca M,Campi P, Fernan-dez J, et al. Drug provocation testing in the diagnosis of drughypersensitivityreactions:generalconsiderations.Allergy. 2003;58:854---63.
14.RomanoA,BlancaM,TorresMJ,BircherA,AbererW,BrockowK, etal.Diagnosisofnonimmediatereactionsto-lactam antibi-otics.AllergyEurJAllergyClinImmunol.2004;59:1153---60. 15.ChiriacAM,WangY,SchrijversR,BousquetPJ,MuraT,Molinari
N,etal.Designingpredictivemodelsforbeta-lactamallergy usingthedrugallergyandhypersensitivitydatabase.JAllergy ClinImmunolPract.2018;6:139---48,e2.
16.MayorgaC,Do˜naI,Perez-InestrosaE,FernándezTD,TorresMJ. Thevalueofinvitroteststodiminishdrugchallenges.IntJMol Sci.2017;18:pii:E1222.
17.Barni S, Mori F, Sarti L, Pucci N, Rossi EM, de Martino M, etal.Utilityofskintestinginchildrenwithahistoryof non-immediatereactionstoamoxicillin.ClinExpAllergy.2015;45: 1472---4.
18.PadialA,AntunezC,Blanca-LopezN,FernandezTD, Cornejo-GarciaJA,MayorgaC,etal.Non-immediatereactionsto beta-lactams:diagnosticvalueofskintestinganddrugprovocation test.ClinExpAllergy.2008;38:822---8.
19.ChambelM,MartinsP,SilvaI,Palma-CarlosS,RomeiraAM,Leiria PintoP.Drugprovocationteststobetalactamantibiotics: expe-rienceinapaediatricsetting. AllergolImmunopathol(Madr). 2010;38:300---6.
20.VezirE,DibekMisirliogluE,CivelekE,CapanogluM,GuvenirH, GinisT,etal.Directoralprovocationtestsinnon-immediate mildcutaneous reactions relatedto beta-lactam antibiotics. PediatrAllergyImmunol.2016;27:50---4.
21.Blanca-LópezN,ZapateroL, AlonsoE,TorresMJ,FuentesV, Martínez-MoleroMI,etal.Skintestinganddrugprovocationin thediagnosisofnonimmediatereactionstoaminopenicillinsin children.AllergyEurJAllergyClinImmunol.2009;64:229---33. 22.MoralL,GardeJ,ToralT,FuentesMJ,MarcoN.Shortprotocol
for thestudyof paediatricpatientswithsuspected betalac-tamantibiotic hypersensitivity andlow riskcriteria.Allergol Immunopathol(Madr).2011;39:337---41.
23.Mirakian R, Leech SC, Krishna MT, Richter AG, Huber PAJ, FarooqueS,etal.Managementofallergytopenicillinsandother beta-lactams.ClinExpAllergy.2015;45:300---27.
24.Misirlioglu ED, Toyran M, Capanoglu M, Kaya A, Civelek E, Kocabas CN. Negative predictive value of drug provo-cation tests in children. Pediatr Allergy Immunol. 2014;25: 685---90.
25.FranssonS,MosbechH,KappelM,HjortlundJ,PoulsenLK, Kvis-selgaardAD,etal.Theimportanceofprolongedprovocationin drugallergy---resultsfromaDanishallergyclinic.JAllergyClin ImmunolPract.2017;5:1394---401.
26.HjortlundJ,MortzCG,SkovPS,Bindslev-JensenC.Diagnosisof penicillinallergyrevisited:thevalueofcasehistory,skin test-ing,specificIgEandprolongedchallenge.AllergyEurJAllergy ClinImmunol.2013;68:1057---64.
27.HjortlundJ,MortzCG,SkovPS,EllerE,PoulsenJMH,BorchJE, etal.One-week oralchallenge withpenicillinindiagnosisof penicillinallergy.ActaDermVenereol.2012;92:307---12. 28.Picard M, Paradis L, Nguyen M, Bégin P, Paradis J, Roches
AD.Outpatient penicillin useafternegativeskintesting and drugchallengeinapediatricpopulation.AllergyAsthmaProc. 2012;33:160---4.
29.Ratzon R, Reshef A, Efrati O, Deutch M, Forschmidt R, Cukierman-YaffeT,etal.Impactofanextendedchallengeon the effectiveness of -lactam hypersensitivity investigation. AnnAllergyAsthmaImmunolAmCollAllergyAsthmaImmunol. 2016;116:329---33.
30.CapanogluM,VezirE,MisirliogluED,GuvenirH,Buyuktiryaki B,ToyranM,etal.Additionalprovocationtestinginpatients withnegative provocation test resultswith -lactam antibi-otics. Ann Allergy Asthma Immunol Am Coll Allergy Asthma Immunol.2016;116:82---3.
31.Iglesias-SoutoJ,GonzálezR,PozaP,Sanchez-MachínI,Matheu V.Evaluatingtheusefulnessofretestingforbeta-lactamallergy inchildren.PediatrInfectDisJ.2012;31:1091---3.
32.NyhanB,ReiflerJ. Whencorrectionsfail:thepersistenceof politicalmisperceptions.PolitBehav.2010;32:303---30. 33.Waton J,Pouget-Jasson C,Loos-AyavC,TrechotP, Bursztejn
AC,SchmutzJL,etal.Drugre-challengesincutaneousadverse drugreactions:informationandeffectivenessinthelong-term managementofpatients.AllergyEurJAllergyClinImmunol. 2011;66:941---7.
34.DemolyP,Romano A, BotelhoC,Bousquet-RouanetL, Gaeta F,SilvaR,etal.Determiningthenegativepredictivevalueof provocationtestswithbeta-lactams.AllergyEurJAllergyClin Immunol.2010;65:327---32.