w w w . r b o . o r g . b r
Original
Article
Clinical
repercussions
of
Martin-Gruber
anastomosis:
anatomical
study
夽
Cristina
Schmitt
Cavalheiro
a,∗,
Mauro
Razuk
Filho
a,
Gabriel
Pedro
a,
Maurício
Ferreira
Caetano
b,
Luiz
Angelo
Vieira
a,
Edie
Benedito
Caetano
aaSchoolofMedicalandHealthSciences,PontifíciaUniversidadeCatólicadeSãoPaulo,Sorocaba,SP,Brazil bHandSurgeryService,ConjuntoHospitalardeSorocaba,Sorocaba,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received4May2015 Accepted11June2015
Availableonline23February2016
Keywords: Arteriovenous
anastomosis/anatomy&histology Mediannerve
Ulnarnerve
a
b
s
t
r
a
c
t
Objective:The mainobjective ofthis study wastodescribe Martin-Gruberanastomosis anatomicallyandtorecognizeitsclinicalrepercussions.
Method:100forearmsof50adultcadaversweredissectedinananatomylaboratory.The dissectionwasperformedbymeansofamidlineincisionalongtheentireforearmandthe lowerthirdoftheupperarm.Twoflapsincludingskinandsubcutaneoustissuewerefolded backontheradialandulnarsides,respectively.
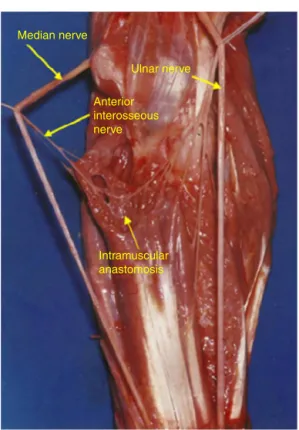
Results:Nervecommunicationbetweenthemedianandulnarnervesintheforearm (Martin-Gruberanastomosis)wasfoundin27forearms.Theanastomosiswasclassifiedintosix types:typeI:anastomosisbetweentheanteriorinterosseousnerveandtheulnarnerve (n=9);typeII:anastomosisbetweentheanteriorinterosseousnerveandtheulnarnerve attwopoints(doubleanastomosis)(n=2);typeIII:anastomosisbetweenthemediannerve andtheulnarnerve(n=4);typeIV:anastomosisbetweenbranchesofthemediannerveand ulnarnerveheadingtowardtheflexordigitorumprofundusmuscleofthefingers;these fasciclesformaloopwithdistalconvexity(n=5);typeV:intramuscularanastomosis(n=5); andtypeVI:anastomosisbetweenabranchofthemediannervetotheflexordigitorum superficialismuscleandtheulnarnerve(n=2).
Conclusion:Knowledgeoftheanatomicalvariationsrelatingtotheinnervationofthehand hasgreatimportance,especiallywithregardtophysicalexamination,diagnosis, progno-sisandsurgicaltreatment.Ifthesevariationsarenotgivendueregard,errorsandother consequenceswillbeinevitable.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedintheDepartmentofSurgery,SchoolofMedicalandHealthSciences,SorocabaCampus,PontifíciaUniversidade CatólicadeSãoPaulo,Sorocaba,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.S.Cavalheiro). http://dx.doi.org/10.1016/j.rboe.2016.02.003
anatômico
Palavras-chave: Anastomose
arteriovenosa/anatomiae histologia
Nervomediano Nervoulnar
r
e
s
u
m
o
Objetivos: DescreveranatomicamenteaanastomosedeMartin-Gruberereconhecersuas repercussõesclínicas.
Método: Foramdissecados100antebrac¸osde50cadáveresadultosnolaboratóriode anato-mia.Adissecc¸ãofoifeitaatravésumaincisãomedianaemtodooantebrac¸oeterc¸oinferior dobrac¸o,doisretalhosincluindoapeleesubcutâneoforamrebatidos,paraoladoradiale ulnarrespectivamente.
Resultados: Acomunicac¸ãonervosaentreosnervosmedianoseulnarnoantebrac¸o (anas-tomosedeMartin-Gruber)foiregistradaem27antebrac¸os.Classificamosaanastomoseem seistipos.TipoI:anastomoseentreonervointerósseoanterioreonervoulnar(nove mem-bros);TipoII:anastomoseentreonervointerósseoanterioreonervoulnaremdoispontos (duplaanastomose-doismembros);TipoIII:anastomoseentreomedianoeonervoulnar (quatromembros);TipoIV:anastomoseentreramosdosnervosmedianoeulnardestinada aomúsculoflexorprofundoosdedos,essesfascículosformamumaalc¸adeconvexidade distal(cincomembros);TipoV:anastomoseintramuscular(cincomembros);TipoVI: anas-tomoseentreramodonervomedianoparaomúsculoflexorsuperficialenervoulnar(dois membros).
Conclusão: Oconhecimentodasvariac¸õesanatômicasemrelac¸ãoàinervac¸ãodamãotem importânciarelevante,principalmentequandoseconsideraoexamefísico,diagnóstico, prognósticoetratamentocirúrgico.Seessasvariac¸õesnãoforemvalorizadas,errose con-sequênciasserãoinevitáveis.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Theanatomyoftheupperlimbsisextremelycomplex.In addi-tiontothe complexityoftheformatofthebrachial plexus andtheexistenceofstrategicanatomicalzonessuchasthe epitrochlear-olecranongroove(ulnarcanal),carpalcanaland Guyoncanal,anomalousnervebranchescanbefound.These mayformanastomosesinparticularsitesthathaveclinical andfunctionalimportance.
Theinnervationpatternthatismostacceptedinrelation totheintrinsicmusclesthatactinrelationtofinemovements ofthehandisthattheopposingshortabductormuscle,the superficial portion ofthe short flexormuscle and the first andsecondlumbricalmusclesreceiveinnervationfromthe mediannerve.Thedeepportionoftheshortflexormuscle,the adductormuscleofthethumb,themusclesofthehypothenar region,thedorsalandpalmarinterosseousmusclesandthe fourthandfifthlumbricalmusclesareinnervatedbytheulnar nerve. The great varietyof clinical conditions observed in casesofisolatedlesionsofthemedianorulnarnerveledus toinvestigatethis.
Clinically,variationsoftheinnervationofthesesmall mus-clesareveryimportant,inthatevenifthemedianorulnar nerveiscompletelytorn,someofthesemusclesmaynot nec-essarilybeparalyzed.Thiscouldleadtothewrongconclusion thatthenervehadnotbecomecompletelytorn.
The studies that we consulted showed many diver-gences,andthesebecame moremarkedwhenthe authors
used different investigative methods. The methods used includedelectroneuromyography,selectiveanesthetic block-ageofnervesandanatomicaldissection.Clinicalreportsand electroneuromyographic studies have suggested that these musclesmayreceivedoubleinnervationfromthemedianand ulnar nerves.Highet1analyzed45patientswithcompletely tornmedianorulnarnervesandfoundthattheshortflexor muscleofthethumbwastotallyparalyzedinonlyfiveofthem. Forrest2drewattentiontothisandstatedthatcommunication betweenthemedianandulnarnervesinthehandmightbe morefrequentthanisimaginedandthatthemuscleslocated closeto thiscommunication (nerveanastomosis) mightbe receivinginnervationfrombothnerves(doubleinnervation).
Fig.1–Medianincisioninthevolarfacealongtheentire forearm.
Nerve communication between the median and ulnar nervesintheforearm,whichisknownasMartin-Gruber anas-tomosis,causestransferofnervefasciclesfromthemedian nervetotheulnarnerve.Thisgivesrisetoalterationofthe nor-malanatomicalpatternofthemotorandsensoryinnervation ofthehand.ItwasfirstdescribedbyMartin,3whoconsidered thepossibilityofcommunicationbetweenthesenervesinthe forearm.Around100 yearslater,in1870,Gruber4 dissected 250forearmsandfoundcommunicationbetweenthesetwo nervesin38ofthem.
It has been demonstrated in the literature that the incidenceofthis nervecommunication varieswhen differ-ent investigative methods are compared, i.e. according to whetherelectroneuromyography,selectiveanesthetic block-ageofnervesoranatomicaldissectionisused.Accordingto Sunderland,5severalfactorscausedifficultyinevaluatingthe motorfunctionofthehand.Themostimportantoftheseare anatomicalvariationsorfailuretoevaluatetheroleof decep-tivemovements,giventhatthesemayimitateandcoverup forlossofthe originalmovements.If thesefactorsare not properlyvalued,errorsinmakingdiagnosesandassessingthe resultswillbeinevitable.
Methods
Dissectionswereperformedon100forearmsof50adult cadav-ersbelongingtoourAnatomy Laboratory,amongwhich46 weremaleandfourwerefemale.Theiragesrangedfrom28to 77years;27werewhiteand23werenonwhite.Forearmsthat hadbeendeformedthroughinjury,malformationorscarring wereexcluded.
Thedissectionwasperformedbymeansofamedian inci-sion along the entire forearm and the lower third of the upperarm.Twoflapsthatincludedtheskinandsubcutaneous tissuewere pulled backtoward the radialand ulnar sides, respectively.Thesamewasdoneinrelationtothefasciaof theforearm, andthus theentiremusculaturewasexposed (Figs.1and2).
All ofthemuscles ofthe forearmwere dissected. Their innervation and the presence of nerve communication betweentheforearmnerveswereanalyzed.Alltheanatomical variationsencounteredwererecorded,annotatedand photo-graphed.AKeelermagnifyingglassof2.5×wasused.A1cm
segmentoftheanastomoticramuswasremovedandtaken toasurgicalmicroscope.Withtheaidofmicrosurgical twee-zers,thefascicleswereseparated,countedandphotographed.
Fig.2–Twoflapsthatincludedtheskinandsubcutaneous tissuewerepulledbacktoexposethefasciaandthenthe musculatureoftheforearm.
Infourlimbs,werecordedonlyonefascicle;ineight,two;in nine,three;infour,four;inone,five;andinone,seven.
InadditiontoinvestigatingMartin-Grubernerve commu-nication,therelationshipbetweentheGantzermuscleandthe anteriorinterosseousandmediannervesandtheanatomical variationsoftheforearmmuscleswereanalyzed.Thisstudy wasapprovedbytheResearchEthicsCommittee.
Results
Werecordedthe presenceofMartin-Gruberanastomosisin 27ofthe100forearmsdissected.Bilateralitywasobservedin threecadavers.In13cases,nervecommunicationoccurredin theleftforearmandin14casesintherightforearm.Regarding thetopographiclocation,mostofthenervecommunications occurredintheproximalthirdoftheforearm.
Inthemostfrequentlyencounteredformof communica-tion, whichwas seeninnine forearms, the nervefascicles originatedfromtheanteriorinterosseousnerve,atavarietyof sites,andheadeddistallyatwidelyvaryingdegreesof obliq-uity. They were locatedposteriorly tothe ulnar artery and weresupportedonthedeepflexorsofthefingers,anteriorly tothem.Theyheadedtowardtheulnarnerveandjoinedtoit closetothejunctionbetweentheproximalthirdandmiddle thirdoftheforearm.Inallofthesecases,thefascicles origi-nateddistallytotheelbowjoint.Weconsideredthistobetype I(Fig.3).
TypeIIwasrecordedintwolimbs.Thenervefascicles orig-inatedfromtheanteriorinterosseousnerve,justlikeintype I,withbifurcationofthefascicles,whichcommunicatedwith theulnarnerveattwodifferentpoints(Fig.4).
Median nerve
Ulnar nerve
Anterior interosseous nerve
Fig.3–TypeI.Thiswasthemostfrequentformof communication(seeninninelimbs).Thenervefascicles originatedfromtheanteriorinterosseousnerveand headedtowardtheulnarnerve.
Type V, which was also observed in five forearms, dif-fered from the preceding type in that the communication between the fascicles coming from the median and ulnar nervesoccurred insidethemusclemassofthedeepflexors ofthefingers.ThiswascalledintramuscularMartin-Gruber communication(Fig.7).
IntypeVI,whichwasrecordedintwoforearms,the fasci-clesoriginatedfromthebranchofthemediannervetoward thesuperficialflexormuscleandheadedobliquelyanddistally tocommunicatewiththeulnarnerve(Fig.8).
Segmentsoftheanastomoticramusoflength0.5–1.0cm wereremoved.Thenumberoffascicleswascountedundera surgicalmicroscope,atmagnificationsrangingfrom10to16×.
Withtheaidofmicrosurgicaltweezers,the fasciclesofthe anastomoticramuswereseparated.Infourlimbs,werecorded onlyonefascicle;ineight,two;innine,three;infour,four;in one,five;andinone,seven(Fig.9).
Discussion
Theincidenceofnervecommunicationbetweenthemedian andulnarnervesintheforearmisvariableandthisbecomes more marked when the results obtained through elec-troneuromyographicstudies arecomparedwiththose from anatomicaldissections.Table1showstheauthors,thenature ofthestudy,thenumberofcasesandthepercentageofnerve communication.
Ulnar nerve
Median nerve
Anterior interosseous nerve
Fig.4–IntypeII,whichwasrecordedintwolimbs,the nervefasciclesoriginatedfromtheanteriorinterosseous nerve,withbifurcation,andcommunicatedwiththeulnar limbattwodifferentpoints.
To the best of our knowledge, no anatomical studies regarding the innervation of the opposing muscle of the thumbthroughtheulnarnervehavebeenconducted. How-ever,throughelectromyographicstudies,itwasrecordedby Sala6in32%ofthecases,byForrest2in20%,byHarnessand Sequeles7in77%,byHighet1in20%andbyRosen8in16.7%.In comparingthestudiesofSala6andForrest,2inwhichexactly thesametechniquewasusedyetcompletelydifferentresults wereachieved(Sala677%andForrest220%),itcanbeseenthat intheopinionofForrest,2thisoccurredbecausetheauthors placedelectrodesatdifferentdepthsandbecauseSala6placed electrodesincontactwiththemusclefibersoftheshortflexor muscle, thereby obtaininga higherpercentage. This differ-encedemonstratesthatstudiesconductedthroughelectrical stimulation are notasprecise asthose conductedthrough anatomicaldissection.
Median nerve
Anterior interosseous nerve
Ulnar nerve
Fig.5–IntypeIII,whichwasrecordedinfourlimbs,the fasciclesoriginatedfromthemediannerve,proximaltothe emergenceoftheanteriorinterosseousnerve,andheaded towardtheulnarnerve.
themediannerveclosetotheulnarnerve,inthedistalthird oftheforearm.Thisanatomicalformathassofarnotbeen recorded in the literature.It isprobably anextremely rare anatomicalvariation,oravariationofgroupIIofourfindings,
Median nerve
Ulnar nerve
Anterior interosseous nerve
Deep flexor muscle of the fingers
Fig.6–IngroupIV,whichwasrecordedinfivelimbs,
communicationoccurredbetweennervefasciclesthatwere
headingforthedeepflexormuscleofthefingers,andthe fasciclesformedaloopwithdistalconvexity.
inwhichunionwiththeulnarnervewouldoccurinthedistal thirdoftheforearm.
Theclassificationdrawn upbySrinivasan andRhodes12 is theone thatcomes closestto ourobservations. We dis-agreewith itonlyin relationtotwopoints. These authors consideredtypeItobecommunicationsthatoriginatedinthe proximalportionoftheanteriorinterosseousnerveandgroup
Table1–Summaryoftheliteratureinvolvingtheincidenceofanastomosisbetweenthemedianandulnarnerves (Martin-Gruberanastomosis),accordingtoauthor.
Year Authors Study Casesstudied Casesthatpresented Martin-Gruber anastomosis(%)
1870 Gruber4 Anatomical 250 15.2
1893 Thomson9 Anatomical 406 15.5
1931 Hirasawa10 Anatomical Nodata 10.5
1976 Kimuraetal.11 Electrophysiological 328 17
1981 SrinivasanandRhodes12 Anatomical,genetic 200 15
1992 UchidaandSugioka13 Electrophysiological 47(cubitalsyndrome) 17
87(normal) 16
1992 Amoiridis26 Electrophysiological 100 32
1993 Nakashima14 Anatomical 108 21.3
1999 Shuetal.16 Anatomical,histological 72 23.6
2002 Rodriguez-Niedenfuhretal.17 Anatomical 140 13.6
236 13.1
2005 Leeetal.18 Anatomical,electrophysiological 102(anatomical) 39.2
224(electrophysiological) 23.2
Median nerve
Ulnar nerve
Anterior interosseous nerve
Intramuscular anastomosis
Fig.7–IntypeV,whichwasrecordedinfivelimbs,nerve
communicationoccurredinsidethemusclemassofthe
deepflexorsofthefingers(intramuscularanastomosis).
IItobethoseoriginatinginthedistalportionofthisnerve.We observedthatnervecommunicationcouldoriginateat differ-entlevelsoftheanteriorinterosseousnerve,butwedidnot seeanyreasontoconsiderthemtobedifferentgroups,since theyoriginatedinthesamenerveandhadthesameformat. Theotherpointofdisagreementisthattheseauthorsdidnot describeanyoccurrenceofintramuscularanastomosis.
It is still not possible to identify the origin and desti-nationofeachnerve fascicle,eitherbyelectrophysiological or by anatomical means. Anatomical studies are based on the apparent path the fascicles are following, from one nerve to another. In agreement with the majority of authors,4,5,9,10,12,14–17 wecanaffirmthatwedidnotobserve anypassageofmotorfasciclesfromthe ulnarnervetothe median nerve, in any of the limbs. We recorded that the communicationsweredirectedfromthemediannervetothe ulnar.However,nervesarecomposedofmotorfascicles (effer-ent)andsensory fascicles(afferent).Itisthereforepossible thatsensoryfascicles(afferent)aredirectedfrom theulnar tothemediannerve.IngroupIII,itislikelythatin commu-nicationsoriginatinginthemediannerve(whichisamixed nerve),therearebothefferent(motor)andafferent(sensory) fascicles.Intheotherlimbs,communicationwasbymeansof amotornerve:anteriorinterosseousintypesI,II,IVorV;or bymeansofabranchofthemediannervetothesuperficial flexormuscleintypeVI.Inthissituation,itisunlikelythat sensoryfascicleswillexist.
Shaficetal.19reportedthecaseofapatientwhopresented allofthesymptomsofcarpaltunnelsyndrome,buthad neg-ativeresultsfromprovocativetestssuchasTinel’ssignand
Median nerve
Ulnar nerve Superficial
flexor muscle
Anastomose
Fig.8–IntypeVI,whichwasrecordedintwolimbs, fasciclescomingfromthebranchofthemediannerveto thesuperficialflexormuscleheadedtoward
communicationwiththeulnarnerve.
Phalen’s test.Thispatient presentedevidentsigns ofulnar nerve compression in the elbow. Nerve stimulation in the epitrochlear-olecranongroovetriggeredthetypicalsymptoms ofcarpaltunnelsyndrome,whichdemonstratedthattransfer ofsensorynervefascicles(afferent)fromtheulnarnerveto themediannerveexisted.
Marinacci20describedthecaseofapatientwhosuffered traumatic sectioningof the median nerve in the proximal forearm.Anelectromyographicevaluationshowed denerva-tion ofthelong flexormusclesofthethumb andthe deep flexoroftheindexandmiddlefingers,whichareusually inner-vatedbythemediannerve.However,thehanddidnotpresent motoralterationsseeneitherclinicallyor electromyographi-cally.Fromapplyingelectromyographicstimuliandfromthe velocityofmotorconductionofthemediannervesinthewrist andelbow,itwasconcludedthatthisalterationoccurredasa consequenceofpassageofnervefibersfromtheulnarnerve tothemediannerveintheforearm,distallytotheinnervation ofthelongflexorofthethumbandthedeepflexoroftheindex andmiddlefingers.Theauthornamedthistypeofinnervation ofalloftheintrinsicmusclesbytheulnarnerve“totalulnar hand”.Amongourresults,werecordedonelimbwithfiveand anotherwithsevenfascicles,butwecannotaffirmthatthese fascicleswouldbesufficienttoinnervatealloftheintrinsic musclesofthehand.
Fig.9–Distributionofthenumberoffasciclesinthe27recordsofMartin-Gruberanastomosis.Infourlimbs,weonly recordedonefascicle;ineight,two;innine,three;infour,four;inone,five;andinone,seven.
werefoundtobeinnervatedandsensitivitywaspreserved, despitecompleteruptureoftheulnarnerve.Thisauthoralso describedanothercaseinwhichtherewascompleterupture ofthemediannerveandalltheintrinsicmuscleswerefound tobefunctioning,despitetheabsenceofsensitivityinthearea ofinnervationofthemediannerve.Inthefirstsituation,all theintrinsicmusclesreceivedinnervationfromthemedian nerveandinthesecond,fromtheulnarnerve.These varia-tionswereattributedtoMartin-Gruberanastomosis.Basedon ourstudies,22itismorelikelythatthesevariationsoccurred becauseofCannieu-Richéanastomosis(communicationfrom motorbranchesofthemediannervetothemuscles ofthe
thenarregionandthedeepbranchoftheulnarnerve,inthe palmofthehand),becausethiscommunicationisthreetimes morefrequentthanMartin-Gruberanastomosis.
nerves.
Year Authors Classificationproposed;anastomosisbetweenthemedianandulnarnerves
1893 Thomson9 ClassI:anteriorinterosseousnerveandulnarnerve
ClassII:mediannerveandulnarnerve
ClassIII:musclebranchtodeepflexormuscleofthefingers
1931 Hirasawa10 Obliqueanastomosis:anteriorinterosseousnerveandulnarnerve
mediannerveandulnarnerve
Loopanastomosis:musclebranchtodeepflexormuscleofthefingers Combinedanastomosis:combinationsbetweenothers
1976 Kimuraetal.11 TypeI:mediannerveandulnarnerveinnervatingthehypothenarmuscle
TypeII:mediannerveandulnarnerveinnervatingthedeepflexormuscleofthefingers TypeIII:mediannerveandulnarnerveinnervatingthethenarmuscle
1981 SrinivasanandRhodes12 TypesI,II,VI:anteriorinterosseousnerveandulnarnerveorother
TypeIII:mediannerveandulnarnerve TypesIV,V:combinationsofothers
1992 UchidaandSugioka13 TypeI:mediannerveandulnarnerveinnervatingthehypothenarmuscle
TypeII:mediannerveandulnarnerveinnervatingthethenarmuscle
TypeIII:mediannerveandulnarnerveinnervatingthedeepflexormuscleofthefingers
1993 Nakashima14 TypeIa:anteriorinterosseousnerveandulnarnerve
TypeIb:mediannerveandulnarnerve TypeIII:combinationoftypesIa,IbandII
1995 Ohetal.15 TypeI:mediannerveandulnarnerveinnervatingthehypothenarmuscle
TypeII:mediannerveandulnarnerveinnervatingthedeepflexormuscleofthefingers TypeIII:mediannerveandulnarnerveinnervatingthethenarmuscle
1999 Shuetal.16 TypeI:anteriorinterosseousnerveandulnarnerve
TypeII:mediannerveandulnarnerve
TypeIII:musclebranchtodeepflexormuscleofthefingers
TypeIV:anteriorinterosseousnerveandulnarnerve,musclebranchtodeepflexor muscleofthefingersoriginatingfromtheconnection
TypeV:twoanastomoticbranches
2002 Rodriguez-Niedenfuhr
etal.17
PatternI:oneanastomoticramus PatternII:twoanastomoticrami
TypeA:anastomoticramusoriginatingfromabranchofthemediannervetothenerve ofthesuperficialflexormuscleoftheforearm
TypeB:anastomoticramusoriginatingfromthemediannerve
TypeC:anastomoticramusoriginatingfromtheanteriorinterosseousnerve
2005 Leeetal.18 TypeI:anteriorinterosseousnerveandulnarnerve
TypeII:mediannerveandulnarnerve
TypeIII:musclebranchtodeepflexormuscleofthefingers
TypeIV:twoanastomoticramifromtheulnarnerveoranteriorinterosseousnerveand ulnarnerve
2015 Ourclassification TypeI:anteriorinterosseousnerveandulnarnerve
TypeII:anteriorinterosseousnerveandulnarnerve(doubleanastomosis) TypeIII:mediannerveandulnarnerve
TypeIV:loopbetweenanteriorinterosseousnerveandulnarnervewithbranchesto deepflexormuscleofthefingers
TypeV:intramuscularanastomosis
TypeVI:branchfromthemediannervetothesuperficialflexormuscleandulnarnerve
forearmorinthepalmofthehand.Itismorelikelythatthis wasCannieu-Richéanastomosis,becausethisisthreetimes morefrequentthanMartin-Gruberanastomosis.
Brandsmaetal.24describedtwoclinicalcasesofpatients withcomplete ruptureoftheulnarnerveintheelbowand injurytothemediannerveinthe wrist,secondaryto neu-ropathyduetoleprosy,whichmaintainedgoodfunctioningof thefirstdorsalinterosseousmusclesandtheshortflexorof thethumb.Theyattributedthesefindingstothepresenceof Martin-Gruberanastomosis.Ourresultscontributesupportto
thisclinicalobservationthatthisoccurrencecouldonlyhave beenduetoMartin-Gruberanastomosis.
notrecordanynervecommunicationfromthemediantothe ulnarnerve.Theseresultsaresurprising,becausethey com-pletelydisagreewiththoseintheliterature,consideringthat theyshowulnar–mediananastomosisasbeingmorefrequent thanmedian–ulnar.
Amoiridis26 reported being surprised about the results publishedbyGolovchinsky,27whofoundthatnerve communi-cationfromtheulnarnervetothemediannervewaspresent in16.7%.ThisauthorstatedthatGolovchinsky27hadnottaken intoconsiderationsomebasicprinciplesof electrophysiologi-calstudiesandthatthiswaswhythepercentageofthistype ofnervecommunicationwassohigh.Inaddition,thisauthor statedthatGolovchinsky27hadnottakenintoconsideration thataresponsefromtheelbowtothewristdiminishedbyup to15%couldbefoundeveninnormalindividuals.
Komaret al.28 reportedthe caseofapatientwith com-pleterupture ofthemediannerve abovetheelbow, witha conditionofincompleteparalysisofthemediannerveinthe handandlossofsensitivityintheareaofsensoryinnervation bythemedian nerve.They reportedthat their electromyo-graphicevaluationsuggestedthatnervefibertransferfromthe ulnarnervetothemediannerveintheforearmwaspresent. AmoiridisstatedthatthiscasedescribedbyKomarwasnot oneofnervecommunicationintheforearm,since stimula-tioninthewristdidnotshowaresponsefromthemusclesin thethenarregion.WeagreewithAmoiridis,sinceitislikely thattransferoffasciclesfromtheulnartothemediannerve occurreddistallytothewrist(Cannieu-Richéanastomosis).
Streib29reportedthecaseofa77-year-oldpatientwitha complaintofweakness inthehands.Electricalstimulation demonstrated thatthe response ofthemusculature ofthe thenarregionhadanamplitudegreaterthan50%whenthe mediannervewasstimulatedinthewrist,inrelationtothe elbow.Theoppositeoccurredinrelationtotheulnarnerve, i.e.theamplitudewas50%greaterintheelbow.Thereisno doubtthatinthiscase,nervecommunicationoccurredinthe forearm(Martin-Gruberanastomosis).
Doganetal.30describedthecaseofapatientwitha con-dition of compressive neuropathy ofthe ulnar nerve who presentedalteredsensitivityintheringfingerandlittlefinger, butwithatrophyoftheshortabductormuscleofthethumb. Theyattributedthisfindingtoananomalyofinnervationof theshortabductor.
ThemainclassicaltreatisesdescribeMartin-Gruber anas-tomosisasnervecommunicationintheforearmbetweenthe medianandulnarnerves,butdonotmentioneithertheorigin orthedestinationofthenervefibers.
Conclusion
Knowledge of the anatomical variations relating to inner-vationofthehand isparticularlyimportantwithregard to performingphysicalexaminations,makingdiagnoses, deter-miningtheprognosisandimplementingsurgicaltreatment. Ifthesevariationsarenotgiventheirpropervalue,errorsand consequenceswillbeinevitable.
Nerve communications between the median and ulnar nerves may cause alterations to clinical symptoms, espe-ciallyinpatientswithcarpal tunnelsyndrome,sincethese
variations mayexacerbate orattenuatethe symptoms and cause motor and sensory alterations that differ from the usualpattern.Clinically,variationsinmotorinnervationare very important, inthat evenwithcomplete rupture ofthe medianorulnarnerve,someofthesemusclesmaynot nec-essarilybecomeparalyzed.Suchsituationscouldleadtothe wrongconclusionthatthenervehadnotbecomecompletely severed. Itis essentialto differentiatebetween partialand totalrupture.However,correctidentificationofthesevariables is notalways easy, sincerigorous clinical and electromyo-graphicexaminationisneeded. Alterationsrecorded inthe electroneuromyographicexaminationwithoutclinical proof areinsufficientforindicatingasurgicalprocedure.Careful dis-sectionduringthesurgicalproceduremaypreventinjurytoan anastomoticramus.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HighetWH.Innervationanfunctionofthethenarmuscles. Lancet.1943;241(6234):227–30.
2.ForrestWJ.Motorinervationofhumanthenarand hypothenarmusclesin25hands:astudycombining electromyographyandpercutaneousnervestimulation.CanJ Surg.1967;10(2):196–9.
3.MartinR.TalomNerversallmannaEgenskaperiManniskans Kropp.Stockholm:LasSalvius;1763.
4.GruberW.Ueberdieverbindungdesnervusmedianusmit demnervusulnarisamunteramedesmenschenumder saugethiere.ArchPhysiol.1870;37(2):501–22.
5.SunderlandS.Nerviosperiféricosysuslesiones.2ed. Barcelona:Salvat;1985.
6.SalaE.Studioelletromiograficodellinervazionedeimusculi flessrebreveedopponentdlpolice.RivPatNervMent. 1958;80:131–47.
7.HarnessD,SekelesE.Thedoubleanastomoticinnervationof thenarmuscles.JAnat(London).1974;117:329–31.
8.RosenAD.Innervationofthehand:anelectromyographic study.ElectromyogrClinNeurophysiol.1973;13(2):175–8. 9.ThomsonA.Thirdannualreportofcommitteeofcollective
investigationofanatomicalsocietyofGreatBritainand Irelandfortheyear1891–92.JAnatPhysiol.1893;27:183–94. 10.HirasawaK.Untersuchugenuberdasperipherenervensysten,
plexusbrachialisunddiennervenderobernextremitat.Arb AnatInstKaiserlichenUnivKyoto.1931;1(2):135–40.
11.KimuraJ,MurphyMJ,VaradaDJ.Electrophysiologicalstudyof anomalousinnervationofintrinsichandmuscles.Arch Neurol.1976;33(12):842–4.
12.SirinivasanR,RhodesJ.Themedianulnaranastomosis (MartinGruber)innormalandcongenitallyfetuses.Arch Neurol.1981;38(7):418–9.
13.UchidaY,SugiokaY.ElectrodiagnosisofMartinGruber connectionanditsclinicalimportanceinperipheralnerve surgery.JHandSurgAm.1992;17(1):54–9.
14.NakashimaT.AnstudyontheMartinGruberanastomosis. SurgRadiolAnat.1993;15(3):193–5.
Martin-Grubercommunicatingbranch:anatomicaland histologicalstudy.SurgRadiolAnat.1999;21(2):115–8. 17.Rodriguez-NiedenfuhrM,VazquezT,ParkinI,LoganB,
SanudoJR.Martin-Gruberanastomosisrevisited.ClinAnat. 2002;15(2):129–34.
18.LeeKS,OhCS,ChungIH,SunwooIN.Ananatomicstudyof theMartin-Gruberanastomosis:electrodiagnostic
implications.MuscleNerve.2005;31(1):95–7.
19.ShaficA,MoussalenC,StaffordJ.Cubitaltunnelsyndrome presentingwithcarpaltunnelsymptoms:clinicalevidence forsensoryformediantoulnarnervecommunication.AmJ Orthop.2009;38(6):104–6.
20.MarinacciA.Theproblemofunusualanomalousinnervation ofhandmuscles.Thevalueofelectrodiagnosisinits evaluation.BullLosAngelesNeuroSoc.1964;29:133–42. 21.ClifftonEE.Unusualinnervationoftheintrinsicmuscleofthe
handbymedianandulnarnerve.Surgery.1948;23(1):12–31. 22.CaetanoEB.Contribuic¸ãoaoestudodainervac¸ãodos
músculosdaregiãotenaredaanastomosedeCannieue Riché[tese].Sorocaba(SP):CentrodeCiênciasMédicase Biológicas–PUCSP;1982.
anómaladelamano.RevNeurol.2001;32(2):112–8. 24.BrandsmaJW,BirkeJA,SimsDSJr.TheMartin-Gruber
innervatedhand.JHandSurgAm.1986;11(4):536–9.
25.RosénB,LundborgG.Sensoryre-educationafternerverepair: aspectsoftiming.HandchiMikrochirPlasticChir.
2004;36(1):8–12.
26.AmoiridisG.Frequencyofulnar-to-mediannerve anastomosis[carta].EletromyogrClinNeurophisiol. 1992;32(4–5):255–6.
27.GolovchinskyV.Ulnar-to-mediananastomosisanditsrolein thediagnosisoflesionsofthemediannerveattheelbowand thewrist.ElectromyogrClinNeurophysiol.1990;30(1):31–4. 28.KómárJ,SzegváriM,GloviczkyZ,SzántóA.Traumaticsection
ofthemediannervewithoutcompletemotorparesis:the Martin-Gruberanastomosis.Nervenarzt.1978;49(12):697–9. 29.StreibEW.Ulnar-to-mediannerveanastomosisinthe
forearm:electromyographicstudies.Neurology. 1979;29(11):1534–7.