SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Surgical
treatment
of
femoroacetabular
impingement
using
controlled
hip
dislocation
after
occurrence
of
slipped
capital
femoral
epiphysis
夽
Weverley
Rubele
Valenza
∗,
Jamil
Faissal
Soni,
Christiano
Saliba
Uliana,
Fernando
Ferraz
Faria,
Gisele
Cristine
Schelle,
Daniel
Sakamoto
Sugisawa
UniversidadeFederaldoParaná,HospitaldoTrabalhador,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received21March2015 Accepted5October2015 Availableonline4July2016
Keywords:
Femoroacetabularimpingement Osteochondroplasty
Hipdislocation Hipjoint
a
b
s
t
r
a
c
t
Objective:Topresentourexperienceandpreliminaryresultsfromusingcontrolledhip dis-locationtotreatcam-likefemoroacetabularimpingement,inteenagersandyoungadults withsequelaeofslippedcapitalfemoralepiphysis.
Methods:Thiswasaretrospectiveanalysison15patientswhoweretreatedinatertiary-level hospitalbetween2011and2013.Thefollowingdatawerecollectedforanalysisfromthese patients’files:demographic data,surgicalprocedurereports,jointmobilityevaluations, patients’perceptionsregardingclinicalimprovementandwhethertheywouldchooseto undergotheoperationagain,previoushipsurgeryandcomplications.Theexclusioncriteria were:follow-upshorterthansixmonths,thepresenceofanyotherhipdisease,osteotomyof theproximalfemurperformedatthesametimeastheosteochondroplastyandincomplete medicalfileswithregardtotheinformationneededforthepresentstudy.
Results:Fifteenpatients(17hips)whounderwentosteochondroplastytotreat femoroac-etabularimpingementwereevaluated.Nineofthemwerewomen,themeanagewas18 yearsoldandtheminimumfollow-upwastwoyears.Twopatientsunderwent osteochon-droplastybilaterally;eightpatientswereoperatedontheleftsideandfiveontherightside. In14cases,thegreatertrochanterwaslowered(relativelengtheningoftheneck)in asso-ciationwiththeosteochondroplasty.For13patients,theirprevioussurgeryconsistedof fixationofanoccurrenceofslippedcapitalfemoralepiphysis;forsixpatients(eighthips), flexorosteotomywasperformedpreviously;andforonepatient,hiparthroscopywas per-formedpreviously.Fourteenpatientspresentedimprovementofmobilityandhippainrelief, incomparisonwithbeforetheoperation,andtheysaidthattheywouldundergothe opera-tionagain.Twocomplicationswereobserved:oneoflooseningofthefixationofthegreater trochanterandoneofheterotopicossification.
夽
StudyconductedatUniversidadeFederaldoParaná,HospitaldoTrabalhador,Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](W.R.Valenza). http://dx.doi.org/10.1016/j.rboe.2015.10.013
Conclusion:Thepreliminaryresultsfromthisstudysuggestthatosteochondroplastythrough controlledsurgicalhipdislocationisagoodoptionfortreatingfemoroacetabular impinge-ment.Throughthismethod,thepatientsreportedachievingimprovementofjointmobility andhippain,withfewcomplications.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Tratamento
cirúrgico
do
impacto
femoroacetabular
pós-
epifisiólise
pelo
método
da
luxac¸ão
controlada
do
quadril
Palavras-chave:
Impactofemoroacetabular Osteocondroplastia Luxac¸ãodoquadril Articulac¸ãodoquadril
r
e
s
u
m
o
Objetivo: Relatarnossaexperiênciaeosresultadospreliminarescomaluxac¸ãocirúrgica controladadoquadrilnotratamentodoimpactofemoroacetabular(IFA)tipoCAMem ado-lescenteseadultosjovenscomsequeladeepifisiólisefemoralproximal.
Métodos: Análiseretrospectivade15pacientestratadosemhospitalterciário,ondeforam selecionadosprontuáriosdepacientesquefizeramoprocedimentode2011até2013.Os dadoscoletadosparaanáliseforam:dadosdemográficos,descric¸ãodoprocedimento cirúr-gico,avaliac¸ãodamobilidadearticular,impressãosubjetivadopacientenoqueserefereà melhoriaclínicaeseoptariamporfazeracirurgianovamente,cirurgiasanterioresnoquadril ecomplicac¸ões.Foramexcluídospacientescomseguimentomenordoqueseismeses, por-tadoresdeoutrasdoenc¸asdoquadril,submetidosa osteotomiasdofêmurproximalno mesmomomentodaosteocondroplastiaecujoprontuárioestivesseincompletoquantoàs informac¸õesnecessáriasparaopresenteestudo.
Resultados:Foramavaliados15pacientese17quadrissubmetidosaosteocondroplastiapara otratamentodoIFA,novepacienteseramdosexofeminino,médiade18anoseseguimento mínimodedoisanos.Quantoàlateralidade,oitopacientesforamoperadosdoladoesquerdo ecincodoladodireito,alémdedoispacientesnosquaisaosteocondroplastiafoifeitade formabilateral.Em14 casos,abaixamentodotrocântermaior(alongamentorelativodo colo)foiassociadoàosteocondroplastia.Trezepacientestinhamcomocirúrgiapréviaa fixac¸ãodaepifisiólise,emseis(oitoquadris)foifeitaosteotomiaflexorapréviaeumfez umaartroscopiadoquadril.Em14pacienteshouvemelhoriadamobilidadeedadorno quadril,quandocomparadacomopré-operatório.Esses14pacientesrelataramquefariam acirurgianovamente.Foramobservadasduascomplicac¸ões,umasolturadafixac¸ãodo trocântermaioreumaossificac¸ãoheterotópica.
Conclusões: Osresultadospreliminaresdeste estudosugeremqueaosteocondroplastia pelatécnicadaluxac¸ãocirúrgicacontroladadoquadriléumaboaopc¸ãonotratamentodo impactofemoroacetabular.Poressemétodoospacientesrelatarammelhoriadamobilidade articularedornoquadriletiverampoucascomplicac¸ões.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
SlippedCapitalFemoralEpiphysis(SCFE)(epiphysiolysis)isa conditionthataffectspre-adolescentsandadolescents with-out a definite cause. In moderate and severe grades, this pathologycauseschangesintheepiphysisand thefemoral neckshape,andcanpredisposefemoroacetabular impinge-ment (FAI). This impingement predisposes biomechanical changes,pain, and deteriorationofthe acetabulararticular cartilage.Inturn,thesefactorsmayincreasetheriskofearly hiposteoarthritis.
Recently, controlled surgical dislocation of the hip was showntobeanappropriatemethodfortreatingFAI,providing
improvementsinhippainandmobility,aswellaspreventing arthrosis.1,2Thistechnique,initiallydescribedbyGanzetal.,3 isbasedontheanatomicalknowledgeofthepreservationof themedialfemoralcircumflexarterypathway,4allowingfor anexcellentvisualizationofthefemoralepiphysisand acetab-ulum,andthusminimizingtheriskofavascularnecrosis.It alsoallows,whennecessary,correctionoftheextra-articular impingement,throughfemurosteotomiesanddistaltransfer ofthegreatertrochanter.5
Material
and
methods
This study retrospectively included patients with FAI sec-ondary to SCFE, in which an osteochondroplasty was performedusingthecontrolledhipdislocationmethod.
Datawerecollectedthroughanalysisofmedicalrecords. Patientswithaminimumfollow-up ofsixmonths,who were previously diagnosed with SCFE and underwent this technique,wereincluded.
Exclusion criteriacomprised patientswith less than six monthsoffollow-up; diagnosis ofFAIcaused byother hip pathologies;patientswhounderwentosteotomyofthe prox-imalfemuratthesametimeofosteochondroplasty;patients withhip osteoarthritis (Tonnis0),as thisis arelative con-traindicationfortheprocedure;andpatientswhosemedical recordswereincompleteorwerelosttofollow-up.
Allsurgerieswereperformedbythesamesurgeon. Surgi-caltechniquecomprisedposterolateralaccess,osteotomyof thegreatertrochanter,preservationoftherotatormusclesand theobturatorinternustendon,anteriorT-shapedcapsulotomy (thisisanalterationinthetechniquedescribedbyGanz,3who performed a Z-shaped capsulotomy,which does not inter-ferewithfemoralneckexposure,labrum,andacetabulum), anterior dislocationof the hip, complete exposition ofthe epiphysisandfemoralneck, chondrosternoplasty, impinge-mentremoval,andacetabularinspectiontoassesschondral injuryanddamagetotheacetabularlabrum.After osteochon-droplasty,therangeofmotionofthehipwastested;control wasconductedwithanimageintensifiertoassesstheabsence ofimpingement.
Subsequently, capsule was sutured and the greater trochanterwasfixedwithtwoorthree4.5-mmcorticalscrews. In cases wherethe greater trochanter was raised, causing trochantericimpingement,atransferwasmade,withdistal fixationofthetrochanter(arelativelengtheningofthefemoral neck)(Figs.1–4).
Postoperatively,fullweightsupportonthelimbwasnot allowedforameanofsixweeks,whichistheestimatedtime forconsolidationofthegreatertrochanter.Physicaltherapy wasstartedfromthefirstpostoperativedayaimingtoincrease rangeofmotion.
Thedatacollectedforanalysisweresex(gender),ageat timeofsurgery,theaffectedside,dateofsurgery,description
Fig.1–X-rayinanteroposterorincidenceofapatientwith FAI,afterinsitufixationofSCFE.
Fig.2–X-rayinprofileofapatientwithFAI,afterinsitu
fixationoftheSCFE.
of the surgical procedure, previous hip surgery, subjective impression of the patient regarding clinical improvement (mobilityandpain)andwhethertheywouldchoosetohave surgeryagain,andcomplicationsrelatedtothisprocedure.
Complications were determined in accordance with the adaptationproposedbySinketal.6oftheclassificationof sur-gicalcomplicationsbyClavien7andDindoetal.,8asdescribed below:
Fig.4–X-rayinprofile,sixmonthspostoperatively.
Sinketal.6classification:
GradeI:requiresnochangeinthepost-operative manage-ment.
GradeII:requireschangeinthepost-operativemanagement. GradeIII:requiresurgicalorradiologicalmanagement. GradeIV:associatedwithlong-termmorbidity. GradeV:death.
ThecollecteddatawereevaluatedusinganExcel® spread-sheet.
This study was approved by the Research Ethics Com-mitteeoftheinstitutionunderthefollowingnumber:CAAE: 30485814.4.0000.5225.
Results
FromFebruary2011toDecember2013,15patients(17hips) underwentosteochondroplastytotreatFAI secondarytoSCFE. Minimumfollow-upwasoftwoyearsandmaximumoffour yearsandsixmonthsinthelastclinicalandradiographic eval-uation.
Ninepatientswerefemale.Twopatientsunderwent bilat-eralosteochondroplasty;ineight,ontheleftside;andinfive, ontherightside.Ageatsurgeryrangedfrom14to26years, withameanof18years.In14hips,inadditiontothe osteo-chondroplasty,adistaltransferofthegreatertrochanterwas performed(relativelengtheningofthefemoralneck).Previous surgeriestotreatSCFEwereinsitufixationin13patients(15 hips);insixpatients(eighthips),flexionosteotomy;andone patienthadundergonearthroscopy(Table1).
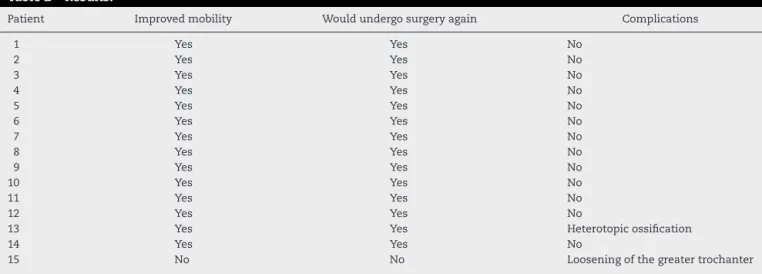
As a subjective impression of the patients, 14 reported improvementsinjointmobilityandpainwhencomparedwith preoperative period. These same 14 patients reported that theywouldundergosurgeryagain.
ThelastcontrolX-raysofthe15patients–atleasttwoyears aftersurgery–showednosignsofcoxarthrosis.Two complica-tionswereobserved:onelooseningofthegreatertrochanter fixation,whichwasnottreatedandevolvedinto pseudarthro-sis,classifiedastypeIII/IV bythecriteriaofSinketal.6(type III,complicationthatrequiressurgicalintervention,andtype
IV,long-termsequelae).Otherwasoneheterotopic
ossifica-tion,classifiedastypeI (complicationthatdoesnotchange the postoperativecourse,withoutclinical relevance).Inthe
Table1–Epidemiology,associatedandpriorsurgeries.
Patient Sex Side Ageatsurgery Trochanterlowering Priorsurgery
1-A Female Bilateral–R 19 No insitufix.,flex.ost.
1-B Female Bilateral–L 17 Yes insitufix.,flex.ost.
2-A Male Bilateral–R 26 Yes insitufix.,flex.ost.
2-B Male Bilateral–L 23 No insitufix.,flex.ost.
3 Female Left 14 Yes insitufix.
4 Female Right 25 Yes insitufix.,flex.ost.
5 Female Left 17 Yes insitufix.
6 Male Left 17 Yes No
7 Female Left 16 Yes insitufix.
8 Male Right 19 Yes insitufix.
9 Female Left 17 Yes insitufix.
10 Male Left 16 Yes No
11 Male Left 15 Yes insitufix.,flex.ost.
12 Male Right 16 Yes insitufix.
13 Female Right 20 Yes insitufix.,flex.ost.
14 Female Right 22 No insitufix.,arthro.
15 Female Left 17 Yes insitufix.,flex.ost.
Table2–Results.
Patient Improvedmobility Wouldundergosurgeryagain Complications
1 Yes Yes No
2 Yes Yes No
3 Yes Yes No
4 Yes Yes No
5 Yes Yes No
6 Yes Yes No
7 Yes Yes No
8 Yes Yes No
9 Yes Yes No
10 Yes Yes No
11 Yes Yes No
12 Yes Yes No
13 Yes Yes Heterotopicossification
14 Yes Yes No
15 No No Looseningofthegreatertrochanter
presentstudy,nocasesofavascularnecrosis,femoralneck fractures,andsciaticnerveinjurywereobserved(Table2).
Discussion
FAI hasbeen described as a series ofanatomical changes in the hip, which may be located in the femoral epiph-ysis(CAM),intheacetabulum(PINCER),orcombined.These deformities cause damage to the acetabular labrum and acetabularcartilage,thereforeleadingtohipdegeneration.9,10 Astheseabnormalitiesprogress,theycausepainanddecrease hipfunction.Inthemedicalliterature,severalstudies have demonstratedthatFAI isoneofthemaincausesofsecondary hiposteoarthrosis.9–14
Hipswithsequelaefromchildhoodandadolescence dis-eases,suchasLegg-Calve-PerthesdiseaseandSCFE,develop seriousandcomplexdeformities;theirresolutionwithlimited accessorhiparthroscopyisdifficult.Inthesecases,surgical dislocationprovidesawideaccesstothefemoralepiphysis,to thetransitionfromthenecktothefemoralhead,andtothe acetabulum,allowingforthetreatmentoflabraltear, osteo-chondroplasty,redirectionalosteotomy,anddistaltransferof the greater trochanter (relative lengtheningof the femoral neck).15
Anotheroptioninthisapproach,oftenmentionedinthe literature, is femoral intra- or extracapsular osteotomies. However,long-term studiesthat assessedintertrochanteric osteotomyforthetreatmentofSCFEsequelaewithoutfemoral neckosteochondroplastywerenotsuccessfulintheirattempt tochangethenaturalcourseofcoxarthrosis.15,16
Inthepresentstudy,ninefemalepatientswereincluded; theliteratureindicatesahigherincidenceofSCFEinmales. Thiscanbeexplainedbythefactthatthepresentstudydidnot showtheincidenceofepiphysiolysis,butratherthepatients intheclinicwhohadSCFEandFAIcomplaints.
Inthepresentstudy,osteochondroplastieswereperformed using the controlled surgical hip dislocation technique in patientswithproximalfemoralepiphysiolysissequelae. Thir-teenhipshadbeenfixedwithcannulatedscrewstoprevent theprogressionoftheslip;eighthipshadundergoneflexion andderotationalintertrochantericosteotomyinanattempt
to improve mobility; and one patient had undergone an arthroscopyinordertotreattheCAM.
Prior to surgical treatment of FAI, these patients com-plained oflimitations inhip mobility. Thephysical exami-nationshowedapositiveimpingementtest(painonflexion, adduction,andinternalhiprotation)andX-raysalsoshowed signs of hip impingement; no hips had coxarthrosis sig-nals. Thus, osteochondroplasty withcontrolled dislocation wasindicated,withorwithoutdistaltransferofthegreater trochanter on the principle of femoral neck lengthening, whichwouldimprovetheabductormechanism.
Resultsobtainedwereimprovementinpainandespecially inmobility.Inthesubjectiveassessment,14patientswere sat-isfiedandreportedthattheywouldundergosurgeryagain.The contralateralsideprocedurewasperformedintwopatients, andonlyonepatientreporteddissatisfactionwiththeresult of the surgical procedure and would not undergo surgery again.
Thepresentresultsreflectthetrendindicatedinthe lit-erature,whichshowsasignificantimprovementinpainand mobilitywithosteochondroplastyusingthe described tech-niqueforFAI.6,10,15,17
However, althoughthesestudies showed good improve-mentintheshort-andmedium-term,thissurgicalprocedure andhiparthroscopyarerelativelyrecent;therefore,alonger follow-uptimeisnecessarytodeterminewhethertheychange thenaturalcourseofcoxarthrosis.5,10,17,18
Themostprevalentcomplicationsreportedinthis proce-dure are heterotopic ossification, avascular necrosisof the femoral head, sciatic nerve injury, pseudarthrosis of the greatertrochanter,femoralneckfractures,and thromboem-bolicdiseases(TEP,DVT);mostoftheseweredescribedinthe multicenterstudybySinketal.6
Asaclinical inference, it isreasonableto estimatethat longerfollow-up ofthepresent sampleisneededtoassess changeintheinstallationofhiparthrosis,aswellastoanalyze long-termresults.
Conclusions
The preliminary results of this study indicate that osteo-chondroplasty using the technique of controlled surgical hip dislocation isan option to treatFAI. Patients reported improvementsin hip mobility and pain. Thefew reported complicationsmayberelatedtothesteeplearningcurvefor thissurgicaltechnique.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. BediA,KellyBT.Femoroacetabularimpingement.JBoneJoint SurgAm.2013;95(1):82–92.
2. LeunigM,BeauléPE,GanzR.Theconceptof
femoroacetabularimpingement:currentstatusandfuture perspectives.ClinOrthopRelatRes.2009;467(3):616–22. 3. GanzR,GillTJ,GautierE,GanzK,KrügelN,BerlemannU.
Surgicaldislocationoftheadulthipatechniquewithfull accesstothefemoralheadandacetabulumwithouttherisk ofavascularnecrosis.JBoneJointSurgBr.2001;83(8): 1119–24.
4. GautierE,GanzK,KrügelN,GillT,GanzR.Anatomyofthe medialfemoralcircumflexarteryanditssurgical
implications.JBoneJointSurgBr.2000;82(5):679–83.
5. TiborLM,SinkEL.Prosandconsofsurgicalhipdislocationfor thetreatmentoffemoroacetabularimpingement.JPediatr Orthop.2013;33Suppl.1:S131–6.
6.SinkEL,BeauléPE,SucatoD,KimYJ,MillisMB,DaytonM, etal.Multicenterstudyofcomplicationsfollowingsurgical dislocationofthehip.JBoneJointSurgAm.
2011;93(12):1132–6.
7.ClavienPA,StrasbergSM.Severitygradingofsurgical complications.AnnSurg.2009;250(2):197–8.
8.DindoD,DemartinesN,ClavienPA.Classificationofsurgical complications:anewproposalwithevaluationinacohortof 6336patientsandresultsofasurvey.AnnSurg.
2004;240(2):205–13.
9.GanzR,ParviziJ,BeckM,LeunigM,NötzliH,SiebenrockKA. Femoroacetabularimpingement:acauseforosteoarthritisof thehip.ClinOrthopRelatRes.2003;(417):112–20.
10.ClohisyJC,StJohnLC,SchutzAL.Surgicaltreatmentof femoroacetabularimpingement:asystematicreviewofthe literature.ClinOrthopRelatRes.2010;468(2):555–64.
11.AronsonJ.Osteoarthritisoftheyoungadulthip:etiologyand treatment.InstrCourseLect.1986;35:119–28.
12.BeckM,KalhorM,LeunigM,GanzR.Hipmorphology influencesthepatternofdamagetotheacetabularcartilage: femoroacetabularimpingementasacauseofearly
osteoarthritisofthehip.JBoneJointSurgBr. 2005;87(7):1012–8.
13.BeckM,LeunigM,ParviziJ,BoutierV,WyssD,GanzR. Anteriorfemoroacetabularimpingement:partII.Midterm resultsofsurgicaltreatment.ClinOrthopRelatRes. 2004;(418):67–73.
14.GanzR,LeunigM,Leunig-GanzK,HarrisWH.Theetiologyof osteoarthritisofthehip:anintegratedmechanicalconcept. ClinOrthopRelatRes.2008;466(2):264–72.
15.RebelloG,SpencerS,MillisMB,KimYJ.Surgicaldislocationin themanagementofpediatricandadolescenthipdeformity. ClinOrthopRelatRes.2009;467(3):724–31.
16.SchaiPA,ExnerGU,HänschO.Preventionofsecondary coxarthrosisinslippedcapitalfemoralepiphysis:along-term follow-upstudyaftercorrectiveintertrochantericosteotomy.J PediatrOrthopB.1996;5(3):135–43.
17.SinkEL,KimYJ.Femoroacetabularimpingement:current clinicalevidence.JPediatrOrthop.2012;32Suppl.2:S166–71. 18.PhilipponMJ,PattersonDC,BriggsKK.Hiparthroscopyand