ContentslistsavailableatScienceDirect
Ageing
Research
Reviews
j o ur na l h o me p a g e :w w w . e l s e v i e r . c o m / l o c a t e / a r r
Review
Relationship
between
depression
and
frailty
in
older
adults:
A
systematic
review
and
meta-analysis
Pinar
Soysal
a,
Nicola
Veronese
b,c,
Trevor
Thompson
d,
Kai
G.
Kahl
e,
Brisa
S.
Fernandes
f,g,
A.
Matthew
Prina
h,
Marco
Solmi
c,i,j,
Patricia
Schofield
k,
Ai
Koyanagi
l,m,
Ping-Tao
Tseng
n,
Pao-Yao
Lin
o,p,
Che-Sheng
Chu
q,
Theodore
D.
Cosco
r,s,
Matteo
Cesari
t,u,
Andre
F.
Carvalho
v,
Brendon
Stubbs
h,k,w,∗aKayseriEducationandResearchHospital,GeriatricCenter,Kayseri,Turkey bNationalResearchCouncil,NeuroscienceInstitute,AgingBranch,Padova,Italy cInstituteofClinicalResearchandEducationinMedicine(IREM),Padova,Italy dFacultyofEducationandHealth,UniversityofGreenwich,London,UnitedKingdom
eDepartmentofPsychiatry,SocialPsychiatryandPsychotherapy,HannoverMedicalSchool,Carl-Neuberg-Str.1,30625Hannover,Germany fIMPACTStrategicResearchCentre,DeakinUniversitySchoolofMedicine,andBarwonHealth,Geelong,VIC,Australia
gLaboratoryofCalciumBindingProteinsintheCentralNervousSystem,DepartmentofBiochemistry,FederalUniversityofRioGrandedoSul,PortoAlegre, Brazil
hHealthServiceandPopulationResearchDepartment,InstituteofPsychiatry,PsychologyandNeuroscience,King’sCollegeLondon,DeCrespignyPark, London,BoxSE58AF,UnitedKingdom
iDepartmentofNeurosciences,UniversityofPadova,Padova,Italy jLocalHealthUnit17,MentalHealthDepartment,Padova,Italy
kFacultyofHealth,SocialCareandEducation,AngliaRuskinUniversity,Chelmsford,UnitedKingdom
lResearchandDevelopmentUnit,ParcSanitariSantJoandeDéu,UniversitatdeBarcelona,FundacióSantJoandeDéu,Dr.AntoniPujadas,42,SantBoide Llobregat,Barcelona08830,Spain
mInstitutodeSaludCarlosIII,CentrodeInvestigaciónBiomédicaenReddeSaludMental,CIBERSAM,MonfortedeLemos3-5Pabellón11,Madrid28029, Spain
nDepartmentofPsychiatry,Tsyr-HueyMentalHospital,KaohsiungJen-Ai’sHome,Taiwan
oDepartmentofPsychiatry,KaohsiungChangGungMemorialHospitalandChangGungUniversityCollegeofMedicine,KaohsiungCity,Taiwan pInstituteforTranslationalResearchinBiomedicalSciences,KaohsiungChangGungMemorialHospital,Kaohsiung,Taiwan
qKaohsiungVeteransGeneralHospital,KaohsiungCity,Taiwan
rMRCUnitforLifelongHealthandAgeingatUCL,33BedfordPlace,LondonWC1B5JU,UnitedKingdom sOxfordInstituteofPopulationAgeing,UniversityofOxford,66BanburyRoad,Oxford,OX26PR,UnitedKingdom tInsermUMR1027,UniversitédeToulouseIIIPaulSabatier,Toulouse,France
uGérontopôle,CentreHospitalierUniversitairedeToulouse,Toulouse,France
vTranslationalPsychiatryResearchGroupandDepartmentofClinicalMedicine,FacultyofMedicine,FederalUniversityofCeará,Fortaleza,CE,Brazil wPhysiotherapyDepartment,SouthLondonandMaudsleyNHSFoundationTrust,DenmarkHill,LondonSE58AZ,UnitedKingdom
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2February2017
Receivedinrevisedform7March2017 Accepted21March2017
Availableonline31March2017
Keywords: Depression Frail Geriatrics Olderadults Meta-analysis Psychiatry
a
b
s
t
r
a
c
t
Aim:Depressionandfrailtyareprevalentandburdensomeinolderage.However,therelationships betweentheseentitiesareunclearandnoquantitativemeta-analysisexists.Weconductedasystematic reviewandmeta-analysistoinvestigatetheassociationsbetweendepressionandfrailty.
Methods:TwoauthorssearchedmajorelectronicdatabasesfrominceptionuntilNovember-2016for cross-sectional/longitudinalstudiesinvestigatingdepressionandfrailty.Thestrengthofthereciprocal associationsbetweenfrailtyanddepressionwasassessedthroughoddsratios(ORs)adjustedforpotential confounders.
Results:From2306nonduplicatedhits,24studieswereincluded.Theoverallprevalenceof depres-sionin8023peoplewithfrailtywas38.60%(95%CI30.07–47.10,I2=94%).Thosewithfrailtywereat increasedoddsofhavingdepression(ORadjustedforpublicationbias4.42,95%CI2.66–7.35,k=11), alsoafteradjustingforpotentialconfounders(OR=2.64;95%CI:1.59–4.37,I2=55%,k=4).The preva-lenceoffrailtyin2167peoplewithdepressionwas40.40%(95%CI27.00–55.30,I2=97%).Peoplewith depressionwereatincreasedoddsofhavingfrailty(OR=4.07,95%CI1.93–8.55,k=8).ThepooledORfor incidentfrailty,adjustedforamedianof7confounders,was3.72(95%CI1.95–7.08,I2=98%,k=4),whilst intwostudiesfrailtyincreasedtheriskofincidentdepressionwithanOR=1.90(95%CI1.55–2.32,I2=0%).
∗Correspondingauthorat:PhysiotherapyDepartment,SouthLondonandMaudsleyNHSFoundationTrust,DenmarkHill,London,UnitedKingdom. E-mailaddress:[email protected](B.Stubbs).
Conclusion:Thismeta-analysispointstoareciprocalinteractionbetweendepressionandfrailtyinolder adults.Specifically,eachconditionisassociatedwithanincreasedprevalenceandincidenceoftheother, andmaybeariskfactorforthedevelopmentoftheother.However,furtherprospectiveinvestigations arewarranted.
©2017ElsevierB.V.Allrightsreserved.
Contents
1. Introduction...79
2. Materialsandmethods...80
2.1. Searchstrategy...80
2.2. Studyselection...80
2.3. Dataextraction...80
2.4. Outcomes...80
2.5. Assessmentofstudyquality...80
2.6. Statisticalanalysis...80
3. Results ... 80
3.1. Studyandparticipants’characteristics...81
3.2. Measurementoffrailty...81
3.3. Measurementofdepression...82
3.4. Cross-sectionalmeta-analysisfindings...82
3.4.1. Prevalenceofdepressioninpeoplewithfrailty...82
3.4.2. Oddsofdepressioninpeoplewithfrailtyversuscontrols...82
3.4.3. Prevalenceoffrailtyinpeoplewithdepression...82
3.4.4. Oddsoffrailtyinpeoplewithdepressionversuscontrols...83
3.5. Longitudinalmeta-analysisfindings...83
3.5.1. Studiesinvestigatingincidentfrailtyinolderpeoplewithdepression ... 83
3.5.2. Studiesinvestigatingincidentdepressionamongpeoplewithfrailty...83
4. Discussion...83
5. Limitations...85
Conflictofinterest...86
Financialdisclosure...86
AppendixA. Supplementarydata...86
References...86
1. Introduction
Frailtyanddepressionaretwocommonandpervasive medi-calconditionsamongolderadults.Theprevalenceofdepression inolderagerangesfrom10to20%(Roddaetal.,2011)andthe prevalence of frailty is estimated to be similar (Collard et al., 2012).Recentstudieshavesuggestedthat16–35%offrail individ-ualshave alsoexperiencedco-existing depression,and thatthe prevalenceofdepression infrail individualsis ashighas46.5% ınolderadults(Buiguesetal.,2015).Bothdepressionandfrailty areassociatedwitharangeofdeleteriousoutcomesinolderage suchaslower qualityof life(QOL), increaseduseof healthcare services,increased morbidity and mortality(Clegget al., 2013; FugateWoodsetal.,2005;Hareetal.,2014;Roddaetal.,2011). Furthermore,co-existingdepressionandfrailtyisassociatedwith particularlyworseoutcomessuchasacceleratedcognitive impair-mentanddisability(Potteretal.,2016).Thereareseveralreasons thatmay accountfor thehighlevelsofcommorbidity between depressionandfrailty.Oneistheoverlapinsomeareasofdiagnostic criteria,e.g.unintentionalweightloss,makingitdifficultto distin-guishfromeachother,particularlywithadvancingage.Another factoristhatdepressionandfrailtyhavesomecommonetiology thatmakesdisentanglementdifficult(Brownetal.,2014).Giventhe highlevelsofdepression(Buiguesetal.,2015)andfrailty(Soysal etal.,2016)inolderageandthedeleteriousoutcomeswhenthey co-exist,understandingtherelationshipbetweenthesefactorsis ofutmostimportance.
Despitethepublichealthimportance,theprevalenceand inci-denceofdepressionamongpeoplewithfrailtyandtheopposite
relationship is largelyunknown.The convergence of thefrailty anddepressionspectruminmid-andlate-lifealsogiverisetothe hypothesisof‘overlappingsyndromes’(Katz,2004),withpossible biologicalmechanismsaccountingforbothsyndromes(Vaughan etal.,2015).Mostevidencetodatesuggeststhatthefrailtyand depressioncriteriaconsistofahighlyoverlappingbutdistinct sub-population(Mezuketal.,2013);moreover,theassociationbetween thetwoconstructscannotbefullyexplainedbytheoverlapping oftheirsymptoms(Lohman,2013)sofrailtyanddepressionmust beconsideredinterrelatedratherthanoverlappingsyndromes.To date,previousnarrativeand/orselectivereviewshavesuggested theremaybearelationshipbetweenfrailtyanddepression(Brown et al., 2016; Buigues et al., 2015; Mezuket al., 2012; Benraad etal.,2016;Dreyetal.,2011).Forinstance,oneprevious narra-tivesystematicreview(Vaughanetal.,2015)suggestedthatthe co-occurrenceofdepressionand frailtywasgreaterthan10%in olderadults ≥55years old,but notedthat thereis considerable variationintheestimatesandameta-analysiswasnotconducted. Todate,tothebestofourknowledge,nometa-analysishasbeen conductedtoconsidertherelationshipbetweendepressionand frailty.
2. Materialsandmethods
This systematic review was conducted according to the Strengthening the Reporting of Observational Studies in Epi-demiology [STROBE] criteria (von Elm et al., 2008) and the recommendationsinthePreferredReportingItemsforSystematic Reviewsand Meta-Analyses[PRISMA]statement(Liberatietal., 2009).Thereviewfollowedapredetermined,butunpublished pro-tocol.
2.1. Searchstrategy
Twoindependentauthors(BSandNV)searchedMedline(via Ovid), Psychinfo and EMBASE for studies from inception until 11/2016withnolanguagerestrictions.Thesearchtermsusedwere (frailtyorfrail*)and(depress*ordepressiveormajordepressive disease).Conferenceabstractswerealsoincludedandtheauthors werecontactedforobtainingmissinginformationatleasttwotimes inamonth.
2.2. Studyselection
Includedstudieswerepublishedquantitativestudiesofacross sectionalorlongitudinaldesignthat:(1)Reportedtheprevalence orincidenceof frailty<--->depression in olderadults witha meanage over 60 years and older;(2) Capturedfrailtywith a recognizedcriteria (e.g.Fried’s criteria (Fried et al., 2001)); (3) Captureddepressionaccordingtostructuredinterviewdiagnostic criteria(e.g.DSMandmajordepressivedisorder(MDD))or depres-sivesymptomswithavalidateddepressionscreeningmeasure(e.g. CenterforEpidemiologicStudiesDepressionScale(CES-D)(Radloff, 1977))(henceforthcalled‘depression’,althoughwherepossiblein theresultswedifferentiatebetweenMDDanddepressive symp-toms);and(4) includeda controlgroup(pre-frailandrobustas separateentitiesortogether).
Studieswereexcludedifthey(1)didnotuseaclear diagnos-ticcriteriaforfrailtyoronlyusedoneitemforitsdiagnosis(e.g. lowgaitspeed)or (2)reporteddepression withanunvalidated screeningtoolormeasure.
2.3. Dataextraction
Twoauthors(NV,PS)independentlyextracteddatafromthe selectedstudies in a standardized Microsoft Excel spreadsheet. Anydisagreementwasresolvedbyconsensuswithathirdauthor (BS).Thefollowinginformationwasextracted:1)characteristics ofthestudypopulation(e.g.samplesize,demographics,country inwhichthestudywasperformed);2)settinginwhichthestudy wasperformed;3)diagnosticcriteriaforfrailtyanddepression;4) demographiccharacteristics(meanageandpercentageofwomen) byfrailtyanddepressionstatus;5)typeandnumberofadjustments inthemultivariateanalyses(forlongitudinalstudies);6)follow-up period(onlyforlongitudinalstudies).
Ifwerequiredadditionaldatatoeitherconfirmorenablestudy inclusion,wecontactedtheprimaryauthorsuptothreetimesover amonthperiod.
2.4. Outcomes
The primary outcomes were a) the prevalence and comor-bidoddsofdepression/depressivesymptomsinfrailtyandb)the prevalenceand comorbidoddsoffrailtyinpeoplewith depres-sion/depressivesymptoms.Inaddition,wecalculatedtheincidence ofc)depression/depressivesymptomsonsetinpeoplewithfrailty, andd)frailtyonsetinpeoplewithdepression/depressive symp-toms.
2.5. Assessmentofstudyquality
Studyqualitywasassessedbytwoinvestigators(PS,BS)using theNewcastle-Ottawa Scale (NOS) (Wells et al., 2012). A third reviewerwasavailableformediation(NV).TheNOSassignsa max-imumof 9pointsbased onthree qualityparameters:selection, comparability,andoutcome(Wellsetal.,2012).
2.6. Statisticalanalysis
Analyseswereperformedbytwoindependentinvestigators(BS, NV)using ComprehensiveMeta-Analysis (CMA) 3(http://www. meta-analysis.com).Duetotheanticipatedheterogeneity,a ran-dom effects meta-analysis was undertaken. The analyseswere conductedinthefollowingsteps.First,theprevalenceofdepression amongpeoplewithfrailtytogetherwith95%confidenceintervals (CIs)wascalculated.Second,theoddsratioand95%CIoffrailty amongpeoplewithandwithoutdepressionwascalculated.Third, theprevalenceoffrailtyamongpeoplewithdepressionand95%CI wascalculated.Fourth,theoddsratioand95%CIoffrailtyamong peoplewithandwithoutdepressionwascalculated.Foreachofthe aboveanalyses,whenpossible,weconductedsubgroupanalyses investigatingdifferencesaccordingtogeographicalregion,study setting, depression classification(structured clinical assessment versusscreeningmeasure)andfrailtymeasure(e.g.Friedcriteria versusothers)(Friedetal.,2001).Whereavailable,adjusted esti-matesoftheassociationbetweenfrailtyanddepression (orthe contrary)wereextractedandpooledasORs.Finally,ORsadjusted forthemaximumnumberofcovariatesavailableforeachstudy wereusedtoassesstheassociationbetweenfrailty(ordepression) atthebaselineandincidentdepression(orfrailty)atfollow-up.
StudyheterogeneitywasmeasuredusingtheCochran’sQand I-squaredstatistics,assumingthata p≤0.10 fortheformer and a value≥50%for thelatterindicated asignificantand substan-tialheterogeneity(HigginsandThompson,2002).Givensignificant heterogeneity,ameta-regressionanalysiswasperformedusing dif-ferencesinmeanage,bodymassindex(BMI)andpercentageof females amonggroups (frail,pre-frail,robust)asmoderators in singlemetaregression.Publicationbiaswasassessedbyvisually inspectingfunnelplots,andtoaccountforpublicationbias,weused theDuvalandTweedietrim-and-fillmethod(DuvalandTweedie, 2000),basedontheassumptionthattheeffectsizesofallthe stud-iesarenormallydistributedaroundthecenterof afunnelplot; intheeventofasymmetries,itadjustsforthepotentialeffectof unpublishedstudies.
3. Results
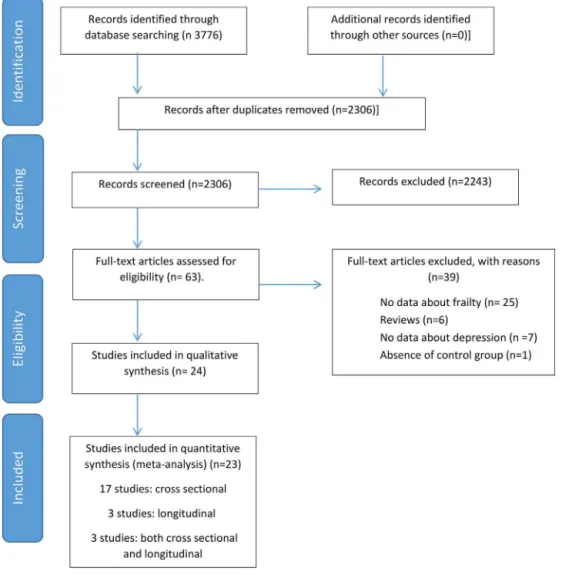
Thesearchidentified2306non-duplicatedpotentiallyeligible studies.Followingadetailedreviewoftitleandabstracts,atotal of63fulltextarticleswerereviewed.Theeligibilitycriteriawere appliedand 39 articles wereexcluded (reasons summarized in
Fig.1. PRISMAflow-chart.
etal.,2016)didnotcontainanydatathatcouldbeincludedinthe meta-analysis.
3.1. Studyandparticipants’characteristics
Studyandparticipants’characteristicsofcross-sectionalstudies are summarized in SupplementaryTables 1 and 2. The major-ity of the studies were conducted among community-dwellers (n=19 (79.1%))and in North America (n=12 (50.0%)),followed byEurope(n=4),Asia(n=3),Australia(n=3),andLatinAmerica (n=2).(SupplementaryTable1).Theoverallqualityofthestudies, assessedthroughNOS,wasgenerallygoodwithamedianscore=8 (range=5–9)(FulldetailsareavailableinSupplementaryTable5). Overall12cross-sectionalstudies(Jarschiketal.,2012;Pegorari andTavares,2014;Fengetal.,2014;Matheusetal.,2016;Dentand Hoogendijk,2014;Changetal.,2010;Sanchez-Garciaetal.,2014; PatriciodeAlbuquerqueSousaetal.,2011;Friedetal.,2001;Fugate Woodsetal.,2005;Jungetal.,2016; McAdams-DeMarcoetal., 2016)investigatedtheprevalenceofdepressioninfrailtyincluding atotalof8023frailolderparticipantswithameanageof74.6years, ofwhom94.0%werefemale.Theseparticipantswerecompared with45,775participantswithnofrailty(meanage:70.2;88.1% females).Furthermore,the8crosssectionalstudiesinvestigating theprevalenceoffrailtyinpeoplewithdepression(Collardetal., 2014;Lohmanetal.,2016;Almeidaetal.,2015;Brownetal.,2014;
Lohmanetal.,2014;Mezuketal.,2013;PaulsonandLichtenberg, 2013;Almeidaetal.,2016)included2164depressedolderadults
withameanageof69.3years,66.5%ofwhichwerefemales.These subjectswerecomparedwith14,932subjectswithnodepression. Inaddition,therewere311frailolderadultsinthe3 longitudi-nalstudies(Fengetal.,2014;Makizakoetal.,2015;Moninetal., 2016)(meanage75.1,39.1%females)investigatingtheincidenceof depressionoverameanfollowupof4.67years.Thesesubjectswere comparedwith5801subjectswithnofrailtyatbaseline.Finally, therewere6404depressedolderadultsin4longitudinalstudies (FugateWoodsetal.,2005;PaulsonandLichtenberg,2013;Lakey etal.,2012;Hajeketal.,2016)thatinvestigatedtheincidenceof frailtyoverameanfollowupof2.87years.Theseparticipantswere comparedwith51,610participantswithnodepression (Supple-mentaryTables3and4).
3.2. Measurementoffrailty
Table1
Meta-analysisresultsofprevalenceandoddsofdepressioninolderpeoplewithfrailty.
Analysis Numberof study estimates
Numberof participants
Meta-analysis Between groupp value
Trimandfilleffect size(95%CI) [adjustedstudies]
I2
Prevalenceofdepressioninolderpeoplewithfrailty
Prevalence 95%CI
Mainanalysis 11 8023 38.60% 30.07 47.10 Unchanged 94
Geographicalregion 0.751
NorthAmerica 5 7478 41.08% 29.02 54.31 Unchanged 97
Asia 2 211 34.63% 17.57 56.83 N/A 46
Europe 2 147 30.12% 14.93 51.44 N/A N/A
LatinAmerica 2 190 44.02% 24.78 65.24 N/A N/A
StudySetting 0.737
Community 10 7830 39.00% 30.05 48.13 Unchanged 94
Communityandinpatients 1 96 34.02% 13.84 62.32 N/A N/A
Depressionoutcome 0.737
Screeningmeasure 10 7830 39.00% 30.05 48.13 Unchanged 94
Structuredinstrument 1 96 34.02% 13.84 62.32 N/A N/A
Frailtymeasure <0.001
Fried 10 1302 40.04% 33.60 47.60 Unchanged 83
WHI-OS 1 6619 26.16% 12.98 45.70 N/A N/A
Oddsofdepressioninolderpeoplewithfrailty
OR 95%CI
Mainanalysis 11 53626 3.94 2.36 6.58 <0.001 4.42(2.66–7.35)[1] 96
Geographicalregion 0.312
NorthAmerica 5 49181 6.700 2.92 15.34 <0.001 Unchanged 98
Asia 2 2207 4.582 1.24 18.92 0.02 N/A 69
Europe 2 889 1.298 0.23 7.12 0.763 N/A N/A
LatinAmerica 2 1349 2.437 0.45 13.12 0.299 N/A N/A
StudySetting 0.28
Community 10 53260 4.420 2.57 7.65 <0.0001 4.99(2.93–8.51)[1] 96 Outpatientsandinpatients 1 366 1.240 0.24 6.20 0.86 N/A N/A
Depressionoutcome 0.28
Screeningmeasure 10 53260 4.420 2.57 7.65 <0.0001 4.99(2.93–8.51)[1] 96 Structuredinstrument 1 366 1.240 0.24 6.20 0.86 N/A N/A
Frailtymeasure 0.34
Fried 10 12969 4.074 1.96 8.84 0.001 4.65(2.30–9.38)[1] 96
WHI-OS 1 40657 2.855 0.28 28.69 0.372 N/A N/A
Key:N/A=notapplicable,CI:Confidenceinterval;OR:Oddsratio;WHI-OS:Women’sHealthInitiativeObservationalStudy.
and lossof weight(≥3criteria) (Abellan vanKan et al.,2008); theadaptedfrailtyindexincludingthefollowing:wasting, weak-ness,slowness,fatigueorexhaustion,andfalls(n=1)(Paulsonand Lichtenberg,2013);andClinicalFrailtyScalerangingfrom1(very fit)to7(severelyfrail)(n=1)(Rockwoodetal.,2005).
3.3. Measurementofdepression
Depressive symptoms were assessed using the CES-D scale (n=11),theGeriatricDepressionScale(GDS)(n=8)(Radloff,1977), and Composite International Diagnostic Interview (CIDI) (n=2) (Wittchenetal.,1991).Threestudiesadopteddifferentmethods includingthePatientHealthQuestionnaire(PHQ-9)(requiringat least5/9 symptoms)(Kroenkeet al.,2001), interview schedule basedontheDiagnosticandStatisticalManualofMentalDisorders (DSMIII-R)andtheBurnam8-itemdepressionscreening instru-ment(Burnametal.,1988).
3.4. Cross-sectionalmeta-analysisfindings
3.4.1. Prevalenceofdepressioninpeoplewithfrailty
Fulldetailsoftheprevalenceofdepressioninpeoplewithfrailty aresummarizedinTable1.Theoverallprevalenceofdepressionin 8023peoplewithfrailtywas38.6%(95%CI30.07–47.10,I2=94%). Table1showstheprevalenceofdepressioninfrailpeoplestratified bygeographicalregion,studysetting,depressionoutcomeand def-initionoffrailty.Thesemoderatorsdidnotsignificantlyaffectour results,althoughtheprevalenceoffrailtywashigherinstudiesin
LatinAmerica,amongcommunity-dwellers,usingscreening mea-suresfordepressivesymptoms(insteadofstructuredinterviews forMDD)andusingthecriteriasuggestedbyFriedetal.(Table1). Avisualinspectionoffunnelplots(availablefromcorresponding authoronrequest)didnotsuggestpublicationbiasandthetrim andfillanalysesallremainedunchangedwhenanypotential pub-licationbiaswasadjustedfor(Table1).
3.4.2. Oddsofdepressioninpeoplewithfrailtyversuscontrols
Acrosselevenstudies,takingpeoplewithoutfrailtyasthe ref-erence group,frailpeople had higherodds of havingcomorbid depression(OR=3.95,95%CI2.36–6.58,p<0.001).Afteradjusting forpublicationbias,theORincreasedto4.42(95%CI2.66–7.35). Thebetweengrouppvaluesforthesubgroupanalysesremained non-significant(Table1),however,someresultsinthesubgroups becamenon-significantwhichmaybeduetoasmallnumberof studiesinsomegroupings.Nostudyreportedtheoddsof depres-sioninpeoplewithfrailty,adjustedforpotentialconfounders.
3.4.3. Prevalenceoffrailtyinpeoplewithdepression
Table2
Meta-analysisresultsofprevalenceandoddsoffrailtyinolderpeoplewithdepression.
Analysis Numberof study estimates
Numberof participants
Meta-analysis Between grouppvalue
Trimandfilleffect size(95%CI) [adjustedstudies]
I2
Prevalenceoffrailtyinolderpeoplewithdepression
Prevalence 95%CI
Mainanalysis 8 2167 40.40% 27.00 55.30 Unchanged 97
Geographicalregion 0.027
NorthAmerica 5 1381 31.26% 17.32 49.67 Unchanged 97
Australia 2 398 72.9% 39.1 91.9 N/A N/A
Europe 1 378 27.24% 0.64 67.38 N/A N/A
Studysetting 0.576
Community 7 1789 42.60% 27.10 59.70 Unchanged 97
Communityandinpatient 1 378 27.24% 5.450 70.86 N/A N/A
Depressionclassification 0.03
Screeningtool 6 1701 49.50% 32.50 66.60 Unchanged 97
Structuredinterview 2 466 17.62% 5.460 44.22 N/A 90
Frailtymeasure 0.007
Fried 5 1592 27.12% 15.9 49.29 Unchanged 96
Friedadapted 1 167 51.49% 20.04 81.80 N/A N/A
IanaTask 2 408 85.45% 54.31 96.67 N/A N/A
Oddsoffrailtyinolderpeoplewithdepression
OR 95%CI
Mainanalysis 8 17099 4.068 1.93 8.55 <0.001 Unchanged 96
Geographicalregion 0.063
NorthAmerica 5 9185 2.256 1.00 5.08 0.05 Unchanged 96
Australia 2 7404 19.35 3.91 95.76 <0.001 N/A 93
Europe 1 510 3.745 0.573 24.48 0.168 N/A N/A
Studysetting 0.675
Community 7 16589 4.11 1.82 9.28 0.001 Unchanged 97
Communityandinpatient 1 510 3.74 0.42 33.31 0.23 N/A N/A
Depressionclassification 0.655
Screeningtool 6 15906 4.60 1.93 11.80 0.001 Unchanged 96 Structuredinterview 2 1193 2.67 0.55 12.78 0.29 N/A N/A
Frailtymeasure 0.056
Fried 5 11680 2.18 0.93 5.09 0.09 Unchanged 95
Friedadapted 1 580 4.22 0.60 29.34 0.145 N/A N/A
IanaTask 2 4839 19.12 1.23 16.13 <0.001 N/A N/A
Key:N/A=notapplicable,CI:Confidenceinterval;OR:Oddsratio.
althoughsomecautionshouldbegivenduetosmallnumberof studies in each group (Table 2).The trim and fill analyses all remainedunchanged.
3.4.4. Oddsoffrailtyinpeoplewithdepressionversuscontrols
Takingtheparticipantswithnodepressionasreference,people withdepressionhadanincreasedriskofhavingfrailty(OR=4.07, 95% CI 1.93–8.55, p<0.0001; I2=96%) (Table 2). This associa-tion was significant in five studies including North Americans (OR=2.25;95%CI1.00–5.08,p=0.05;I2=96%)comparedtoother settings (Table 2). As shown in Table 2, publication bias was unlikely.
Fourstudies(Changetal.,2010;deAlbuquerqueSousaetal., 2012;Jarschiketal.,2012;PegorariandTavares,2014)reportedthe ORforfrailtyinadjustedanalysesindepressedvs.nonedepressed people,takingrobustparticipantsasreference.Afteradjustingfora medianof6potentialconfounders(range:3–12),thepooledORwas 2.64(95%CI:1.59–4.37;I2=55%;Fig.2).Anotherstudy(Jungetal., 2016)reportedthatanORof5.25(95%CI:2.55–10.83)forfrailtyvs. pre-frailty/robustness,afteradjustingfor4potentialconfounders.
3.5. Longitudinalmeta-analysisfindings
3.5.1. Studiesinvestigatingincidentfrailtyinolderpeoplewith depression
Overall, 6404olderadults with depression atbaseline were followedoverameanof2.87yearsinvestigatingincidentfrailty (FugateWoodsetal.,2005;PaulsonandLichtenberg,2013;Lakey
etal.,2012;Hajeketal.,2016).ThepooledORforincidentfrailty, adjustedfor amedian of7potentialconfounders (range:0–21) (SupplementaryTable3),was3.72(95%CI1.95–7.08;p<0.0001; I2=98%),asshowninFig.3.
3.5.2. Studiesinvestigatingincidentdepressionamongpeople withfrailty
Overall,twolongitudinalstudies(Fengetal.,2014;Makizako et al., 2015) including 4852 older adults investigated incident depressionastheoutcome.Thesetwostudiesfoundthatfrailtyat thebaselineincreasedtheriskofincidentdepressionbyabout90% (OR=1.90;95%CI1.55–2.32,p<0.0001;I2=0%),afteradjustingfor 11covariates(Fig.4;SupplementaryTable4).Onestudy(Monin et al.,2016)withnometa-analyzabledatareportedan associa-tionbetweendepressionandfrailtyin1260community-dwelling marriedcouples.
4. Discussion
Fig.2. Oddsoffrailtyinpeoplewithdepressionversuscontrols.
Fig.3.Oddsforincidentfrailtyinolderpeoplewithdepression.
Fig.4.Oddsforincidentdepressionamongpeoplewithfrailty.
inolderpeoplewithdepressionversusthosewithoutdepression. Longitudinalstudiessubstantiallyconfirmedthesefindingsdespite beingmorelimitedinnumber.
Frailty,isamultifactorialgeriatricsyndrome,whichcouldbe influencedbypain,mobilityandbalanceproblems,weakness,poor enduranceetc.Alloftheseriskfactorsmayleadtodisability,or functionaldependence,andthusleadtodepression(FugateWoods etal.,2005).Ontheotherhand,depressionmayalsopredict indi-catorsoffrailtyduetothedecreaseinsocialties,gaitspeed,and lessphysicalactivities,orduetotheincreaseinsedentarylife,fall risk,weightloss,andmalnutrition,whichmayincreasethe per-petuationofaffectivesymptoms typicalof depressionincluding sadness,anhedonia,andhelplessness(Hajeketal.,2016;Paulson andLichtenberg,2013).Additionally,depressionmaynotonlybe
Grow-ingevidencealsosupportsapositiveassociationbetweenfrailty andtheinflammatorycytokines,suchasinterleukin6(IL6)(Soysal et al., 2016), which is also known to be elevated in individu-alswithlatelifedepression(Vaughanetal.,2015).Inflammatory cytokinesare associatedwithboth decreased musclemass and strength,andalsonegativelyaffectthecentraldopaminergic func-tion,whichmayresultindepressiveaffect,fatigue,andcognitive andmotorslowing(Brownetal.,2016).Mitochondrialdysfunction hasalsobeenidentifiedinnumerousneurodegenerativediseases aswellasdepression.Musclebiopsiesinpatientswithdepression haveshowndecreasedATPproduction,andadultswithdepression hadalsoimpairedmitochondrial respirationinperipheralblood mononuclearcells,moststronglycorrelatingwiththesymptom of fatigue (Brown et al., 2016).The detrimental cycle between declinedactivity,mobility,andenergylevelsresemblestheclinical presentationofdepressionaswellasthosewiththefrailty syn-drome(Brownetal.,2016).AnotherhypothesisisthatHPAaxis dysregulation,aswellasaberrationsinothermediators,suchas insulin-likegrowthfactor,andtestosterone(Belvederietal.,2014), have beenreported in frail personswith significantdepressive symptomsandmayaccountforthereciprocalassociationherein observed(vonZerssenetal.,1986).Moreover,thebeneficialeffects of theapproaches topreventfrailty ordepression may protect theother.Forexample, thesuccessfultreatmentof the depres-sionitselfmayresultinincreasedbehavioralandsocialactivation, therebyincreasingphysicaland socialactivitylevels,improving musclemassandstrength,andtheelder’soverallenergylevels, thereby, reducing frailty(Lakey etal., 2012).Similarly, increas-ingphysicalactivityisaneffectiveinterventionforfrailtyinolder adults,andcanprotectandmanagedepressivesymptomsinthe elderlythroughpotentialneurobiologicalchangesandasa con-sequenceofsocialandphysicalengagement(Brownetal.,2016;
Schuchetal.,2016a,b).Otherinterventionssuchasimproving bal-anceandmusclestrength,andvitaminDsupplementationmayalso playaroleinpreventingortreatingfrailty(Brouwer-Brolsmaetal., 2013).DepressivesymptomsmaycausevitaminDdeficiencyvia decreasedsunexposure,poorerdietaryintakeandmoresmoking (Brouwer-Brolsmaetal.,2013).Infact,allthesefindingssupport thebidirectionalityofthedepression–frailtyrelationship.Clearly, futureresearchisrequiredtoexploreandunderstandsuch rela-tionships.
Ourcomprehensivemeta-analysisresultsadvancetheliterature frompreviouslypublishednarrativeand/orselectivereviewsthat haveconsideredtherelationshipbetweendepressionandfrailty. Meta-analysesenablethelogicalpoolingofdataandenableamore preciseestimateoftheprevalenceand/oroddsofanoutcomethan whenmakingsubjectiveconsiderationsofindividualstudies sep-aratelysuchasthoseinpreviousnarrativereviews(Ioannidisand Lau,1999).Nonetheless,thepreviousreviewshaveillustratedsome interestingfindings.Onereview,including28studies,reportedthat frailtyanddepressionarecomorbidgeriatricsyndromesina sub-groupofolderindividuals,andthatfrailtyisalsoariskfactorfor thedevelopmentandpersistenceofdepressivesymptoms(Buigues etal.,2015).Anotherreview,includingbothcross-sectional(n=16) andcohortstudies(n=23)indicatedthatfrailty,itscomponents, andfunctionalimpairmentareriskfactorsfordepression(Mezuk etal.,2012).Ontheotherhand,anotherreviewfoundthatthe rela-tionshipbetweendepressivesymptomatologyandincreasedrisk ofincidentfrailtywasrobust,whiletheoppositerelationshipwas lessconclusive(Vaughanetal.,2015).However,thepotentialrole ofantidepressantmedicationsonfrailtyhasnotbeenclearly eval-uatedinanyofthesereviews.Because,asshowninthereviewby Benraadetal,geriatriccharacteristicsarerarelytakenintoaccount intrialsonantidepressantdrugsinlate-lifedepression(Benraad etal.,2016).Todifferentiatefromthesepreviousreviews,the meta-analysiswasperformedinthepresentstudy(Buiguesetal.,2015;
Mezuketal.,2012).Specificallyourdataestablishedthatfrailolder peoplearefourtimesmorelikely tohave depressioncompared tocontrols, withsimilarincreasedodds forfrailtyamongthose withdepressionversuscontrols.Whilecross-sectionalstudiesare unable toclarify the directionalityof the relationship between frailtyanddepression,itclearlyindicatesthatthereisahighlevel ofcomorbidity.Whetherornotthisisattributedtomutually exclu-siveoroverlappingsymptomologyofeachconditionisnotclearand futureprospectiveresearchmayhelptodisentanglethis relation-shipandexplorepotentialoverlappingsymptomologyanddisease onset.Nonetheless,thelimitednumberprospectivestudiesdoes suggestthatafteradjustingforconfounders,peoplewith depres-sionareatincreasedriskofdevelopingfrailty,whilsttheconverse relationshipalsoappearstobeevident.However,thesmall num-beroflongitudinalstudiesprecludesanydefinitiveconclusionsand futurelongitudinalresearchisrequiredtospecificallyattemptto differentiatebetweenthesignsandsymptomsofbothconditions. Somefactorswereidentifiedinouranalysesasbeing poten-tiallyimportantinexplainingtheassociationbetweendepression andfrailty.Theprevalenceofdepressioninfrailpeople,infact,was higherinstudiesfromLatinAmerica,amongcommunity-dwellers, those using depression screening measures (instead structured interviews)andinstudieswhichconsideredcriteriasuggestedby
Friedetal.(2001)Arecentinternationalstudydemonstratedthat depressivesymptomsaremorepronouncedwithintraditional fam-ilybasedvaluepatterns,likeLatinAmerica, possiblybecauseof higherexpectationsoftheavailabilityoffamilysupportthatare oftenonlypartiallyfulfilledduetorecentchangesinfamily struc-ture(Yllietal.,2016).Fried’scriteriasharessymptomswiththe CES-Dandthiscouldpartiallyexplainthehighcorrelation. How-ever,somestudieshavefoundthatthestrongassociationbetween frailtyanddepressionisnotuniquetoasingledefinitionoffrailty suchastheClinicalFrailtyIndex, andthus,ourfindings donot seemtobefullyexplainedbysharedsymptomatology(Lohman etal.,2014).Wealsoexaminedtheoppositerelationship,i.e.the prevalenceofdepressionamongthefrailandtheoddsand inci-denceofdepressioninfrailolderindividualscomparedtorobust ones.Depressedpeopleshowedsignificantlyhigherlevelsoffrailty (∼40%),mainlyinNorthAmericanstudiesandinoneAustralian study(Almeidaetal.,2015).
Prospectivestudiesoftherelationshipbetweendepressionand incidentfrailtyalsosuggestthatdepressionmayincreasetherisk of frailty (Vaughan et al., 2015).Depression is associated with increasedweakness,mobilitydeficits,andfatigue,whichmaythus increasetheriskoffrailtyandincreasedmortalityoveraperiod ofupto5years (Veroneseetal.,2016).Theroleof antidepres-santdrugtreatmentintherelationshipbetweendepressionand frailtydeserve furtherinvestigation.Antidepressants have been associatedwithahigherriskofincidentfrailty(Lakeyetal.,2012). Thisassociationcouldsimplybeexplainedbyamoresevereand chronicformofdepressionthatrequiredtheuseofantidepressant drugs(Vaughanetal.,2015),butalargeprospectiveobservational studyreportedthatevenintheabsenceofdepressivesymptoms, antidepressantusewasassociatedwithbecomingfrail(Lakeyetal., 2012).Therefore,non-pharmacologicalinterventionsmaybean importantapproachfordepressedfrailolderadults.Clearlyfurther researchisneededtoelucidatethepossibleroleofdrugsinthe depression-frailtyrelationship(Mezuketal.,2012).
5. Limitations
betweenthesetwoconstructsisnotclear.Inaddition,the num-berofprospectivestudieswaslimited,thereforefutureprospective research is required to allow a better elucidation of potential moderatorswhichcouldinfluencethereciprocalprospective asso-ciationsbetweendepressionandfrailty.Asecondlimitationisthe highheterogeneityobserved. Thedifferentmethods and differ-entcut-offvaluesusedfordefiningfrailtyanddepressionmight playarole,butourfindingssuggestthatthesefactorscannot com-pletelyexplaintheobservedreciprocalassociations.Third,there waslimitedinformationonimportantmoderatorssuchasphysical activity,medicationuse,presenceofdementia,andinflammatory cytokines.Fourth,depressionwasdiagnosedthroughnon-original methods(DSM),andonlyfourstudies(Anandetal.,2012;Feng etal.,2014;Friedetal.,2001;Lakeyetal.,2012)reporteddata regardingantidepressants,thusprecludingthepossibilityto con-ductameta-analysis.However,inonelargelongitudinalstudy,the useofantidepressantswasassociatedwithahigherincidenceof frailtyindicatingthatthisfactorisofimportanceintheassociation betweendepressionandfrailty(Lakeyetal.,2012).Thus, future researchshouldconsidertherelationshipbetweenantidepressant medicationandfrailty/depression.Finally,thepresenceof depres-sivesymptomsintheconstructoffrailtymayartificiallycontribute totherelationshipbetweenfrailtyanddepression.Moreresearchis requiredtoinvestigatetherelationshipbetweenmajordepression andclearlydefinedfrailtyinparticular.Suchresearchmightalso considertherelationshipofimportantpotentialmoderatorssuch asphysicalactivity,antidepressantmedicationandinflammatory markers.
Inconclusion,ourresultsprovideevidenceforaconsistent bidi-rectionalrelationshipbetweenfrailtyanddepressionamongolder people. However, the precise mechanisms underpinning those reciprocalepidemiologicalassociationsdeservefurther investiga-tion.Ourdatasuggestthatoverathirdofpeoplewithfrailtyhave depressionandasimilarproportionofpeoplewithdepressionhave frailty,whiletheoddsofeachconditionarefourtimeshigherthan controls.Therefore,interventionsdesignedtodecreaseoneofboth syndromescanpreventtheemergenceofother.Ourdataisof pub-lichealthimportanceandmayopenimportantperspectivesforthe preventionandtreatmentofthosehighlyco-occurringand preva-lentconditions.
Conflictofinterest
None.
Financialdisclosure
Soysal, Veronese, Thompson, Kahl, Fernandes, Prina, Solmi, Schofield,Koyanagi,Tseng,Lin,Chu,Cosco,Cesari,Carvalho,Stubbs havenothingtodisclose.
AiKoyanagi’sworkissupportedbytheMiguelServetcontract financedbytheCP13/00150andPI15/00862projects,integrated intotheNationalR+D+IandfundedbytheISCIII–GeneralBranch EvaluationandPromotionofHealthResearch–andtheEuropean RegionalDevelopmentFund(ERDF-FEDER).TDCissupportedby aCanadianInstitutesofHealthResearchPostdoctoralFellowship (MFE-146676).
BrendonStubbsissupportedbytheNationalInstituteforHealth Research(NIHR) Collaborationfor Leadershipin Applied Health ResearchandCareSouthLondonatKing’sCollegeHospitalNHS FoundationTrust.Theviewsexpressedarethoseoftheauthor(s) andnotnecessarilythoseoftheNHS,theNIHRortheDepartment ofHealth
AppendixA. Supplementarydata
Supplementarydataassociatedwiththisarticlecanbefound,in theonlineversion,athttp://dx.doi.org/10.1016/j.arr.2017.03.005.
References
AbellanvanKan,G.,Rolland,Y.,Bergman,H.,etal.,2008.TheI.A.N.ATaskForceon frailtyassessmentofolderpeopleinclinicalpractice.J.Nutr.HealthAging12, 29e37.
Almeida,O.P.,Hankey,G.J.,Yeap,B.B.,Golledge,J.,Norman,P.E.,Flicker,L.,2015. Depression,frailty,andall-causemortality:acohortstudyofmenolderthan 75years.J.Am.Med.Dir.Assoc.16,296–300,http://dx.doi.org/10.1016/j. jamda.2014.10.023.
Almeida,O.P.,McCaul,K.,Hankey,G.J.,Yeap,B.B.,Golledge,J.,Norman,P.E.,Flicker, L.,2016.Durationofdiabetesanditsassociationwithdepressioninlaterlife: theHealthinMenStudy(HIMS).Maturitas86,3–9,http://dx.doi.org/10.1016/ j.maturitas.2016.01.003.
Anand,A.,Gunn,A.D.,Barkay,G.,Karne,H.S.,Nurnberger,J.I.,Mathew,S.J.,Ghosh, S.,2012.Earlyantidepressanteffectofmemantineduringaugmentationof lamotrigineinadequateresponseinbipolardepression:adouble-blind, randomized,placebo-controlledtrial.BipolarDisord.14,64–70,http://dx.doi. org/10.1111/j.1399-5618.2011.00971.x.
Badalà,F.,Nouri-mahdavi,K.,Raoof,D.A.,2008.NIHpublicaccess.Computer(Long. Beach.Calif.)144,724–732,http://dx.doi.org/10.1038/jid.2014.371.
Benraad,C.E.M.,Kamerman-Celie,F.,vanMunster,B.C.,OudeVoshaar,R.C.,Spijker, J.,OldeRikkert,M.G.M.,2016.Geriatriccharacteristicsinrandomised controlledtrialsonantidepressantdrugsforolderadults:asystematicreview. Int.J.Geriatr.Psychiatry31,990–1003,http://dx.doi.org/10.1002/gps.4443. Belvederi,M.Murri,Pariante,C.,Mondelli,V.,Masotti,M.,Atti,A.R.,Mellacqua,Z.,
Antonioli,M.,Ghio,L.,Menchetti,M.,Zanetidou,S.,Innamorati,M.,Amore,M., 2014.HPAaxisandagingindepression:systematicreviewandmeta-analysis. Psychoneuroendocrinology41,46–62,http://dx.doi.org/10.1016/j.psyneuen. 2013.12.004.
Bortolato,B.,Miskowiak,K.W.,Köhler,C.A.,Maes,M.,Fernandes,B.S.,Berk,M., Carvalho,A.F.,2016.Cognitiveremission:anovelobjectiveforthetreatmentof majordepression?BMCMed.22(14:9), http://dx.doi.org/10.1186/s12916-016-0560-3.
Brouwer-Brolsma,E.M.,vandeRest,O.,Tieland,M.,vanderZwaluw,N.L., Steegenga,W.T.,Adam,J.J.,vanLoon,L.J.,Feskens,E.J.,deGroot,L.C.,2013. Serum25-hydroxyvitaminDisassociatedwithcognitiveexecutivefunctionin Dutchprefrailandfrailelderly:across-sectionalstudyexploringthe associationsof25-hydroxyvitaminDwithglucosemetabolism,cognitive performanceanddepression.J.Am.Med.Dir.Assoc.06,010.
Brown,P.J.,Roose,S.P.,Fieo,R.,Liu,X.,Rantanen,T.,Sneed,J.R.,Rutherford,B.R., Devanand,D.P.,Avlund,K.,2014.Frailtyanddepressioninolderadults:a high-riskclinicalpopulation.Am.J.Geriatr.Psychiatry22,1083–1095,http:// dx.doi.org/10.1016/j.jagp.2013.04.010.
Brown,P.J.,Rutherford,B.R.,Yaffe,K.,Tandler,J.M.,Ray,J.L.,Pott,E.,Chung,S., Roose,S.P.,2016.Thedepressedfrailphenotype:Theclinicalmanifestationof increasedbiologicalaging.Am.J.Geriatr.Psychiatry.24(11),1084–1094, http://dx.doi.org/10.1016/j.jagp.2016.06.005.
Buigues,C.,Padilla-Sánchez,C.,Garrido,J.F.,Navarro-Martínez,R.,Ruiz-Ros,V., Cauli,O.,2015.Therelationshipbetweendepressionandfrailtysyndrome:a systematicreview.AgingMent.Health19,762–772,http://dx.doi.org/10.1080/ 13607863.2014.967174.
Burnam,M.A.,Wells,K.B.,Leake,B.,Landsverk,J.,1988.Developmentofabrief screeninginstrumentfordetectingdepressivedisorders.MedCare26(8), 775–789.
Chang,S.S.,Weiss,C.O.,Xue,Q.L.,Fried,L.P.,2010.Patternsofcomorbid inflammatorydiseasesinfrailolderwomen:thewomen’shealthandaging studiesIandII.J.Gerontol.Ser.A-Biol.Sci.Med.Sci.65,407–413,http://dx. doi.org/10.1093/gerona/glp181.
Clegg,A.,Young,J.,Iliffe,S.,Rikkert,M.O.,Rockwood,K.,2013.Frailtyinelderly people.Lancet381,752–762,
http://dx.doi.org/10.1016/S0140-6736(12)62167-9.
Collard,R.M.,Boter,H.,Schoevers,R.A.,OudeVoshaar,R.C.,2012.Prevalenceof frailtyincommunity-dwellingolderpersons:asystematicreview.J.Am. Geriatr.Soc.60,1487–1492,http://dx.doi.org/10.1111/j.1532-5415.2012. 04054.x.
Collard,R.M.,Comijs,H.C.,Naarding,P.,OudeVoshaar,R.C.,2014.Physicalfrailty: vulnerabilityofpatientssufferingfromlate-lifedepression.AgingMent. Health18,570–578,http://dx.doi.org/10.1080/13607863.2013.827628. deAlbuquerqueSousa,Patrício,Dias,R.C.,Macielálvaro,C.C.,Guerra,R.O.,2012.
Frailtysyndromeandassociatedfactorsincommunity-dwellingelderlyin NortheastBrazil.Arch.Gerontol.Geriatr.,54,http://dx.doi.org/10.1016/j. archger.2011.08.010.
Dent,E.,Hoogendijk,E.O.,2014.Psychosocialfactorsmodifytheassociationof frailtywithadverseoutcomes:aprospectivestudyofhospitalisedolder people.BMCGeriatr.14,108,http://dx.doi.org/10.1186/1471-2318-14-108. Drey,M.,Pfeifer,K.,Sieber,C.C.,Bauer,J.M.,2011.TheFriedfrailtycriteriaas
Duval,S.,Tweedie,R.,2000.Trimandfill:asimplefunnel-plot-basedmethodof testingandadjustingforpublicationbiasinmeta-analysis.Biometrics56, 455–463,http://dx.doi.org/10.1111/j.0006-341x.2000.00455.x.
Feng,L.,Nyunt,M.S.Z.,Feng,L.,Yap,K.B.,Ng,T.P.,2014.Frailtypredictsnewand persistentdepressivesymptomsamongcommunity-dwellingolderadults: findingsfromsingaporelongitudinalagingstudy.J.Am.Med.Dir.Assoc.15, http://dx.doi.org/10.1016/j.jamda.2013.10.001.
Fried,L.P.,Tangen,C.M.,Walston,J.,Newman,A.B.,Hirsch,C.,Gottdiener,J., Seeman,T.,Tracy,R.,Kop,W.J.,Burke,G.,McBurnie,M.A.,2001.Frailtyinolder adults:evidenceforaphenotype.J.Gerontol.ABiol.Sci.Med.Sci.56, M146–M156.
FugateWoods,N.,LaCroix,A.Z.,Gray,S.L.,Aragaki,A.,Cochrane,B.B.,Brunner,R.L., Masaki,K.,Murray,A.,Newman,A.B.,2005.Frailty:emergenceand
consequencesinwomenaged65andolderinthewomen’shealthinitiative observationalstudy.J.Am.Geriatr.Soc.53,1321–1330,http://dx.doi.org/10. 1111/j.1532-5415.2005.53405.x.
Hajek,A.,Brettschneider,C.,Posselt,T.,Lange,C.,Mamone,S.,Wiese,B.,Weyerer, S.,Werle,J.,Fuchs,A.,Pentzek,M.,Stein,J.,Luck,T.,Bickel,H.,Mosch,E.,Heser, K.,Jessen,F.,Maier,W.,Scherer,M.,Riedel-Heller,S.G.,Konig,H.-H.,2016. Predictorsoffrailtyinoldage–resultsofalongitudinalstudy.J.Nutr.Health Aging20,952–957,http://dx.doi.org/10.1007/s12603-015-0634-5. Hare,D.L.,Toukhsati,S.R.,Johansson,P.,Jaarsma,T.,2014.Depressionand
cardiovasculardisease:aclinicalreview.Eur.HeartJ.35,1365–1372,http://dx. doi.org/10.1093/eurheartj/eht462.
Higgins,J.P.T.,Thompson,S.G.,2002.Quantifyingheterogeneityinameta-analysis. Stat.Med.21,1539–1558,http://dx.doi.org/10.1002/sim.1186.
Ioannidis,J.P.,Lau,J.,1999.Poolingresearchresults:benefitsandlimitationsof meta-analysis.Jt.Comm.J.Qual.Improv.25(9),462–469.
Jarschik,P.,Nunin,C.,Botigu,T.,Escobar,M.A.,Lavedan,A.,Viladrosa,M.,2012. Prevalenceoffrailtyandfactorsassociatedwithfrailtyintheelderly populationofLleidaSpain:theFRALLEsurvey.Arch.Gerontol.Geriatr.55, 625–631,http://dx.doi.org/10.1016/j.archger.2012.07.002.
Jung,H.,Jang,I.,Lee,Y.S.,Lee,C.K.,Cho,E.,Kang,W.Y.,Kim,D.H.,2016.Prevalence offrailtyandaging-relatedhealthconditionsinolderkoreansinrural communities:across-sectionalanalysisoftheagingstudyofpyeongchang ruralarea.J.KoreanMed.Sci.,345–352,http://dx.doi.org/10.3346/jkms.2016. 31.3.345.
Katz,I.R.,2004.Depressionandfrailty:theneedformultidisciplinaryresearch.Am. J.Geriatr.Psychiatry12,1–6.
Kroenke,K.,Spitzer,R.L.,Williams,J.B.,2001.ThePHQ-9:validityofabrief depressionseveritymeasure.J.Gen.Intern.Med.16(9),606–613. Lakey,S.L.,Lacroix,A.Z.,Gray,S.L.,Borson,S.,Williams,C.D.,Calhoun,D.,Goveas,
J.S.,Smoller,J.W.,Ockene,J.K.,Masaki,K.H.,Coday,M.E.,Rosal,M.C.,Woods, N.F.,2012.Antidepressantuse,depressivesymptoms,andincidentfrailtyin womenaged65andolderfromtheWomen’SHealthInitiativeObservational Study.J.Am.Geriatr.Soc.60,854–861,http://dx.doi.org/10.1111/j.1532-5415. 2012.03940.x.
Liberati,A.,Altman,D.G.,Tetzlaff,J.,Mulrow,C.,Gøtzsche,P.C.,Ioannidis,J.P.A., Clarke,M.,Devereaux,P.J.,Kleijnen,J.,Moher,D.,2009.ThePRISMAstatement forreportingsystematicreviewsandmeta-analysesofstudiesthatevaluate healthcareinterventions:explanationandelaboration.PLoSMed.6,http://dx. doi.org/10.1371/journal.pmed.1000100(e1000100).
Lohman,M.,Dumenci,L.,Mezuk,B.,2014.Sexdifferencesintheconstructoverlap offrailtyanddepression:evidencefromthehealthandretirementstudy.J. Am.Geriatr.Soc.62,500–505,http://dx.doi.org/10.1111/jgs.12689. Lohman,M.,Dumenci,L.,Mezuk,B.,2016.Depressionandfrailtyinlatelife:
evidenceforacommonvulnerability.J.Gerontol.-Ser.BPsychol.Sci.Soc.Sci. 71,630–640,http://dx.doi.org/10.1093/geronb/gbu180.
Lohman,L.,2013.Constructoverlapbetweendepressionandfrailtyinlaterlife: evidencefromthehealthandretirementstudy.Compr.Psychiatry,http://dx. doi.org/10.1016/j.comppsych.2012.07.032.
MatheusArts,H.L.,Collard,R.M.,Comijs,H.C.,Zuidersma,M.,deRooij,S.E., Naarding,P.,OudeVoshaar,R.C.,2016.Physicalfrailtyandcognitive functioningindepressedolderadults:findingsfromtheNESDOstudy.J.Am. Med.Dir.Assoc.17,36–43,http://dx.doi.org/10.1016/j.jamda.2015.07.016. Makizako,H.,Shimada,H.,Doi,T.,Yoshida,D.,Anan,Y.,Tsutsumimoto,K.,Uemura,
K.,Liu-Ambrose,T.,Park,H.,Lee,S.,Suzuki,T.,2015.Physicalfrailtypredicts incidentdepressivesymptomsinelderlypeople:prospectivefindingsfromthe ObuStudyofHealthPromotionfortheElderly.J.Am.Med.Dir.Assoc.16, 194–199,http://dx.doi.org/10.1016/j.jamda.2014.08.017.
McAdams-DeMarco,M.A.,Ying,H.,Olorundare,I.,King,E.A.,Haugen,C.,Buta,B., Gross,A.L.,Kalyani,R.,Desai,N.M.,Dagher,N.N.,Lonze,B.E.,Montgomery,R.A., Bandeen-Roche,K.,Walston,J.D.,Segev,D.L.,2016.Individualfrailty componentsandmortalityInkidneytransplantrecipients.Transplantation,1, http://dx.doi.org/10.1097/tp.0000000000001546.
Mezuk,B.,Edwards,L.,Lohman,M.,Choi,M.,Lapane,K.,2012.Depressionand frailtyinlaterlife:asyntheticreview.Int.J.Geriatr.Psychiatry27,879–892, http://dx.doi.org/10.1002/gps.2807.
Mezuk,B.,Lohman,M.,Dumenci,L.,Lapane,K.L.,2013.Aredepressionandfrailty overlappingsyndromesinmid-andlate-life?Alatentvariableanalysis.Am.J. Geriatr.Psychiatry21,560–569,http://dx.doi.org/10.1016/j.jagp.2012.12.019.
Monin,J.,Doyle,M.,Levy,B.,Schulz,R.,Fried,T.,Kershaw,T.,2016.Spousal associationsbetweenfrailtyanddepressivesymptoms:longitudinalfindings fromthecardiovascularhealthstudy.J.Am.Geriatr.Soc.64,824–830,http:// dx.doi.org/10.1111/jgs.14023.
Newberg,A.R.,Davydow,D.S.,Lee,H.B.,2006.Cerebrovasculardiseasebasisof depression:post-strokedepressionandvasculardepression.Int.Rev. Psychiatry18,433–441,http://dx.doi.org/10.1080/09540260600935447. Paulson,D.,Lichtenberg,P.A.,2013.Vasculardepression:anearlywarningsignof
frailty.AgingMent.Health17,85–93,http://dx.doi.org/10.1080/13607863. 2012.692767.
Pegorari,M.S.,Tavares,D.M.D.S.,2014.Factorsassociatedwiththefrailty syndromeinelderlyindividualslivingintheurbanarea.Rev.Lat.Am. Enfermagem22,874–882,http://dx.doi.org/10.1590/0104-1169.0213.2493. Potter,G.G.,McQuoid,D.R.,Whitson,H.E.,Steffens,D.C.,2016.Physicalfrailtyin late-lifedepressionisassociatedwithdeficitsinspeed-dependentexecutive functions.Int.J.Geriatr.Psychiatry31,466–474,http://dx.doi.org/10.1002/gps. 4351.
Radloff,L.S.,1977.TheCES-Dscale:aself-reportdepressionscaleforresearchin thegeneralpopulation.Appl.Psychol.Meas.1,385–401,http://dx.doi.org/10. 1177/014662167700100306.
Rockwood,K.,Song,X.,MacKnight,C.,Bergman,H.,Hogan,D.B.,McDowell,I., Mitnitski,A.,2005.Aglobalclinicalmeasureoffitnessandfrailtyinelderly people.CMAJ173(5),489–495.
Rodda,J.,Walker,Z.,Carter,J.,2011.Depressioninolderadults.BMJ343,http://dx. doi.org/10.1136/bmj.d5219.
Sanchez-Garcia,S.,Sanchez-Arenas,R.,Garcia-Pereira,C.,Rosas-Carrasco,O., Avila-Funes,J.A.,Ruiz-Arregui,L.,Juarez-Cedillo,T.,2014.Frailtyamong community-dwellingelderlyMexicanpeople:prevalenceandassociationwith sociodemographiccharacteristics,healthstateandtheuseofhealthservices. Geriatr.Gerontol.Int.14,395–402,http://dx.doi.org/10.1111/ggi.12114. Schuch,F.B.,Deslandes,A.C.,Stubbs,B.,Gosmann,N.P.,Silva,C.T.,Fleck,M.P.,
2016a.Neurobiologicaleffectsofexerciseonmajordepressivedisorder:a systematicreview.Neurosci.Biobehav.Rev.61,1–11,http://dx.doi.org/10. 1016/j.neubiorev.2015.11.012.
Schuch,F.B.,Vancampfort,D.,Rosenbaum,S.,Richards,J.,Ward,P.B.,Veronese,N., Solmi,M.,Cadore,E.L.,Stubbs,B.,2016b.Exercisefordepressioninolder adults:ameta-analysisofrandomizedcontrolledtrialsadjustingfor publicationbias.Rev.Bras.Psiquiatr.38(3),247–254,http://dx.doi.org/10. 1590/1516-4446-2016-1915.
Soysal,P.,Stubbs,B.,Lucato,P.,Luchini,C.,Solmi,M.,Peluso,R.,Sergi,G.,Isik,A.T., Manzato,E.,Maggi,S.,Maggio,M.,Prina,A.M.,Cosco,T.D.,Wu,Y.-T.,Veronese, N.,2016.Inflammationandfrailtyintheelderly:asystematicreviewand meta-analysis.AgeingRes.Rev.31,1–8,http://dx.doi.org/10.1016/j.arr.2016. 08.006.
SoysalPinar,IsikAhmetTuran,CarvalhoAndreF.,FernandesBrisaS.,SolmiMarco, SchofieldPatricia,VeroneseNicola,StubbsBrendon,2017.Oxidativestressand frailty:Asystematicreviewandsynthesisofthebestevidence.
http://dx.doi.org/10.1016/j.maturitas.2017.01.006(inpress).
vonElm,E.,Altman,D.G.,Egger,M.,Pocock,S.J.,Gøtzsche,P.C.,Vandenbroucke,J.P., fortheSTROBEInitiative,2008.TheStrengtheningtheReportingof
ObservationalStudiesinEpidemiology(STROBE)statement:guildelinesfor reportingobservationalstudies.J.Clin.Epidemiol.61,344–349,http://dx.doi. org/10.1016/j.jclinepi.2007.11.008.
vonZerssen,D.,Berger,M.,Dose,M.,Doerr,P.,Krieg,C.,Bossert,S.,Riemann,D., Pirke,K.M.,Dolhofer,R.,Müller,O.A.,1986.Thenatureofneuroendocrine abnormalitiesindepression:acontroversialissueincontemporarypsychiatry. Psychiatr.Dev.4,237–256.
Vaughan,L.,Corbin,A.L.,Goveas,J.S.,2015.Depressionandfrailtyinlaterlife:a systematicreview.Clin.Interv.Aging10,1947–1958,http://dx.doi.org/10. 2147/CIA.S69632.
Veronese,N.,Stubbs,B.,Fontana,L.,Trevisan,C.,Bolzetta,F.,Rui,M.,Sartori,De, Musacchio,L.,Zambon,E.,Maggi,S.,Perissinotto,S.,Corti,E.,Crepaldi,M.C., Manzato,G.,Sergi,E.,2016.Acomparisonofobjectivephysicalperformance testsandfuturemortalityintheelderlypeople.J.Gerontol.A.Biol.Sci.Med. Sci.(July28),http://dx.doi.org/10.1093/gerona/glw139,pii:glw139. Wells,G.,Shea,B.,O’Connell,D.,Peterson,J.,Welch,V.,Losos,M.,Tugwell,P.,2012.
TheNewcastle-OttawaScale(NOS)forAssessingtheQualityIfNonrandomized StudiesinMeta-Analyses.,http://dx.doi.org/10.2307/632432(Availablefrom URL:http//www.ohrid.ca/programs/clinicalepidemiology/oxford.asp). Wittchen,H.U.,Robins,L.N.,Cottler,L.B.,Sartorius,N.,Burke,J.D.,Regier,D.,1991.
Cross-culturalfeasibility,reliabilityandsourcesofvarianceoftheComposite InternationalDiagnosticInterview(CIDI).ThemulticentreWHO/ADAMHA fieldtrials.Br.J.Psychiatry:J.Ment.Sci.645–653,658,159(JournalArticle). Woods,N.F.,LaCroix,A.Z.,Gray,S.L.,Aragaki,A.,Cochrane,B.B.,Brunner,R.L.,
Masaki,K.,Murray,A.,Newman,A.B.,2005.Frailty:emergenceand consequencesinwomenaged65andolderintheWomen’sHealthInitiative observationalstudy.J.Am.Geriatr.Soc.53,1321–1330,http://dx.doi.org/10. 1111/j.1532-5415.2005.53405.x.