THREE LEVELS MODEL FOR DIFFERENTIATED
PHARMACIST CLINICAL ACTIVITIES
IN THE COMMUNITY PHARMACY – THE PROPOSAL
Abstract
Due to the weak implementation of the change of pharmaceutical profession focus from the product to the patient, a new concept of services, based on pharmaceutical consultations should be developed and imple-mented. The aim of this paper is to introduce a new organizational model for pharmaceutical care services provision in the community pharmacy to answer differentiated patient’s health needs.
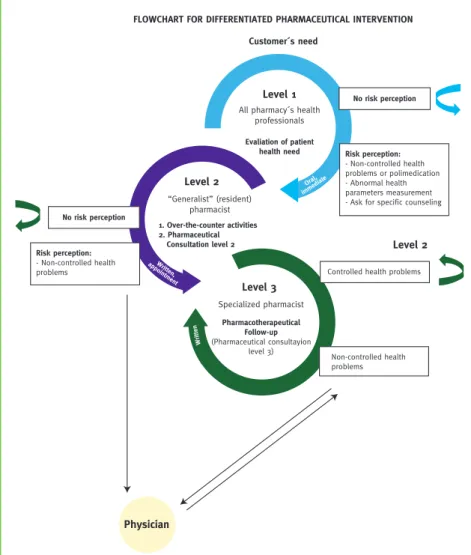
According to the model, pharmacist activities are structured in three interconnected levels, depending on patient´s health needs and expectations. Level 1 is the basic level of services provided by all the pharmacy professionals and addressed to customers asking for a comfort product or a medicinal product in the ab-sence of non-controlled health problem. Level 2 is the pharmaceutical generalist service provided by a resi-dent pharmacist and addressed to patients with common non-controlled health problems or asking for a specific and personalized counseling. It could be provided over-the-counter or in the office, configured as pharmaceutical consultation. Level 3 is the pharmaceutical specialized service, the Pharmacotherapeutic Follow-up consultation, provided by a specialized pharmacist, external to the pharmacy and is addressed to patients with recurrent non-controlled health problems or complex situations.
The provision of pharmaceutical care services through differentiated pharmacist intervention levels, based on the pharmacy customer´s health needs, seem to be a suitable model for its routine implementation in the community pharmacy. Most of the previously identified barriers for real implementation of clinical services in the pharmacy can be pulled down by the new strategy here proposed.
Keywords: Community pharmacy, pharmaceutical care services, pharmacotherapeutic follow-up consultation.
7
Resumo
É consensual que a atividade do farmacêutico na farmácia comunitária necessita de alterar o seu foco de atuação, do medicamento, sua manipulação e dispensa, para o doente e respetivos resultados clínicos decor-rentes da utilização da medicação que lhe é dispensada. Melhorar os resultados em saúde e a qualidade de vida do doente é o desafio que se coloca à profissão farmacêutica. Se, em teoria, tal já é contemplado no ato farmacêutico desde 2001, na prática ainda muito caminho há a percorrer.
O conceito de serviços farmacêuticos é bastante abrangente, envolvendo desde a habitual dispensa da me-dicação, o aconselhamento em transtornos minor, a manipulação magistral, a revisão da medicação até ao serviço mais especializado de consulta farmacêutica. Assim, nesta ampla gama de serviços com níveis de exigência e diferenciação bastante diversificados, é de esperar que a prestação efetiva dos vários serviços farmacêuticos obrigue a significativas mudanças na farmácia, sobretudo ao nível da sua filosofia de trabalho e organização de recursos humanos.
Por outro lado, a prestação da consulta farmacêutica, provavelmente o serviço farmacêutico mais efetivo na melhoria do estado de saúde do doente, apresenta uma expressão e nível de implementação muito baixos na maioria das farmácias portuguesas.
Rev Port Farmacoter| 2014;6:83-88 Mónica Condinho
ACF – Acompanhamento Farmacoterapêutico, Lda., Pavia, Portugal
Margarida Cavaco
ACF – Acompanhamento Farmacoterapêutico, Lda., Pavia, Portugal
Fernando Miranda
Motta pharmacy, Évora, Portugal. ACF – Acompanhamento Farmacoterapêutico, Lda., Pavia, Portugal
Carlos Sinogas
What Is Known
It is commonly accepted that the pharmacist activi-ties in the community pharmacy should change from the traditional manipulation of drugs and dispensing medicines to patient´s clinical outcomes as a result of medicinal products use1. Improvement on patient´s
health condition and quality of life is the pharmaceuti-cal profession´s challenge, which is already legal binding in Portugal2.
Provision of pharmaceutical care services imposes dras-tic changes in attitudes and procedures to fulfill the objectives. Dispensing of products, with or without a medical prescription, compounding medicines, pro-viding a simple medication review or performing phar-maceutical consultations are within the large scope of pharmaceutical services.
8
Vários fatores têm sido apontados como barreiras à implementação deste tipo de serviços na farmácia co-munitária. À cabeça, a falta de tempo devido ao excesso de trabalho administrativo, a falta de formação, conhecimentos e competências adequadas à prestação de um serviço mais orientado ao doente e o medo da mudança/receio de errar.
Acresce que diferentes doentes têm, naturalmente, diferentes necessidades de saúde, e portanto de serviço, exigindo da parte da equipa uma constante avaliação e adaptação.
Neste contexto, impõe-se uma reorganização das atividades do farmacêutico para responder às diferentes necessidades de saúde dos seus doentes, ultrapassando as referidas barreiras de implementação. Perspetiva--se, por isso, neste trabalho, um novo modelo funcional de organização dos serviços farmacêuticos em far-mácia comunitária para atender às necessidades clínicas dos utentes.
O modelo que se propõe estrutura as atividades do farmacêutico em três níveis inter-relacionados e dinâ-micos, de acordo com as necessidades de saúde e expectativas dos utentes. O nível 1 corresponde ao nível básico de serviço, aquele que é suscetível de ser prestado por todos os profissionais de saúde da farmácia. Destina-se ao utente sem problemas de saúde, ou com problemas de saúde controlados, sem perceção de risco associado e sem necessidade de aconselhamento específico. Inclui as situações de aconselhamento em transtornos minor, sempre devidamente suportadas por protocolos específicos e determinações de parâ-metros. O foco é o produto. Sempre que a este nível exista perceção de risco ou de problema de saúde não controlado, o doente deverá ser convidado para o nível 2. O nível 2 é o serviço farmacêutico central e genera-lista a ser prestado por farmacêutico da farmácia e destina-se a todos os doentes que apresentem problemas de saúde não controlados ou careçam de aconselhamento específico. Aqui o foco é o doente. Em virtude da avaliação efetuada, o farmacêutico poderá aconselhar, de imediato, ao balcão ou carecer de informação mais detalhada, convidando então o doente para a consulta farmacêutica, a qual apenas deverá estar disponível por marcação. Quando a situação não for controlada no nível 2, ou caso o farmacêutico percecione que se trata de uma situação complexa, que exige estudo pormenorizado, deverá encaminhar o doente para o nível 3. Este, por sua vez, constitui o serviço farmacêutico especializado, correspondendo ao acompanhamento farmacoterapêutico. Para ser eficaz só poderá ser prestado por farmacêutico especializado, externo à farmá-cia, e inteiramente dedicado à prática deste serviço. Destina-se a doentes com situações clínicas complexas e/ou problemas de saúde recorrentemente não controlados. O foco mantém-se no doente. Quando, a este ní-vel, o doente estiver controlado, ou caso não existam intervenções adicionais passíveis de induzir resultados positivos adicionais, o doente retorna ao nível 2, onde mantém a normal vigilância do seu estado de saúde. Trata-se assim de um modelo que, baseado nas necessidades de saúde dos doentes, parece ser adequado à prática diária da farmácia comunitária, uma vez que permite ultrapassar a maioria das barreiras identifica-das para a efetiva e regular implementação dos cuidados farmacêuticos.
Palavras-chave: Farmácia comunitária, serviços farmacêuticos, acompanhamento farmacoterapêutico.
In particular, the provision of pharmaceutical con-sultations, probably the most effective pharmaceu-tical service to improves patient´s health condition, remains with a low expression in most of the Portu-guese community pharmacies3. Several reasons have
been appointed as barriers for the development of this cognitive service in the community pharmacy, namely the lack of time, insufficient suitable training, lack of knowledge and skills, the fear of the change and lack of payment4.
Different patients would require different levels of pharmaceutical services. Reorganization of pharmacist´s activities to answer different patient’s health needs and to overcome the identified barriers is required.
Rev Port Farmacoter| 2014;6:83-88 Rev Port Farmacoter| 2014;6:83-88
FLOWCHART FOR DIFFERENTIATED PHARMACEUTICAL INTERVENTION Customer´s need
Level 1
All pharmacy´s health professionals Evaliation of patient health need Level 2 1. Over-the-counter activities 2. Pharmaceutical Consultation level 2 “Generalist” (resident) pharmacist Level 3 Pharmacotherapeutical Follow-up (Pharmaceutical consultayion level 3) Specialized pharmacist No risk perception Risk perception: - Non-controlled health problems or polimedication - Abnormal health parameters measurement - Ask for specific counseling
No risk perception Risk perception: - Non-controlled health problems Non-controlled health problems
Controlled health problems
Physician Level 2 Oral, immedia te Written , app ointment W rit te n
9
Objective
The objective of this paper is to introduce a new orga-nizational model for pharmaceutical care services pro-vision in the community pharmacy, answering to dif-ferentiated patient’s health needs and expectations.
What Is Proposed
The methodology applied is intended to struc-ture the pharmacy and its professional’s activities according with the patient´s health needs and expec-tations, from the simple selling of a comfort product to the specialized pharmaceutical consultations.
The Model
To focus the activity in the patient’s health needs and ex-pectations, the pharmacy services should be structured in three interconnected levels, as illustrated in the Figure 1.
Figure 1 – Graphic model to structure the pharmaceutical services in the community pharmacy based on the patient’s health needs and expectations
Based on most frequent scenarios observed on at-tendance at the community pharmacy, the authors envisage:
• Level 1 – the basic level services
A customer asking for a comfort product, non-related with health problems, or a medicinal product for a controlled health problem not requiring specific counseling or information does not suggest any risk perception to the pharmacy professional. The selling or dispensing the requested product fulfils the attendance and constitutes the basic service offered by all the community pharmacies. Requests for mi-nor disease can be responded at this level when based on specific protocols in use. Simple measurements of health parameters, as blood pressure or glycaemia, for instance, at request of other health professionals, will be also included within this first level of service. All the pharmacy professionals can provide this service. The product is the focus and selling it pays for the service of dispensing it. When at this level the pharmacy professional detects or suspects of any non-controlled health problem, which require a specific counseling, the customer should be invited to the next level of ser-vice. This invitation is oral and immediate. If the pharmacy pro-fessional is not a pharmacist, the pharmacist should be immedi-ately involved in the attendance. • Level 2 – the pharmaceutical
generalist services
When the customer’s health problem is not controlled or sus-pected of non-control, specific counseling by the pharmacist may be required. Depending on the situation and on the risk per-ception, the patient should be invited for a particular appoint-ment with the pharmacist. Dis-pensing of medicinal products for non-controlled health prob-lems, promotion of medication adherence, identification and re-porting of adverse drug reactions or interactions, brief medication review, promotion of healthy lifestyles and administration of
Rev Port Farmacoter| 2014;6:83-88 Rev Port Farmacoter| 2014;6:83-88
FLOWCHART FOR DIFFERENTIATED PHARMACEUTICAL INTERVENTION Customer´s need
Level 1
All pharmacy´s health professionals Evaliation of patient health need Level 2 1. Over-the-counter activities 2. Pharmaceutical Consultation level 2 “Generalist” (resident) pharmacist Level 3 Pharmacotherapeutical Follow-up (Pharmaceutical consultayion level 3) Specialized pharmacist No risk perception Risk perception: - Non-controlled health problems or polimedication - Abnormal health parameters measurement - Ask for specific counseling
No risk perception Risk perception: - Non-controlled health problems Non-controlled health problems
Controlled health problems
Physician Level 2 Oral, immedia te Written , app ointment W rit te n
Pharmaceutical level 2 consultation form
The first appointment is based on a formulary, mainly with closed questions, with an expected duration no longer then 30 minutes, addressing the following points:
- Part A: Identification of the health problem motivating the pharmaceutical consultation.
- Part B: Analysis of patient’s medication. Summary registration of all medicinal products used by the patient, with particular attention to
the posology and appropriate preservation.
- Part C: Health parameters analysis. Pharmacist considers the last patient’s laboratory tests, registering all the non-controlled values.
Depending on the health problem, some tests could be proposed, in order to better characterize and identify patient’s health condition.
- Part D: Health problems identification. Based on medicinal products used and test parameters, all the potential health problems should be
identified and listed. Based also on the patient concerns, one health problem is selected for intervention.
- Part E: Health problem evaluation. Detailed evaluation of the selected health problem is performed, searching for potential reasons of
the non-control. Medication (posology used versus prescribed, time to take the product, adherence and potential side effects) and lifestyle habits (food, exercise, smoking and alcoholic habits) are considered.
- Part F: Pharmacist intervention. Depending on previous evaluation, pharmacological and/or non-pharmacological interventions are
proposed to improve health condition. Timings and immediate therapeutic goals are agreed with the patient.
- Part G: Follow-up or referral. When the pharmacist feels the health problem can be solved by the proposed intervention, the consultation
is closed or a new appointment is proposed for confirmation. If the health problem seems complex and requires additional specialized study, the patient is invited to integrate the Pharmacotherapeutic Follow-up program. When the health problem requires intervention of other professional (physician, nurse or specific dietary recommendations, for instance) the patient is referred, by writing, to the other health professional.
- Part H: General remarks for future reference are registered in the file if necessary. vaccines or injections, for instance, require mastery
of pharmacotherapy by the pharmacist. This is the generalist pharmaceutical service, provided by a resi-dent professional, to be classified as level 2. It is as-sumed that at this level, the pharmacist expertise al-lows for an intervention not requiring specific study (“simple” intervention). The level 2 service can be provided over-the-counter, by standing attendance when a immediate intervention is envisaged, or in a private office when more detailed information should be considered. In this case, a meeting with the phar-macist should be arranged by appointment to the scheduled periods reserved for level 2 consultations, occurring weekly in the Pharmacy. These consulta-tions are oriented/supervised by a specialized phar-macist (responsible for level 3 service) and supported by a specifically developed form (see the box below). The health problem is the focus and the patient pays for the service only when the pharmacist interven-tions are supported by private consultainterven-tions.
By definition, the interventions at this level are not time consuming and allow controlling “simple” health problems. No more than 3 or 4 consultations should be needed to resolve the negative outcome.
When, at this level 2, the health problem cannot be controlled by “simple” interventions and a more detailed study is required, the patient should be addressed for level 3 service, the Pharmacotherapeu-tic Follow-up consultations. In this case, the referral should be in a written form and through appointment. Reference to the physician should also be considered if a clinical immediate intervention is required.
• Level 3 – pharmaceutical specialized services The main pharmacy activity included in the level 3 is the Pharmacotherapeutic Follow-up, a specialized pharmaceutical consultation. Pharmacotherapeutic Follow-up is a patient-centered practice in which, through a global and clinical approach of patient´s health needs, the pharmacist study and follow-up his Pharmacotherapeutic Profile, pathologies and health concerns, with the objective of improving the patient´s health condition and quality of life. The wide knowledge, time consuming, specific skills and training necessary to perform this cognitive service are incompatible with routine activities of the phar-macist in the Community Pharmacy5. A specialized
pharmacist in an outsourcing regimen is required to provide the service. The specialized pharmacist is an external health care provider, full-time dedicated to pharmacotherapeutic follow-up, with post-graduated education (about methodology, pharmacotherapy and pathologies) and specifically trained in the practice, including the skills needed to provide the service. Patient clinical history, pharmacotherapeutic profile and personal health concerns are considered for the evaluation of the negative clinical outcomes and for the management of pharmacist interventions, in or-der to solve the heath problem. All the interventions are based on immediate therapeutic goals defined in agreement with the patient. To control the health problem several consultations and different pharma-cist interventions may be required, either directed to the patient or to his physician (usually in a written form and through the patient).
10
11
The external and specialized pharmacist visits the community pharmacy biweekly and the frequency of consultations depends on the situation and the evolution of patient’s health condition. When all the health problems are solved or when the specialized pharmacist have no additional interventions to im-prove the patient’s quality of life, he is returned to the second level, to the local pharmacist, with a detailed written report.
The patient with recurrent non-controlled health problems is the target for this level and pays directly for the service.
Need for Differentiated Services
The frequency proposed for consultations, weekly for level 2 and bi-weekly for level 3 is based on a brief survey applied to evaluate the percentages of phar-macy customers requiring pharmacist interventions to improve his health condition.
Discussion about the Model
In spite of the aforementioned barriers, daily applica-tion of the principles of pharmaceutical care services are on trial for implemented in a number of European countries6. There are several models depending on the
country, its professional institutions and legislation. According to the recent annual report 2013 of Phar-maceutical Group of the European Union, United Kingdom (UK), Belgium, Norway and French were examples of pharmaceutical care services imple-mentation, recognizing that the poor medication adherence is a significant problem in the medication process use, being responsible for the worsening of patient´s health condition. In the UK, the service is available for a range of medicines and requires an initial consultation, then a follow-up consultation, usually over a period of 3-4 weeks, with new ap-pointment two weeks later. In Belgium the service is similar but limited to asthma patients. The patient is counseled about the disease’s symptoms, medication side effects and good medicines inhalation technique. It is the first of its kind to be funded by the Belgian health services. In Norway and France, the interven-tion is addressed to patients taking anti-coagulant medication for the first time and is also funded by the national health authorities. Across the consultations they receive written instructions for correct use, as well as, pharmacist counseling based on a checklist especially designed for the service7.
The authors are unaware of the existence of any other global approach for all customers’ health problems, as proposed in this paper. The services above mentioned
in the four European countries would be configures as level 2 services, according with the model pro-posed. The difference resides on the fact that, within this three levels model, the services are not restricted to specific pathologies or medicinal products.
The Australian experience with Home Medicines Review (HMR) is a service, funded by the common-wealth government, in which an accredited pharma-cist visit the patient at home and review all his medi-cines. After this the pharmacist works together with the general practitioner to develop a plan to manage the medication profile9. According with the three
levels model, this Australian service seems to bridge activities considered within the scopes of levels 2 and 3. A major difference resides in the fact that in HMR the pharmacist works together with the gen-eral practitioner following a protocol initiated by the physician, while here the target patient is identified by the pharmacist and referred to the physician only when pharmacological interventions are required. Usually there is no direct contact between the phar-macist and the physician in the ambulatory environ-ment. It would be advantageously in the future the development of direct contacts between the pharma-cist and the patient’s physician, because it is known that a solid relationship between both professionals have been appointed as a facilitator in the implemen-tation of pharmaceutical care services8.
In Portugal strong efforts have been developed by the National Association of Pharmacies and several aca-demic institutions, but it is recognized that the real implementation of pharmaceutical care failed3.
Based on the concept and on the practical experience, with clinical results reported in the accompanying paper, the proposed three levels model centre the Pharmacy on the patient, optimize clinical activities of pharmacy professional and allow for the routine implementation of these cognitive services by over-coming most of the identified barriers. In the absence of specific studies on the subject the pharmacists acting on the scope of these three levels model show professional satisfaction due to the induced added valorization and report patient recognition and sat-isfaction. The constant support and assistance pro-vided by the specialized pharmacist to the resident pharmacist on the level 2 service, as foreseen in the model, is considered essential for the success of the implementation phase and for the routine practice. The “fear of error”, limitations on pharmacology, pa-thology and methodology knowledge are minimized. Based on a brief survey to quantify the needs for dif-ferentiated services, the pharmacist interventions to
12
improving health parameters, are required for less than 20 % of pharmacy customers. In particular, level 3 service, the pharmacotherapeutic follow-up consultations, would be required for approximately 7 % of customers. This means that none pharmacy can afford for a professional exclusively dedicated to the level 3 service. Sharing an external specialized phar-macist is the solution developed to answer the prob-lem. Activities considered within the scope of level 2 service can easily be added to the other pharmacist activities in the Community Pharmacy as proved by the real exercise performed and reported in the ac-companying paper.
Globally, the proposed model centres the clinical pharmacy activities on the level 2 service provided by the resident pharmacist. When necessary the pa-tient assists level 3, returning back to level 2 when the health problem is solved.
What Is New and Conclusion
The provision of pharmaceutical services through three differentiated pharmacist intervention levels, based on the pharmacy customer´s health needs, seem to be a suitable model for the routine implementation of pharmaceutical care in the community pharmacy. Most of previously identified barriers for real imple-mentation of clinical services in the Pharmacy can be pulled down by the new strategy here proposed. The change of the focus from the product to the patient was the reason for the development of the model and is the consequence of its implementation.
Positive outcomes for patients, resulting from grow-ing clinical pharmacist interventions, will result also, certainly, in an added public recognition of the phar-maceutical profession.
References
1. From Making Medicines to Optimising Outcomes: the evolution of a profession 1912-2012. International Pharmaceutical Federation. Available on http://www.fip.org/centennial/files/ static/UCL_BOOKLET_Web.pdf (last access April 18, 2014). 2. Decreto-lei n.º 288/2001, 10 de novembro; Estatuto da Ordem dos Farmacêuticos. Available on http://www.ordemfarmaceuticos.pt/ xfiles/scContentDeployer_pt/docs/doc2848.pdf (last access April 18, 2014).
3. Martins S, Costa FA, Caramona M. Implementação de Cuidados Farmacêuticos em Portugal, Seis Anos Depois. Rev Port Farmacoter. 2013;5:255-263.
4. Gastelurrutia MA, Fernández-Llimos F, Benrimoj SI, Castrillon CC, Faus MJ. Barriers for the Implementation of Cognitive Services in Spanish Community Pharmacies. Aten Primaria. 2007;39(9):465-72.
5. Strand LM. A personal perspective on 25 years of pharmaceutical care. Conferencia de clausura. Seguim Farmacoter. 2004;(Supl 1):21-23.
6. Hughes CM, Hawwa AF, Scullin C, Anderson C, Bernsten CB, Björnsdóttir I, Cordina MA, da Costa FA, De Wulf I, Eichenberger P, Foulon V, Henman MC, Hersberger KE, Schaefer MA, Søndergaard B, Tully MP, Westerlund T, McElnay JC. Provision of pharmaceutical care by community pharmacists: a comparison across Europe. Pharm World Sci. 2010 Ago;32(4):472-487. 7. Community Pharmacy, the Accessible Local Healthcare Resource. Annual Report 2013. Pharmaceutical Group of European Union. Available on
http://www.pgeu.eu/en/library/1-annual-report/224-annual-report-2013.html (last access April 18, 2014).
8. Roberts AS, Benrimoj SI, Chen TF, Williams KA, Aslani P. Practice change in community pharmacy: quantification of facilitators. Ann Pharmacother. 2008 Jun;42(6):861-8.
9. Sorensen L, Stokes JA, Purdie DM, Woodward M, Elliott R, Roberts MS. Medication reviews in the community: results of a randomized, controlled effectiveness trial. Br J Clin Pharmacol. 2004 Dec;58(6):648-64.
Funding
No funding was received for this work.
Conflicts of Interest
No conflicts of interest to declare.