www.revportpneumol.org
ORIGINAL
ARTICLE
The
typical
presentation
of
an
atypical
pathogen
during
an
outbreak
of
Legionnaires’
disease
in
Vila
Franca
de
Xira,
Portugal,
2014
A.
Dias
a,∗,
A.
Cysneiros
a,
F.T.
Lopes
a,
B.
von
Amann
a,
C.
Costa
a,
P.
Dionísio
a,
J.
Carvalho
a,
V.
Durão
a,
G.
Carvalho
b,
F.
Paula
a,c,
M.
Serrado
a,
B.
Nunes
d,e,
T.
Marques
f,
F.
Froes
a,c,∗,
C.
Bárbara
a,gaChestDepartment,CentroHospitalarLisboaNorte,Lisboa,Portugal
bInternalMedicineDepartment,HospitaldeCascaisDr.JosédeAlmeida,Cascais,Portugal cIntensiveCareUnit,ChestDepartment,CentroHospitalarLisboaNorte,Lisboa,Portugal dEpidemiologyDepartment,InstitutoNacionaldeSaúdeDr.RicardoJorge,Lisboa,Portugal
eCenterforResearchinPublicHealth,EscolaNacionaldeSaúdePública,UniversidadeNOVAdeLisboa,Lisboa,Portugal fConsultantofDirectorate-GeneralofHealth,Portugal
gInstituteofEnvironmentalHealth(ISAMB),FacultyofMedicine,UniversityofLisbon,Lisboa,Portugal
Received28November2016;accepted23January2017 Availableonline1March2017
KEYWORDS
Legionnaires’disease; Outbreak;
Clinicalpresentation
Abstract
Background: AnoutbreakofLegionellapneumophilaserogroup1,with403caseswasidentified onthe7thNovember2014inVilaFrancadeXira,Portugal.Outbreaksourcewasthewetcooling systemofalocalfactory.HospitalPulidoValentewasoneofthehospitalsreceivingpatients withLegionnaires’disease(LD).
Methods:Wedescribetheclinicalfindingsanddiagnosticmethodsusedamongthe43confirmed orprobablecasesadmittedtoourdepartment.
Results:60.5%weremale,meanagewas56.1±13.5yearsandtobaccosmokingwasthemost frequentriskfactor(76.7%).Allpatientshadfever,62.8%≥39.5◦C,72.1%hadchillsand myal-gia/arthralgiaand62.8%haddrycough.Extrapulmonarysymptomswerefrequent:confusion andheadacheoccurredin34.9%andgastrointestinalsymptomsin20.9%.
HighC-ReactiveProtein(55.8%≥30mg/dL)andhyponatremia(62.8%)werethelaboratorial abnormalities mostcommonlyfound. Hypoxemiaoccurred in55.8% andhypocapnia in93%. UrinaryAntigenTest(UAT)waspositivein83.7%ofthecases.
Conclusions: Although notspecific, acombination ofrisk factors, symptomsandlaboratory findings can be highlysuggestiveofLD, evenin anoutbreak. This shouldprompt diagnosis
∗Correspondingauthors.
E-mailaddresses:[email protected](A.Dias),fi[email protected](F.Froes).
http://dx.doi.org/10.1016/j.rppnen.2017.01.007
2173-5115/©2017SociedadePortuguesadePneumologia.PublishedbyElsevierEspa˜na,S.L.U.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
confirmation.RoutineuseofUATinlessseverecasesofcommunityacquiredpneumoniamight contributetoearlierdiagnosis.
©2017SociedadePortuguesadePneumologia.PublishedbyElsevierEspa˜na,S.L.U.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Legionella species(spp.) is a relatively commonagent of communityandhospitalacquired pneumonia.1 Itwasfirst
identifiedasthepathogenresponsibleforapneumonia out-breakduringanAmericanLegionConventioninJuly1976in Philadelphia.Hence itsname,Legionnaires’ disease(LD).2
Itoccursinoutbreaksorsporadically.3,4
BacteriaofthegenusLegionella include56speciesand more than 70 serogroups. The most common specie is
Legionellapneumophila,serogroup1whichaccountsfor90%
ofcasesofLDandwastheagentresponsible forthe1976 outbreak.5,6Legionellapneumophilaserogroup1isfurther
dividedintomultiplesubtypes.
AlthoughL.pneumophilaserogroup1accountsfor90%of casesinEuropeandAmerica,thisincidencecouldbelower insomecountries,suchasAustraliaandNewZealand,where
Legionellalongbeacheaeaccountsfor30%ofcases.7
Theincubationperiodisusuallybetween2and10days.4,8
Inabout 10%ofcasestheincubation periodcanbelonger, lastingmorethan10daysandupto19days.9,10
Diagnosis is based on clinical suspicion together with laboratory confirmation. Legionella culture of a respira-tory specimen and urinary antigen testing are the most widely used.4,8 Although the clinical manifestations are
non-specific,a combinationof risk factors,symptomsand laboratorialfindingscanbesuggestiveofLD.11---13Itusually
presentsasseverepneumoniawithaparticularpatternof multisystemdysfunction.Aswithotherpneumoniascaused by ‘‘atypical pathogens’’, respiratory symptoms may not be the most prominent. Neurological and gastrointesti-nalinvolvement,myalgiaandarthralgia,hepaticcytolysis, hyponatremia,hypophosphatemiaandrenalfailureare fre-quentlypresent.4,11---15
An outbreak of L. pneumophila serogroup 1 with 403 cases,377confirmedand26probablecases,wasidentified onthe7thNovember2014inVilaFrancadeXira,located30 KmnorthofLisbon,Portugal.16Theoutbreakstartedonthe
12th October, with peakincidence on the 6th November. Control of outbreak was achieved onthe 21st November, withitsend declaredonthe 2ndDecember(dateof start of symptomsof the lastcase). Of the total of 403cases, therewere 14 reporteddeaths, leading toa 3.5% overall case fatalityrate. Epidemiological investigationidentified themostprobableoutbreaksourceasthewetcooling sys-temof alocalfactory.These facilitieswereshut downon the9thNovember.17Interestinglyitwasduringthisoutbreak
thattheveryfirstprobablepersontopersontransmissionof LDhasbeendescribed.18
During the outbreak several hospitals were appointed toreceive patientsfromVilaFrancadeXira,andHospital PulidoValente---CentroHospitalarLisboaNortewasoneof
them. Theauthors describetheclinical findingsand diag-nostic methodsused amongthe43 confirmed or probable casesofLDadmittedinourtrust.
Materials
and
methods
Forty-three patients withconfirmed or probable LD were admittedtotheChestDepartmentatHospitalPulidoValente betweenthe7thand15thNovember2014.Casedefinition wasbasedonestablishedcriteriabytheLegionnaires’ Dis-easeSurveillanceEuropean Union(EU)whichwasadopted by the Portuguese Directorate General of Health (DGH) (Table1).8,19
Aquestionnaire wasappliedtoallpatients transferred fromtheat riskareaswithaclinicalsuspicionofLD.Data regardingdemographics,riskfactors,clinicalpresentation, laboratorial and radiological features and microbiological testingwascollectedandanalyzed.
Asmokerwasdefinedasapersonwho,atthetimeofthe survey,hadsmokedatleast100cigarettesinhis/herlifetime andcurrentlysmokescigarettes everydayoroccasionally. Anex-smokerwasapersonwhousedtobeasmokerbuthad notsmokedat allforatleast6monthsatthetimeofthe survey.20
Statisticalanalysiswasperformedaimedatadescriptive analysis of the LD cases.More specificallyfor categorical variablesabsoluteandrelativefrequencieswerecalculated, fornumericalvariablesmeans,mediansandstandard devi-ations(sd)wereusedtocharacterizetheirdistribution.All dataanalysiswasperformedusingMicrosoftExcel(2007).
Results
Ofthe43patients,38(88.4%)wereconfirmedcasesand5 (11.6%)were probablecases.The totalof 43cases repre-sentsaround10.7%ofthetotal403casesidentifiedduring theoutbreak.
Allpatientsreceivedlevofloxacinandinourseriesthere werenodeaths.Sevenpatientswereadmittedtothe Inten-sive CareUnit (ICU) and11totheIntermediateCareUnit (ITCU). Invasive Mechanical Ventilation(IMV) wasneeded intwopatientsandNonInvasiveVentilation(NIV)ineight patients.Allpatientswereadmittedaftertheoutbreakhad beendeclared.ThemajoritywasfirstseenintheEmergency Room(ER)closesttotheoutbreaksource(HospitaldeVila FrancadeXira).
Feverwaspresentforameanof4.0daysbeforepatients soughtmedicalassistance.EverypatientwithsuspectedLD andepidemiologicallinkwasmedicatedwithhighdose levo-floxacin(750mg)beforebeingtransferredtoourhospital.
Table1 OutbreakcasedefinitionadoptedbyPortugueseDirectorate-GeneralofHealthbasedontheLegionnaires’Disease SurveillanceEuropeanUnion(EU)casedefinitioncriteria.
Casedefinition Probablecase:Anypersonmeetingtheclinicalandepidemiologicalcriteriaandat leastonelaboratorycriterionforaprobablecase
Confirmedcase:Anypersonmeetingtheclinicalandepidemiologicalcriteriaand atleastonelaboratorycriterionforaconfirmedcase
Clinicalcriteria Anypersonwithpneumonia
Epidemiologicalcriteria Symptomonsetoccurringbetween12/10/2014and02/12/2014andhistoryof living,workingorvisitingatriskareas7duringtheperiodof2to19daysbefore symptomonset.
Laboratorycriteriaforconfirmedcase Atleastoneofthethreefollowinglaboratoryfindings:a)isolationofLegionella
spp.fromrespiratorysecretionsoranynormallysterilesite;b)detectionof
Legionellapneumophilaantigeninurine;c)significantriseinspecificantibody leveltoLegionellapneumophilaserogroup1inpairedserumsamples.
Laboratorycriteriaforprobablecase Atleastoneofthefollowingfourlaboratoryfindings:a)detectionofLegionella pneumophilaantigeninrespiratorysecretionsorlungtissuee.g.byDFAstaining usingmonoclonal-antibodyderivedreagents;b)detectionofLegionellaspp. nucleicacidinrespiratorysecretions,lungtissueoranynormallysterilesite;c) significantriseinspecificantibodyleveltoLegionellapneumophilaotherthan serogroup1orotherLegionellaspp.inpairedserumsamples;d)singlehighlevel ofspecificantibodytoLegionellapneumophilaserogroup1inserum.
Table2 Demographicsandhostriskfactorsofthe43 con-firmed/probablepatients. Characteristics Confirmed/probable cases N(%) Gender Male 26(60.5) Female 17(39.5) Age(mean±SD) 56.1±13.5 Agemedian 59
Activesmokerorex-smoker 33(76.7)
Chronicrespiratorydisease 9(20.9)
COPD 6(14.0)
Asthma 2(4.7)
OSAS 2(4.7)
Diabetesmellitus 7(16.3)
Activecancer/Malignancy 1(2.3)
Chronictherapywithsystemic steroidsorother
immunosuppressivetreatment
0
≥1riskfactor 10(23.3)
SD:standarddeviation;COPD:ChronicObstructivePulmonary Disease;OSAS:ObstructiveSleepApneaSyndrome.
Patientswere maintainedonmonotherapy withhigh dose levofloxacinforameanperiodof8.9days.
Demographiccharacteristicsandhostriskfactors
Demographic characteristicsandhost risk factorsare pre-sented in Table 2. Twenty-six patients were maleand 17 were female.Mean age was56.1 and medianage was 59 yearsold.Theyoungestandoldestpatientswere22and85 yearsold,respectively.Aroundthreequarterswereofactive age:74.4%werewithin35---65years.
The main risk factors identifiedwere tobacco smoking (active smokers or ex-smokers) accounting for 76.7% of patients,chronic respiratorydisease (20.9%)and diabetes mellitus(16.3%).Morethan1riskfactorwaspresentin23.3% ofpatients.Onepatienthadgastriccancerandnonewere understeroidsorotherimmunosuppressivetreatment.HIV serologywasperformed in35patients(81.4%).HIV-2 sero-logywaspositiveinonepatientwithaCD4+lymphocytecell countof454cells/L.Althoughnotestablishedasarisk fac-tor,56.8%hadcardiovasculardisease,mainlyhypertension. Clinical,laboratorialandradiologicalpresentation Clinicalfeatures,radiologicalandlaboratoryresultsare pre-sentedinTable3.Allpatientshadfever(T≥38◦C),in79.1% ofpatients≥39◦C,in62.8%≥39.5◦Candmaximum temper-aturewas40.5◦C.
Chills,myalgia andarthralgiawerepresent in72.1% of the patients. Dry cough was the most frequent respira-torysymptom (62.8%)andproductivecough wastheleast (16.3%).Bothdyspneaandchestpainwerepresent inless than40%ofthecases.Extrapulmonarysymptomswere fre-quent, with 34.9% of patients presenting with confusion and/orheadache.Gastrointestinalsymptoms,suchas nau-sea,vomitingand diarrheawerereportedin 20.9%of the patients.
Fifty-sixpercentofthepatientshadC-ReactiveProtein (CRP)above30mg/dL (meanvalueof 33.8,minimum14.3 andmaximum66.9mg/dL).Leukocytosiswasfoundin48.8% ofthepatients(meanvalueof12210×109cells/L).Normal plateletcount (150---450×109/L) wasfound in the major-ityofpatients(n=36,83.7%)and22.5%hadplateletcount below171×109/L.Themostcommonlaboratory abnormal-itieswere:hyponatremia(Na<135mmol/L)in 62.8%,with Na<130in20.9%,hepaticcytolysis(AST>34U/L)in54.8%, raisedcreatininein51.2%,andhypophosphatemiain42.9% ofthecases.
Table3 Clinicalandlaboratoryfeatures.
Characteristics Confirmed/probable cases
N(%)
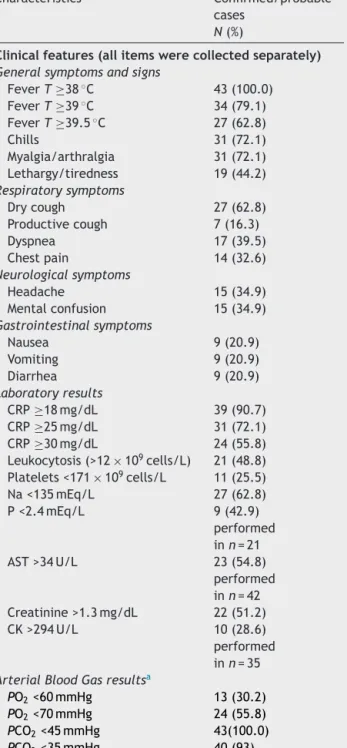
Clinicalfeatures(allitemswerecollectedseparately)
Generalsymptomsandsigns
FeverT≥38◦C 43(100.0) FeverT≥39◦C 34(79.1) FeverT≥39.5◦C 27(62.8) Chills 31(72.1) Myalgia/arthralgia 31(72.1) Lethargy/tiredness 19(44.2) Respiratorysymptoms Drycough 27(62.8) Productivecough 7(16.3) Dyspnea 17(39.5) Chestpain 14(32.6) Neurologicalsymptoms Headache 15(34.9) Mentalconfusion 15(34.9) Gastrointestinalsymptoms Nausea 9(20.9) Vomiting 9(20.9) Diarrhea 9(20.9) Laboratoryresults CRP≥18mg/dL 39(90.7) CRP≥25mg/dL 31(72.1) CRP≥30mg/dL 24(55.8) Leukocytosis(>12×109cells/L) 21(48.8) Platelets<171×109cells/L 11(25.5) Na<135mEq/L 27(62.8) P<2.4mEq/L 9(42.9) performed inn=21 AST>34U/L 23(54.8) performed inn=42 Creatinine>1.3mg/dL 22(51.2) CK>294U/L 10(28.6) performed inn=35
ArterialBloodGasresultsa
PO2<60mmHg 13(30.2)
PO2<70mmHg 24(55.8)
PCO2<45mmHg 43(100.0)
PCO2<35mmHg 40(93)
aABGperformedatadmissionwithFIO 221%.
Allpatientshadarterialbloodgassamplesdrawnonroom air(FiO221%)onadmission.Hypoxemia(PO2<70mmHg)was foundin55.8%ofthepatientsand93%hadhypocapnia(PCO2 <35mmHg).
Allpatients had achest X-ray onadmission document-ingevidenceofpneumonia.X-raywasrepeatedwithin72h, despiteclinicalevolution.Fourteenpercent(n=6)had bilat-eralinvolvement at admission and half of these patients were treated in the intermediate/intensive Care Units. Twenty-three percent (n=10) had worsening radiological
featureswithinthefirst72hof hospitalizationandhalf of themwereadmittedtotheICU.
Microbiologicaltesting
AllpatientshadUrinaryAntigenTestingforL.pneumophila
serogroup 1 (Alere BinaxNOW® Legionella Urinary Antigen Card).Thiswaspositiveinn=36(83.7%).Inthe36confirmed casesby UAT,serologywasnot performedand respiratory secretions werecollected in 15patients, and culturewas positive in 6. Among the 7 patients with negative UAT, there weretwo additionalconfirmed cases:one by
isola-tionofLegionellaspp.fromrespiratorysecretionsandone
byanalysisofsignificantserologicaltiterelevationinpaired samples.The5remainingcaseswereprobablecases,with a singlehigh level ofspecific antibody toL.pneumophila
serogroup1inserum.
Bloodcultureswereperformed inallpatientsand neg-ativeinallforanypathogen,specificallyforStreptococcus pneumoniae.
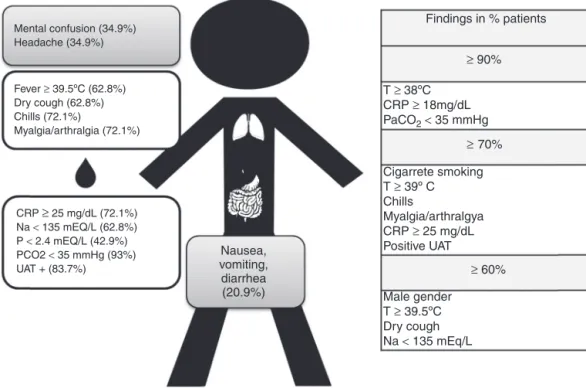
Fig.1showsthestandarddemographicandclinical find-ingsofLDinourstudiedpopulation(our‘‘typical’’patient).
Discussion
To date, the largest outbreak of LD happened in Murcia, Spainin2001with449confirmedcases.TheVilaFrancade Xiraoutbreak,with403cases,wasthesecondlargest.16,17,21
Theoutbreakstartedonthe12thOctober2014butwas only declared, 26 days later, on the 7th November.8 Our
study was not able to identify the reason for the delay in declaring the outbreak, but we hypothesize that this could be related to the high population density of the areaaffectedbytheoutbreakandthenumberofdifferent health care facilities involved. Other reasons include the factthattherearenonationalrecommendationsin Portu-galforrequestingUATinpatientswithCommunityAcquired Pneumonia.As for this,UATisperformed insevere cases, those admitted to ICU or during an outbreak, as recom-mended by the Portuguese Respiratory Society guidelines forthemanagementofcommunity---acquiredpneumoniain immunocompetentadults.22
As the outbreak had already been declared when the patientswereadmittedtoourhospital,UATwasperformed onallofthem,regardlessofdiseaseseverity.
Althoughourpopulationofpatientsamountedto43cases (10.7%ofthetotalnumberofcases)webelieveitis repre-sentativeoftheclinicalmanifestationsofLD,whicharein linewiththeliterature.Thedistributionofgenderandage reflect the demographic characteristics of the population exposedtocontamination.Thisismainlyaworking popula-tioninanindustrialarea,manyofwhomcommutetowork inthecapital.
All series report a greater incidence in males11,14,23,24
althoughtheagedistributioninourserieswasyoungerwith 74.4%ofcasesbeingbetween35and65yearsofagewith ameanageof56.1years.TheMurciaoutbreakshowedan olderpopulationwith70%ofpatientsbeingolderthan5021
andinthereviewbySopena52.2%whereolderthan60.3In
theanalysisofCAPNETZbyvonBaumetal.,themeanage was63.25
Patient ID: male, 56 years old Findings in % patients T ≥ 38ºC CRP ≥ 18mg/dL PaCO2< 35 mmHg Cigarrete smoking T ≥ 39º C Chills Myalgia/arthralgya CRP ≥ 25 mg/dL Positive UAT Male gender T ≥ 39.5ºC Dry cough Na < 135 mEq/L ≥ 60% ≥ ≥ 90% 70% Mental confusion (34.9%) Headache (34.9%) Fever ≥ 39.5ºC (62.8%) Dry cough (62.8%) Chills (72.1%) Myalgia/arthralgia (72.1%) CRP ≥ 25 mg/dL (72.1%) Na < 135 mEQ/L (62.8%) P < 2.4 mEQ/L (42.9%) PCO2 < 35 mmHg (93%) UAT + (83.7%) Nausea, vomiting, diarrhea (20.9%)
Figure1 Our‘‘typical’’patient.
Our series showed that the most prevalent risk factor wassmokinghistory(currentorpast)whichwaspresentin 76.7%ofpatients.Againthiswasinaccordancewithprevious series.3,25---27Chronicrespiratorydiseases,frequentlyquoted
asariskfactor, 9.7%intheSopenaseries3and36%invon
Baum’s,25 wasidentifiedin 20.9%of ourpopulationIn our
series,diabetesmellituswasfoundin16.3%ofpatients. Sim-ilarvalueswerealsofoundinotherstudies.3,13,26However,
diabetesmellitus prevalencein thePortuguesepopulation aged20---79yearsoldwas13.1%in2014.28Also,inan
out-breakofLDin2000inMelbourne,Australia,acase---control study did not find significant difference in risk factors between patients and the general population, with the exceptionofsmoking.26
Thelowincidenceofimmunosuppressivetherapyand/or active cancer as well as a high incidence of high blood pressure in the population reflect the demographic char-acteristicsandis likelytohave noother significance.Itis unknown what the HIV prevalence wasin the population exposed to LD outbreak, however the patient diagnosed withHIV-2hadaCD4lymphocytecellcount≥350cells/L. Thus, in this patient HIV infection probably did not con-tributesignificantlyasarisk factor forLD, whichremains inaccordancetootherpublisheddata.29
Allpatientshadfever,≥39◦Cinnearly80%ofpatients. Accordingtosomeauthorsthisaloneshouldraisethe sus-picionofLD.15Asexpected,respiratorysymptomswerenot
predominant,withthemostcommonbeingadrycoughin two thirds of patients.15,30 Chills, myalgia and arthralgia
werepredominantinourseries(72.1%ofcases)andis doc-umented intheliterature,15 howeverthelatter wasmore
prevalentwhencomparedwithotherstudiesthatquoteda prevalencearound40%.15,30,31
Aroundonethirdofpatientshadneurologicalcomplaints (headacheand/orconfusion)and20.9%hadgastrointestinal symptoms,mainlydiarrhea,nauseaandvomit.Thesevalues aresimilartovaluesfromotherstudies.15,23,30,32
Regarding laboratory findings our series confirms very high CRP (mean value: 33.8mg/dL) which is in line with otherseries.13,33,34Other findingsalreadydescribed inthe
literatureincludehyponatraemia,13,30,35hypophosphatemia,
raised liver enzymes and decreased renal function.15
AlthoughCRPwasmarkedlyhigh,51%ofthepatientsdidnot haveraised whitecellcountorneutrophilia, whichagain, wasfoundbySopena,3Viasus30andBenito.32
In25.5% of patients,therewasa plateletcountbelow 171×109/L, which is one of the independent predic-tor variables in the LD score proposed by Fiumefreddo etal.13
Themajorityofpatientshadhypoxemia(PO2<70mmHg), with30.2%havingPO2<60mmHg,findingsthataresimilarto thosefoundbyBenitoetal.,32with33%andSopenaetal.3
with31%.Itisunusualtofindanyreferencesintheliterature toPCO2valuesbutourseriesshowedthatPCO2wasbelow 35mmHgin93%ofpatientsandthishypocapniacouldbean indirectmarkeroftachypnea.
Twenty-three percent of cases showed worsening of radiologicalfindingsduringthefirst72hofadmission.This hasbeendescribedinotherstudies36suggestingthatitcould
beamoreparticular featureofLD thanofother pneumo-nias.HalfofthesepatientsneededadmissiontotheICUand tworequiredIMV.
Despitebeinghighlysensitive,asensitivitycloseto100% according to Rihs et al.,37 the UAT for L. pneumophila
serogroup 1(Alere BinaxNOW® Legionella Urinary Antigen Card),which wasappliedtoallourpatients,waspositive
in83.7%.AnevensmallernumberwasfoundintheMurcia outbreak,withonly47.7%ofthecaseshavingpositiveUAT. Thevariabilityofsensitivitycouldreflectdiseaseseverity; withhigherpositiveratesinmoreseveredisease.38Ourdata
alsoquestions theindication for blood culturesduring LD outbreaks.
Finally,inourseriesallpatientsweretreatedwithhigh doselevofloxacininmonotherapyandtherewerenodeaths. However, alertness was high because the outbreak had already been declared when our patients were admitted (after7thNovember2014).Toevaluatecasefatalityrate, theDGHincludeddeathsoccurringsince1stOctober2014 andafewpatientsdiedwithinthisperiod.8
Inourseriesearlydiagnosis,prompttreatmentand opti-mizationofprocessofcaremayhavecontributedtothese results.
Conclusions
Although clinical presentation is not specific, our study shows that even during an outbreak, the combination of riskfactors,symptomsandlaboratoryfindingscanbehighly suggestiveofLD.Thiscanandshouldpromptfurther inves-tigations in order to confirm LD, particularly in patients withless severe presentation or withnegative UAT. Also, widespreaduseof UAT,notlimitedtothesevere casesof communityacquired pneumonia withICU admission crite-ria,mightcontributetoearlierdiagnosis,both insporadic casesandinoutbreaksofLD.
Ethical
responsibilities
Protection of human and animal subjects.The authors
declarethatnoexperimentswereperformedonhumansor animalsforthisstudy.
Confidentialityofdata.Theauthorsdeclarethattheyhave followedtheprotocolsoftheirworkcenteronthe publica-tionofpatientdata.
Righttoprivacyandinformedconsent.Theauthorshave
obtainedthe written informed consentof the patients or subjectsmentionedinthearticle.Thecorrespondingauthor isinpossessionofthisdocument.
Conflict
of
interest
Theauthorsdeclarethattheyhavenoconflictofinterest.
Acknowledgments
The authors would like to thank Dr. Francisco George, Director-GeneralofthePortuguese DirectorateGeneralof Health.
References
1.MarrieTJ,PeelingRW,FineMJ,SingerDE,ColeyCM,Kapoor WN.Ambulatorypatientswithcommunity-acquiredpneumonia: thefrequencyofatypicalagentsandclinicalcourse.AmJMed. 1996;101:508---15.
2.FraserDW,TsaiTR,OrensteinW,ParkinWE,BeechamHJ, Shar-rarRG,etal.Legionnaires’disease:descriptionofanepidemic ofpneumonia.NEnglJMed.1977;297:1189---97.
3.SopenaN,ForceL,Pedro-BotetML,BarrufetP,SaucaG, García-Nú˜nezM,etal.Sporadicandepidemiccommunitylegionellosis: twofacesofthesameillness.EurRespirJ.2007;29:138---42. 4.Diederen BMW. Legionella spp. and Legionnaires’ disease. J
Infect.2008;56:1---12.
5.BeninA,BensonR,BesserR.TrendsinLegionnaires’disease, 1980---1998:decliningmortalityandnewpatternsofdiagnosis. ClinInfectDis.2002;35:1039---46.
6.JosephJ.EuropeanWorkingGroup for Legionella Infections. Legionnaires’sDiseaseinEurope2000---2002.EpidemiolInfect. 2004;132:417---24.
7.YuVL,PlouffeJF,PastorisMC,StoutJE,SchousboeM,Widmer A,etal.DistributionofLegionellaspeciesandserogroup iso-latedbycultureinpatientswithsporadiccommunityacquired legionellosis:aninternationalcollaborativesurvey.JInfectDis. 2002;186:127---8.
8.Direc¸ão-Geral da Saúde Relatório do Surto de Doenc¸a dos LegionáriosdeVila FrancaDeXira. Direcc¸ão-Geral daSaúde 2015(www.dgs.pt).Datelastupdated:June1,2015.Datelast accessed:June1,2015.
9.EuropeanCentrefor DiseasePreventionand Control. Legion-naires’ disease outbreak investigation Toolbox. https: //legionnaires.ecdc.europa.eu/?pid=107. Date last accessed: January06,2017.
10.DenBoerJW,YzermanE,SchellekensJ,LettingaKD,Boshuizen HC,VanSteenbergenJE,etal.AlargeoutbreakofLegionnaires’ diseaseataflowershow,theNetherlands,1999.EmergInfect Dis.2002;8:37---43.
11.MulazimogluL,YuVL.Canlegionnairesdiseasebediagnosedby clinicalcriteria?Chest.2001;120:1049---53.
12.CunhaBA. Legionnaires’diseaseclinicaldifferentiationfrom typicaland otheratypicalpneumonias.Infect DisClinNAm. 2010;24:73---105.
13.Fiumefreddo R, Zaborsky R, Haeuptle J. Clinical predictors forLegionellainpatientspresentingwithcommunity-acquired pneumonia to the emergency department. BMC Pulm Med. 2009;9:4.
14.Chidiac C, Che D, Pires-Cronenberger S. Factors associated withhospitalmortalityincommunity-acquiredlegionellosisin France.EurRespirJ.2012;39:963---70.
15.YuVL, Stout JE,Sopena N.Clinicalmanifestationsand diag-nosisofLegionella infection. UpToDate 2016.http://www. uptodate.com/contents/clinical-manifestations-and-diagnosis-of-legionella-infection?source=seelink. Date last updated: April07,2016.Datelastaccessed:June01,2016.
16.GeorgeF,ShivajiT,SousaPintoC.Alargeoutbreakof Legion-naires’DiseaseinanindustrialtowninPortugal.RevPortSaúde Pública.2016;34:199---208.
17.ShivajiT,SousaPintoC,San-BentoA.Alargecommunity out-breakofLegionnaires’diseaseinVilaFrancadeXira,Portugal, OctobertoNovember2014.EuroSurveill.2014;19,pii=20991. 18.Correia AM,Ferreira JS,Vítor Borges V. Probable
person-to-persontransmission ofLegionnaires’ disease. N Engl J Med. 2016;374:497---8.
19.EuropeanCentrefor DiseasePreventionand Controlwebsite; Legionellosis Surveillance EU case definition. http://ecdc. europa.eu/en/healthtopics/legionnairesdisease/surveillance/ Pages/EU-case-definition.aspx.Datelastaccessed:August17, 2016.
20.WorldHealth Organization (WHO). Guidelines for controlling andmonitoringthetobaccoepidemicWHOtobaccoorhealth programme.Geneva;1997.
21.García-FulgueirasA,NavarroC,FenollD.Legionnaires’disease outbreakinMurcia,Spain.EmergInfectDis.2003;9:915---21. 22.FroesF,Diniz A, Henriques J, Ramalho de Almeida A, Alves
C,Amado J,et al.PortugueseRespiratorySocietyguidelines forthemanagement ofcommunity--- acquiredpneumoniain immunocompetentadults.RevPortPneumol.2003;IX:435---61. 23.SopenaN,Sabrià-LealM,Pedro-BotetML.Comparativestudy
of the clinical presentation of Legionella pneumonia and other community acquired pneumonias. Chest. 1998;113: 1195---200.
24.UedaA,OkiM,YanagiH.ClinicalcharacteristicsofLegionella
pneumonia diagnosed with Legionella urinary antigen test. TokaiJExpClinMed.2016;41:8---13.
25.vonBaumH,EwigS,MarreR.Community-acquiredLegionella
pneumonia:new insights fromthe Germancompetence net-work for community acquired pneumonia. Clin Infect Dis. 2008;46:1356---64.
26.GreigJE,CarnieJA,TallisGF,RyanNJ,TanAG,GordonIR,etal. AnoutbreakofLegionnaires’diseaseattheMelbourne Aquar-ium,April2000:investigationandcase---controlstudies.MedJ Aust.2004;180:566---72.
27.DenBoer JW, NijhofJ, Friesema I.Risk factors for sporadic community-acquiredLegionnaires’disease. A3-year national case-controlstudy.PublicHealth.2006;120:566---71.
28.Sociedade Portuguesa de Diabetologia. Diabetes Factos e Números --- O Ano de 2014 --- Relatório Anual do Obser-vatório Nacional da Diabetes; 2015. http://spd.pt/images/ ond2015.pdf.Datelastaccessed:January01,2017.
29.SandkovskyU,SandkovskyG,SuhJ,SmithB,SharpV,PolskyB. LegionellapneumoniaandHIV:casereportsandreviewofthe literature.AIDSPatientCareSTDs.2008;22:473---81.
30.ViasusD, YacovoS, Garcia-VidalC, VerdaguerR, Manresa F, Dorca J,et al. Community-acquiredLegionella pneumophila pneumonia. A single-center experience with 214 hospital-ized sporadic cases over 15 years. Medicine (Baltimore). 2013;92:51---60.
31.GranadosA,PodzamczerD,GudiolF,ManresaF.Pneumoniadue toL.pneumophilaandpneumococcalpneumonia:similarities anddifferencesonpresentation.EurRespirJ.1989;2:130---4. 32.BenitoJR,MontejoJM,LauraCanceloL,ZalacaínR,LópezL,
GildeParejaJF,et al.NeumoníacomunitariaporLegionella pneumophilaserogrupo1.Estudiode97casos.EnfermInfecc MicrobiolClin.2003;21:394---400.
33.HaubitzS,HitzF,GraedelL.RulingoutLegionellain community-acquiredpneumonia.AmJMed.2014;127,1010.e11---1010.e19. 34.VázquezEG,MartínezJA,MensaJ,SánchezF,MarcosMA,de RouxA,etal.C-reactiveproteinlevelsincommunityacquired pneumonia.EurRespirJ.2003;21:702---5.
35.YuVL,KrobothFJ, ShonnardJ,BrownA, McDearmanS, Mag-nussenM,etal.Legionnaires’disease:newclinicalperspective fromaprospectivepneumoniastudy.AmJMed.1982;73:351---7. 36.Tan MJ, Tan JS, Hamor RH, File TM Jr, Breiman RF. The radiologic manifestations of Legionnaire’s disease. Chest. 2000;116:398---403.
37.RihsJD,JarraudS,LuckC,etal.Lackofcomparable sensitiv-ityandspecificityamongsevenLegionellaurinaryantigentest kits:aninternationalcollaborativestudy(abstractno.2473). In:50thinterscience conferenceonantimicrobialagentsand chemotherapy.2010.
38.Blázquez RM, Espinosa FJ, Martínez-Toldos CM, Alemany L, García-Orenes MC, Segovia M. Sensitivity of urinary antigen test in relation to clinical severity in a large outbreak of
LegionellapneumoniainSpain.EurJClinMicrobiolInfectDis. 2005;24:488---91.