www.revportpneumol.org
ORIGINAL
ARTICLE
Does
any
association
exist
between
Chronic
Obstructive
Pulmonary
Disease
and
Erectile
Dysfunction?
The
DECODED
study
夽
M.
Dias
a,∗,
M.J.
Oliveira
a,
P.
Oliveira
b,c,
I.
Ladeira
a,
R.
Lima
a,
M.
Guimarães
a aPulmonologyDepartment,CentroHospitalarVilaNovadeGaia/Espinho,VilaNovadeGaia,PortugalbISPUP-EPIUnit,UniversidadedoPorto,Porto,Portugal
cPopulationStudiesDepartment,InstitutodeCiênciasBiomédicasAbelSalazar(ICBAS),UniversidadedoPorto,Portugal
Received13February2017;accepted18April2017 Availableonline16June2017
KEYWORDS Chronicobstructive pulmonarydisease; Erectiledysfunction; Sexualactivity Abstract
Introduction:Erectiledysfunction(ED)istheinabilitytoachieveormaintainanerectionfor satisfactorysexualactivity.RecentstudieshaveshownanassociationbetweenEDandchronic obstructivepulmonarydisease(COPD).However,thisissueisoftenignored.Weaimedto eval-uatetheEDprevalenceinCOPDpatientsanditsriskfactorsandtostudytheimpactofdyspnea insexualactivity.
Methods:Cross-sectional study thatincluded sexuallyactivemalepatients with COPD.The InternationalIndexofErectileFunction(IIEF-5)questionnaireevaluatedEDandthe Respira-toryExperienceswithSexualityProfile(RESP)wasusedtoevaluatetheimpactofdyspneaon sexualactivity.Riskfactorsformild-moderateormoderateEDweredeterminedusinglogistic regression.
Results:84patientswereconsecutivelyassessedforeligibility,67wereincluded(medianage: 65 years, 13% never-smokers). Twenty two percent had COPD 2011-GOLD A; 22% GOLD B, 14% GOLD C and42% GOLD D. Fifty-eight patients (87%) hadsome degree ofED: 26 (45%) mild,20(34%)mild-moderateand12(21%)moderateED.EDoccurredinallGOLD stagesof COPD,mainlyinGOLDBandDstages.HigherCATscorewasindependentlyassociatedto mild-moderate/moderateED.Mostpatients(85%)reporteddyspneaduringtheirsexualactivitybut 72%hadnevertalkedaboutitwiththeirphysician.
夽 Institutionwherethestudywasperformed:CentroHospitalarVilaNovadeGaia/Espinho,VilaNovadeGaia,Portugal. ∗Correspondingauthor.
E-mailaddress:[email protected](M.Dias).
http://dx.doi.org/10.1016/j.rppnen.2017.04.005
2173-5115/©2017SociedadePortuguesadePneumologia.PublishedbyElsevierEspa˜na,S.L.U.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Conclusions:EDishighlyprevalentamongCOPDpatientsanditismoresevereinpatientswith higherCATscores.Dyspneaaffectstheirsexualactivitybutthisisnotatopicoftendiscussed betweenpatientsanddoctors,somethingwhichneedstobeimproved.
©2017SociedadePortuguesadePneumologia.PublishedbyElsevierEspa˜na,S.L.U.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Chronicobstructivepulmonarydisease(COPD)isacommon preventableandtreatablediseasecharacterizedby persis-tentrespiratorysymptomsandairflowlimitation.1However,
COPDisnotonlyapulmonarydiseasebutalsoachronic ill-nessassociatedwithsystemicinflammationandwithvarious comorbiditiesinvolvingmultipleorgans.1---3
Erectiledysfunction(ED)isaconditionofinabilityto per-sistentlyreachand/ormaintainanadequateandnecessary erectiontohavesatisfactorysexualactivity.4
GOLDguidelinesstatethatsexualactivityshouldbe eval-uatedin allCOPDpatients,but theydonotincludeED as oneofthepossiblecomorbiditiesofCOPD.1However,some
studieshavereportedEDasacommoncomorbidityinCOPD patientsbutthisisstillanunder-researchedarea.5---8
More-over, theinformationabout the impactof therespiratory symptomsonsexualactivityamongCOPDpatientsissparse.9
Theaimsofthisstudyweretodeterminetheprevalence ofED amongpatients withCOPD,toinvestigatetheCOPD patients’characteristicsassociatedwithEDandtheimpact ofCOPDsymptomsonsexualactivityand,therefore,draw attentiontothisissue.
Methods
StudydesignAcrosssectionalstudywasconductedonCOPDoutpatients followed in the Pulmonology department of a Portuguese hospital,CentroHospitalarVilaNovadeGaia/Espinho.
Inclusion criteriawere: beingmale, having a diagnosis of COPD and having had sexual relations in the previous 6 months. The exclusion criteriawere: having ED caused by structuralor anatomicalterations or havingany COPD exacerbationinthepreviousmonth.Patientswereincluded consecutivelyduringa6-monthperiod.
Datacollection
Abookletcontainingaquestionnairedividedintotwoparts wasused.The firstpartofthequestionnairewas adminis-teredby amedicaldoctor. It evaluatedseveralvariables, such as demographic data, marital status, level of edu-cation,smokingstatus,modifiedMedicalResearchCouncil Dyspnea Scale (mMRC),10 COPD Assessment Test (CAT)11
score, the levels of anxiety and depression according to the Hospital Anxiety and Depression Scale (HADS),12
co-morbiditiesandmedication.
Thesecondpartofthequestionnairewasfilledoutbythe patientaloneintheoutpatientroomandincludedtheshort versionoftheInternationalIndexofErectileFunction (IIEF-5)13 to evaluate ED and the Respiratory Experiences with
SexualityProfile(RESP)9toassesstheimpactofdyspneaon
sexualactivity.
On the same day that the questionnaire was admin-istered, all patients had a pulmonary function test using a spirometer (MasterScopeTM, CareFusion, Höchberg, Ger-many).
ThestudywasapprovedbytheMedicalEthical Commit-teeofCentroHospitalarVilaNovadeGaia/Espinhoandall patientssignedaninformedconsentformpriortothestudy. Definitions
COPDwasdefinedasthepresenceofapost-bronchodilator forced expiratory volume in 1s (FEV1) over forced vital capacity(FVC)ratiobelow0.70.1COPDstagesweredefined
according2011GOLDguidelines.14
Comorbiditywasdefinedasthepresenceofoneormore diseases, except COPD, that could be caused by or be directlyrelatedtoCOPD,regardlessofwhetheritwaspart ofthenaturalspectrumofCOPD.15
EDwasdefinedaccordingtotheIIEF-5score.13TheIIEF-5
questionnairehasamaximumscoreof25points(1---7points: severeED;8---11:moderateED;12---16points:mild-moderate ED;17---21:mildED;22---25points:noED)(AppendixA). Statisticalanalysis
The age-adjustedprevalence wascalculatedbythedirect method,assumingthetotalstudypopulationasstandard.
Descriptive statistics of the variables of interest were expressedasabsoluteandrelativefrequenciesormeanand standard deviation.Chisquared andMann---WhitneyUtest were used to compare groups. The strength of the asso-ciationbetween IIEF-5scoreandtheother medicalscores wasevaluatedbythePearsonorSpearman-rankcorrelation coefficient,asappropriate.
Logisticregression wasusedtoidentifythe riskfactors forEDamongCOPDpatients.
AllstatisticalanalyseswerecarriedoutusingtheIBMSPSS StatisticsforMacintosh,version22.0.(Armonk,NY,USA:IBM Corp).Thesignificancelevelwassetat0.05.
Results
Atotalof84patientswereassessedforeligibility.Ofthese, 17wereexcludedfromanalysisdueto:refusaltoparticipate
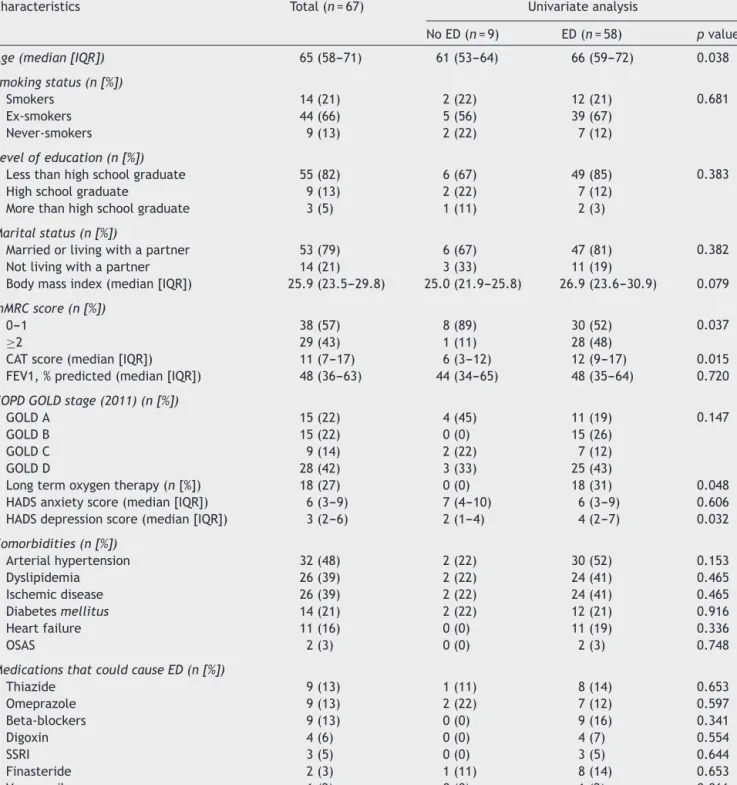
Table1 Demographicandclinicalcharacteristicsofthepatientsandunivariateanalysisoffactorsassociatedtothepresence oferectiledysfunctioninthesepatients.
Characteristics Total(n=67) Univariateanalysis
NoED(n=9) ED(n=58) pvalue
Age(median[IQR]) 65(58---71) 61(53---64) 66(59---72) 0.038
Smokingstatus(n[%])
Smokers 14(21) 2(22) 12(21) 0.681
Ex-smokers 44(66) 5(56) 39(67)
Never-smokers 9(13) 2(22) 7(12)
Levelofeducation(n[%])
Lessthanhighschoolgraduate 55(82) 6(67) 49(85) 0.383
Highschoolgraduate 9(13) 2(22) 7(12)
Morethanhighschoolgraduate 3(5) 1(11) 2(3)
Maritalstatus(n[%])
Marriedorlivingwithapartner 53(79) 6(67) 47(81) 0.382 Notlivingwithapartner 14(21) 3(33) 11(19)
Bodymassindex(median[IQR]) 25.9(23.5---29.8) 25.0(21.9---25.8) 26.9(23.6---30.9) 0.079
mMRCscore(n[%])
0---1 38(57) 8(89) 30(52) 0.037
≥2 29(43) 1(11) 28(48)
CATscore(median[IQR]) 11(7---17) 6(3---12) 12(9---17) 0.015 FEV1,%predicted(median[IQR]) 48(36---63) 44(34---65) 48(35---64) 0.720
COPDGOLDstage(2011)(n[%])
GOLDA 15(22) 4(45) 11(19) 0.147
GOLDB 15(22) 0(0) 15(26)
GOLDC 9(14) 2(22) 7(12)
GOLDD 28(42) 3(33) 25(43)
Longtermoxygentherapy(n[%]) 18(27) 0(0) 18(31) 0.048 HADSanxietyscore(median[IQR]) 6(3---9) 7(4---10) 6(3---9) 0.606 HADSdepressionscore(median[IQR]) 3(2---6) 2(1---4) 4(2---7) 0.032
Comorbidities(n[%]) Arterialhypertension 32(48) 2(22) 30(52) 0.153 Dyslipidemia 26(39) 2(22) 24(41) 0.465 Ischemicdisease 26(39) 2(22) 24(41) 0.465 Diabetesmellitus 14(21) 2(22) 12(21) 0.916 Heartfailure 11(16) 0(0) 11(19) 0.336 OSAS 2(3) 0(0) 2(3) 0.748
MedicationsthatcouldcauseED(n[%])
Thiazide 9(13) 1(11) 8(14) 0.653 Omeprazole 9(13) 2(22) 7(12) 0.597 Beta-blockers 9(13) 0(0) 9(16) 0.341 Digoxin 4(6) 0(0) 4(7) 0.554 SSRI 3(5) 0(0) 3(5) 0.644 Finasteride 2(3) 1(11) 8(14) 0.653 Verapamil 1(2) 0(0) 1(2) 0.866
IQR:interquartilerange;mMRC:ModifiedBritishMedicalResearchCouncil;CAT:ChronicObstructivePulmonaryDiseaseAssessmentTest; FEV1:forcedexpiratoryvolumeinthefirstsecond;COPD:chronicobstructivelungdisease;HADS:HospitalAnxietyandDepressionScale; OSAS:obstructivesleepapneasyndrome;ED:erectiledysfunction;SSRI:selectiveserotoninreuptakeinhibitor.
(n=6),havingnosexualrelationsintheprevious6months (n=6),havingaCOPDexacerbationin thepreviousmonth (n=3)andhavingEDduetoanatomicalterations(n=2).
The characteristics of the 67 patients included in the studyarepresentedinTable1.Patientshadamedianage of65yearsandmost(66%)wereex-smokers.
RegardingCOPDstage,22%ofthepatientswereGOLDA, 22%wereGOLDB,14%wereGOLDCand42%wereGOLDD. There was no comorbid disease in 19 (28%) of the patients.Theremainingpatientshadatleastone comorbid-ity,mostlyarterial hypertension(48%),dyslipidemia(39%) andischemicdisease(39%).Forty-onepatients(61%)hadno
Table2 Multiplelogisticregressionmodeltoidentifyfactorsassociatedtomild-moderateormoderateerectiledysfunction amongCOPDpatients.
Variables Coefficients Standarderrors pvalue OR(95%CI)
Constant −1.927 0.663 0.004
---mMRCscore≥2 1.061 0.584 0.069 2.889(0.919---9.082)
CATscore 0.116 0.053 0.029 1.123(1.012---1.247)
mMRC:Modified BritishMedicalResearchCouncil;CAT: ChronicObstructivePulmonary DiseaseAssessmentTest;OR:oddsratio;CI: confidenceinterval.
medicationthatcouldcauseED. Noneof thepatientswas takinganymedicationforED.
AccordingtotheIIEF-5score,58 (87%)patientshadED withvaryingdegrees:26(45%)mild,20(34%)mildto moder-ateand12(21%)moderateED.Therewerenopatientswith severeED.Theage-adjustedprevalenceofEDwas80%.
The patient characteristics associated tothe presence ofED areshown inTable1. PatientswithED were signifi-cantlyolder(66vs.61,p=0.038),hadmorefrequentlyan mMRCscore≥2(48vs.11%,p=0.037),ahighermedianCAT score(12vs.6,p=0.015)andahighermedianHADS depres-sion score (4 vs. 2, p=0.032). Those patients were more frequentlyreceivinglongtermoxygentherapy(31%vs.0%,
p=0.048).
As thenumberofpatientswithout ED wassmall, logis-tic regression was not performed. Instead, we divided ourpopulation into 2groups (noED/mild ED versus mild-moderate/moderateED)andperformedalogisticregression toevaluateriskfactorsformild-moderateormoderateED (n=32)(Table2).ThefinalmodelidentifiedtheCATscore tobepositivelyassociatedwithmild-moderateormoderate ED(OR=1.123[1.012---1.247]).Thatis,foreachincreaseof 1point in CAT score, the oddsof mild-moderateor mod-erateEDincrease 112%.Moreover,mMRCscore≥2tended tobepositivelyassociatedwithmild-moderateormoderate ED,although itwasnotstatisticallysignificant (OR=2.889 [0.919---9.082]).Therefore,sincethesampleissmallandthe
p valuefor mMRCis closeto0.05,we decidedtoinclude mMRCscoreinthefinalmodel.
Weevaluatedthecorrelation betweenIIEF-5scoreand age, mMRCscore, CAT score, HADS score andpercentage predicted FEV1. Despite being significant for age, mMRC, CATandHADSdepressionscore,itwas,nonetheless,aweak correlation(r<0.5).
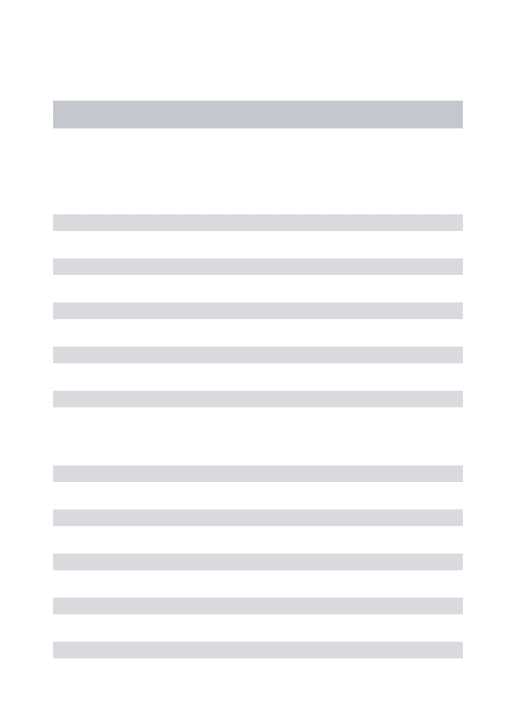
The presenceand thedegree of EDaccording toGOLD stagesarepresentedinFig.1.GOLDBandGOLDDpatients had more frequently mild-moderate or moderate ED. In addition to having, by definition, a higher mMRC and/or CATscore,GOLDBandGOLDDpatientshadahigherHADS depressionscore(5[3---7]vs.3[1---4]points,p=0.013)and ahigherprevalenceof arterialhypertension(61%vs.25%,
p=0.001) and dyslipidemia (49% vs. 21%, p=0.036) than GOLD A and GOLD C patients. All GOLD B patients had somedegree of ED.These patients hadarterial hyperten-sion more frequently (GOLD A=33%, GOLD B: 60%, GOLD C:11%andGOLDD:49%,p=0.031)aswellasdyslipidemia (GOLDA=27%,GOLDB:73%,GOLDC:11%andGOLDD:36%,
p=0.009). They also more frequently took beta-blockers (GOLDA=7%,GOLDB:33%,GOLDC:0%andGOLDD:11%,
p=0.048)andthiazides(GOLDA=13%,GOLDB:33%,GOLD C:0%andGOLDD:7%,p=0.041). 27% 22% 10% 60% 20% 44% 36% 7% 53% 11% 36% 7% 27% 22% 18% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
GOLD A GOLD B GOLD C GOLD D
No ED Mild ED Mild-moderate ED Moderate ED
Figure 1 Prevalence and degree of erectile dysfunction accordingtotheGOLDstages.
Regarding the impact of dyspnea in sexual activity of COPDpatients, theanswers tothe fourquestionsof RESP questionnaireareshowninFig.2.Thirty-ninepercentofthe patientsreportedhavingbreathingdifficultiesduringtheir sexual activity often or frequently and73% reported that thebreathingdifficultiesduringsexualactivitydidnotallow themtobeassexuallyactiveastheywouldlike. Neverthe-less, 24% of the patients reportedthat theynever talked aboutthistopicwiththeirpartnerand72%ofthepatients nevertalkedaboutitwiththeirphysician.
Discussion
Erectile dysfunction is an underestimated problem in COPD patients. The mechanism through which COPD can lead to ED is not yet fully understood. Possible mecha-nismsaresmoking,4systemicinflammationandendothelial
dysfunction,7chronichypoxia,16hormonalimbalance,7
mus-cularweakness,17decreasedexerciseintolerance17andfear
ofdyspnea.17
Our study showed an age-adjusted prevalence of ED amongCOPDpatientsof80%.Thisprevalenceishigherthan thereportedage-adjustedprevalenceof EDin Portuguese general population (48.1%)18 and is also higher than the
reported prevalence of ED among patients with diabetes (71%),arterial hypertension(67%)or evenamongpatients withboth diseases(77%).19 However,while theassociation
betweendiabetesorarterialhypertensionandEDiswidely known,theassociationbetweenCOPDandEDisstillpoorly recognized.
The firstdata suggesting thatsexual dysfunctioncould belinkedtoCOPDwaspublishedin1982.20Sincethen,few
7% 18% 18% 25% 2% 19% 27% 14% 19% 39% 28% 46% 72% 24% 27% 15%
I talk to my physician about the consequences that my breathing difficulties have on my sexual activity I talk to my partner about the consequences that my
breathing difficulties have on our sexual activity Because of my breathing difficulties I am not capable to be
as sexualy active as I would like to be During sexual activity I experience breathing dificulties
Often Frequently Sometimes Never
Figure2 RESPanswersofCOPDpatients.RESP:RespiratoryExperienceswithSexualityProfile.
reportedaprevalenceofEDamongCOPDbetween72%and 87%,whichisinlinewithourfindings.Thevariationsamong studiescanbeexplainedbydifferencesinthemethodology usedtoevaluateED.
We found no severe ED in our population. This can be explainedbythepossibleexclusionofthesepatientsinthe category of not having sexual relations in the previous 6 monthsor for refusal to participatein thisstudy because ofembarrassmentabouttheircondition.Nevertheless,the degreeofEDwasmoresevereinCOPDpatientsGOLDBand GOLDD,whichmaybeduetoworserespiratorysymptoms and to more frequent cardiovascular comorbidities, par-ticularlyarterial hypertension(p=0.001)anddyslipidemia (p=0.036).Interestingly,allGOLDBpatientshadED,which canbeexplained,atleastinpart,bythehigherprevalence ofcardiaccomorbiditiesandahigheruseofbeta-blockers andthiazides.Thisisinagreementwithpreviousstudiesthat reportedahigherprevalenceofcomorbiditiesandpersistent systemicinflammationinGOLDBpatients.21Comorbidities,
medicinesandsystemicinflammation canallcontributeto ED.
Inthepresentstudy,itwasnotpossibletoidentify predic-torsofEDthroughtheanalysisoflogisticregression,asthe numberofCOPD patientswithout EDwastoosmall. How-ever, the univariate analysis of groups showed that COPD patientswithED weresignificantly older(p=0.038), were more depressed (HADS depression score, p=0.032), had more dyspnea(mMRC score,p=0.028), a higher reported impact of COPD on their life (CAT score, p=0.015) and weremorefrequently receivinglong termoxygentherapy (p=0.048). Contrary to other studies,6---8 but in line with
Collinsetal.5wefound nosignificantassociationbetween
thepercentpredictedFEV1andED.
The effectof age onEDis well known,18 soit wasnot
surprisingthatCOPDpatientswithEDwereolder.However, agebyitselfmaynotjustifythehighprevalenceofEDamong COPDpatients.Forinstance,Collinsetal.showedthat,ata similarage,EDisworseinCOPDpatientsthaninthegeneral population.5
TheassociationbetweenEDanddepressionamongCOPD patientshasbeenpreviouslydescribed,butotherdepression
scaleswereused,suchastheGeriatricDepressionScaleand theBeck scale.5,6 Depressioncan impairerectile function
by reducing libido and by interfering with the parasym-patheticrelaxationof penilesmoothmusclenecessary for erection.4,22Moreover,therelationshipbetweendepression
andEDcouldbetwo-wayandmutuallyreinforcing.5
Ourstudyalsoconfirmed theimpactofa highermMRC scorein ED,described by Turanet al.23 The energyspent
duringanorgasmisequaltotheenergyrequiredfor contin-uousstairclimbingfor3---4minutes5so,manyCOPDpatients
mayavoidsexualactivitybecauseofthedyspneaassociated withthisactivity.
The median CAT score of COPD patients with ED was twice the median score of patients with no ED. Moreover,CATscorewasindependentlyassociatedtoa mild-moderate/moderateED.Asfarasweknow,thisisthefirst studytoevaluatetheassociationofCATscoreandED. Nev-ertheless,itseemslogicalthatEDmaybemorefrequentin patientsinwhomCOPDsymptomshadagreaterimpacton theirlife.
A curious finding was that COPD patients with ED were receiving long term oxygen therapy more fre-quentlythanpatientswithoutED.Itisknownthatchronic hypoxia decreases testosterone levels and impairs nitric oxide synthesis, which subsequently reduces the func-tionalintegrityof penile smoothmuscles.16,24 However,it
wasdemonstratedthat reversal ofED canbe achievedin patientsreceivinglong-termoxygentherapy24 butwe
can-notguaranteeoxygentherapy complianceofthe included patients,and thelack of compliance mayhave created a bias.
Patient medication can contribute toED, mainly drugs used to treat cardiac comorbidities.25 In our study, 61%
of the patients were not taking any medication associ-ated to ED and for the patients who took these drugs, therewasnostatistical differencebetween patients with EDandwithoutED.Nevertheless,allpatientstreatedwith beta-blockers, digoxin, verapamil and selective serotonin reuptakeinhibitor hadsome degree of ED. Therefore,we cannotguaranteetherewasnocontributionofthesedrugs toprevalenceofED.
Neither the CAT score nor the mMRC score evaluate dyspneaduringsexual activity.10,11 We found thatmost of
the COPD patients felt that dyspnea affects their sexual activity and 39% reported that it happened often or fre-quently. On the other hand, patients seldom discuss this sexual problem with their partner and only one in four patientshadtalkedabout thisissue withtheirphysicians. This probably happens because both patients and physi-cians feel uncomfortable discussing this topic. However, previousstudies suggestedthatan opendiscussionof sex-uality with patients with chronic diseases can improve theirqualityoflife.26,27Moreover,sexualproblemscannot
betreated until they arediagnosed. So an open commu-nication between physicians and patients is fundamental for a successful therapeutic strategy. Besides that, it is fundamental to train the doctors on how to take sex-ual history from COPD patients and manage their sexual problems.
The major strengths of our study were the analysis of multiple demographic and clinical characteristics that were prospectively collected and the use of a validated andinternationallyusedinstrument(IIEF-5)toestimatethe prevalenceandseverityofED.
However,ourstudyhassomelimitations.First,thegroup ofCOPDGOLDDpatientsisoverrepresented,sothe gener-alizationoftheconclusionsofthisstudyfortheothergroups shouldbemadewithcaution.Second, wedidnotmeasure thesexualhormones,andconsequentlywedidnotruleout hypogonadism which is a rare cause of ED.25 Finally, the
exclusionofpatientswhohadhadnosexualactivityinthe previous6monthsmayhaveunderestimatedtheED preva-lence,asmenwithoutsexualactivitymayhaveahigherED rate.18
Furtherlargerstudiesareneededtovalidateourfindings andtocontributetotheidentificationofmechanismsofED amongCOPDpatientsandconsequentlytothedevelopment ofpreventiveandcurativetreatments.
Conclusions
This study highlights the high prevalence of ED among patients with COPD and the impact of dyspnea in their sexual activity. Nevertheless, sexual problems are not a topic commonly discussed between patients and physicians.
PhysiciansshouldkeepinmindthatCOPDpatientsneeda comprehensiveevaluation,includingsexualfunction.COPD guidelinesshouldpaymoreattentiontotheimpactofthis diseaseinsexualactivityandincludeaconsensusdocument withsexual counselingfor thesepatients,asalready hap-penswithotherdiseases.28
Ethical
responsibilities
Protection of human and animal subjects.The authors declarethatnoexperimentswereperformedonhumansor animalsforthisstudy.
Confidentialityofdata.Theauthorsdeclarethattheyhave followedtheprotocolsoftheirworkcenteronthe publica-tionofpatientdata.
Righttoprivacyandinformedconsent.Theauthorshave obtained the written informedconsent of thepatients or subjectsmentionedinthearticle.Thecorrespondingauthor isinpossessionofthisdocument.
Funding
sources
Thisresearchdidnotreceiveanyspecificgrantfromfunding agenciesinthepublic,commercial,ornot-for-profitsectors.
Conflicts
of
interest
Nonedeclared.
Appendix
A.
Supplementary
material
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.
rppnen.2017.04.005.
References
1.Globalstrategyforthediagnosis,management,andprevention ofchronic obstructivepulmonarydisease:2017report. Avail-ablefromhttp://www.goldcopd.org/.
2.FabbriLM,RabeKF.FromCOPDtochronicsystemic inflamma-torysyndrome?Lancet.2007;370:797---9.
3.Areias V, Carreira S, Anciães M, Pinto P, Bárbara C. Co-morbiditiesinpatientswithgoldstage4 chronic obstructive pulmonarydisease.RevPortPneumol.2014;20:5---11.
4.NIHConsensusConference---Impotence.NIHConsensus Devel-opmentPanelonImpotence.JAMA.1993;270:83---90.
5.CollinsEG,HalabiS,LangstonM,SchnellT,TobinMJ,LaghiF. SexualdysfunctioninmenwithCOPD:impactonqualityoflife andsurvival.Lung.2012;190:545---56.
6.KahramanH,SenB,KoksalN,Kilinc¸M,ResimS.Erectile dysfunc-tionandsexhormonechangesinchronicobstructivepulmonary diseasepatients.MultidiscipRespirMed.2013;8:66.
7.KaradagF,OzcanH,KarulAB,CeylanE,CildagO.Correlatesof erectiledysfunctioninmoderate-to-severechronicobstructive pulmonarydiseasepatients.Respirology.2007;12:248---53.
8.Köseo˘gluN,Köseo˘gluH,CeylanE,CimrinHA,OzalevliS,Esen A.Erectiledysfunctionprevalenceandsexualfunctionstatus inpatientswithchronicobstructivepulmonarydisease.JUrol. 2005;174:249---52.
9.KapteinAA,vanKlinkRC,deKokF,ScharlooM,SnoeiL, Broad-bentE,etal.SexualityinpatientswithasthmaandCOPD.Respir Med.2008;102:198---204.
10.FletcherCM.Standardisedquestionnaireonrespiratory symp-toms: a statement prepared and approved by the MRC CommitteeontheAetiologyofChronicBronchitis(MRC breath-lessnessscore).BMJ.1960;2:1665.
11.JonesPW,HardingG,BerryP,WiklundI,ChenWH,KlineLeidy N.Developmentand firstvalidationof theCOPDAssessment Test.EurRespirJ.2009;34:648---54.
12.DowsonC,LaingR,BarracloughR,TownI,MulderR,NorrisK, et al.The use oftheHospital Anxietyand Depression Scale (HADS)inpatientswithchronicobstructivepulmonarydisease: apilotstudy.NZMedJ.2001;114:447---9.
13.Pechorroa P, Calvinho AM, Pereira NM, Vieira RX. Validac¸ão deumaversãoportuguesado ÍndiceInternacionaldeFunc¸ão Eréctil-5(IIEF-5).RevIntAndrol.2011;9:3---9.
14.VestboJ,HurdSS,AgustíAG,JonesPW,VogelmeierC,Anzueto A, et al. Global strategy for the diagnosis, management,
and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187:347---65.
15.Rodriguez-RoisinR,SorianoJB.Chronicobstructivepulmonary diseasewithlungcancerand/orcardiovasculardisease.Proc AmThoracSoc.2008;5:842---7.
16.Sáenzde Tejada I,Angulo J, Cellek S, González-Cadavid N, HeatonJ,PickardR, etal.Physiologyoferectilefunction.J SexMed.2004;1:254---65.
17.SchönhoferB.Sexualityinpatientswithrestrictedbreathing. MedKlin.2002;97:344---9.
18.TelesAG,CarreiraM,Alarcão V,Sociol D,AragüésJM,Lopes L,etal.Prevalence,severity,andriskfactorsforerectile dys-functionina representativesampleof3,548Portuguesemen aged 40 to 69 years attending primary healthcare centers: resultsofthePortugueseerectiledysfunctionstudy.JSexMed. 2008;5:1317---24.
19.GiulianoFA,LericheA,JaudinotEO,deGendreAS.Prevalence oferectiledysfunctionamong7689patientswithdiabetesor hypertension,orboth.Urology.2004;64:1196---201.
20.Fletcher EC, Martin RJ. Sexual dysfunction and erectile impotencein chronic obstructive pulmonary disease. Chest. 1982;81:413---21.
21.Agusti A, Edwards LD, Celli B, Macnee W, Calverley PM, MüllerovaH,etal.,ECLIPSEInvestigators.Characteristics, sta-bilityand outcomes of the 2011 GOLD COPD groups in the ECLIPSEcohort.EurRespirJ.2013;42:636---46.
22.AraujoAB,DuranteR, FeldmanHA,GoldsteinI,McKinlayJB. Therelationshipbetweendepressivesymptomsandmale erec-tiledysfunction:cross-sectionalresultsfromtheMassachusetts MaleAgingStudy.Psychosom.1998;60:458---65.
23.TuranO,UreI,TuranPA.ErectiledysfunctioninCOPDpatients. ChronRespirDis.2016;13:5---12.
24.Aasebø U, Gyltnes A, Bremnes RM, Aakvaag A, Slørdal L. Reversal of sexualimpotence in male patients with chronic obstructivepulmonarydiseaseandhypoxemiawithlong-term oxygentherapy.JSteroidBiochemMolBiol.1993;46:799---803.
25.CarsonCC.Urologicalandmedicalevaluationofmenwith erec-tiledysfunction.RevUrol.2002;4:S2---8.
26.PerezMA,SkinnerEC,MeyerowitzBE.Sexualityandintimacy followingradicalprostatectomy:patientandpartner perspec-tives.HealthPsychol.2002;21:288---93.
27.TanG,WaldmanK,BostickR.Psychosocialissuessexuality,and cancer.SexDisabil.2002;20:297---318.
28.Steinke EE, Jaarsma T, Barnason SA, Byrne M, Doherty S, DoughertyCM,etal.CouncilonCardiovascularandStroke Nurs-ingoftheAmericanHeartAssociationandtheESCCouncilon Cardiovascular Nursingand AlliedProfessions(CCNAP) Sexual counsellingforindividualswithcardiovasculardiseaseandtheir partners:aconsensusdocumentfromtheAmericanHeart Asso-ciationandtheESCCouncilonCardiovascularNursingandAllied Professions(CCNAP).EurHeartJ.2013;34:3217---35.