Narrative Therapy and the Nature Of “Innovative Moments” in the Construction of Change
32
0
0
Texto
(2) 2 Narrative therapy and the nature of “innovative moments” in the construction of change. Miguel M. Gonçalves, PhD, Marlene Matos, PhD & Anita Santos, PhD student* University of Minho, Portugal. * All correspondence to be directed to Miguel M. Gonçalves, Department of Psychology, University of Minho, 4710 Braga, Portugal Email: [email protected].
(3) 3 Narrative therapy and the nature of “innovative moments” in the construction of change. Abstract According to the narrative metaphor of psychotherapy, clients transform themselves by changing their life stories. According to the narrative therapy of White and Epston (1990), the construction of change occurs from the expansion of unique outcomes, or innovative moments as we prefer to call them, that is, the development of episodes outside the problem-saturated narrative. Unique outcomes operate as exceptions to the rule (i.e., to the problem-saturated story) that can be changed to a new rule (i.e., a new narrative). We suggest that some forms of unique outcomes can operate as shadow-voices (Gustafson, 1992) of the problem-saturated story, allowing a temporary release from the problem, but facilitating a return to it. In our view, there is a particular type of unique outcome —re-conceptualization— that facilitates sustained change. This kind of innovation facilitates the emergence of a meta-level perspective about the change process itself, and in turn, enables the active positioning of the person as an author of the new narrative.. Key-words: Narrative Therapy; Dialogical Processes; Unique Outcomes; Innovative Moments.
(4) As every therapist knows, independently of his or her theoretical orientation, clients bring stories of their lives to psychotherapy. According to the narrative metaphor of psychotherapy (see Hermans & Hermans- Jansen, 1995; Parry & Doan, 1994; Omer & Alon, 1997; White & Epston, 1990), clients transform themselves by changing the stories they tell about their lives. This metaphor of the person as a narrator has been inspiring a diversity of changes in the way psychotherapy is conceived and practiced. Documenting this growing interest, several handbooks (see Angus & McLeod, 2004; Hermans & Dimmaggio, 2004; Hoyt, 1998; Lieblich, McAdams & Josselson, 2004; Neimeyer & Raskin, 2000) were published in this field from a variety of clinical orientations (e.g., cognitive, constructivist, and family therapy). In this article, we will further explore this metaphor of the client as a story-teller, from the perspective of one of the most influential types of narrative therapy, the re-authoring model of White and Epston (1990). We will reflect upon the way change is pictured in this model and the concept of “unique outcome” as a window of opportunity for the construction of new narratives will be discussed. We also analyse the central ideas of the narrative therapy from a dialogical perspective (Hermans & Kempen, 1993), highlighting the dialogical processes behind the narrative content. We stress the heterogeneous nature of unique outcomes, suggesting that not all of them have the same potency (Giacomo & Weissmark, 1987) for the construction of new narratives or capacity to evoke sustained change.. Persons as narrators In psychology, for quite some time now, there has been an effort to understand human lives from a narrative perspective (Bruner, 1986; McAdams, 1993; Polkinghorne, 1988; Sarbin, 1986), in which the identity of the person is the result of his/her efforts to make meaning out of an almost infinite amount of episodes that life is made of. According to.
(5) 5 Sarbin’s (1986) seminal work and his “narratory principle… human beings think, perceive, imagine, and make moral choices according to narrative structures” (p. 8). Sarbin (1986) also proposed a rereading of the distinction proposed by James (1890) between the I and the Me. The I is the author, while the Me is the actor of the narrative. In this metaphor of the self, the person’s agency is revealed in the authorship process: it is the person who narrates the life that is lived (and performed as an actor). These narrative ideas have been the target of further development in two main fields: narrative therapy and dialogical self-theories. From one side, narrative therapy has been producing a rich diversity of therapeutic strategies and applications (e.g., Brown & AugustaScott, 2007; Freedman & Combs, 1996; Strong & Paré, 2004; White, 2004), after the seminal book from White and Epston (1990). On the other, dialogical perspectives have been exploring, in the therapeutic field, how their principles can be applied to the understanding of psychopathology and psychotherapy (e.g., Hermans & Dimaggio, 2004; Lysaker & Lysaker, 2006; Osatuke & Stiles, 2006). The connection between narrative and dialogical processes is strengthened by the idea that life narratives can be conceived as the outcome of dialogical processes of negotiation, tension, disagreement, alliance, and so on, between different voices (or perspectives) of the self. As Hermans suggested (Hermans & Kempen, 1993), individuals have the role of authors narrating their own stories. Therefore, narratives of life are multifaceted and multivocal (with different voices) (see Hermans, 1996). For Hermans (1996), a dialogical perspective of the distinction made by Sarbin between the author and the actor of the narrative means that the person’s self is a multitude of authors (or I-positions) narrating their story while enacting as actors these different positions. Each voice or I position can tell a story from its own perspective, and this transforms the self into a space of potentiality, in which the meaning is constructed and re-constructed as different positions gain or lose power..
(6) 6 In these dynamic struggles between voices, a dialogical disruption can occur when the diversity of voices collapses into the monologue of a single voice. The other voices of the self are silenced, making different constructions of the events very difficult or even impossible. Accordingly, in these narratives, the construction of reality is characterized by redundancy and loss of complexity. The experiential diversity is rejected or ignored and the narrative outcome reflects this reduction of voice variety. In the narrative therapy field this is akin to White’s (White & Epston, 1990; see also Freedman & Combs, 1996) problem-saturated stories, given that all other accounts and possibilities, besides the problematic one, are undermined. These narratives impose strong constraints to life, excluding all the experiential possibilities outside the problem-saturated story. Thus, for instance, if a person narrates him/herself as depressed, he/she is blind to all other possibilities (e.g., situations in which he or she feels, thinks or behaves differently). All the episodes from his/her life are a further proof that he/she is a depressed person and this way the problem occupies the whole identity. This author (I-as depressed person) constrains the person to live life according to this plot. However, as Bakhtin (1981/2000) suggested, this attempt to suppress the other (external or internalised) is never totally accomplished, given the dialogical nature of existence (see Fogel, 1993; Gonçalves & Guilfoyle, 2006; Salgado & Gonçalves, in press; Valsiner, 2004). So, in fact, instead of monologism, we should talk about attempts to suppress dialogism, given the impossibility of achieving a situation of total monologism. Similarly, White and Epston (1990) suggested that life is more than what is narrated, which means that in life there are episodes outside the domination of the problem-saturated story that need to gain voice in order for a new story to unfold. Thus, this impossibility to achieve a complete monological situation is akin, in the narrative therapy models, with the idea that there are always.
(7) 7 exceptions to the problem-saturated narrative, which these authors call “unique outcomes” (see White & Epston, 1990). This acknowledgment of the way voices emerge out of the dominant narrative plot and their development in psychotherapy into an emergent position has also been extensively studied by Stiles and his colleagues (Honos-Webb & Stiles, 1998; Stiles, Elliot, Llewelyn, Firth-Cozens, Margison, Shapiro, & Hardy, 1990; Stiles, Meshot, Anderson & Sloan, 1992; Stiles, 1999). They developed a model in which change is depicted through a process of assimilation of voices, drawing upon a narrative framework and a dialogical approach (Honos-Webb & Stiles, 1998), where narratives act like “meaning bridges – the semiotic glue that holds our experience together” (Osatuke, Glick, Gray, Reynolds, Humphreys, Salvi & Stiles, 2004, p. 194). Therefore, the assimilation model aims to describe change processes in psychotherapy through qualitative narrative analysis, entailing a dialogical view of self. In this article we will address two main questions: the first is how new narratives are constructed from problem-saturated narratives or, to put it in a dialogical frame, how monological or rigid narratives become dialogical in therapy. The second related question will address how unique outcomes facilitate the production of preferred identity narratives in psychotherapy. Our starting point is the narrative therapy tradition and our final aim is to contribute with a new coding system of therapeutic sessions that can allow empirical research into these processes: the Innovative Moments Coding System (Gonçalves, Matos & Santos, 2007).. Unique outcomes and change According to narrative therapy, the construction of new and preferred narratives of life is the result of the elaboration of unique outcomes. What defines a unique outcome (UO) is.
(8) 8 the emergence of something that was not predicted by a dominant story (White & Epson, 1990), and that is different from the way the client usually narrates himself/herself. Unique outcomes (UOs) are considered openings to new stories, and in this way, they are opportunities for therapeutic change to occur. The term, borrowed from Goffman (1961), is somewhat unfortunate, because as De Shazer (1991) points out, the idea of “unique” suggests that it happens only once. But, in fact, the proposal of White and Epston (1990) was that UOs are always happening but are trivialized and ignored by people when problemsaturated stories are very active. Also, the term “outcome” seems to emphasize the idea of an output instead of the processes behind change. However, the idea of unique outcome (or perhaps more poetically, “sparkling moments”) is used in the narrative therapy tradition as a way to emphasize the small but significant changes in the narrative text, and in this sense they are outcomes (or markers) in the narrative development of novelty. Freedman and Combs (1996), following White and Epson’s original work, suggested that in the construction of a new plot in psychotherapy, outside the problem-saturated story, the therapist should emphasize the conversation around UOs in the landscape of action and connect these with the ones in the landscape of consciousness (using a distinction made by Bruner, 1986). For Bruner (1986) a good story is made in this dual landscape, the landscape of action including the setting, the actors and the actions, while the landscape of consciousness refers to how actors feel, know and think. The UOs in the landscape of action are events involving actions or, as Freedman and Combs (2002) suggested, answers the question “what happened, in what sequence, involving which characters?” (p. 318). When therapist and client step back and talk about the meanings involved in these UOs sequences, they are constructing the story in the landscape of consciousness. Here, they can guide the conversation towards intentions, desires, values or beliefs. Freedman and Combs (1996) proposed a therapeutic structure in which the therapist promotes the consolidation of a new.
(9) 9 story through the questioning of UOs between elements in the landscape of action and elements in the landscape of consciousness, as well as making connections between past, present and future UOs. According to these authors, this process leads to the transformation of UOs into new stories and new meanings. Metaphorically, one can say that these three dimensions – time, action and consciousness – act like vectors in a narrative matrix, transforming isolated episodes into an alternative life-story that challenges the problematic story. Thus, in the conversation, therapists and clients need to develop these dimensions (landscape of action and landscape of consciousness along different time frames) for a new story to develop and become a viable alternative to the story saturated by the problem. A time frame is vital for the development of a coherent narrative. But a temporal dimension alone is not enough for a good story to unfold – one also needs actions and emotions, values and thoughts, as well as other elements from both landscapes of action and consciousness. These elements are central for a story to become meaningful and plausible for the person who is constructing and living it, as these constructions further evolve. What makes this elaboration of novelties so meaningful in narrative therapy is the assumption that what is not narrated becomes irrelevant and is easily forgotten or trivialized (see Freedman & Combs, 1996; White & Epston, 1990; Winslade & Monk, 1999). However, as every narrative therapist also knows, sometimes the effort to develop UOs into alternative stories is not enough for change to happen; otherwise the therapist’s task would be a simple one. So, one can say that change happens through the elaboration of unique outcomes (necessary condition), but this elaboration could be insufficient for change to take place. Dialogically, UOs are opportunities for new voices to gain power to tell their own stories, different from the voice of the dominant story. With other voices or perspectives claiming to be heard, the problematic narrative can not maintain its authoritarian status..
(10) 10. Heterogeneous nature of unique outcomes Despite the differences traced between landscape of action and landscape of consciousness, or the distinction between past, present and future UOs, there is, to our knowledge, no theoretical reflection about the influence of the diversity of UOs on change. What if there are different kinds of UOs that are related to different patterns of change? This is a question that we aim to explore in this section of the article. In a previous research study that we have completed with women who were victims of partner’s abuse (Matos, 2006; Matos & Gonçalves, 2004), we found that different kinds of UOs emerge in their stories. In this study we coded the therapeutic sessions for the emergence of unique outcomes, in good and poor outcome narrative therapy, trying to find what types of unique outcomes emerged. We identified five different types of UOs: action, reflection, protest, re-conceptualization and new experiences UOs. Given the problems referred before with this designation we will call them from now on innovative moments. This typology of innovative moments (IMs) will allow us to develop process research in psychotherapy that pays close attention to the emergence of these novelties and to the way these allow the development of a new life narrative. Here we define the various types of IMs and offer an illustration of each drawn from therapies addressing a variety of presenting problems.. (1) Action IMs involve specific actions against the problematic story. In the study referred above, all the actions initiated against or to prevent the abuse were integrated in this category. Clinical vignette.
(11) 11 T (therapist): Was it difficult for you to take this step (not accepting the rules of “fear” and going out)? C (client): Yes, it was a huge step. For the last several months I barely got out. Even coming to therapy was a major challenge. I felt really powerless going out. I have to prepare myself really well to be able to do this.. (2) Reflection IMs involve the emergence of new understandings or thoughts that are at not congruent with the dominant plot. The cognitive challenge of the problem, seeing new perspectives of the problem and defying cultural prescription that facilitates the development of the problematic narrative are examples of these IMs. Clinical vignette C: I’m starting to wonder about what my life will be like if I keep feeding my depression. T: It’s becoming clear that depression had a hidden agenda for your life? C: Yes, sure. T: What is it that depression wants from you? C: It wants to rule my whole life and in the end it wants to steal my life from me.. (3) Protest IMs are present when there is some sort of protest against the problem and its specifications and also against the persons who are somehow the problem’s supporters. It can be an action (as in action IM) or even a thought (as in reflection IM), but they are more than a mere action or thought, since they involve a way of repositioning the self and through this, a more proactive process can emerge (e.g., deciding something relevant about the problem that reduces its power over the client’s live). As an example, we can consider a woman that tells herself or others that she will no longer accept the responsibility for the.
(12) 12 abuse and says that her partner should always be responsible for his actions, independently of the supposed “provocations” that he saw in her. Clinical vignette C: I talked about it just to demonstrate what I’ve been doing until now, fighting for it… T: Fighting against the idea that you should do what your parents thought was good for you? C: I was trying to change myself all the time, to please them. But now I’m getting tired, I am realising that it doesn’t make any sense to make this effort. T: That effort keeps you in a position of changing yourself all the time, the way you feel and think… C: Yes, sure. And I’m really tired of that, I can’t stand it anymore. After all, parents are supposed to love their children and not judge them all the time.. (4) Re-conceptualization IMs involve a kind of meta-reflection level, meaning that the person not only understands what is different in her or him, but also is able to describe the processes involved in the transformation. These IMs involve three components: the self in the past (problematic narrative), the self in the present and the description of the processes that allowed the transformation from the past to the present. While reflection IM’s are related to novelty in terms of a thinking episode or moment (related to the past, present or future) that is outside the prescription of the dominant story, re-conceptualization IM’s are associated with the narration of a meta-reflection process involved in change. Thus, the client not only understands something new but he or she can also establish a distinction from a previous condition. Clinical vignette (victim of partner abuse).
(13) 13 C: I think I started enjoying myself again. I had a time… I think I’ve stopped in time. I’ve always been a person that liked myself. There was a time… maybe because of my attitude, because of all that was happening, I think there was a time that I was not respecting myself… despite the effort to show that I wasn’t feeling… so well with myself… I couldn’t feel that joy of living, that I recovered now… and now I keep thinking “you have to move on and get your life back”. T: This position of “you have to move on” has been decisive? C: That was important. I felt so weak at the beginning! I hated feeling like that…. Today I think “I’m not weak”. In fact, maybe I am very strong, because of all that happened to me, I can still see the good side of people and I don’t think I’m being naïve… Now, when I look at myself, I think “no, you can really make a difference, and you have value as a person”. For a while I couldn’t have this dialogue with myself, I couldn’t say “you can do it” nor even think “I am good at this or that”…. (5) New experience IMs refer to the anticipation or planning of new experiences, projects or activities. In these IMs the client may apply newly learned skills to new experiences, get back to former and abandoned projects and activities, or think about what she has learned with the problematic story that could make the next change in her life meaningful. These IMs are different from White and Epston’s (1990) future IMs, since new experience can happen in the present or in the future. Also, in our taxonomy, with the exception of the impossibility of new experiences occurring in the past, all the IMs can happen in the past, present or future. Clinical vignette T: You seem to have so many projects for the future now!.
(14) 14 C: Yes, you’re right. I want to do all the things that were impossible for me to do while I was dominated by fear. I want to work again and to have the time to enjoy my life with my children. I want to have friends again. The loss of all the friendships of the past is something that still hurts me really deeply. I want to have friends again, to have people to talk to, to share experiences and to feel the complicity of others in my life again.. This taxonomy of IMs is different from the classification of UOs in the landscape of action and the landscape of consciousness, previously provided by narrative therapy. These new categories do not neatly fit in this differentiation. Thus, while the action IM type clearly belongs to the landscape of action and reflection IMs to the landscape of consciousness, the other three categories identified are simultaneously rooted in both landscapes, since they involve some kind of actions, but also values, intentions and feelings. Thus, protest, reconceptualization and future experiences are, from a narrative perspective, more complex IMs1.. Innovative moments processes and patterns of change in psychotherapy We will now suggest some hypotheses, which are still conditional regarding the nature of therapeutic change, seen through the perspective of the patterns of IMs described above. We consider that the diversity of IMs is related to different processes involved in the psychotherapeutic process. It seems very unlikely that self change happens in conjunction with only one type of IM. In the re-authoring process, the development of a coherent, thick description of the experience of change emerges by the articulation of several different kinds of IM’s. Thus, for.
(15) 15 instance, a new narrative constructed only with action IMs would be a very impoverished (and monotonous) type of story. The same can be said of any other IM. Action and reflection are the most elementary IMs, since they involve actions and thoughts that can be very simple and subtle events. They could facilitate therapeutic transformation functioning as good “examples” that change is happening (or at least that a new movement is starting). The diversity and high frequency of these IMs can also work as ways of validating change – they could be signs for the self and for others that something different is in fact taking place. We think, however, that they, by themselves, can not allow the movement towards a new narrative of the self, as we will discuss below. Protest IM are very interesting since they imply the creation of a rhetorical space between the person and the problem, which allows the separation of the person from the problem. If one protests against the problem but sees the problem as something that is “the same as me” (internalized view of problems), the movement of protest can be felt as dangerous towards the self. Actually, this movement happens quite often but, far from leading to change, leads to a process of self-blaming and self-critique that is very typical of problem-saturated stories. When the person is able to protest against the problem, separating the problem from him/herself, this could be a very important moment in the change process. Thus, these IMs are very powerful, since they not only imply resistance but also a re-appreciation of the client’s position in relation to the problem. They are active ways of showing the self and others that people want something very different in their life. It seems, however, that some IMs of this kind can engage the person in protest without expanding the meaning of it (e.g., to disobey when one is incapable of tolerating the abuse, to obey later on when one somehow accepts the imposition)..
(16) 16 Perhaps the main problem with these three types of IM (action, reflection and protest) is the possibility that they become a mere opposition to the problem without creating new meanings outside the semiotic duality “problem” – “no problem”. If this happens, the problem is present even when it is absent, since the meaning of “no problem” requires the meaning of the “problem”, as we will discuss below. Re-conceptualization is a very complex type of IM, since it implies a kind of metaposition over change. These IMs involve a reflexive position toward the change process – the person is not only an actor of that process, but also its author (to use the distinction made by Sarbin, 1986). Without this meta-perspective the person could only be an actor who lacks access to the processes that are beneath the plot, and it is the access to these processes that allows him/her to be an author or his/her own life. We are not referring here to an “access” to something more fundamental or more real, since these processes beneath the plot are constructed as the new narrative develops, so in a sense they are invented, not discovered. We are simply stating that for these IMs to occur the person has to have some form of decentring from him/herself and be able to reflect about the creation of a new plot. This implies a metalevel from which the person can see the difference between the old plot and the (anticipated) new one and from this position favours the development of the new story. It is this decentring that allows the person to obtain more than a mere substitution of one narrative for another. If the client does not have access to the processes of transformation, we would only have the substitution of a monological narrative for another one (perhaps less harmful at that moment). These IM allow the movement of change to be continued in the future. Also, without this access, a collaborative position with the therapist would be very difficult, if not impossible, since client and therapist would be unable to step back and reflect about the change process and the client’s authorship..
(17) 17 Because of its nature, re-conceptualization can not be a mere negation of the problem, since it implies the creation of new semiotic dimensions outside the duality “problem” – “no problem”. While this meta-position is necessary, action, reflection and protest IMs can have the role of narrative markers that change is on its way, given that they represent new actions and new thoughts outside the problem-saturated narrative. The emerging re-conceptualization IMs enables the client to examine and somehow evaluate the flow of other IMs (action, protest and reflection). Then, meaningful connections between these moments of change are enacted and a new comprehension of the process of change is achieved. Re-conceptualization allows a narrative to have structure (e.g., coherence, organization and complexity), by the way it organizes the other emergent IMs. In our view, re-conceptualization is crucial for the change process. In the construction of a new narrative it acts like a gravitational field that attracts and gives meaning to action, reflection and protest IMs. These re-conceptualization IMs expand further through the elaboration of other IMs, which act as internal validations that change is taking place. We refer to internal validation, in the sense that they are intrinsic to the narrative itself. In other words, they are markers or “proofs” of plausibility, since they allow new episodes to emerge that are congruent with a new state. The importance of what we termed re-conceptualization also emerges in the research done by Angus and colleagues with the Narrative Process Model (Angus, Lewin, Bouffard, Rotondi-Trevisan, 2004). Their reflexive narrative sequences are very similar to our re-conceptualization and the main difference occurs because we only code in our sessions the innovative moments, while Angus and colleagues code all the sequences where the reflexive mode emerges. Nevertheless, they also conclude that “the reflexive decentering from and then reengagement with distressing life experiences … facilitates the articulation of new understandings about the self in relation to others (Angus, Lewin, Bouffard & Trevisan, 2004, p. 90)..
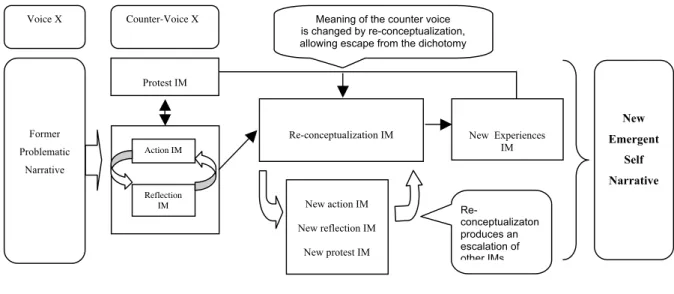
(18) 18 Re-conceptualization IMs are also akin to what Hermans (2003) has called a metaposition, a position from where the other I-positions can be seen and evaluated (see also Dimaggio, Salvatore, Azzara & Catania; Leiman & Stiles, 2001). In fact, in order to code this IM, as we referred before, two positions need to be present, the former self and the emergent self, which means that somehow a meta-position over the former two is needed. Finally, new experience IMs represent the expansion of the story into the future. As Crites (1986) suggested, a narrative without future is a narrative that has no time and allows no change. One needs to be able to imagine future selves in order for the movement into the future to take place (see Valsiner, in press). As Valsiner (2004) proposed “The person is constantly creating meaning ahead of the time when it might be needed – orienting oneself towards one or another side of anticipated experience, and thus preparing oneself for it.” (p. 14) In our view, for the story to be expanded into the future, a meta-position like the one that re-conceptualization allows is needed to imagine a future with other possibilities outside the problem-saturated narrative. We therefore suggest that change happens in a cyclical process, which could start with action, reflection and/or protest IMs, as signs for the person and significant others that something different is happening. The next movement in the cycle could be reconceptualization allowing the person to step back and see him/herself changing. Several movements from action, reflection and protest through re-conceptualization, and back again to action, reflection and protest, could be needed to validate change, before the person is able to project him/herself into the future with a secure narrative, which could certainly entail a new process of internal validation (see Figure 1).. Insert figure 1.
(19) 19. Each cycle could be amplified by the validation of the significant others, which could trigger new cycles of novelty exploration. Of course, other lines of development are plausible and we need to research the different possibilities of change. For instance, the client might start with a glimpse of a new narrative (re-conceptualization IM) and from there develop the more concrete action and reflection IMs. In our proposal, independently of the “starting point” (action, protest or reflection) a new gestalt of IM is necessary for a meaningful story to develop and also that this gestalt unfolds in a cyclical process, similar to the one described in Figure 1, although that path is not necessarily the only one possible. We also think that re-conceptualization is necessary to allow the person to achieve a position of authorship in the self narrative. We would like to emphasize that the new narrative is not something of a different nature from the diversity of IMs (despite what the representation in Figure 1 can suggest). The new narrative is a pattern that emerges from the variety of IMs that were explored in the therapeutic conversation, or in other words, the new narrative is an emergent propriety of the IMs.. Action, reflection and protest IMs: dialogical processes involved in monological narratives A dialogical perspective allows us to understand why isolated action, reflection and protest could be associated with conditions that represent a failure to change. It is our hypothesis that action, reflection and protest IMs have the potential to transform narratives when they interact with re-conceptualization IMs, as we have described above, but that they could have the effect of supporting the problem when re-conceptualization is absent. To make.
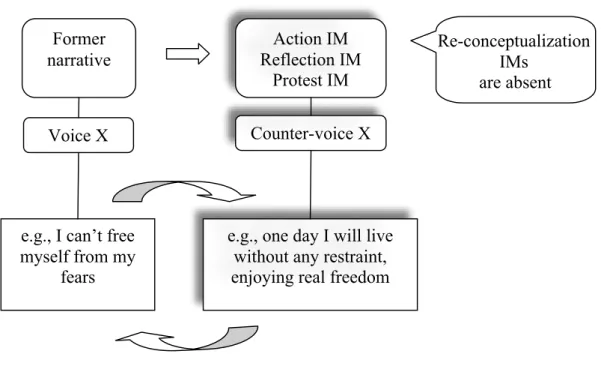
(20) 20 this clear we need to return to the concept of monological narrative (in the terms of narrative therapy, the problem-saturated story). It is our proposal that instead of being monological, problem-saturated narratives can involve, in fact, a situation of mutual in-feeding (see Valsiner, 2002), in which two voices are related to each other in a circular feedback loop. These high ambivalent relations promote the maintenance of a dynamic stability within self’s voices and can lead to an irresolvable dilemma. In these situations, the problematic narrative is dominated by a double voice, in which the second voice works as a shadow of the first. Gustaffson (1992, see also Omer, 1994) suggested a similar process responsible for the maintenance of these stories in which the only alternative to the main story is a shadow story: “these stories seem inescapable because what is viewed as the only alternative (the shadow story) turns out to be a loop that reintroduces the main line” (Omer, 1994, p. 47). That is the case, for example, of a person who is constrained by his or her phobia (i.e., a problem-saturated story) and dreams about an unrealistic freedom (i.e., a reflection IM). When this second voice of unrealistic dreams is given power and becomes dominant, if action follows from it (a counter-phobic reaction), the person is crushed by feelings of impotence and loss of protection, which, of course, makes the first voice (of the phobia) dominant and less aversive than before. Another example could be the depressed client who oscillates between the voice of depression (i.e., a problemsaturated story) and the voice of “true and definitive happiness” (another reflection IM). Each time the voice of depression gains power, the voice of happiness becomes active, bringing with it the implausibility of the move from depression to happiness which only makes the former voice stronger. When the voice of depression becomes more powerful the person dreams again of a state of happiness, and so on.. Insert Figure 2.
(21) 21. Dialogically, there is a voice and a counter-voice that freeze the system of meanings. So, in this example, and contrary to the intuition of White and Epston (1990) that saw unique outcomes as always beneficial, one specific IM actually feeds the problem.. It is the. oscillatory movement between this reflection IM and the problem that makes change impossible. Valsiner (2004) referred to this dance as a clear example of hidden-dialogism, in the sense that there seems to only be one position or voice, but in fact an oscillation between two clashing voices are happening (the Möbius strip could be used as a concrete representation of this process, see Josephs, Valsiner & Surgan, 1999). An interesting path for research would be to try to understand if the large majority of rigid or problem-saturated narratives are monological, without any change in meaning, or narratives where a situation of mutual in-feeding keeps the meaning system in a perpetual movement between the problem and its “solution”2. If we analyze the above examples of mutual in-feeding through our typology of IMs, one can see that the “shadow” voice involves reflection (dreams about a life without difficulties or dreams about absolute freedom) and action (counter-phobic reactions) IMs. It is also our suggestion that action and reflection IMs can operate in women who are victims of partner violence (the sample from which we have tracked the different IMs) as shadow voices of oppression. In these cases, action and reflection IMs can allow an oscillatory movement away from the problem, but the full consequences of this movement are not explored and the person returns to the prior position. It is perhaps because of these oscillatory movements that the temporary abandonment of the partner is so common in these situations. In fact, several studies have demonstrated that half of all the attempts to exit an abusive relationship later result in reunion with the aggressor (e.g., Anderson & Saunders, 2003; Lerner & Kennedy, 2000; Martin, Berenson, Griffing, Sage, Madry, Bingham &.
(22) 22 Primm, 2000). From our perspective, these attempts to exit the relationship could be classified as action IMs. In this case, the problem and these IMs’ interactions may be supporting the maintenance of the same situation over and over again, that is, to continue in the abusive relationship. We think that some forms of protest can also act as shadow voices of the problem, like some forms of defiance of the problem-saturated narrative. An example of this kind of protest would be a woman refusing to do something that the partner ordered, without other forms of elaboration. We are not suggesting that it is bad to refuse what a violent partner wants, but only that without further elaboration, this action is likely to fail the creation of significant change. If the woman elaborates this further, it can turn into different forms of protest (e.g., public repositioning towards culturally dominant values) or even to re-conceptualization, something like: “in the past I did what he asked me to do all the time, but now I discovered X” (being X, something about her life that allows her to keep exploring the novelties of a new way of being). In summary, without the creation of a meta-position (re-conceptualization IM) from which the person can expand and explore the meanings of action, reflection and protest IM, they can act as an invitation to return to the problem. In other words, these IMs can have the power to temporarily free the person from the problem, but without further elaboration (without re-conceptualization) they can make it difficult for the person to evolve onto a new narrative of the self. Thus, re-conceptualization may allow the person to avoid the eternal dichotomy between the two voices in opposition, by transforming the dichotomy itself.. Conclusion In this article, we suggested that the concept of unique outcome, or innovative moments as we prefer, does not always produce therapeutic change. We propose that some patterns of.
(23) 23 IMs allow the construction of new narratives of the self, while others operate as a form of mutual in-feeding, in which the self-narrative is trapped by the saturated-story and its opposite, without further development. From our perspective, re-conceptualization IMs are viewed as opportunities to develop new stories given the fact that the client positions him or herself in the position of the author of his or her story and is able to construct change from the meta-position. In fact, for reconceptualization IMs to occur we precisely need this narrative view over the way self is being transformed, as we suggested before. This taxonomy of IMs allowed us to develop a coding system to be used in process research in psychotherapy (Innovative Moments Coding System). This line of research is close to other research efforts, mainly by Stiles and collaborators (Honos-Webb & Stiles, 1998; Osatuke, Glick, Gray, Reynolds, Humphreys, 2004; Stiles, 1999) from a dialogical perspective, and by Angus and colleagues (Angus, Lewin, Bouffard & Rotondi-Trevisan, 2004; Hardtke & Angus, 2004), from a narrative perspective. Our own contribution aims to explore further the way change is constructed from the way narrative novelties emerge in psychotherapy, that is, how change is in fact constructed from the elaboration of unique outcomes, as proposed by the re-authoring model of White and Epston (1990). From this, we also wish to understand in the future how new voices emerge from the pattern of IMs that are visible in psychotherapy, exploring more the possible connections between dialogical theories of change and narrative therapy. We are currently developing new research projects based on the hypotheses explored in this paper. One path of research involves the microgenetic analysis (cf. Siegler & Crowley, 1991) of the development of each new narrative that appears in the therapeutic conversation and the way IMs develop in the process of narrating each story. The microgenetic analysis will allow a close look at the way IMs and new voices are related. Another path of research is.
(24) 24 the study of other forms of therapy (e.g., cognitive, experiential) to analyze if the same IMs and the same patterns that we propose here apply. We hope, in the near future, to be able to contribute empirical studies that allow us to test and expand the hypotheses explored in this paper.. Notes 1 Naturally, it is not possible to know if these types of IMs are valid for all types of problems, since there is no research demonstrating their general application. We do not know if other problems beyond abuse are re-authored through the elaboration of different types of IMs. This is an interesting research question that we intend to follow in the future. 2 Strategic therapists like Watzlawick and collaborators (e.g., Fisch, Weakland & Segal, 1982; Watzlawick, Weakland & Fish, 1974) analyzed these paradoxical processes with a communicational and cybernetic frame..
(25) 25 Acknowledgments: The authors are very grateful to Jaan Valsiner, Michael Guilfoyle, Carla Machado, three anonymous reviewers and Robert Neimeyer for the comments on the first draft of this article. The authors are also very grateful to Gena Rodrigues for helping with the language. This article was supported by the Portuguese Foundation for Science and Technology (FCT), by the Grant PTDC/PSI/72846/2006 (Narrative Processes in Psychotherapy).. References Anderson, D. & Saunders, D. (2003). Leaving an abusive partner: An empirical review of predictors, the process of leaving and psychological well-being. Trauma, Violence & Abuse, 2, 163-191. Angus, L. E & McLeod, J. (eds.) (2004). The handbook of narrative psychotherapy: Practice, theory and research. London: Sage. Angus, L. E., Lewin, J., Bouffard, B. & Rotondi-Trevisan, D. (2004). “What’s the story?” Working with narratives in experiential psychotherapy. In L. E. Angus & J. Mcleod (eds.), The handbook of narrative psychotherapy: Practice, theory and research (pp. 87-102). London: Sage Bakhtin, M. M. (2000). The dialogical imagination: Four essays. Austin: University of Texas Press. (Edited by M. Holquist, Originally published in English in 1981). Brown, C. & Augusta-Scott, T. (ed.) (2007). Narrative therapy: Making meaning, making lives. London: Sage. Bruner, J. (1986). Actual minds, possible worlds. Cambridge, MA: Harvard University Press..
(26) 26 Crites, F. (1986). Story time: Recollecting the past and projecting the future. In Sarbin, T. R. (Ed.), Narrative psychology: The storied nature of conduct (pp. 152-173). New York: Praeger. de Shazer, S. (1991). Putting difference at work. New York: Norton. Dimaggio, G., Salvatore, G., Azzara, C. & Catania, D. (2003). Rewriting self-narratives: The therapeutic process. Journal of Constructivist Psychology, 16, 155-181. Fisch, R., Weakland, J. H. & Segal, L. (1982). The tactics of change: Doing therapy briefly. San Francisco: Jossey-Bass. Fogel, A. (1993). Developing through relationships: Origins of communication, self and culture. Chicago University Press: Chicago. Freedman, J. & Combs, G. (1996). Narrative therapy: The social construction of preferred realities. New York: Norton. Freedman, J. & Combs, G. (2002). Narrative couple therapy. In A. S. Gurman & N. S. Jacobson (Eds.), Clinical handbook of couple Therapy (pp. 308-334)(3rd Ed.). New York: Guilford Press. Giacomo, D. & Weissmark, M. (1987). Toward a generative theory of the therapeutic field. Family Process, 26, 437-459. Goffman, E. (1961). Asylums: Essays on the social situation of the mental patient and other inmates. New York: Doubleday. Gonçalves, M. M. & Guilfoyle, M. (2006). Therapy as a monological activity: Beliefs from therapists and their clients. Journal of Constructivist Psychology, 19, 251-271. Gonçalves, M. M., Matos, M. & Santos, A. (2007). Innovative moments coding system. University of Minho: Available from the authors. Gustafson, J. P. (1992). Self-delight in a harsh world. New York: Norton..
(27) 27 Hardtke, K. K. & Angus, L. E. (2004). The narrative assessment interview: Assessing selfchange in psychotherapy. In L. E Angus J. & McLeod (Eds.). The handbook of narrative psychotherapy: Practice, theory and research (pp. 247-262). London: Sage. Hermans, H. J. M. & Dimaggio, G. (eds.) (2004). The dialogical self in psychotherapy. New York: Brunneer-Routledge. Hermans, H. J. M. & Kempen, H. J. G. (1993). The dialogical self: Meaning as movement. San Diego: Academic Press. Hermans, H. J. M. (1996). Voicing the self: From information processing to dialogical interchange. Psychological Bulletin, 119, 31-50. Hermans, H. J. M. (2003). The construction and reconstruction of a dialogical self. Journal of Constructivist Psychology, 16, 89-130. Hermans, H. J. M., & Hermans-Jansen, E. (1995). Self-narratives: The construction of meaning in psychotherapy. New York: Guilford. Honos-Webb, L. & Stiles, W. B. (1998). Reformulation of assimilation analysis in terms of voices. Psychotherapy, 35, 23-33. Hoyt, M. F. (Ed.) (1998). Handbook of constructive therapies. New York: Guilford. James, W. (1890). The principles of psychology (Vol. I). New York: Dover. Josephs, I. E., Valsiner, J., & Surgan, S. E. (1999). The process of meaning construction: Dissecting the flow of semiotic activity. In J. Brandtstädter & R. M. Lerner (eds.), Action & self-development: Theory and research through the life span. Thousand Oaks, Ca: Sage. Leiman, M. & Stiles, W. B. (2001). Dialogical sequence analysis and the zone of proximal development as conceptual enhancements to the assimilation model: The case of Jan revisited. Psychotherapy Research, 11, 311-330..
(28) 28 Lerner, C. F. & Kennedy, L. T. (2000). Stay-leave decision making in battered women: Trauma, coping and self-efficacy, Cognitive therapy and research, 2, 215-232. Lieblich, A., McAdams, D. P. & Josselson, R. (Eds.) (2004). Healing plots: The narrative basis of psychotherapy. Washington, DC: American Psychological Association. Lysaker, P. H & Lysaker J. T. (2006). A typology of narrative impoverishment I schizophrenia: implications for understanding the process of establishing and sustaining dialogue in individual psychotherapy. Counseling Psychology Quarterly, 18, 57-68. Martin, A., Berenson, K, Griffing, S., Sage, R., Madry, L., Bingham, L. & Primm, B. (2000). The process of leaving an abusive relationship: The role of risk assessments and decision-certainty. Journal of Family Violence, 2, 109-122. Matos, M. & Gonçalves, M. M. (2004). Narratives on marital violence: The construction of change through re-authoring. In R. Abrunhosa, R. Roesch, C. Machado, C. Soeiro & F. Winkel (Eds.), Assessment, intervention and legal issues with offenders and victims. Bruxelas: Politea. Matos, M. (2006). Violência nas relações de intimidade. Estudo sobre a mudança psicoterapêutica da mulher [Violence in intimate relationships: A research about the psychotherapeutic change in women]. University of Minho: Unpublished doctoral dissertation. McAdams, D. P. (1993). The stories we live by: Personal myths and the making of the self. New York: William Morrow. Neimeyer, R. A. & Raskin, J. D. (Eds.) (2000). Constructions of disorder: Meaning-making frameworks for psychotherapy (pp. 207-242). Washington: American Psychological Association. Omer, H. & Alon, N. (1997). Constructing therapeutic narratives. Northvale, N. J.: Jason Aronson..
(29) 29 Omer, H. (1994). Critical interventions in psychotherapy: From impasse to turning point. New York: Norton. Osatuke, K. & Stiles, W. B. (2006). Problematic internal voices in clients with borderline features: an elaboration of the assimilation model. Journal of Constructivist Psychology, 19, 287-319. Osatuke, K., Glick, M. J., Gray, M. A., Reynolds, D. J., Humpreys, C. L., Salvi, L. M. & Stiles, W. B. (2004). Assimilation and Narrative – Stories as meaning bridges. In L. E Angus J. & McLeod (Eds.). The handbook of narrative psychotherapy: Practice, theory and research (pp. 193-210). London: Sage. Parry, A. & Doan, R. D. (1994). Story re-visions. New York: Guilford Press. Polkinghorne, D. E. (1988). Narrative knowing and the human sciences. Albany: State University of New York Press. Salgado, J. & Gonçalves, M. (in press). The dialogical self: Social, personal and (un)conscious. In A. Rosa & J. Valsiner (Eds.), The Cambridge handbook of sociocultural psychology. Cambridge, UK: Cambridge University Press. Sarbin, T. R. (1986). The narrative and the root metaphor for psychology. In T. R. Sarbin (Ed.), Narrative psychology: The storied nature of human conduct (pp. 3-21). New York: Praeger. Siegler, R. S., & Crowley, K. (1991). The microgenetic method: A direct means for studying cognitive development. American Psychology, 46, 606-620. Stiles, W. B. (1999). Signs and voices in psychotherapy. Psychotherapy Research, 9, 1-21. Stiles, W. B., Elliot, R., Llewelyn, S. P., Firth-Cozens, J. A., Margison, F. R., Shapiro, D. A. & Hardy, G. (1990). Assimilation of problematic experiences by clients in psychotherapy. Psychotherapy, 27, 411-420..
(30) 30. Stiles, W. B., Meshot, C. M., Anderson, T. M. & Sloan, W., W., Jr., (1992). Assimilation of problematic experiences: The case of John Jones. Psychotherapy Research, 2, 81-101. Strong, T. & Paré, D. (ed.) (2004). Furthering talk: Advances in the discursive therapies. New York: Kluwer/Plenum. Valsiner, J. (2002). Forms of dialogical relations and semiotic autoregulation within the self. Theory & Psychology, 12, 2, 251-265. Valsiner, J. (2004). The promoter sign: Developmental transformation within the structure of Dialogical Self.. Paper presented at the Symposium (Hubert Hermans, Convener). Developmental aspects of the dialogical self. ISSBD, Gent, July 12, 2004. Valsiner, J. (in press). The notion of development: Basic epistemological and methodological implications for developmental science. In R. Lerner (Ed.), Handbook of child psychology (Vol. 1): Theoretical models of human development (6th Ed.). New York: Wiley. Watzlawick, P., Weakland, J. & Fisch, R. (1974). Change: Principles of problem formation and problem resolution. New York: Norton. White, M. & Epston, D. (1990). Narrative means to therapeutic ends. New York: Norton. White, M. (2004). Narrative practices and exotic lives: Resurrecting diversity in everyday life. Adelaide: Dulwich Centre Publications. Winslade, J. & Monk, G. (1999). Narrative counselling in schools. California: Corvin Press..
(31) 31 Figure 1. IMs and the creation of a new narrative. Voice X. Counter-Voice X. Meaning of the counter voice is changed by re-conceptualization, allowing escape from the dichotomy. Protest IM. New Former Problematic. Re-conceptualization IM Action IM. New Experiences IM. Narrative. Self Narrative. Reflection IM. New action IM New reflection IM New protest IM. Therapy’s evolution. Emergent. Reconceptualizaton produces an escalation of other IMs.
(32) 32 Figure 2. Mutual in-feeding (Valsiner, 2002) in action, reflection and protest IMs.. Former narrative. Action IM Reflection IM Protest IM. Voice X. Counter-voice Protest IM X. e.g., I can’t free myself from my fears. e.g., one day I will live without any restraint, enjoying real freedom. Re-conceptualization IMs are absent.
(33)
Imagem
Documentos relacionados