www.jped.com.br
REVIEW
ARTICLE
Gastroesophageal
reflux
disease:
exaggerations,
evidence
and
clinical
practice
夽
Cristina
Targa
Ferreira
a,b,c,∗,
Elisa
de
Carvalho
d,e,f,g,
Vera
Lucia
Sdepanian
c,h,
Mauro
Batista
de
Morais
c,h,i,
Mário
César
Vieira
c,j,k,e,
Luciana
Rodrigues
Silva
c,l,maPediatricGastroenterologyService,HospitaldaCrianc¸aSantoAntônio,ComplexoHospitalarSantaCasa,PortoAlegre,RS,Brazil bPediatricsDepartment,UniversidadeFederaldeCiênciasdaSaúdedePortoAlegre,PortoAlegre,RS,Brazil
cGastroenterologyDepartment,SociedadeBrasileiradePediatria,RiodeJaneiro,RJ,Brazil dPediatricsUnit,HospitaldeBasedoDistritoFederal,DF,Brazil
eHospitaldaCrianc¸adeBrasília,DF,Brazil fCentroUniversitáriodeBrasília,DF,Brazil
gPediatricGastroenterologyDepartment,SociedadeBrasileiradePediatria,Brasília,DF,Brazil
hPediatricsDepartment,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil iClínicadeEspecialidadesPediátricas,HospitalIsraelitaAlbertEinstein,SãoPaulo,SP,Brazil
jPediatricsDepartment,PontifíciaUniversidadeCatólicadoParaná,Curitiba,PR,Brazil kPediatricGastroenterologyService,HospitalPequenoPríncipe,Curitiba,PR,Brazil
lPediatricsGastroenterologyandHepatologyService,UniversidadeFederaldaBahia,Salvador,BA,Brazil mAcademiaBrasileiradePediatria,RiodeJaneiro,RJ,Brazil
Received31January2013;accepted23May2013 Availableonline30October2013
KEYWORDS
Gastroesophageal
refluxdisease;
Gastroesophageal reflux;
Abstract
Objective: therearemanyquestionsandlittleevidenceregardingthediagnosisandtreatment ofgastroesophagealrefluxdisease(GERD)inchildren.TheassociationbetweenGERDandcow’s milkproteinallergy(CMPA),overuseofabdominalultrasonographyforthediagnosisofGERD, andexcessivepharmacologicaltreatment,especiallyproton-pumpinhibitors(PPIs)aresome aspectsthatneedclarification.Thisreviewaimedtoestablishthecurrentscientificevidence forthediagnosisandtreatmentofGERDinchildren.
夽 Pleasecitethisarticleas:FerreiraCT, CarvalhoE,SdepanianVL, MoraisMB,VieiraMC,SilvaLR.Gastroesophagealrefluxdisease:
exaggerations,evidenceandclinicalpractice.JPediatr(RioJ).2014;90:105---18.
∗Correspondingauthor.
E-mail:[email protected](C.T.Ferreira).
Protonpump inhibitors;
Protonpump
inhibitors/therapeutic use;
Infant; Child
Datasource: asearchwasconductedintheMEDLINE,PubMed,LILACS,SciELO,andCochrane Libraryelectronicdatabases,usingthefollowingkeywords:gastroesophagealreflux; gastroe-sophagealrefluxdisease;proton-pumpinhibitors;andprokinetics;indifferentagegroupsof thepediatricagerange;uptoMayof2013.
Datasynthesis: abdominalultrasonographyshouldnotberecommendedtoinvestigate gastroe-sophagealreflux(GER).SimultaneoustreatmentofGERDandCMPAoftenresultsinunnecessary useofmedicationorelimination diet.There isinsufficient evidencefor theprescriptionof prokineticstoallpatientswith GER/GERD.Thereislittleevidencetosupportacid suppres-sioninthefirstyearoflife,totreatnonspecificsymptomssuggestiveofGERD.Conservative treatmenthasmanybenefitsandwithlowcostandnoside-effects.
Conclusions: therehavebeenfewrandomizedcontrolledtrialsthatassessedthemanagement ofGERDinchildrenandnoexaminationcanbeconsideredthegoldstandardforGERDdiagnosis. Forthesereasons,thereareexaggerationsinthediagnosisandtreatmentofthisdisease,which needtobecorrected.
©2013SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Doenc¸adorefluxo
gastroesofágico; Refluxo
gastroesofágico;
Inibidoresdebomba
deprótons;
Inibidoresdabomba
deprótons/uso
terapêutico; Lactente; Crianc¸a
Doenc¸adorefluxogastroesofágico:exageros,evidênciaseapráticaclínica
Resumo
Objetivo: hámuitasdúvidasepoucasevidênciasparaodiagnósticoetratamentodadoenc¸ado refluxogastroesofágico(DRGE)nacrianc¸a.Arelac¸ãoentreaDRGEeaalergiaàsproteínasdo leitedevaca(APLV),ousoexageradodaultrassonografiaabdominalparadiagnósticodaDRGE eoexcessodemedicamentos,especialmentedosinibidoresdebombadeprótons(IBP),são algunsaspectosquenecessitamesclarecimentos.Estarevisãotemcomoobjetivoestabelecer asevidênciascientíficasatuaisparaodiagnósticoetratamentodaDRGEempediatria.
Fontesdosdados: foram pesquisadas nas bases de dados eletrônicos do Medline, Pubmed, Lilacs,CochraneLibraryeScielo,nasdiferentesfaixasetáriasdapediatria,atémaiode2013,as seguintespalavras-chave:refluxogastroesofágico,doenc¸adorefluxogastroesofágico,inibidores dabombadeprótonseprocinéticos.
Síntesedosdados: aultrassonografiadeabdomenãodeveserrecomendadaparapesquisade refluxo gastroesofágico (RGE). O tratamentosimultâneo da DRGEe da APLV induz, muitas vezes,aousodesnecessáriodemedicac¸ãooudietadeexclusão.Nãoexistemevidências sufi-cientesparaprescric¸ãodeprocinéticosemtodososportadoresdeRGE/DRGE.Poucasevidências fornecemsuporteparaasupressãoácida,noprimeiroanodevida,paratratamentodesintomas inespecíficos,sugestivosdeDRGE.Otratamentoconservadortrazmuitosbenefíciosepoucos gastos,semefeitoscolaterais.
Conclusões: existempoucosestudoscontroladoserandomizadosqueavaliamaDRGEnacrianc¸a enenhum exame pode consideradopadrão-ouro para oseu diagnóstico. Poresses motivos, ocorremexagerosnodiagnósticoenotratamentodessadoenc¸a,equenecessitamsercorrigidos. ©2013SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Gastroesophageal reflux (GER) is a condition that most
commonly affects the esophagus, and is one of the most
frequentcomplaintsincentersof pediatricsandpediatric
gastroenterology.1---3
According to the latest guidelines from the North AmericanSociety for PediatricGastroenterology, Hepatol-ogy, and Nutrition (NASPGHAN)and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN), published in 2009, GER is the passage of the gastriccontentsintotheesophagus,withorwithout regur-gitation and/or vomiting.1 It is a normal, physiological process,whichoccursseveraltimesaday ininfants, chil-dren, adolescents, and adults, when it causes few or no symptoms.1 Conversely, it may represent a pathological
condition named gastroesophageal reflux disease (GERD), when it causes symptomsor complications that are asso-ciated with significant morbidity.1,3 These concepts were recently reinforced in April of 2013 by a new guide-line that emphasizes important concepts for the general pediatrician.3
months of life, which does not mean that they have the disease.2---4
The diagnosis of GERD is primarily clinical. In spite of thewiderangeofdiagnostictestsavailable,noneis consid-eredasthegoldstandard.1,3,4Ininfantswithmildsymptoms and nowarningsigns, drug therapy is unnecessary. These infants areconsidered‘‘happyspitters’’ andtherefore do not require any medicaltreatment. In infants and young children with GERD symptoms, non-pharmacological ther-apymaybetheoptionofchoice,duetolackofdrugswith provenefficacy.3Inolderchildrenandadolescents,inwhom symptoms areclearer andmore specific, pharmacological treatmentismoreoftenused.1
Theobjectiveofthisreviewwastoestablishtheexisting evidenceinthescientificliterature,inthelightofcurrent knowledge,onthediagnosisandtreatmentofGERD.
Diagnostic
tests:
clinical
application
ConsideringthatGERisaphysiologicalprocessthatoccurs
dailyinallchildren,infants,adolescentsandadults,itis
dif-ficult,insomesituations,todifferentiatethisprocessfrom
thepathologicalcondition,i.e.,GERD.1,5
Complementary examinations often do not clarify whetherGER is physiological or pathological,as, todate, there areno well established standards for the diagnosis ofGERD throughdefinitivediagnosticmethods. Significan-tly, the detection of reflux of gastric contents into the esophagusduringanexaminationdoesnotnecessarilymean thatthepatienthasGERD. Therefore,it iscrucialtotake intoaccounttheclinicalhistoryandphysicalexamination. According to the latest consensus, the clinical history is enoughtoconfirmthediagnosisinolderchildrenand adoles-cents,whohavemorespecificGERDsymptoms.Ininfants, symptoms arenonspecific (suchascrying, irritability, and refusal toeat)and areinsufficient todiagnose or predict responsetotherapy.1
Thereis agroupofpediatricpatientsthathasahigher risk of GERD, with greater severity, and chronic disease anditscomplications.Theyaretheneurologicallyimpaired, childrenwithoverweightandobesity,patientswithgenetic syndromes,thosewithoperatedesophageal atresia,those withchroniclungdisease,andprematureinfants.1,3
Complementaryexaminationsaimtodocumentthe pres-enceofGERoritscomplications;toestablishanassociation between GER and symptoms; to assess treatment effec-tiveness;andtoexcludeotherconditions.Asnodiagnostic method can answer all these questions, it is essential to understand the usefulness and limitations of each of the diagnostic tests for adequate patient evaluation, as dis-cussed below,to preventsubmitting patients to invasive, expensive,andinappropriatetests.1,5,6
Contrast
radiography
of
the
esophagus,
stomach
and
duodenum
Contrastradiography of the esophagus,stomach and
duo-denumisalow-cost,easy-to-performexamination,butitis
notappropriatefordiagnosisofGERD.1Itevaluatesonlythe
immediatepostprandialGER,anditisunabletoquantifythe refluxepisodes.2Therefore,itsroutineuseforthediagnosis
ofGERD1,4 is notjustified. Itsmainrole istheanatomical evaluationoftheupperdigestivetract,4andshouldbe indi-catedinselectedpatients.
Gastroesophagealscintigraphy
As with the radiological evaluation, gastroesophageal
scintigraphyassessesonlytheimmediatepostprandialGER.
ItsadvantagesincludetheidentificationofGERevenafter
a diet with neutral pH, gastric emptying evaluation, and
detectionofpulmonaryaspiration.4However,thedetection
ofslowgastric emptying does notconfirm GERD diagnosis andshouldbestudied only inpatients withclinical mani-festationsof gastricretention. Additionally, anormal test resultdoes notexclude thepossibility ofpulmonary aspi-ration.Thus, this test shouldnot be required for routine evaluationofGERDininfantsandchildren.1,4
Esophagogastricultrasound
Esophagogastric ultrasound (US) is not recommended for
routineclinicalevaluationofGERDininfantsandolder
chil-dren,accordingtotherecommendationsoftheconsensus.1
Whenthe resultsofthe esophagogastricUS arecompared withthoseofthe24-houresophagealpH-metry,the sensitiv-ityis95%,butthespecificityisonly11%forthediagnosisof GERD,withnocorrelationbetweenthefrequencyofreflux detectedbycolorDopplerUSandtherefluxindexdetected bypH-metry.7 Esophagogastric US playsan importantrole inthedifferentialdiagnosis ofhypertrophicpyloric steno-sis,asthelattercanbediagnosedthroughultrasonographic evaluation.1
Recently, Savinoetal8 published an article onthe use of US for the diagnosis of GERD in pediatrics. This study established that the purposes of this examination in the evaluationofGERDare:toevaluateother causesof symp-tomssuchasvomiting,apartfromGERD;andtomeasurethe abdominalesophageallength,theesophagealdiameterand wallthickness, andthe angle of His,providing functional andanatomicaldata.8However,theauthorsemphasizethe need to define diagnostic criteria, the standardization of tests,andreportedmeasures.8
Whatiscurrentlyobservedinclinicalpracticeisthatthe esophagogastric US provides information on the presence andnumberofGERepisodesduringtheexamination. This informationaddsnothingtotheinvestigation,becausethe refluxmaybephysiological, i.e.,onafull stomachandin thesupinepositionafterthechildhasbeenfed.Therefore, theUS,asithasbeenused,doesnotdifferentiateGERfrom GERDand isnot helpful tothepediatrician and gastroen-terologistdiagnosticapproach.Thus,atthemoment,there isnoplacefor USasaroutinediagnostictest for GERDin pediatricpatients.1,5
EsophagealpH-monitoring
ThemajoradvantagesofpH-monitoringare:toevaluatethe
patientundermorephysiologicalconditionsandforlonger
periods,toquantifyGER,andtocorrelateepisodesofreflux
withsignsandsymptoms.9Itsmainlimitationisthe
Thus,especiallyininfantswhoarepredominantlyor exclu-sivelyfedwitmilk,postprandialGERmaynotbedetected, duetotheneutralizationofacidrefluxbymilk.
AccordingtothepreviousguidelinesoftheNorth Ameri-canSocietyofPediatricGastroenterology,pH-metryshould beperformedonlyinsituationsthatwouldprovidechanges inpatientdiagnosis, treatment,or prognosis.9Inthis con-text,themainindicationsforGERassessmentbypH-metry remain:evaluationofextra-digestiveoratypicalsymptoms ofGERD; detection of occultGER; evaluation ofresponse toclinicaltreatmentinpatientswithBarrett’sesophagusor GERDthatisdifficulttocontrol;andpre-andpostoperative assessmentofthepatientwithGERD.4,9,11
When symptoms are typical or when GERD has been diagnosedbyother methodssuchasupperendoscopy, pH-monitoring is not indicated. pH-metry represents a valid quantitative measure of esophageal acid exposure, with well-establishedreferencevalues.1,3However,theseverity
ofacidrefluxis notconsistentlycorrelatedwithsymptom severityorwithdemonstrablecomplications.1
Esophagealintraluminalimpedance
Thisisanewmethodthatdetectstheretrogrademovement
offluids,solids,andairintheesophagus,toanylevelandat
anyamount,regardlessofpH,thatis,regardlessofchemical
orphysicalcharacteristics,asitmeasureschangesin
elec-tricalresistanceandis performedwithmultiple channels.
Therefore,thisnewtechniquemayhavegreatervaluethan
pH-metryto monitor thequantity andquality of refluxed
material.1,5,12
Currently, it is always used in association with pH monitoring(pH-multichannelintraluminalimpedance--- pH-MII).12,13pH-MIIissuperiortopHmonitoringalonetoassess thetemporalassociationbetweensymptomsandGER.1The twotechniquesusedtogetherprovideusefulmeasures,but theyareyettobewelldetermined.1
Esophagealmanometry
Esophagealmanometry assessesthemotilityofthe
esoph-agus and is indicated in those patients with symptoms
suggestiveofesophagealdysmotility,whosemainsymptoms
aredysphagiaandodynophagia.1Itmaybeusefulinpatients
who have not responded to acid suppression and have a negativeendoscopicfindingsinordertodetectmotor abnor-malitiessuchasachalasiathemaymimicGERD.1Itcanalso beusedtolocatethe loweresophagealsphincter(LES) in thepH-metry.
Uppergastrointestinalendoscopywithbiopsy
Uppergastrointestinalendoscopyallowsdirectvisual
exam-inationoftheesophagealmucosaandcollectionofsamples
for histophatological analysis.1,3 Thus, it is useful for the
diagnosisofesophagealcomplicationsofGERD(esophagitis, peptic stricture, or Barrett’s esophagus), which is impor-tantfortheimplementationofappropriatetherapyandfor patientprognosis.1---3,5 It alsohas akey rolein the differ-entialdiagnosiswithotherpeptic andnonpepticdiseases,
such aseosinophilicesophagitis (EoE), fungal esophagitis, duodenalulcer,gastritisbyH.pylori,eosinophilic gastroen-teropathy, malformations, andcancer, which can produce symptomssimilartoGERD.1
Currently,refluxesophagitisis definedasthe presence of mucosal lesions visible on endoscopy, in the esopha-gus, or immediatelyabove the esophagogastricjunction.1 Esophageal mucosaerythema andirregular Z line arenot sensitive enough todiagnose refluxesophagitis. Similarly, the histological findings of mild eosinophilia, elongated papillae, basallayer hyperplasia,and dilationof intercel-lular spaces (spongiosis) are not adequate to make the diagnosis of refluxesophagitis.1They onlyconstitute non-specific, reactive changes, which may be found in other typesofesophagitisor eveninnormalsubjects.1 Although the histological assessment of refluxesophagitis is notas important,endoscopicbiopsiesareessentialinthisgroupof patientsfor thedifferentialdiagnosiswithotherdiseases, suchasEoE.
Itshouldalsobeconsideredthattheabsenceof esophagi-tisonendoscopydoesnotexcludeGERD,assomepatients haveendoscopy-negativerefluxdisease(non-erosivereflux disease[NERD]).
Empiricaltherapeutictestwithacidsuppression
Older children and adolescents with typical symptoms of
GERD,withoutwarningsigns,canbesubmittedtoan
empir-icaltherapeutictrialwithprotonpumpinhibitors(PPIs)for
four weeks, which can be extended to 12 weeksif there
isclinical improvement.1Typicalsymptomsareheartburn,
burning epigastric pain, chronic cough, especially related tofood,nauseaandregurgitation,chestpain,and dyspep-sia.However,symptomaticimprovementdoesnotprovethe presenceofGERD,assymptomsmayrespondtoplaceboor improve spontaneously. The timeof response is also con-troversialandvaries frompatienttopatient.Thewarning signsthatshouldbeinvestigatedarebleeding,weightloss, chronicanemia,asthenia,andprostration.Thereisno evi-dencetoindicateatherapeutictestinyoungerchildren,in whomsymptomsarelessspecific.1
GERD
and
cow’s
milk
protein
allergy
GERD and cow’s milk protein allergy (CMPA) are common
conditionsinpediatricpatients,especiallyinfants.14 There
iscurrentlyalargenumberofinfantswhoaretreated con-comitantly for GERD and CMPA. There is a subgroup of patients,ingeneral,youngerthan6months,whohaveCMPA thatmanifest asvomitingandregurgitation, indistinguish-ablefromGERD.Intheseinfants,theeliminationofcow’s milkfromtheinfant’sorthemother’sdietmayimprove vom-iting substantially,and symptoms may recurwhen milk is reintroducedinthediet.1
conditionsoftencausesexaggerations,frequentlyresulting in unnecessary pharmacological treatment or elimination diet.
Several studies support the hypothesis that there is a causal relationship between the two conditions, suggest-ing that there is a subgroup of infants in whom GERD is attributable to CMPA.14---19 The debate is the logical consequence of the fact that the two conditions require diagnosticexaminations.14Therefore,theconsensusofthe NASPGHAN/ESPGHAN1onGERDadvisesatherapeutictrialof twotofourweekswithanextensivelyhydrolyzedoramino acid formula, and for infants who are breastfed, with a maternal strictCMP elimination diet.1 In thesecases, the possibilityofGERDcausedbyCMPAwouldbeexcluded with-outusingunnecessary medications.Conversely,therecent consensuson the diagnosis and treatment of food allergy of ESPGHAN states thereare insufficient data to support theconceptthat gastroesophagealrefluxmaybetheonly manifestationofCMPAinbreast-fedinfants.20 This consen-susstatement,however,citesvomitingandregurgitationas possible symptoms of CMPA, and recommends elimination dietforthemother.20
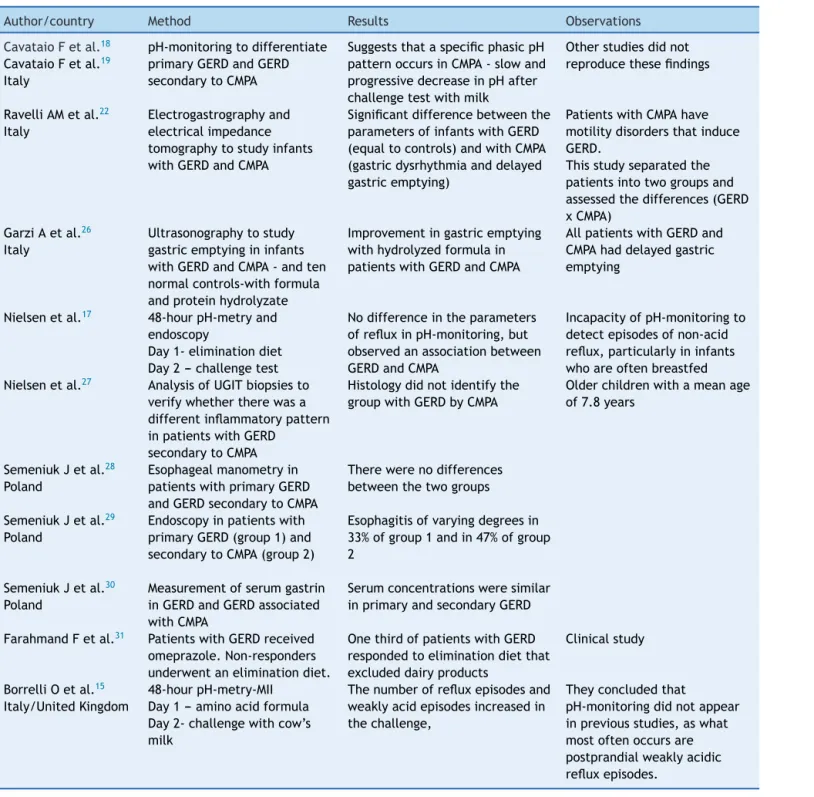
Although it hasbeen estimated that the prevalenceof GERD attributable to CMPA is as high as 56%, this asso-ciation is not scientifically proven.14---17 There are several uncontrolled studies, with very different methodologies, aimedatclarifyingtherelationshipbetweenGERDandCMPA (Table 1).18,19 However, to date, this association remains unclearandtherearestillmanypointstobeclarified.
Recently, Borrelli etal.15 evaluateda group of infants withCMPAand suspectedGERD(17 children,meanageof 14 months), through 48-hour pH-impedance testing with multiplechannels. Inthefirst24hours,theyweretreated withCMPeliminationdiet(aminoacidformula,whichthey had already been receiving to treat CMPA); in the subse-quent 24hours, a challenge test with cow’s milk (cow’s milkformula,withosmolarity andcomponentsother than theprotein,similartoaminoacidformula)wasperformed. TheseauthorsreportedthatininfantswithCMPAand sus-pectedGERD,exposuretocow’smilkincreasedthenumber ofweaklyacidicrefluxepisodes,identifyingasubgroupof patients with allergen-induced GER.15 Thus, they recom-mend pH-impedancetesting asa diagnostictest for some casesofinfantswithGERDandCMPA.15 Thesedataarenot fullycorroboratedandshouldbeinterpretedwithcaution.
The mechanisms by which CMPA induces GER are still poorly understood.15 Data from animal models show neu-ral abnormalities in gastrointestinal motility secondary to immediatehypersensitivityreactions,inducingdelayed gas-tricemptyingandchangesingastricacidsecretion21Other studieshaveshown changesingastricmyoelectricactivity inatopicpatients,whenexposedtocow’s milk.22,23These changes would occur by activation and degranulation of mastcellsandeosinophils,causingthereleaseofcytokines andactivationofreceptorsinnervefibersofthedigestive tractmucosa,whichwouldresultincontractileand motil-ity abnormalities, triggering reflux episodes secondary to exposuretotheantigen.14,15,21---23
Emerenziani and Sifrim,24 evaluating gastric emptying andpH-impedancetestingofsomepatients,observedthat the slower the gastric emptying, the higher the pH and proximalextensionofrefluxepisodes.Itiswellestablished
thatnon-acidicrefluxepisodesoccurduringfeedingandin thefirsthoursof the postprandialperiods.15,23 Therefore, Borrelliet al.15 speculate thatneuroimmuneinteractions, induced during the challenge test with cow’s milk, sup-pressgastric acid productionand alter themotor activity ofthestomach,whichslowsgastricemptyingandincreases transient relaxation of the lower esophageal sphincter, resultinginanincreaseinthenumberofweaklyacidicreflux episodes.ThiscouldexplainhowCMPAcausesGERD,butit isyettobeproven.
Nevertheless,asthesetestsarestillexpensiveandnot widely available, in addition to being invasive for small infants, probablythe most practical test in routine prac-ticewhenthereis doubtisatrial ofCMP-eliminationdiet fortwotofourweeksininfantswithGERDinwhomCMPAis suspected.
The variety and availability of different formulas is another important issue in this discussion. The addition ofnucleotides,longchainpolyunsaturatedfattyacids (LC-PUFAS), pre- and probiotics may improve immunity and decreasetheincidenceofgastrointestinaldisorders includ-ingfoodallergiesandmotility disorderssuchasGERDand constipation.Ifthetheoreticalbenefitproclaimedby phar-maceutical companies is real, it should result in clinical benefit,reducingtheprevalenceofthesefrequent gastroin-testinalcomplaints;however,furtherstudiesarenecessary tosubstantiate theseeffects,14 andtheESPGHANandthe AmericanAcademyofPediatricsconsensusstatethatthere isnotenough scientific supporttoroutinelyemploythese additivesininfantformulas.25
Thestudiesthatdiscussthepossibleassociationbetween GERDandCMPAareshowninTable1.15,17---19,22,26---31
GERD
treatment
The main objectives of therapy are topromote adequate
growthandweightgain,symptomrelief,healingoftissue
injuries,andtopreventrecurrenceandcomplications
asso-ciatedwithGERD.
Firstly,itis importanttodifferentiate between
physio-logicalGER andGERD.In infants,GERD resolution occurs,
in most cases, as the child grows and develops.
Sponta-neous resolution is common and the course is generally
benign,withlow incidenceofcomplications. Thus,inthis
group,clinicaltreatmentwithanti-GERDmeasures,changes
in diet and, less often, pharmacotherapy result in
clini-calresolution.Asmallpercentageofyounginfantsdevelop
more severe pulmonary manifestationsdue toaspiration,
cyanosis, and swallowing disorders, especially premature
infantsandthosewithcerebral palsy.Differently, inolder
children,aswellasinadults,GERDhasoftenachronicand
relapsingcourse,andmayleadtocomplications.Theremay
alsobespontaneousresolutioninthisgroup.3,6
Table1 StudiesoftheassociationbetweenGERDandCMPA.
Author/country Method Results Observations
CavataioFetal.18
CavataioFetal.19
Italy
pH-monitoringtodifferentiate primaryGERDandGERD secondarytoCMPA
SuggeststhataspecificphasicpH patternoccursinCMPA-slowand progressivedecreaseinpHafter challengetestwithmilk
Otherstudiesdidnot reproducethesefindings
RavelliAMetal.22
Italy
Electrogastrographyand electricalimpedance tomographytostudyinfants withGERDandCMPA
Significantdifferencebetweenthe parametersofinfantswithGERD (equaltocontrols)andwithCMPA (gastricdysrhythmiaanddelayed gastricemptying)
PatientswithCMPAhave motilitydisordersthatinduce GERD.
Thisstudyseparatedthe patientsintotwogroupsand assessedthedifferences(GERD xCMPA)
GarziAetal.26
Italy
Ultrasonographytostudy gastricemptyingininfants withGERDandCMPA-andten normalcontrols-withformula andproteinhydrolyzate
Improvementingastricemptying withhydrolyzedformulain patientswithGERDandCMPA
AllpatientswithGERDand CMPAhaddelayedgastric emptying
Nielsenetal.17 48-hourpH-metryand
endoscopy
Day1-eliminationdiet Day2---challengetest
Nodifferenceintheparameters ofrefluxinpH-monitoring,but observedanassociationbetween GERDandCMPA
IncapacityofpH-monitoringto detectepisodesofnon-acid reflux,particularlyininfants whoareoftenbreastfed Nielsenetal.27 AnalysisofUGITbiopsiesto
verifywhethertherewasa differentinflammatorypattern inpatientswithGERD
secondarytoCMPA
Histologydidnotidentifythe groupwithGERDbyCMPA
Olderchildrenwithameanage of7.8years
SemeniukJetal.28
Poland
Esophagealmanometryin patientswithprimaryGERD andGERDsecondarytoCMPA
Therewerenodifferences betweenthetwogroups
SemeniukJetal.29
Poland
Endoscopyinpatientswith primaryGERD(group1)and secondarytoCMPA(group2)
Esophagitisofvaryingdegreesin 33%ofgroup1andin47%ofgroup 2
SemeniukJetal.30
Poland
Measurementofserumgastrin inGERDandGERDassociated withCMPA
Serumconcentrationsweresimilar inprimaryandsecondaryGERD
FarahmandFetal.31 PatientswithGERDreceived
omeprazole.Non-responders underwentaneliminationdiet.
OnethirdofpatientswithGERD respondedtoeliminationdietthat excludeddairyproducts
Clinicalstudy
BorrelliOetal.15
Italy/UnitedKingdom
48-hourpH-metry-MII Day1---aminoacidformula Day2-challengewithcow’s milk
Thenumberofrefluxepisodesand weaklyacidepisodesincreasedin thechallenge,
Theyconcludedthat
pH-monitoringdidnotappear inpreviousstudies,aswhat mostoftenoccursare postprandialweaklyacidic refluxepisodes.
CMPA,cow’smilkproteinallergy;GERD,gastroesophagealrefluxdisease;UGIT,uppergastrointestinaltract.
tocloselyfollowtheevolutionofthepatient.Prolongedor
repeatedcoursesofdrugtreatmentshouldnotbeprescribed
priortodiagnosticconfirmation.1
Conservativetreatment(non-pharmacological)
Recommendationsofferedtotheparentsandsupporttothe
familyare essential measures, especially in small infants
who vomit and present adequate growth.1 The lifestyle
changes recommended toall pediatric patients with GER andGERD,regardlessofseverity,include:notwearingtight
clothes;diaperchangesbeforebreastfeeding,toavoidusing drugsthatexacerbateGER;slowinfusionsinchildrenwith nasogastric tubes; and to avoid smoking (active or pas-sive),astobaccoexposureinducesLESrelaxation,increases rates of asthma, pneumonia, apnea, and sudden infant deathsyndrome;inadditiontoanti-GERdietaryandposition guidelines,4discussedindetailbelow.
Dieteticrecommendations
Adolescents should avoid high-volume and high-calorie
gastric emptying and reduce LES pressure.1,4 Some foods suchaschocolate,softdrinks,tea,andcoffeearenot advis-able.Asimpleanduncontroversialmeasureistorefrainfrom eatingafewhoursbeforebedtime,unlessthereissignificant malnutrition.There is noevidencetosupportthe routine elimination ofcertainfoods for thetreatment of GERDin olderchildren,1suchasacidicfruit.Therecommendationof smaller,morefrequentmealsisbasedonthelikely correla-tionbetweengastricvolumeandtherefluxindex.However, thishabitincreasesthefrequencyofpostprandialperiods, whichareassociatedwithgreaternumberofweaklyacidic ornon-acidGERepisodes.15
pH-monitoringandgastroesophagealscintigraphystudies havedemonstratedthatthickened feedsarenoteffective anti-GER measures, although they may decrease the vol-umeandfrequencyofregurgitationandvomiting.1Whileit reducescryingandincreasescaloricintake,excessive calo-rieintakeisapotentialproblemofathickeneddiet.1,3Its therapeuticeffecthasnotbeendeterminedinpatientswith GER that donot present vomiting or regurgitation.3 Anti-regurgitationformulasmayreducevisibleregurgitation,but donot resultin measurable decrease in thefrequency of refluxepisodes.1Ameta-analysishasdemonstratedthat,in healthy children,thickened formulas areonly moderately effectiveinthetreatmentofphysiologicalGER.32
Positionguidelines
Thepronepositionisproventobethemosteffective
anti-GERposition.3 However,itsassociation withsudden death
ininfants,aswellasthatofthelateraldecubitusposition,
has generated much controversy regarding the best
anti-GERposition.1,3 Currently,itis recommendedthat normal
infantsorpatientswithGERDshouldsleepinthesupine posi-tion,sincetheriskofsuddendeathismoreimportantthan the benefitbrought by the anti-GERposition.1,3 Elevating theheadboardhasbeenrecommended,althoughnotproven beneficialincontrolledstudies.1---4Thesittingorsemi-sitting positionsforinfantsbelowoneyearwerealsonotshownto beaneffectiveanti-GERposition,duetothemuscletonus ofinfants.33
For adolescents and adults, it is likely that the best positionistheleftlateraldecubitusposition,withthe head-boardelevated.1,3
Pharmacologicaltreatment
In general, physiological GER should not be treated with
medication,exceptforcaseswherethepresenceofGERDis
evident.Pharmacologicaltreatmentisdirectedprimarilyto
acid suppression. PPIs and H2 receptor antagonists
effec-tively increase gastric pH and prevent acid reflux,which
is harmfulto theesophageal mucosa.However,currently,
weaklyornon-acidrefluxareknowntobefrequentandto
causesymptoms.14,15
ThereisnoalgorithmforthetreatmentofGERDin chil-drenthatdoesnotprovokesdiscussionandcontroversybut therecommendeddrugsare:
• Contact antacids, recommended only as symptomatic
drugs for sporadic symptoms or to decrease nocturnal acidity.1
• Prokinetics,whichhelptocontrolsymptoms,mainly
vom-itingandregurgitation.
• Medications that reduce acid secretion (histamine H2
-receptor antagonists or PPIs), when symptoms such as retrosternal pain and heartburn, and/or complications, suchasesophagitis,areassociatedwiththepresenceof theacidintheesophagusorinotherorgans,suchas res-piratorytract.
Prokineticagents
Theuseofprokineticsisbasedonthefactthattheyincrease
LES tonus and improve esophageal clearance and gastric
emptying.However,noneof thesemedicationswasshown
to be effective in decreasing the frequency of transient
relaxation of theLES, the main physiopathological
mech-anismof GER. They arenot effective in inducing healing
of esophageal lesionsand donot have a proven anti-GER
effect,ratherananti-regurgitationeffect.Thus,the
proki-netic medications are often used in children who have a
predominance of symptoms of motility abnormalities and
whohavemoreregurgitationthanpain.
Currently, there is insufficient evidence for the
rou-tine use of prokinetics.1 Furthermore, the potential side
effectsofthesedrugsaremoreimportantthanthebenefits achievedbytheiruseinthetreatmentofGERD.1
Indailypractice,theuseofprokineticsisalways associ-atedwithantacidsinthetreatmentofGERD.Basedonthese concepts,eachmedicationhasitspreciseindications,and thereisnoneedandnoplausibleexplanationtojustifythe indiscriminateuseoftwomedications(prokineticsandacid secretioninhibitors)atthebeginningoftreatment.
Metoclopramide
Metoclopramideimprovesgastricemptyingandesophageal
peristalsis,andincreasesthe pressurein theLES, butthe
narrowmarginbetweentherapeuticandadverseeffectson
the CNS hinders its use in children with GERD. A
meta-analysisofsevencontrolledstudiesshowedthat,inchildren
aged1monthto2years,metoclopramidereducesthedaily
symptoms of GER and GER index in pH-monitoring, but
withsignificant adverse effects.33 The adverse effects of
metoclopramide in infants and children include lethargy, irritability, gynecomastia, galactorrhea, and extrapyrami-dalreactions, which havebeen reportedin 11%to34% of patients.3,33
Bromopride
Therearenocontrolledtrialstosupportitsuseorproveits
benefits.Asbromopridehasneurologicalsideeffects,such
asextrapyramidalchanges,itmustnotbeindicatedforthe
treatmentofGERD.34Bromoprideisnotmentionedinanyof
thepediatricguidelines.1,3
Domperidone
Domperidoneisaprokineticagentthatincreasesthe
pediatricsgiventhelackofstudiesthathavedemonstrated
itseffectiveness.Arecentsystematicreviewofstudieswith
domperidoneidentifiedonlyfourcontrolledstudiesin
pedi-atricpatients,noneofwhichshowedanyrobustevidenceof
efficacyinpediatricGERD.1,3,35
Domperidonealsocausesoccasionalextrapyramidalside effects.1,35 One of the major side effects is increased irritability and colic in infants, which often worsens the clinical picture or further confuses the pediatrician. The simple action of stopping the use of domperi-done in infants who are experiencing side effects of the medication can greatly improve patient symp-toms. More recently, the occurrence of cardiovascular events associated with the use of domperidone, includ-ingQT prolongationand ventriculararrhythmia, has been demonstrated.36,37
Acid
secretion
inhibitors
HistamineH2-receptorantagonists
Histamine H2-receptor antagonists are drugs that reduce
gastric acidity by inhibiting the histamine H2 receptors
on gastric parietal cells. A dose of 5mg/kg of ranitidine
increasesthegastric pHfor 9to10hoursininfants.1
Gas-tric pH begins to increase within 30minutes,allowing its use for fast symptom relief.1 Doses of 5mg/kg of raniti-dine,every12hours;orof3mg/kg,threetimesaday,have beenrecommendedinchildren.2,38 AccordingtoOrenstein et al.,2 the therapeutic failure of these medications can beattributedtothesmalldosescommonlyusedinclinical practice.
Studies have demontrated that H2 antagonists
(cime-tidine, ranitidine, famotidine) are more effective than placeboinrelievingGERDsymptomsandhealingesophageal mucosal injury.1 The effectiveness of H
2 blockers in
healing erosive lesions is much higher in mild to moderate cases. PPIs are more effective in more severe injuries, even when compared to high doses of ranitidine.1
Regarding side effects of ranitidine, some infants may haveheadaches, drowsiness,head bangingandother side effects which, if interpreted as persistent symptoms of GERD,couldresultinaninappropriateincreaseindosage.1 Furthermore,tachyphylaxisordecreaseintheresponseisa problemforitschronicuse.
Asranitidinehasaliquidformula,itshouldbeusedwhen necessaryininfants.Ifnosatisfactoryresponseisattained, itwouldbemoreappropriatetoevaluateotherdiagnostic possibilitiesbeforeprescribingPPIs.
Ininfantswithnonspecificsymptomssuchascryingand irritability,diagnostictestsforGERDdonotcontributemuch to the investigation, unless it is a severe case or there areassociatedcomorbidities,suchasneurologicaldisease or operated esophagus. The healthy infant that does not respondtoconservativemeasuresisunlikelytohaveGERD. Thereis noevidencetojustify empirictreatment with acid suppression in infants and young children, as GERD symptoms are less specific.1 Hence, these drugs should be indicated when the diagnosis of reflux esophagitis is established.1
PPIs
PPIs areindicated in cases of erosive esophagitis, peptic
stricture,orBarrett’sesophagus,aswellasinchildrenthat
need amoreeffectiveblockade ofacidsecretion,for
ins-tance,in thosewithsevere chronicrespiratory diseaseor
neurologicalproblems.1 Thedifferences betweenthe PPIs
appeartobevery small,andpresentation playsacritical roleintheirselection.
PPIs are superior to H2-receptor antagonists, both in
ameliorating symptoms and healing lesions, and both are superior to placebo medication.1 In contrast with H
2
-blockers,theeffectofPPIsdoesnotdecreasewithchronic use. It maintains gastric pH > 4 for longer periods, and inhibitsacidsecretioninducedbyfeeding,whichare char-acteristics not presented by H2-blockers. Its potent acid
suppressionleadstoareductionofintragastricvolumefor 24hours,which facilitatesgastricemptyinganddecreases refluxvolume.1
The currently available PPIs are omeprazole, pan-toprazole, esomeprazole, lansoprazole, rabeprazole and dexlansoprazole. They may cause four types of side effects in children: idiosyncratic reactions, interactions with other drugs, hypergastrinemia, and drug-induced hypochlorhydria.1Theidiosyncraticeffectsoccurin approx-imately 14% of pediatric patients using PPIs:1 the most common are headache, diarrhea, constipation, and nau-sea, each of them occurs in approximately 2% to 7% of patients.1,3Parietalcellhyperplasiaandhyperplasticpolyps of the gastric fundus are benign abnormalities caused by acidblockingandbyhypergastrinemia.1Itshouldbe consid-ered that severalstudies have associatedhypochlorhydria due to PPIs tocommunity-acquired pneumonia, gastroen-teritis, candidiasis, and even enterocolitis in preterm infants.1,39,40 In adults, they may cause acute intersti-tial nephritis.1 Moreover, PPIs may alter the patient’s intestinal microbiota and some studies suggest that acid suppression may predispose to the development of food allergies.1,41
PPIsalsohavetheirlimitations,asaconsequenceoftheir pharmacologicalproperties.Theymustbeusedbeforethe firstmeal,42 andmust beprotectedfromstomachacid by an enteric coating. A major problem of PPIs in Brazil is thatthereis noliquid formulation.Customizedliquid for-mulationsarenottestedandtherefore,theireffectiveness is unknown. Opening the pill or crushing the tablet may inactivatethemedicationbyremovingthegastricacid pro-tection,sincePPIsneedtobeintactinordertobeabsorbed intheduodenum.Multiunitpelletsystem (MUPS) formula-tions,sincetheyaresolubleandcontainalargenumberof individualmicrosphereswithindividualentericprotection, allow forthe useof omeprazoleand esomeprazoleat any age andthrougha feedingtube, asit ispossible todilute thedrug.42
Omeprazolemay beused at dosesranging from 0.7to 3.5mg/kg/day.1,42.43 The maximum dose used in children
althoughscientificevidencefortheuseinthisagegroupis limited.44,45
Long-termPPIadministrationisnotadvisablewithout a previous investigation.1In caseswhereacid suppressionis required,theminimumpossibledoseshouldbeused.Most patients require a single daily dose. The routine use of twicedailydoseisnotindicated.Treatmentdiscontinuation shouldbeattemptedwheneverpossible,asfewpatientswill requirelong-termtreatments.38,40
Hassall et al.,46 in a recent study, demonstrated that 62.5%ofpatientswitherosiveesophagitiswhohadarelapse andrequiredchronictreatmentwithPPIshadapredisposing disease,suchasneurologicalalterationsoresophageal atre-sia.Only33% ofthosewhohadnopredisposingconditions toGERDrequiredprolongedtreatment.46
After prolonged use, the dose should be gradually reduced. In some patients, abrupt discontinuation of PPI treatment may cause a rebound effect on acid produc-tion, thus it is necessary to gradually wean the patient from the therapy.1 When PPIs are abruptly discontinued, theparietalcellmassthatwasblockedisreleasedfromits suppressionandacidhypersecretionreboundoccurs.47This may cause symptom exacerbation, requiring more PPIs,47 anaspectdemonstratedinastudyofasymptomaticadults that received PPIs for three months and developed gas-trointestinalsymptomswhenthe medicationwasabruptly discontinued.48
Use
and
abuse
of
acid
suppression
therapy
in
pediatrics
GERisaphysiologicalprocessinmostinfants.Studiesin
nor-malinfantshave demonstratedrefluxepisodesasoftenas
73timesaday,49 withregurgitationassociatedwithreflux
episodesin67%ofchildreninthefourthmonthoflife.50For thegreatmajorityofinfants(98%),GERsymptomsimprove upto12to15monthsofage,asthechilddevelops,lower esophagealsphinctermaturationoccurs,solidfoodis intro-duced, muscle toneincreases, andthe babyspends more timeintheupright position.51 Insummary,GER symptoms aremorecommoninyounginfants,withapeakat4months ofage,andtendtodisappearduringthesecondhalfofthe firstyearoflife.50,52Differently,GERDisnotfrequentinthis agegroup.
The response of infants to different stimuli, including GER and GERD, are nonspecific and very similar, making it sometimes difficult to establish the cause of irritabil-ityorcrying. Severalstudieshave demonstratedthat acid suppressiondoesnotcontrolsymptomssuchasirritability, crying, and fussiness, which areinterpreted as symptoms of GERD.53,54 There is also some evidence that placebo improves symptoms ininfants as muchasPPIs.53,54 In the largest double-blind,randomized, placebo-controlledtrial in which infants with GERD symptoms received a PPI or placebo,theresponsewasexactlythesameinbothgroups. Inthisstudy outofthepatientswhoreceivedplacebo,as wellasthosewhoreceivedPPI(lansoprazole)forfourweeks, 54%showedsatisfactoryresponse,butthegroupreceiving the active medication had more side effects.53 A smaller placebo-controlled trial with a different PPI showed very similarfindings.54
Itmustnotbeforgottenthatculturalfactorsaffect feed-ingpractices,andstudieshaveshownthatinfantswithGERD shouldbeevaluatedintermsoffeedingbehaviorrelatedto maternalpractices,problems,andbeliefs.
Maternal aspects that must be evaluated are depres-sion,anxiety,feedingproblems,andimpairedmother---child interaction.55,56 Maladaptive eating behaviors should also receive proper attention. Interventions may be needed beforeanegativereinforcement,includingtestsand medi-cations,iscreated.55,56
Accordingtosomestudies,38,40,57---59thereisanepidemic ofoveruseofPPIsinthefirstyearoflifeinNorthAmerica; thisalsoappearstobethecaseinBrazil.Astudyof575,000 prescriptionsin theUnited States,demonstrated thatthe numberof gastricacid-suppressingmedicationsprescribed to children under 4 years of age increased 56% between 2002and2006.60 Theyestimatedthat3%ofallchildrenin thisagegroupwerereceivingsometypeofmedicationfor acidsuppression.60 Thehighestincreasewasamonginfants below1yearofage.AnotherNorthAmericanstudyobserved an increase of more than seven-fold in PPI use between the years of 1999 and 2004, and the use of a liquid for-mulationforbabiespresenteda16-foldincreaseduringthis period.60
ReviewersoftheFoodandDrugAdministration(FDA)in theUnitedStatespublishedanarticleintheJournalof Pedi-atricGastroenterologyandNutrition61 inJanuary of2012, reviewingthestudiescommissionedtothepharmaceutical industryon PPI use in the first year of life. According to theseauthors,theincreaseinprescriptionsforPPIsinthe firstyearoflifewas11-foldbetween2002and2009.61They evaluatedfourrandomizedcontrolledtrialsandconcluded thatPPIsshouldnotbeadministeredtotreatsymptomsof GERinnormalinfantswithoutsolidevidencethatacidisthe causeofthe symptoms.61 This article offersthe following conclusions:
• NormalinfantswithsymptomsofGERshouldbeinitially
treatedwithconservativemeasures(dietaryandpostural guidelines),andevaluatedforCMPA.Mostoftheseinfants improvewithtimeanddonothaveacid-induceddisease, and thus theydonot benefitfromPPIs. Ifconservative measures fail,andtheinvestigationof anotheretiology isnegative,thepatientshouldbereferredtoapediatric gastroenterologist.
• TheuseofPPIsshouldbereservedforinfantswith
docu-mentedacid-induceddisease,suchaserosiveesophagitis. Withoutprovenevidence,thebalancebetweenrisksand benefitsofPPIsisnotfavorableinthisagegroup,andthe long-termeffectsoftheirusehavenotbeenstudied.
• Shortandlong-termsafetystudiesarelimited.
• Thediagnostictestsavailableandsymptomsarenot
accu-rateenoughtoindicatetreatmentwithPPIsininfants.
• MorestudiesevaluatingPPIsshouldbeperformed,
espe-ciallyin infantswitherosiveesophagitis,cysticfibrosis, shortbowel,andextra-esophagealmanifestations.In ero-siveesophagitis,efficacycanbeextrapolatedfromother studiesinadultsandchildren.61
Ferreira
CT
et
al.
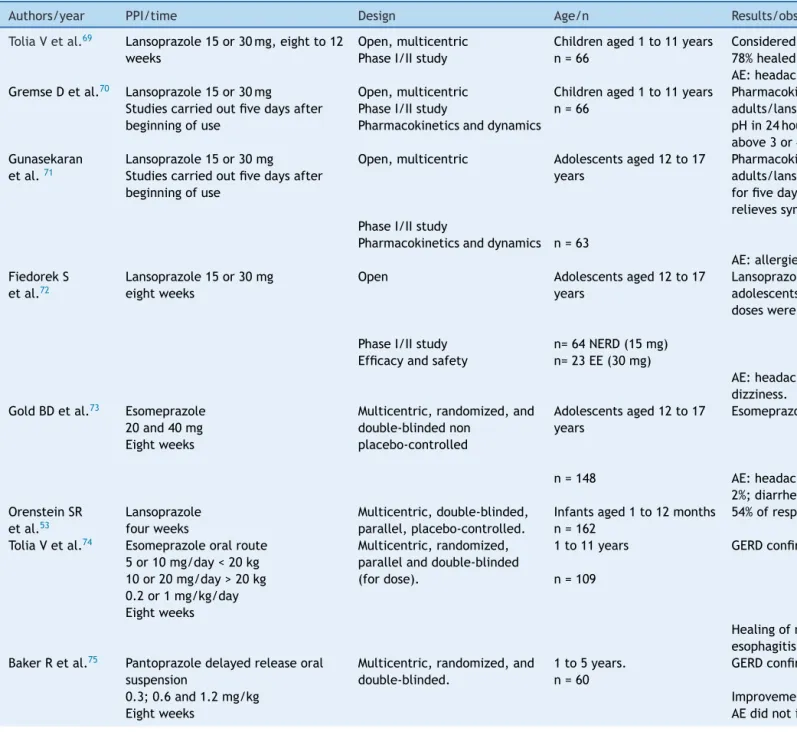
Table2 StudieswithPPIsinpediatricGERD.
Authors/year PPI/time Design Age/n Results/observations
ToliaVetal.69 Lansoprazole15or30mg,eightto12
weeks
Open,multicentric PhaseI/IIstudy
Childrenaged1to11years n=66
Consideredsafeandwelltolerated
78%healedEEinweekeight,and100%inweek12 AE:headache,constipation.
GremseDetal.70 Lansoprazole15or30mg
Studiescarriedoutfivedaysafter beginningofuse
Open,multicentric PhaseI/IIstudy
Pharmacokineticsanddynamics
Childrenaged1to11years n=66
Pharmacokineticpropertiessimilarto
adults/lansoprazoleincreasesmeanintragastric pHin24hoursandthe%oftimeinwhichpHis above3or4
Gunasekaran etal.71
Lansoprazole15or30mg Studiescarriedoutfivedaysafter beginningofuse
Open,multicentric Adolescentsaged12to17 years
Pharmacokineticpropertiessimilarto
adults/lansoprazole15mgor30mg1x/dayused forfivedaysincreasestheintragastricpH, relievessymptoms,andiswelltolerated PhaseI/IIstudy
Pharmacokineticsanddynamics n=63
AE:allergies,diarrhea,rash,dizziness. FiedorekS
etal.72
Lansoprazole15or30mg eightweeks
Open Adolescentsaged12to17 years
Lansoprazole15and30mgreducedsymptomsof adolescentswithNERDandEE,respectively.Both doseswereconsideredsafe
PhaseI/IIstudy n=64NERD(15mg) Efficacyandsafety n=23EE(30mg)
AE:headache,abdominalpain,nauseaand dizziness.
GoldBDetal.73 Esomeprazole
20and40mg Eightweeks
Multicentric,randomized,and double-blindednon
placebo-controlled
Adolescentsaged12to17 years
Esomeprazoledecreasedsymptomsinbothgroups
n=148 AE:headache,8%;abdominalpain,3%;nausea, 2%;diarrhea,2%.NosevereAE
OrensteinSR etal.53
Lansoprazole fourweeks
Multicentric,double-blinded, parallel,placebo-controlled.
Infantsaged1to12months n=162
54%ofresponseinthetwogroups
ToliaVetal.74 Esomeprazoleoralroute
5or10mg/day<20kg 10or20mg/day>20kg 0.2or1mg/kg/day Eightweeks
Multicentric,randomized, parallelanddouble-blinded (fordose).
1to11years
n=109
GERDconfirmedendoscopicallyorhistologically
Healingofmacroormicroscopicerosive esophagitis
BakerRetal.75 Pantoprazoledelayedreleaseoral
suspension
Multicentric,randomized,and double-blinded.
1to5years. n=60
GERDconfirmedendoscopicallyorhistologically
0.3;0.6and1.2mg/kg Improvementofsymptoms
reflux
disease
115
Table2(Continued)
Authors/year PPI/time Design Age/n Results/observations
Winteretal.51 Pantoprazoledelayed-releaseoral
granules
Randomized,double-blinded, placebo-controlled(treatment andwithdrawal)
1to11months n=106
PatientswithGERDsymptoms
Inblindphase,nodifferencesbetweenthe withdrawalofpantoprazoleorplacebodueto lackofefficacy
1.2mg/kg/day
Fourweeksofpantoprazoleandfour weeksdouble-blindpantoprazolex placebo
Safeandwelltolerated
TammaraBK etal.76
Pantoprazole 0.6mg/kg 1.2mg/lg
Multicentric,open, randomized. Pharmacokinetics
Study1--- 1monthto12 months
n=43
Exposureincreaseswithincreasingdose,but thereisgreatindividualvariation.
Study1 Oralgranules Study2--- 1yearto<6years Exposurewassimilartoadults. Study2 Measurementsperformedatleast
afterfiveconsecutivedoses
n=17 Welltolerated.
WardRMetal.77 Delayed-releasepantoprazoletablets Multicentric,open,
randomized.
6to16years. PatientswithGERDhavethesamesystemic exposureofadults.
20or40mg/day n=38 Noseriousadverseeffects. Measurementsperformed12hours
afterasingledoseandtwotofour hoursaftermultipledoses
Pharmacokineticsandsafety
SandströmM etal.78
EsomeprazoleIV1x/day Fourdays
Multicentric,open, randomized,PhaseI
0to17years. Clearanceincreaseswithweightandage.
Welltolerated 31patientswithAE Pharmacokineticsand
tolerabilityIV
n=57 NosevereAE
KukulkaMetal.79 MRdexlansoprazole
30or60mgforsevendays
Multicentric,parallel,open, PhaseI
Pharmacokineticsandsafety
2to17years. n=36
Pharmacokineticssimilartoadults Mildadverseeffects(33.3%)
WinterHetal.80 Esomeprazole
2.5to10mg/day Fourweeks
Multicentric,randomized, double-blinded,
placebo-controlled(treatment andwithdrawal)
1to11months n=98
Therewasnostatisticaldifferenceintreatment interruptionduetoworseningofsymptoms betweenesomeprazoleandplacebo
Hassalletal.46 Omeprazole
0.7to3.5mg/kg/day 21months
Prospective,open,long-term totestmaintenancedose.
1to16yearswithhealedEE n=32(completedthestudy)
Remissionwasachievedwithcontinuoususeof omeprazoleinmostpatients.
60%requiredmorethanhalfofthedoserequired forhealing
nonspecificmanifestationsascryingandirritability.55,59This exaggeration regarding the treatment of GERD in infants does not occur without potential adverse effects docu-mented in the literature. Gastric acid is important for protectionagainstinfectionsandfortheabsorptionof cer-tainnutrients.38
Currently, there are very few randomized controlled trials providing support for the use of medications to treat symptoms consistent with GERD in the first year of life.62 However,astudywith1,245Americanpediatricians observedthat82%oftherespondentsagreedthattheywould startempiricalacidsuppressionbeforeorderingdiagnostic tests.63
In this context, the possible benefits of a non-pharmacological conservative treatment, with changes in diet and lifestyle, are important in order to not expose infantstounnecessarymedicationsandtopreventadverse effectsand costs.64 Shalaby etal.65 conducteda study in whichanurse,experiencedinGER/GERDguidelines,advised parentsofinfantswithsuspectedsymptomsofGERDby tele-phoneonconservativemeasures. These recommendations reducedsymptomsin26%ofinfants,thusavoidingtheneed forconsultationwiththegastroenterologist.65Patientswere instructedtousethickenedand/or extensivelyhydrolyzed formula,orthemotherwasinstructed tofollow aCMand soyeliminationdiet,toavoidexposuretosmoke,andto fol-lowthepositionguidelines.Aftertwoweeks,78%ofpatients improved,ofwhom59%presentedadecreaseinatleastfive itemsofthesymptomquestionnaire,and24%remainedfree ofsymptoms.65
Final
considerations
Infants have nonspecific responses to different
patho-logical and non-pathological stimuli: crying, irritability,
refusal to eat, sleep disorders, back arching, and
appar-ent discomfort.66 Pediatricians have less time to listen
to parents and caregivers, rather than taking a com-plete history that includes behavioral and dietary details and reassuring them. Furthermore there is an additional pressure to ‘‘solve the problem’’ and ‘‘do something’’ which leads the pediatrician tochoose the fast track: to prescribe!
Itappearstobelessrisky,butitbringsconsequencesfor thepatients,asitislessexpensivetotryamoreconservative approachratherthan prescribingseveral medications.67,68 In the light of current knowledge, it would be better to advisepatientsandtheircaregiversandtoprescribefewer medications.
Inpatientswithpersistentsymptoms,referraltoa pedi-atricgastroenterologistisadvisedinordertoassesstheneed ofdiagnosticinvestigations,andproperpharmacologicalor possiblesurgicaltreatment. StudiesonPPIuseinchildren arepresentedinTable2.46,51,53,69---80
Conflicts
of
interest
Allauthorshave receivedhonorariafor educational
activ-ities organized by Support, Abbott, Danone, and Nestlé
Nutrition.
References
1.Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, et al. Pediatric gastroesophageal reflux clinical practiceguidelines:jointrecommendationsoftheNorth Amer-ican Societyfor PediatricGastroenterology, Hepatology, and Nutrition(NASPGHAN)andtheEuropeanSocietyforPediatric Gastroenterology,Hepatology,andNutrition(ESPGHAN).J Pedi-atrGastroenterolNutr.2009;49:498---547.
2.OrensteinSR,IzadniaF,KhanS.Gastroesophagealrefluxdisease inchildren.GastroenterolClinNorthAm.1999;28:947---69. 3.LightdaleJR, Gremse DA.Section on Gastroenterology
Hep-atology,andNutrition.Gastroesophagealreflux:management guidanceforthepediatrician.Pediatrics.2013;131:e1684---95. 4.van der Pol R, Smite M, Benninga MA, van Wijk MP.
Non-pharmacologicaltherapiesforGERDininfantsandchildren.J PediatrGastroenterolNutr.2011;53:S6---8.
5.WenzlTG.RoleofdiagnostictestsinGERD.JPediatr Gastroen-terolNutr.2011;53:S4---6.
6.FerreiraCT,CarvalhoE.Doenc¸adorefluxogastroesofágico.In: CarvalhoE,SilvaLR,FerreiraCT,editors.Gastroenterologiae nutric¸ãoempediatria.Barueri,SP:Metha;2012.p.91---132. 7.JangHS,LeeJS,LimGY,ChoiBG,ChoiGH,ParkSH.Correlation
ofcolorDopplersonographicfindingswithpH measurements in gastroesophageal reflux in children. J Clin Ultrasound. 2001;29:212---7.
8.Savino A, Cecamore C, Matronola MF, Verrotti A, Mohn A, ChiarelliF,etal.USinthediagnosisofgastroesophagealreflux inchildren.PediatrRadiol.2012;42:515---24.
9.CollettiRB,ChristieDL,OrensteinSR.StatementoftheNorth AmericanSocietyforPediatricGastroenterologyandNutrition (NASPGN)IndicationsforpediatricesophagealpHmonitoring.J PediatrGastroenterolNutr.1995;21:253---62.
10.PutnamPE. Obituary:thedeathof thepH probe.J Pediatr. 2010;157:878---80.
11.HassallE.EsophagealpHstudy:rumorsofitsdeatharegreatly exaggerated.JPediatr.2011;159:519.
12.Wenzl TG, Moroder C, Trachterna M, Thomson M, Silny J, HeimannG, etal. Esophageal pHmonitoring andimpedance measurement:acomparisonoftwodiagnostictestsfor gastroe-sophagealreflux.JPediatrGastroenterolNutr.2002;34:519---23. 13.WenzlTG,BenningaMA,LootsCM,SalvatoreS,VandenplasY, ESPGHANEURO-PIGWorkingGroup.Indications,methodology, andinterpretationofcombinedesophagealimpedance-pH mon-itoring in children: ESPGHAN EURO-PIG standardprotocol. J PediatrGastroenterolNutr.2012;55:230---4.
14.VandenplasY, Veereman-WautersG, DeGreef E,DevrekerT, HauserB,BenningaM,etal.Gastrointestinalmanifestationof cow’smilkproteinallergyorintoleranceandgastrointestinal motility.JPediatrGastroenterolNutr.2011;53:S15---7. 15.BorrelliO,ManciniV,ThaparN,GiorgioV,ElawadM,HillS,etal.
Cow’smilkchallengeincreasesweaklyacidicrefluxinchildren withcow’smilkallergyandgastroesophagealrefluxdisease.J Pediatr.2012;161:476---81,e1.
16.Iacono G, Carroccio A, Cavataio F, Montalto G, Kazmierska I, Lorello D, et al. Gastroesophageal reflux and cow’s milk allergyininfants:aprospectivestudy.JAllergyClinImmunol. 1996;97:822---7.
17.Nielsen RG, Bindslev-Jensen C, Kruse-Andersen S, Husby S. Severegastroesophageal refluxdisease and cow milk hyper-sensitivity in infants and children: disease association and evaluationofanewchallengeprocedure.JPediatr Gastroen-terolNutr.2004;39:383---91.
19.CavataioF,IaconoG,MontaltoG,SoresiM,TumminelloM, Cam-pagnaP,etal.Gastroesophagealrefluxassociatedwithcow’s milkallergyininfants:whichdiagnosticexaminationsare use-ful?AmJGastroenterol.1996;91:1215---20.
20.Koletzko S, Niggemann B, Arato A, Dias JA, Heuschkel R, HusbyS,etal.Diagnosticapproachandmanagementof cow’s-milk protein allergy in infants and children: ESPGHAN GI Committeepracticalguidelines.JPediatrGastroenterolNutr. 2012;55:221---9.
21.Catto-SmithAG,Tan D,Gall DG,ScottRB. Ratgastricmotor responseto foodprotein-inducedanaphylaxis. Gastroenterol-ogy.1994;106:1505---13.
22.RavelliAM,TobanelliP,VolpiS,UgazioAG.Vomitingandgastric motilityininfantswithcow’smilkallergy.JPediatr Gastroen-terolNutr.2001;32:59---64.
23.SchäppiMG,BorrelliO,KnafelzD,WilliamsS,SmithVV,Milla PJ,etal.Mastcell-nerveinteractionsinchildrenwithfunctional dyspepsia.JPediatrGastroenterolNutr.2008;47:472---80. 24.EmerenzianiS,SifrimD.Gastroesophagealrefluxand gastric
emptying,revisited.CurrGastroenterolRep.2005;7:190---5. 25.BraeggerC,ChmielewskaA, DecsiT, Kolacek S,MihatschW,
MorenoL,etal.Supplementationofinfantformulawith probi-oticsand/orprebiotics:asystematicreviewandcommentby theESPGHANcommitteeonnutrition.JPediatrGastroenterol Nutr.2011;52:238---50.
26.GarziA,MessinaM,FratiF,CarfagnaL,ZagordoL,BelcastroM, etal.Anextensivelyhydrolysedcow’smilkformulaimproves clinicalsymptomsofgastroesophagealrefluxandreducesthe gastricemptyingtimeininfants.AllergolImmunopathol(Madr). 2002;30:36---41.
27.NielsenRG,FengerC,Bindslev-JensenC,HusbyS.Eosinophilia intheuppergastrointestinaltractisnotacharacteristicfeature incow’smilksensitivegastro-oesophagealrefluxdisease Mea-surementbytwomethodologies.JClinPathol.2006;59:89---94. 28.SemeniukJ, Kaczmarski M,U´scinowicz M.Manometric study oflower esophagealsphincter inchildren withprimary acid gastroesophagealrefluxandacidgastroesophagealreflux sec-ondarytofoodallergy.AdvMedSci.2008;53:283---92.
29.SemeniukJ,KaczmarskiM,U´scinowiczM.Endoscopicpicture ofesophagitisinchildrenwithprimaryandsecondaryacid gas-troesophagealreflux.PolMerkurLekarski.2008;24:212---8. 30.SemeniukJ,KaczmarskiM,WasilewskaJ.Serumgastrin
concen-trationsinchildrenwithprimarygastroesophagealrefluxand gastroesophagealreflux secondarytocow’smilkallergy. Adv MedSci.2011;56:186---92.
31.FarahmandF,NajafiM,AtaeeP,ModarresiV,ShahrakiT,Rezaei N.Cow’s milkallergy amongchildren withgastroesophageal refluxdisease.GutLiver.2011;5:298---301.
32.HorvathA,DziechciarzP,SzajewskaH.Theeffectof thickened-feed interventions on gastroesophageal reflux in infants: systematicreviewandmeta-analysisofrandomized,controlled trials.Pediatrics.2008;122:e1268---77.
33.CraigWR,Hanlon-DearmanA,SinclairC,TabackS,MoffattM. Metoclopramide,thickenedfeedings,andpositioningfor gastro-oesophageal reflux in children under two years. Cochrane DatabaseSystRev.2004;(4):CD003502.
34.DunneCE,BusheeJL,ArgikarUA.Metabolismofbromopridein mouse,rat,rabbit,dog,monkey,andhumanhepatocytes.Drug MetabPharmacokinet.2013Apr23[Epubaheadofprint]. 35.PritchardDS, BaberN,StephensonT.Shoulddomperidonebe
usedfor the treatmentof gastro-oesophageal refluxin chil-dren? Systematic review of randomized controlled trials in childrenaged 1month to11yearsold.Br JClinPharmacol. 2005;59:725---9.
36.VieiraMC,MiyagueNI,VanSteenK,SalvatoreS,VandenplasY. EffectsofdomperidoneonQTcintervalininfants.ActaPaediatr. 2012;101:494---6.
37.DjeddiD,KongoloG,LefaixC,MounardJ,LékéA.Effectof dom-peridoneonQTintervalinneonates.JPediatr.2008;153:663---6. 38.HassallE.Over-prescriptionofacid-suppressingmedicationsin infants:howit cameabout,whyit’swrong,and what todo aboutit.JPediatr.2012;160:193---8.
39.CananiRB,CirilloP,RoggeroP,RomanoC,MalamisuraB,Terrin G,etal.Therapywithgastricacidityinhibitorsincreasestherisk ofacutegastroenteritisandcommunity-acquiredpneumoniain children.Pediatrics.2006;117:e817---20.
40.HassallE.Usesandabusesofacid-suppressiontherapyin chil-dren.JPediatrGastroenterolNutr.2011;53:S8---9.
41.UntersmayrE,Jensen-JarolimE.Theroleofproteindigestibility andantacidsonfoodallergyoutcomes.JAllergyClinImmunol. 2008;121:1301---8.
42.AnderssonT,HassallE,LundborgP,ShepherdR,RadkeM,Marcon M,etal.Pharmacokineticsoforallyadministeredomeprazole inchildrenInternationalPediatricOmeprazolePharmacokinetic Group.AmJGastroenterol.2000;95:3101---6.
43.Hassall E, Israel D, Shepherd R, Radke M, Dalväg A, Sköld B, et al., International Pediatric Omeprazole Study Group. Omeprazolefortreatmentofchronicerosiveesophagitisin chil-dren:amulticenterstudyofefficacy,safety,tolerabilityand doserequirements.JPediatr.2000;137:800---7.
44.TafuriG,TrottaF,LeufkensHG,MartiniN,SaglioccaL,Traversa G. Off-labeluse ofmedicinesinchildren: canavailable evi-denceavoiduselesspaediatrictrials?Thecaseofprotonpump inhibitorsforthetreatmentofgastroesophagealrefluxdisease. EurJClinPharmacol.2009;65:209---16.
45.vanderPolRJ,SmitsMJ,vanWijkMP,OmariTI,TabbersMM, Benninga MA. Efficacyof proton-pump inhibitorsin children withgastroesophagealrefluxdisease:asystematicreview. Pedi-atrics.2011;127:925---35.
46.HassallE,ShepherdR,KoletzkoS,RadkeM,HendersonC, Lund-borgP.Long-termmaintenancetreatmentwithomeprazolein childrenwithhealederosiveoesophagitis:aprospectivestudy. AlimentPharmacolTher.2012;35:368---79.
47.Fossmark R,Johnsen G, JohanessenE,Waldum HL.Rebound acidhypersecretionafterlong-terminhibitionofgastricacid secretion.AlimentPharmacolTher.2005;21:149---54.
48.Reimer C, Søndergaard B, Hilsted L, Bytzer P. Proton-pump inhibitor therapy induces acid-related symptoms in healthy volunteers after withdrawal of therapy. Gastroenterology. 2009;137:80---7.
49.VandenplasY,GoyvaertsH,HelvenR,SacreL.Gastroesophageal reflux,asmeasuredby24-hourpHmonitoring,in509healthy infantsscreenedforriskofsuddeninfantdeathsyndrome. Pedi-atrics.1991;88:834---40.
50.NelsonSP, ChenEH,SyniarGM,ChristoffelKK.Prevalenceof symptomsofgastroesophagealrefluxduringinfancy.Apediatric practice-basedsurveyPediatricPracticeResearchGroup.Arch PediatrAdolescMed.1997;151:569---72.
51.WinterH,Kum-NjiP,MahomedySH,KierkusJ,HinzM,LiH,etal. Efficacyandsafetyofpantoprazoledelayed-releasegranulesfor oralsuspensioninaplacebo-controlledtreatment-withdrawal studyin infants 1-11 monthsold withsymptomatic GERD.J PediatrGastroenterolNutr.2010;50:609---18.
52.OrensteinSR, Shalaby TM,KelseySF, FrankelE. Natural his-toryofinfantrefluxesophagitis:symptomsandmorphometric histologyduringoneyearwithoutpharmacotherapy.AmJ Gas-troenterol.2006;101:628---40.
53.Orenstein SR, Hassall E, Furmaga-Jablonska W, Atkinson S, Raanan M. Multicenter, double-blind, randomized, placebo-controlledtrialassessingtheefficacyandsafetyofprotonpump inhibitor lansoprazole in infants with symptoms of gastroe-sophagealrefluxdisease.JPediatr.2009;154:514---20. 54.Moore DJ, Tao BS, Lines DR, Hirte C, Heddle ML,
in irritable infants with gastroesophageal reflux. J Pediatr. 2003;143:219---23.
55.LifschitzC.Thinkingoutsidetheboxwhendealingwithpatients withGERDandfeedingproblems.JPediatrGastroenterolNutr. 2011;53:358.
56.KaracetinG,DemirT,ErkanT,CokugrasFC,SonmezBA. Mater-nalpsychopathologyandpsychomotordevelopmentofchildren withGERD.JPediatrGastroenterolNutr.2011;53:380---5. 57.OrensteinSR,HassallE.Pantoprazoleforsymptoms ofinfant
GERD:theemperorhasnoclothes!JPediatrGastroenterolNutr. 2010;51:537.
58.OrensteinSR, Hassall E.Infantsand proton pumpinhibitors: tribulations, no trials. J Pediatr Gastroenterol Nutr. 2007;45:395---8.
59.HassallE,OwenD.Long-termuseofPPIsinchildren:wehave questions.DigDisSci.2008;53:1158---60.
60.Balistreri WF. The reflex to treat reflux --- let’s be conser-vative regarding gastroesophageal reflux (GER)! J Pediatr. 2008;152:A1.
61.ChenIL,GaoWY,JohnsonAP,NiakA,TroianiJ,KorvickJ,etal. Protonpumpinhibitoruseininfants:FDAreviewerexperience. JPediatrGastroenterolNutr.2012;54:8---14.
62.BarronJJ,TanH,SpaldingJ,BakstAW,SingerJ.Protonpump inhibitorutilizationpatternsininfants.JPediatrGastroenterol Nutr.2007;45:421---7.
63.DiazDM,WinterHS,CollettiRB,FerryGD,RudolphCD,CzinnSJ, etal.Knowledge,attitudesandpracticestylesofNorth Amer-icanpediatriciansregardinggastroesophagealrefluxdisease.J PediatrGastroenterolNutr.2007;45:56---64.
64.OrensteinSR, McGowanJD. Efficacy ofconservativetherapy astaughtintheprimarycaresettingforsymptomssuggesting infantgastroesophagealreflux.JPediatr.2008;152:310---4. 65.Shalaby TM, Orenstein SR. Efficacy of telephone teaching
of conservative therapy for infants with symptomatic gas-troesophageal reflux referred by pediatricians to pediatric gastroenterologists.JPediatr.2003;142:57---61.
66.HassallE,Talkischeap.ofteneffective:symptomsininfants often respond to non-pharmacologic measures. J Pediatr. 2008;152:301---3.
67.Czinn SJ, Blanchard S. Gastroesophageal reflux disease in neonatesandinfants:whenandhowtotreat.PaediatrDrugs. 2013;15:19---27.
68.ForbesD.Mewlingandpuking:infantilegastroesophagealreflux inthe21stcentury.JPaediatrChildHealth.2013;49:259---63. 69.Tolia V, Ferry G, Gunasekaran T, Huang B, Keith R, Book
L. Efficacy of lansoprazole in the treatment of gastroe-sophageal refluxdiseasein children.J PediatrGastroenterol Nutr.2002;35:S308---18.
70.GremseD,Winter H, Tolia V,GunasekaranT, Pan WJ, Karol M,etal.Pharmacokineticsandpharmacodynamicsof lansopra-zoleinchildrenwithgastroesophagealrefluxdisease.JPediatr GastroenterolNutr.2002;35:S319---26.
71.GunasekaranT, Gupta S, Gremse D, Karol M, Pan WJ, Chiu YL,etal. Lansoprazoleinadolescentswithgastroesophageal refluxdisease:pharmacokinetics,pharmacodynamics,symptom reliefefficacy,and tolerability.JPediatrGastroenterolNutr. 2002;35:S327---35.
72.Fiedorek S, Tolia V, Gold BD, Huang B, Stolle J, Lee C, etal.Efficacyand safetyoflansoprazoleinadolescentswith symptomaticerosive andnon-erosivegastroesophageal reflux disease.JPediatrGastroenterolNutr.2005;40:319---27. 73.GoldBD,GunasekaranT,ToliaV,WetzlerG,ConterH,Traxler
B,etal.Safetyandsymptomimprovementwithesomeprazole inadolescentswithgastroesophagealrefluxdisease.JPediatr GastroenterolNutr.2007;45:520---9.
74.ToliaV,YoussefNN,GilgerMA,TraxlerB,IlluecaM. Esomepra-zolefor thetreatmentoferosiveesophagitisin children:an international,multicenter,randomized,parallel-group, double-blind(fordose)study.BMCPediatr.2010;10:41.
75.BakerR,TsouVM,TungJ,BakerSS,LiH,WangW,etal. Clini-calresultsfromarandomized,double-blind,dose-rangingstudy ofpantoprazoleinchildrenaged1through5yearswith symp-tomatichistologicorerosiveesophagitis.ClinPediatr(Phila). 2010;49:852---65.
76.Tammara BK, Sullivan JE, Adcock KG, Kierkus J, Giblin J, RathN, etal. Randomized,open-label, multicentre pharma-cokineticstudiesoftwodose levelsofpantoprazolegranules in infants and children aged 1 month through < 6 years with gastro-oesophageal reflux disease. Clin Pharmacokinet. 2011;50:541---50.
77.WardRM,KearnsGL,TammaraB,BishopP,O’GormanMA,James LP,etal.Amulticenter,randomized,open-label, pharmacoki-neticsandsafetystudyofpantoprazoletabletsinchildrenand adolescents aged 6 through 16 years with gastroesophageal refluxdisease.JClinPharmacol.2011;51:876---87.
78.SandströmM,Davidson G, ToliaV,Sullivan JE, LångströmG, LundborgP,etal.PhaseI,multicenter,randomized,open-label study evaluatingthe pharmacokinetics and safety profile of repeatedonce-dailydosesofintravenousesomeprazolein chil-dren0to17yearsofage.ClinTher.2012;34:1828---38. 79.Kukulka M,Wu J, Perez MC.Pharmacokinetics and safetyof
dexlansoprazoleMRinadolescentswithsymptomaticGERD.J PediatrGastroenterolNutr.2012;54:41---7.