www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Hearing
preservation
and
cochlear
implants
according
to
inner
ear
approach:
multicentric
evaluation
夽
,
夽夽
Alexandre
Caixeta
Guimarães
a,∗,
Guilherme
Machado
de
Carvalho
a,
Alexandre
S.M.
Duarte
a,
Walter
A.
Bianchini
a,
Andrea
Bravo
Sarasty
b,
Maria
Fernanda
di
Gregorio
c,
Mario
Emilio
Zernotti
d,
Edi
Lúcia
Sartorato
e,
Arthur
Menino
Castilho
faFaculdadedeCiênciasMédicas,UniversidadeEstadualdeCampinas(FCM/UNICAMP),Campinas,SP,Brazil bUniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
cUniversidadeNacionaldeCórdoba,Córdoba,Argentina dUniversidadeCatólicadeCórdoba,Córdoba,Argentina
eCBMEG,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
fDepartmentofOtolaryngologyandOphthalmology,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
Received4December2013;accepted4June2014 Availableonline27December2014
KEYWORDS
Cochlearimplants; Innerear;
Correctionofhearing impairment;
Bilateralhearingloss
Abstract
Introduction:Electroacousticstimulationisanexcellentoptionforpeoplewithresidualhearing inthelowfrequencies,whoobtaininsufficientbenefitwithhearingaids.Tobeeffective,the subject’sresidualhearingshouldbepreservedduringcochlearimplantsurgery.
Objectives:Toevaluatethehearingpreservationinpatientsthatunderwentimplantplacement andtocomparetheresultsinaccordancewiththeapproachtotheinnerear.
Methods:19subjectsunderwentasoftsurgicaltechnique,andtheelectrodeMED-ELFLEXTM
EAS,designedtobeatraumatic,wasused.Weevaluatedpre-andpostoperativetonal audio-metrictestswithanaverageof18.4monthsafterimplantation,tomeasuretherateofhearing preservation.
Results:17patientshadtotalorpartialpreservationofresidualhearing;5hadtotalhearing preservation andtwoindividualshadnopreservation ofhearing.The insertionofthe elec-trodeoccurredthroughacochleostomyin3patients,andin2ofthesetherewasnohearing preservation;theother16patients experiencedelectrodeinsertionthrougharoundwindow approach. Allpatients benefitedfrom thecochlearimplant, eventhosewho areonlyusing electricalstimulation.
夽 Pleasecitethisarticleas:GuimarãesAC,deCarvalhoGM,DuarteAS,BianchiniWA,SarastyAB,diGregorioMF,etal.Hearingpreservation
andcochlearimplantsaccordingtoinnerearapproach:multicentricevaluation.BrazJOtorhinolaryngol.2015;81:190---6.
夽夽
Institution:UniversidadeEstadualde(UNICAMP),Campinas,SP,Brazil;andUniversidadeCatólicadeCórdoba,Argentina.
∗Correspondingauthor.
E-mail:[email protected](A.C.Guimarães).
http://dx.doi.org/10.1016/j.bjorl.2014.12.002
Conclusion: The hearing preservation occurred in89.4% ofcases. There was nosignificant differencebetweentheformsofinnerearapproach.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Implantecoclear; Orelhainterna; Correc¸ãode deficiênciaauditiva; Perdaauditiva bilateral
Preservac¸ãoauditivaeimplantecocleardeacordocomaabordagemdaorelha
interna:avaliac¸ãomulticêntrica
Resumo
Introduc¸ão: A estimulac¸ãoeletroacústica éumaexcelente opc¸ão parapessoascomaudic¸ão residual nas baixasfrequências, queobtêm benefício insuficientecom aparelhos auditivos. Parasereficaz,aaudic¸ãoresidualdeveserpreservadaduranteacirurgiadeimplantecoclear.
Objetivos: Avaliarapreservac¸ãoauditivadepacientesimplantadosecompararosresultados deacordocomaabordagemdaorelhainterna.
Método: 19indivíduosforamimplantadoscomumatécnicacirúrgicaparapreservac¸ãoauditiva, tendosidoutilizadooeletrodoMED-EL FLEXTM EAS,concebidoparaser atraumático.Foram
avaliadososexamesaudiométricos tonaisnopréepós-operatório,comuma médiade18,4 mesesapósoimplanteparamedirataxadepreservac¸ãodaaudic¸ãoresidual.
Resultados: 17 pacientes tiveram preservac¸ão total ou parcial da audic¸ão residual; cinco obtiverampreservac¸ãodaaudic¸ãototaledoisindivíduosnãotiverampreservac¸ãodaaudic¸ão. Ainserc¸ãodoeletrodoocorreuporcocleostomiaem3pacientes;em 2destespacientesnão houvepreservac¸ãodaaudic¸ão.Osoutros16 pacientesforamsubmetidos àabordagempela janelaredonda.Todosospacientesforambeneficiadoscomoimplantecoclear,mesmoaqueles pacientesqueutilizandoapenasestimulac¸ãoelétrica.
Conclusão:Apreservac¸ãoauditivaocorreuem89,4%doscasos.Nãohouvediferenc¸a significa-tivaentreasformasdeabordagemdaorelhainterna.
©2014Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Electroacousticstimulationisanexcellentoptionforpeople whohave residual hearing at low frequencies, but notat highfrequencies,andachieveinsufficientbenefitswiththe use of hearingaids. Foran electroacousticstimulation to bemosteffective,thepatient’sresidualhearingshouldbe preservedduringcochlearimplant(CI)surgery.
In recent decades, several electrodes were developed and refined in order to cause the least possible dam-agetothecochlearstructures,therebypreservingresidual hearing.1---4However,forthepreservationtobesuccessful,in
additiontoanappropriateelectrode,aspecialsurgical tech-nique is essential. After the earliestoperations, in which a conventional cochlear implant electrode was partially inserted into the cochlea,5 the so-called ‘‘soft surgery’’
wasdeveloped,strivingforalesstraumaticoperation.This surgeryaimstopreservehearing,andmanyadvanceshave occurredsincethen.6,7
Theroutefortheintroductionoftheelectrodeintothe cochleaisonefacetofthesurgicaltechniquethathasbeen especiallystudiedanddiscussed.
Initially, insertion through the round window was the standard technique for hearing preservation surgery. This technique consists of a minimal incision through the
membrane,withnoneed fordrilling thecochlea,thereby reducingacoustictrauma andthepossibilityof bone frag-mentsenteringthescalatympani.8
However, a recently published study showed that the angle of insertion of the electrode is similar for both techniques (through the round window and by cochleostomy), and in both procedures, tissue dam-age will be minimal if an electrode designed for hearing protection is used.9 In a systematic
litera-ture review in 2013 comparing the two approaches, we could not find a single study specifically comparing insertion techniques; the levels of hearing preservation were similar between the two approaches, being slightly higherin patients undergoinginsertion throughthe round window.8
Currently,suchdatacomprisethelargestcase seriesof patientswhounderwentthetechniqueofhearing preserva-tionincochlearimplantationinLatinAmerica.Furthermore, thisgroupofpatientshasalsobeenbenefitedwithalonger postoperativefollow-up.
125 250 500 750 1000 1500 2000 3000 4000 5000 6000
Frequency (HZ)
A
uditor
y threshold (dB)
-10 0 10 20 30 40 50 60 70 80 90 100 110 120 130
Coventional Hearing Aid
Conventional Cochlear Implant
Cochlear Hybrid Implant
Figure 1 Illustrative graphic of the audiometric pattern expectedinhybrid-implantcandidates.
performanceofthepatientsaccordingtothetypeofinner earapproach.
Methods
This is a retrospective multicenter study of patients who underwentimplantplacementinthelastfouryearsattwo specializedcareinstitutionsinLatinAmerica;bothcenters employedthe samesurgical techniqueandusedthesame hearingpreservation electrode designedto beatraumatic (MED-ELFLEXTMEAS).10
The surgicaltechniqueusedwassimilarinallpatients, andhasbeendescribedinapreviouspublication.10
The general characteristics (age, gender, medical his-tory)andaudiologicaldata(etiologyofdeafness,duration ofdeafness,sequentialaudiometricandspeechtests, pre-andpostoperativeprocedures)ofpatientswereanalyzed.
Inclusionandexclusioncriteria
Inclusioncriteriawere:
--- Bilateralsensorineuralhearinglosswithlittleorno ben-efitwithPersonalSoundAmplificationDevices(PSADs). --- Puretonethresholdsbetterthan65dBatfrequenciesof
125,250and500Hz,andworsethan80dBatfrequencies above1000Hz(Fig.1).
--- Auditorydiscriminationwithmonosyllablesbelow40%in thebestpossiblesoundamplificationcondition.
--- Ahearingloss,stableforatleastthelasttwoyears.
Thosepatientswhodidnotmeetthecriteriaabovewere excludedfromthestudy.
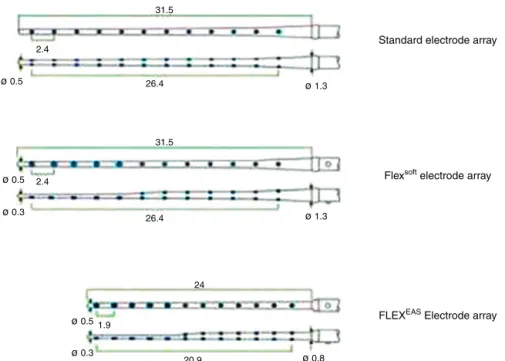
Implantused
TheimplantusedinallcaseswastheMED-ELFLEXTM EAS,
withfullinsertionoftheelectrodebundleinallcases. MED-ELFLEXTMEASelectrodehas24mmofoveralllength,
with0.8mmofdiameteratitsbaseand0.3mmatitsapex, witha 0.5-mm length tip. This device is provided witha
cochlearcoverageofabout1½ turn(Fig.2),giving
approx-imately21mmofintracochlearstimulationlength.
All patients used SonataTM, an internal component,
adapted witha Maestro SystemTM software. Patientswho
received postoperative electroacoustic stimulation used Duet2TM,aspeechprocessor.The groupwithpurely
elec-trical stimulationin the postoperativediffered onlyin its speechprocessor;insuchcases,OPUS2TMwasused.
Surgicaltreatmentofinnerear
Atfirst,theintroductionofanelectrodethroughtheround windowwastriedinallpatients,butinthosewhose expo-sure oftheroundwindownichewaspoor,a cochleostomy wasperformed for theinsertionof theelectrode.Ineach case, all steps proposed for hearing preservation were followed.10
It is noteworthy that, in cases where the exposure of the round window niche was not adequate via a poste-riortympanotomy,acochleostomywaschosen,withoutany instrumentationofthecochlearorroundwindowregion.
Hearingpreservation
To determine the patients’ residual hearing, audiometric testswithoutelectricalstimulationwereperformedas fol-lows:onthedateofactivationonemonthpostoperatively; at3monthspostactivation;at6monthspostactivation;and subsequently at every six months throughfollow-up. Pre-operativetestsuptotwoyearsbeforethetreatmentwere also entered into thedata set. Before the procedure the testswerealsorepeatedontheday ofsurgery.For statis-tical analysis,the most recent preoperative examinations (onthe date of surgery),aswell asthe latest postopera-tiveassessmentregisteredinthesepatients’medicalcharts, wereused.
Theprotocol included pure toneaudiometryfieldtests withtheimplantonandspeechtests,withstandardization accordingtotherulesoftheinstitution.
‘‘Residual hearing preservation’’ was defined in three ways:
• Totalhearingpreservation:0---10dBofhearingloss post-operatively,
• Partial hearing preservation: >10dB of hearing loss postoperatively, while maintaining audiometric indices ≤80dB,atleastatfrequenciesbetween250and1000Hz, • Nohearingpreservation:nobenefitwiththeuseofanEAS, bypresentingapostoperativethresholdwithoutelectrical stimulation>80dB.
Ethicalaspects
This study wasapprovedby thelocalEthics andResearch Committee.
Results
31.5
26.4
ø 0.5
ø 0.5
ø 0.5
ø 0.3
ø 0.3
ø 1.3
ø 1.3
ø 0.8 31.5
26.4 2.4
1.9
24
20.9
2.4 Standard electrode array
Flexsoft electrode array
FLEXEAS Electrode array
Figure2 SchematicrepresentationofMED-ELFLEXTMEAS(21mm)electrode.Standardelectrodearray.
Institution 2. Nine patients were female, and ten male ranging in age from 19 to 70 years, with an average of 48 years. All surgeries were uneventful and without complications.
Regardingtheetiologyofdeafnessinthesepatients,the following distributionwasfound: idiopathicetiology in 11 cases(57.8%),geneticetiology in3cases(15.7%; homozy-gous GJB2), and otosclerosis in two cases (10.5%). In the remaining participants, deafness was caused by trauma, neonatalhypoxiaandchronicotitismedia.
Themeantimeforthelastpostoperativeaudiometrywas 23.6monthsaftercompletionofcochlearimplantsurgery, rangingfrom4.5to81months.
Of the19 patients whounderwentimplant placement, in 16,theelectrode insertionoccurred throughtheround window,andinthreecasesbycochleostomybecauseof dif-ficultyin gettingadequate exposureof the roundwindow niche.Itisnoteworthythat,ofthethreecasesinwhichthe insertionoccurredthroughacochleostomy,deafnesshada geneticbasisintwocases,andthethirdcasehadan idio-pathicetiology.
Fivepatients hadcomplete hearingpreservation; in 12 patientspreservationwaspartial.Intwopatients,therewas nohearingpreservation(Fig.3).Ofthethreepatientswho underwentcochleostomy,therewasnohearingpreservation intwocases,withpartialhearingpreservationinthethird case(Fig.4).
Inallpatients,theaveragetonalresultsof500Hz,1kHz, 2kHz,and3kHzwiththeactivatedimplantwerehigherthan thepreoperativeaudiometryresults(p<0.001)(Fig.5).The Kolmogorov---Smirnovtestwasperformedpriortodata anal-ysistoverifythedatadistribution.Sinceourdatashowedan approximatelynormaldistribution,apairedttestwasused totestthedifferencebetweenrangesofindividualtestsfor theentiregroup.
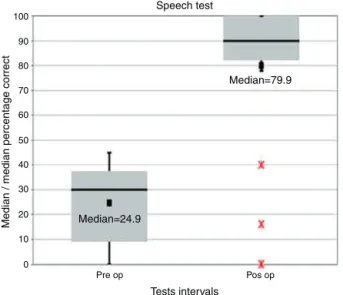
With respecttospeechperception testsin silence,we noted benefit for patients from their cochlear implants
5 2
12
Total
Partial
Absent
Preservation hearing
Figure3 Distributionofpatientsaccordingtopostoperative residualhearingpreservation.
(Figs.6and7).Asthespeechperceptiontests’distribution wasnot normal, the Wilcoxon Signed Rank test was used totestthe differencebetween rangesof individualtests. Theresultsshowedasignificantimprovementinspeechtest
3
1
2 16
Route of insertion of the electrode
Round window
Cochleostomy
Without preservation
Partial preservation
120
110
100
90
80
70
60
50
40
30
20
10
0
Average of tone thresholds
Hear
ing le
ve
l in dB
Pre op
Test intervals
Pos op test without implants
Pos op test using the implant EAS
Figure5 Averagepuretoneaudiometricthresholds(500Hz, 1kHz,2kHz,3kHz):comparisonamongpreoperativetests,last postoperativetestwithoutuseofahearingaid,andlasttest usingtheimplant(EAS)(hearinglevelindB)(n=19).Mean val-uesare shown as vertical black lines, medians as horizontal lines.Redasteriskrepresentsoutliers.
100
90
80
70
60
50
40
30
20
10
0
Speech test
Median / median percentage correct
Median=79.9
Median=24.9
Pre op Pos op
Tests intervals
Figure6 Resultsofthespeechtest:comparisonbetween pre-operativeversus postoperativetests (as apercentage). Mean valuesareshownasblackparcels,mediansashorizontallines. Redasteriskrepresentsoutliers.
100 90 80 70 60 50 40 30 20 10 0
Individual results of speech tests
P
ercentage
Pre op Pos op
Figure 7 Individual results ofspeech tests: comparison of preoperativeversuspostoperativetests(asapercentage).
Table 1 Comparative table between scores of speech perception tests, with round window and cochleostomy approaches.
Roundwindow Cochleostomy
Pre-op Post-op Pre-op Post-op
Mean 25.38 83.19 20.00 62.67 Median 30.00 90.00 25.00 82.00 Standarddeviation 16.395 26.945 18.028 40.612
performancefortheentiregroupbetweenpreoperative ver-suspostoperativetests(p<0.001).
Stratifiedanalysesaccordingtotheinnerear approach
Forstratifiedanalyses,thenonparametricWilcoxontestwas used.Individualstreatedwiththeroundwindowapproach achievedasignificantimprovementinpostoperativehearing thresholdswiththeEASimplantactivated(p<0.001).
The improvement of postoperative pure tone thresh-olds in the group of patients with inner ear approach by cochleostomy was not significant (p=0.109) withthe EAS implantactivated.Itisnoteworthythatthisgroupis numer-icallyverysmall(n=3),whichmaybeabias(Fig.8).
Thereisasignificantdifferencebetweengroupsin
individualtestintervals
To check if there is a difference between the two inner earapproaches (roundwindowversus cochleostomy) with respect toindividual test intervals, Mann---Whitney Utest wasused.Thus,betweenthetwoinnerearapproachesno significantdifferencewasfoundinpreoperative(p=0.866) and postoperative (EAS) (p=0.823) tests;however, a ten-dencytoasignificantdifferenceinpostoperativetestwith theimplantactivated(p=0.073)wasobserved(Table1).
Regarding speech test results between the two inner earapproaches,participantstreatedwitharoundwindow approachachieved significant improvement in the perfor-mance of their speech tests between preoperative and postoperativetests(p=0.001).Whencomparing preopera-tiveversuspostoperativetests,theimprovementforthose patients treatedwithcochleostomyapproachwasnot sig-nificant(p=0.109).
To determine if there was a differencein speechtest performancesbetweentheapproachesusedwithrespectto individualtestintervals,Mann---WhitneyUtestwasutilized. Individuals treated by round window approach achieved higherperformancescoresonpreoperative and postopera-tive speech tests, but the difference was not significant (preoperativetest:p=0.499;postoperativetest:p=0.206).
Discussion
120
110
100
90
80 70
60
50 40
30
20
10
0
Average of tone thresholds
Round window Cochleostomy
Hear
ing le
vel in dB
Pre op Pre op
Test intervals
Pos op test without implants
Pos op test using the implant EAS Pos op test
without implants
Pos op test using the implant EAS
Figure8 Averagepuretonehearingthreshold(500Hz,1kHz,2kHz,3kHz):thegraphshowsthecomparisonbetweenpreoperative versuspostoperativetests,withnouseofthecochlearimplant(hearinglevelindB).Theanalysiswasstratifiedbyinnerearapproach (Roundwindow---n=16;Cochleostomy---n=3).Meanvaluesareshownasverticalblacklines,mediansashorizontallines.Redasterisk representsoutliers.
stimulation by performing a cochlear implant. Although therearestillcontroversiesabouttherealbenefitsofthis combinedstimulation,severalbenefitsresultingfrom com-bined stimulationaredescribed for patients withresidual hearingandwhose hearingwaspreserved, suchasagood speechdiscrimination,11,12betterspeechperceptioninnoisy
environments,12,13 improved music appreciation,14,15 and a
betterdiscriminationofdifferentsoundfrequencies.16
Someclassificationsfor hearingpreservationhavebeen proposed toassess the degree of preservation of residual hearing, and the most commonly employed is that pro-posedby Skarzynski,17 which wasusedin thisstudy.Many
factors are related tohearing preservation, for instance, the surgeon’s experience, the electrode chosen,18 the
speed of electrode insertion,19 the use of preoperative
corticosteroids20 and the technique used. However,some
stepsinsurgical techniqueseemtomakenodifferencein therateofhearingpreservation,21but,thereisstill
contro-versy withrespecttodifferentroutes for insertionof the electrodeintothecochlea.8,22
Generally, hearing preservation occurs in 70---100% of implant technique patients.23 Only two of those patients
who underwent implant placement lost all hearing; our overall hearing preservation rate was 89.4%. Only three of our patients underwent implant placement through a cochleostomy, because of difficulty to expose the round window; 66.7% of these patients did not realize hearing preservation,whereasinallcasesofinsertionthroughthe round window the patients obtained complete or partial hearingpreservation.
This was the first study assessing the hearing preser-vation of patients that underwent implant placement at theinstitutionsoftheauthors.Webelievethat,withmore experience with this surgical technique, we will be able to report higher rates of preservation of residual hear-ing.Amore comprehensivemonitoring andother typesof speech tests are essential for a better evaluation of the results.
The improvement in postoperative pure tone thresh-oldsinsubjectstreatedwiththecochleostomyapproachto the inner earwas not significant (p=0.109) withan EAS-activatedimplant.Thisgrouphadasmallnumber(n=3)of patients,andthiscouldrepresentabias(Fig.8).
In all 19 operated patients, independent of hearing preservation, the pure tone thresholds with an activated implantimprovedsignificantly;therefore,allpatientshave benefited from cochlear implants. A recent study involv-ingpatientswithresidualhearingwhounderwentimplant placement also showed that all patients obtained better hearingoutcomesandqualityoflife.24,25
This study has some bias, especially because of its methodological(retrospective)design.Wealsoshould men-tion a selection bias, since the cochleostomy group was formedasaresultofanimpossibilityofaccessingtheinner earthroughtheroundwindow.Thus,anasymmetrybetween thegroupsresulted,whichcouldcompromisetheanalysis.
Despitethelimitationsdescribed,weconsiderthe num-berof participants in thestudy assubstantial,since they represent the largest number of cases in Latin America with the longest follow-up of these select patients. The reportingof theseresults will helps us achieve a greater understandingand comprehensionof hearing preservation incochlear-implantedpatients.
Conclusion
Thehearingpreservationrateinpatientswithresidual hear-ingsubmittedtoacochlear implantofMED-ELFLEXTM EAS
was89.4%(27% of overallpreservation and 63%of partial preservation),withatendencytoabetterpreservationwith theinsertionoftheelectrodethroughtheroundwindow.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
We thank all the patients and their families,the Unicom cochlearimplantgroup(audiologists,socialworkers,nurse staff, psychologists, speech therapists and all staff), our Department(ENT,HeadandNeckSurgeryDepartment),and everyoneatMED-ELteamwhohelpedus.
References
1.GantzBJ,HansenMR,TurnerCW,OlesonJJ,ReissLA,Parkinson AJ. Hybrid 10clinical trial: preliminary results. Audiol Neu-rootol.2009;14:32---8.
2.Lenarz T, Stover T, Buechner A, Lesinski-Schiedat A, Patrick J, Pesch J. Hearing conservation surgery using the Hybrid-L electrode.Results from thefirst clinicaltrialattheMedical UniversityofHannover.AudiolNeurootol.2009;14:22---31.
3.Skarzynski H, Lorens A, Piotrowska A, Podskarbi-Fayette R. Resultsofpartialdeafnesscochlearimplantationusingvarious electrodedesigns.AudiolNeurootol.2009;14:39---45.
4.GstoettnerW,HelbigS,SettevendemieC,BaumannU, Wagen-blast J, Arnoldner C. A new electrode for residual hearing preservationincochlearimplantation:firstclinicalresults.Acta Otolaryngol.2009;129:372.
5.Gstoettner W, Kiefer J, Baumgartner WD, Pok S, Peters S, Adunka O.Hearing preservationin cochlearimplantation for electric acoustic stimulation. Acta Otolaryngol. 2004;124: 348---52.
6.LehnhardtE.Intracochlearplacementofcochlearimplant elec-trodesinsoftsurgerytechnique.HNO.1993;41:356---9.
7.Mowry SE,Woodson E, Gantz BJ. New frontiers in cochlear implantation:acousticpluselectrichearing,hearing preserva-tion,andmore.OtolaryngolClinNorthAm.2012;45:187---203.
8.HavenithS,Lammers MJ,TangeRA,TrabalziniF,dellaVolpe A, van derHeijden GJ, et al. Hearing preservation surgery: cochleostomyorroundwindowapproach?Asystematicreview. OtolNeurotol.2013;34:667---74.
9.BriggsRJ,TykocinskiM,XuJ,RisiF,SvehlaM,CowanR,etal. Comparison of round window and cochleostomy approaches withaprototypehearingpreservationelectrode.Audiol Neu-rootol.2006;11:42---8.
10.CarvalhoGM,ValenteJP,DuarteAS,MuranakaEB,Guimarães AC,SokiMN,etal.Electroacousticstimulationoftheauditory system:UNICAMP’ssurgicalapproach.BrazJOtorhinolaryngol. 2012;78:43---50.
11.KieferJ,GstoettnerW,BaumgartnerW,PokSM,TilleinJ,Ye Q, et al. Conservation oflow-frequency hearing incochlear implantation.ActaOtolaryngol.2004;124:272---80.
12.Gstoettner WK, van de Heyning P, O’Connor AF, Morera C, SainzM,VermeireK,etal.Electricacousticstimulationofthe auditorysystem:resultsofa multi-centreinvestigation.Acta Otolaryngol.2008;128:968---75.
13.GantzBJ,HansenMR,TurnerCW,OlesonJJ,ReissLA, Parkin-sonAJ.Hybrid10clinicaltrial.AudiolNeurootol.2009;14Suppl 1:32---8.
14.GfellerKE, OlszewskiC,Turner C,Gantz B, OlesonJ. Music perceptionwithcochlearimplantsandresidualhearing.Audiol Neurootol.2006;11Suppl1:12---5.
15.GfellerKE, OlszewskiC,Turner C,GantzB, OlesonJ. Accu-racy of cochlear implant recipients on pitch perception, melodyrecognition,andspeechreceptioninnoise.EarHear. 2007;28:412---23.
16.ReissLAJ,GantzBJ,TurnerCW.Cochlearimplantspeech pro-cessorfrequencyallocationsmay influencepitchperception. OtolNeurotol.2008;29:160---7.
17.SkarzynskiH,SkarzynskiP.Aclassificationforhearing preser-vationincochlearimplantationYTheWarsawexperience.In: Paperpresentedat:HEARINGgroupMeeting.2011.
18.Nguyen Y, Mosnier I, Borel S, Ambert-Dahan E,Bouccara D, Bozorg-Grayeli A, et al. Evolution of electrode array diam-eter for hearing preservationin cochlearimplantation. Acta Otolaryngol.2013;133:116---22.
19.Rajan GP, Kontorinis G, Kuthubutheen J. The effects of insertionspeedoninnerearfunctionduringcochlear implan-tation: a comparison study. Audiol Neurootol. 2013;18: 17---22.
20.Rajan GP, Kuthubutheen J, Hedne N, Krishnaswamy J. The roleofpreoperative, intratympanicglucocorticoids for hear-ingpreservationincochlearimplantation:aprospectiveclinical study.Laryngoscope.2012;122:190---5.
21.PostelmansJT,StokroosRJ,vanSpronsenE,GrolmanW,Tange RA,MaréMJ,etal.Comparisonoftwocochlearimplantation techniques and theireffects on thepreservation ofresidual hearing.Isthesurgicalapproachofanyimportance?EurArch Otorhinolaryngol.2013[Epubaheadofprint].
22.Kang BJ, Kim AH. Comparison of cochlear implant perfor-mance after round window electrode insertion compared with traditional cochleostomy. Otolaryngol Head Neck Surg. 2013;148:822---6.
23.Incerti PV, Ching TY, Cowan R. A systematic review of electric-acoustic stimulation: device fitting ranges, out-comes,andclinicalfittingpractices.TrendsAmplif.2013;17: 3---26.
24.SantaMariaPL,Domville-LewisC,SucherCM,Chester-Browne R,AtlasMD.Hearingpreservationsurgeryforcochlear implan-tation---hearingandqualityoflifeafter2years.OtolNeurotol. 2013;34:526---31.
25.CarvalhoGM,GuimarãesAC,DuarteASM,MuranakaEB,Soki MN, Martins RSZ, et al. Hearing preservation after cochlear implantation: UNICAMP outcomes. Int J Otolaryngol. 2013,