RBCCV 44205-1496 DOI: 10.5935/1678-9741.20130074
Myocardial protection with prophylactic oral
metoprolol during coronary artery bypass grafting
surgery: evaluation by troponin I
Proteção cardíaca com uso proilático de betabloqueador oral em cirurgia de revascularização miocárdica:
avaliação pela troponina I
João Manoel Rossi Neto
1, MD, PhD; Carlos Gun
1, MD, PhD; Rui Fernando Ramos
1, MD, PhD;
Antonio Flavio Sanchez de Almeida
1, MD, PhD; Mario Issa
1, MD, PhD; Vivian Lener Amato
1,
MD, PhD; Jarbas J. Dinkhuysen
1, MD, PhD; Leopoldo Soares Piegas
1, MD, PhD
1Instituto Dante Pazzanese de Cardiologia (IDPC), São Paulo, SP, Brazil.
Work carried out at Instituto Dante Pazzanese de Cardiologia (IDPC), São Paulo, SP, Brazil.
No inancial support.
Correspondence address: João Manoel Rossi Neto
Instituto Dante Pazzanese de Cardiologia Ambulatório novo-Setor de Disfunção Ventricular
Av. Dante Pazzanese, 500 – Vila Mariana – São Paulo, SP, Brazil – Zip code: 04012-180
E-mail: [email protected]
Article received on March 4th, 2013 Article accepted on July 10th,2013
Abstract
Introduction: Biochemical markers of myocardial injury are frequently altered after cardiac surgery. So far there is no evi-dence whether oral beta-blockers may reduce myocardial inju-ry after coronainju-ry arteinju-ry bypass grafting.
Objective: To determine if oral administration of prophylactic metoprolol reduces the release of cardiac troponin I in isolated cor-onary artery bypass grafting, not complicated by new Q waves.
Methods: A prospective randomized study, including 68 patients, divided in 2 groups: Group A (n=33, control) and B (n=35, beta-blockers). In group B, metoprolol tartrate was ad-ministered 200 mg/day. The myocardial injury was assessed by troponin I with 1 hour and 12 hours after coronary artery by-pass grafting.
Results: No signiicant difference between groups regarding
pre-surgical, surgical, complication in intensive care (15% ver -sus 14%, P=0.92) and the total number of hospital events (21%
versus 14%, P=0.45) was observed. The median value of tropo-nin I with 12 hours in the study population was 3.3 ng/ml and was lower in group B than in group A (2.5 ng/ml versus 3.7 ng/ ml, P<0,05). In the multivariate analysis, the variables that have
shown to be independent predictors of troponin I release after 12 hours were: no beta-blockers administration and number of vessels treated.
Conclusion: The results of this study in uncomplicated coro-nary artery bypass grafting, comparing the postoperative release of troponin I at 12 hours between the control group and who used oral prophylactic metoprolol for at least 72 hours, allow to con-clude that there was less myocardial injury in the betablocker group, giving some degree of myocardial protection.
Descriptors: Troponin I. Postoperative care. Adrenergic be-ta-antagonists.
Resumo
Introdução: Os marcadores bioquímicos de lesão miocárdi-ca estão frequentemente alterados após cirurgia miocárdi-cardíamiocárdi-ca. Até o momento não existem evidências de que o betabloqueador oral possa reduzir a lesão miocárdica após cirurgia de revasculari-zação miocárdica.
Objetivo: Determinar se a administração oral proilática de
cirur-to describethe plasma levels ofmarkers of myocardial ne-crosis(MMN) as troponins, releasedinCABGthatare not caused by infarction postoperatively and evaluatepossible myocardial protectionproceduresthat couldreduce theMI. It isplausible to expectthat the resultsof the protective effectsof beta-blockerscan beextrapolated toCABG. Therefore, the aim of this studyis to testthe hypothesis thatthe prophylactic use oforalmetoprolol tartratereducesMI, assessedby the release oftroponinI (TnI) in the irst 12hours of post-CABG alone and notcomplicatedby the presence ofnew Q waveson the electrocardiogram(EKG), conferring myocardial protection.
METHODS
This isa randomized, open-label andsingle center study. Inclusion criteria for the study were indication for CABG regardless of age orgender with signed informed consent term. Exclusion criteria for the study were: previous useof beta-blockers; contraindication tobeta-blockers; clinical signs ofsystolic heart failure, global ejection fractionless than50%; CABGassociated with other procedures(valve replacement oraneurysmectomy or endoaneurysmorrhaphy), presence of new Q waves onEKGduringthe periodof stay in theIntensive Care Unit(ICU) and presence of acute myocardial infarction less than 30days of evolution.
All patients underwent CABG with the same surgical technique(intermittent aortic clamping) anda graft of the left internalthoracic artery had to be implanted.
Themetoprolol tartrate (oral) was initiatedat least 72hours before surgery, in the target dose of 200 mg/day.
TnIconcentrations were determinedby immunometric method using the Immulite Analyser (DPC - Diagnostic ProductsCorporation-LosAngeles, USA). Three samples INTRODUCTION
An increase in troponin levels isobserved following car-diac surgery, indicatingmyocardial injury[1,2]. The values considered normalor expectedafter coronary artery bypass grafting (CABG) suffermultifactorialinluencessuch astype of surgery, duration of ischemiaandmyocardial protection, inlammatory response, reperfusion injury, excessive stretch-ing and contraction of the heart, atheromatous embolism, inadequate coronary perfusion andexcessive perioperative cardiac work.
Beta-blockers can be deined as pharmacologic agents that antagonize speciically, competitive and reversible the action of endogenousorexogenous catecholamine in beta-ad-renergic receptors. Particularly in the heart, beta-adrenergic stimulationleads to increasedheart rate andmyocardial con-tractility. Depending upon theselective abilityto antagonize the effectsof catecholaminesin certaintissuesat doses lower than those requiredin others, beta-blockersmay be classiied asselective and non-selective. Thebeta-1 selectiveblockers are considered cardioselective because the heart contains predominantlybeta-1 and less beta-2; since the bronchodila-tionis mediated bybeta-2 receptors, and this characteristic is dose-dependent and decreases or disappearswhen employing high doses.Possible deleterious effectsresulting from the use of beta-blockersthat could causemyocardial depressionand/ or worseningofexistinglung disease, however, are of concern for somecardiac surgeons.
The clinical beneits of beta-blocker therapyhave been provenin the treatmentof myocardial infarction, heart failure, protection of preoperativepatients withischemic heart disease andin the preventionof atrialibrillationpostoperatively[3,4]. From the clinical and research perspective, it is desirable Abbreviations, acronyms & symbols
CABG Coronary artery bypass grafting EKG Electrocardiogram ICU Intensive Care Unit
MMN Markers of myocardial necrosis TnI Troponin I
gia de revascularização miocárdica isolada não complicada por novas ondas Q.
Métodos: Estudo prospectivo, randomizado, incluindo 68 pacientes divididos em 2 grupos: Grupo A (n=33, controle) e B (n=35, betabloqueador). No grupo B, o tartarato de metoprolol foi administrado na dose de 200 mg/dia. A lesão miocárdica foi avaliada pela troponina I com 1 hora e 12 horas após a cirurgia de revascularização miocárdica.
Resultados: Não foi observada diferença signiicativa entre
os grupos quanto às variáveis pré-cirúrgicas, cirúrgicas,
inci-dência de complicações na terapia intensiva (15% versus 14%;
P=0,92) e o número total de eventos hospitalares (21% versus
14%; P=0,45). O valor da mediana da troponina I com 12 horas
na população estudada foi de 3,3 ng/ml e foi menor no grupo B do que no grupo A (2,5 ng/ml versus 3,7 ng/ml; P<0,05). Na análise multivariada, as variáveis que demonstraram serem preditoras independentes da liberação de troponina cardíaca I com 12 horas foram: não uso de betabloqueadores e número de vasos tratados.
Conclusão: Os resultados desta investigação na cirurgia de revascularização miocárdica isolada, não complicada, compa-rando a liberação pós-operatória de troponina cardíaca I com 12 horas entre os grupos controle e o que usou metoprolol oral
proilático por pelo menos 72 horas, permitem concluir que
houve menor lesão miocárdica no grupo betabloqueador, con-ferindo algum grau de proteção miocárdica.
of blood were collectedfor the determination ofTnI: inthe preoperative period, with one hour and 12 hour arrivalin the ICU. A programdeveloped by the authorsof theEuroSCORE wasusedfor the score calculationof each patient[5].
The intercurrences and complications (inotropes >24 hours, intubation >24 hours, temporarypacemaker, the ICU stayfor >24 hours,stroke, atrial ibrillation, and death) were registeredin the medical recordandtransferredtotheclinical formof the study.
Due to the dificulty of inding information on the variabili-ty of the difference between TnI between the two groups (with and without beta-blockers) initially several simulations were performed to estimate the sample size. After the completion of the study, the statistical difference (1.2) and standard deviation of the difference (1.7) were calculated, and it was observed a test power of 85%.
Results wereexpressed as meanandstandard erroror me-dian andquartilesfor quantitative variables, while qualitative variableswere expressed asrelative frequencies. Possible asso-ciationsbetween qualitative variableswere evaluated usingthe chi-square orFisher exact test. For comparisonof quantitative variablesbetween the controlandbeta-blocker groups was used t-testfor variableswith normal distributionand for those with-out normal distribution(with an hour ITnI, TnI12 hoursand number of vessels treated) theMann-Whitney test was applied. The Spearman correlationwas used to examinethe association betweenquantitative variablesand Tn Iof 12hours.
For the choice of the independent variables on the model of multivariate analysis, variables that had signiicant correlation were selected and by clinical judgment the ones that could also inluence the release of TnI 12 hours. For the selection of best model, which had a reduced number of variables the Akaike method was applied, that uses a generalized linear model of
gamma distribution (link function log). The gamma model was selected by presenting a better it in the residual analysis.
Resultswere considered statistically signiicant when P-valueswere less than0.05.
This studywasapproved by theEthicsResearch Commit-tee of our Institution(protocol number: 2089).
RESULTS
Initially 70patients were selected andafter recruitment, two caseswere not considered from the analysisbecause they hadnew Q waves onEKG12 hoursafter surgery.
Patients wereallocated for two groups, 33(48.5%) pa-tients in the control group, and the other35(51.5%) in the beta-blocker group. The dose in one patient was reduced to 100mg/daydue toasymptomatic heart rate lessthan 50 bpm. The clinical and surgicalcharacteristics of the groupsare describedin Tables 1,2 and 3.
Table 4 presentsthe resultsof the values ofTnIwith 1 hourand12 hoursof arrivalin the ICU between the control and beta-blockers. TnIvalueswere lowerin thebeta-blocker groupthan in thecontrol group.
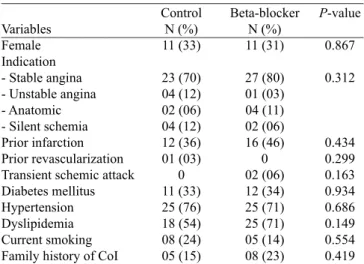
Table 1. Qualitative variables, comparison of the control and beta-blocker groups.
Variables Female Indication - Stable angina - Unstable angina - Anatomic - Silent schemia Prior infarction Prior revascularization Transient schemic attack Diabetes mellitus Hypertension Dyslipidemia Current smoking Family history of CoI
Control N (%) 11 (33) 23 (70) 04 (12) 02 (06) 04 (12) 12 (36) 01 (03) 0 11 (33) 25 (76) 18 (54) 08 (24) 05 (15) Beta-blocker N (%) 11 (31) 27 (80) 01 (03) 04 (11) 02 (06) 16 (46) 0 02 (06) 12 (34) 25 (71) 25 (71) 05 (14) 08 (23) P-value 0.867 0.312 0.434 0.299 0.163 0.934 0.686 0.149 0.554 0.419 N= number of patients; CoI= coronary insuficiency
Table 2. Quantitative variables, comparison of the control and beta-blocker groups.
Variables
Age (years) Weight (Kg) Height (m) BMI (Kg/m2)
Risk index – EUROSCORE Ejection fraction
Pre-operative heart rate
Control Mean ± SE
59.0 ± 1.7 72.3 ± 3.0 1.63 ± 1.0 26.7 ± 0.8 02.1 ± 0.3 64.0 ± 1.0 73.8 ± 1.7
Beta-blocker Mean ± SE
57.9 ± 1.4 74.8 ± 2.4 1.65 ± 1.0 27.1 ± 0.8 02.0 ± 0.3 66.3 ± 1.1 68.0 ± 1.7
P-value 0.619 0.519 0.330 0.740 0.757 0.153 0.021
SE= standard error; BMI= body mass index
Table 3. Surgical characteristics in the control and beta-blocker groups.
Variables
Perfusion time (minutes) Cross clamp time (minutes) ICU stay (hours)
Number of grafts performed
Control group Mean ± SE
86.8 ± 5.2 60.3 ± 3.0 45.4 ± 1.4 3.0 (2.0-3.0)
Beta-blocker group Mean ± SE
84.1 ± 5.1 57.0 ± 3.6 54.3 ± 6.2 3.0 (2.0-3.0) P-value 0.705 0.477 0.181 0.215
Table 4. Analysis of troponin I results (ng/ml) in both groups.
Troponin I
Pre-operative At 1 hour At 12 hours
However, this differencewas onlystatisticallysigniicantin the 12 hourspostoperativelydata (2.50versus3.70, P=0.048).
ThechangesofTnI were analyzed 12 hourspost-operative and their associationwith someclinical and surgical variables. In addition to thevariablegroup, univariate analysisshowed thatthe factorsto be correlated withthe release ofTnI 12 hourswereperfusion time, cross clamptimeand the number of grafts performed(Table 5). Althoughstatisticallysigniicant, this relationshipwas considered weakby analyzingthe values ofcorrelation (R).
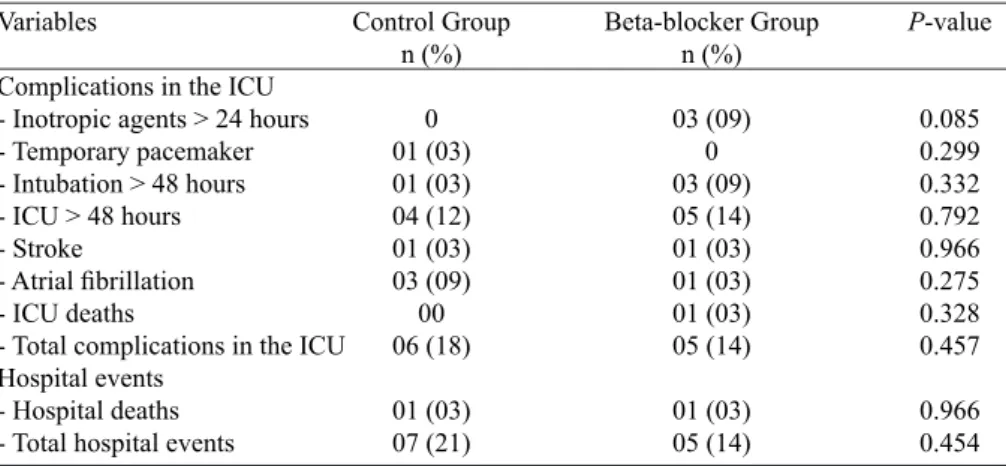
There was nosigniicant differencein relation to postoper-ativecomplicationsin the ICU andin-hospital events between groups(21% in the control groupversus14% in patients with beta-blocker, P=0.454) (Table 6).
In the inal modelof the multivariate analysis, the variables thathave shownto beindependent predictorsofTnIrelease after 12 hourswere: no beta-blockers administration and num-ber of grafts required. Table7 shows thepercentage increase and the results expected. No beta-blockers administration increases in22% the expected valueof troponin12 hours and for each graft required adds a33% increase.
DISCUSSION
The resultsof this studyprospectivelyevaluated 68 pa-tientsundergoing isolated CABGrevealedfor the irsttime in literature, a myocardial injuryreductioninthe group using oralbeta-blockerat a dose of200mg/day for at least72 hours preoperatively.
Some demographic characteristicsin the general popu-lationof the study shouldbe highlightedas the presence of womenin one third ofpatients, average agebelow 60years, morethan a thirdwith previous myocardial infarction, diabetes
Table 5. Correlation between troponin I at 12 hours of postoperative
and variables which could inluence its release.
Variable Weight Height
BMI (body mass index) Age
Ejection fraction Preoperative heart rate Perfusion time Cross clamp time
Number of grafts performed
Correlation (R) -0.10
0.02 -0.17 0.06 -0.10 0.11 0.30 0.30 0.36
P-value 0.379 0.886 0.160 0.622 0.557 0.466 0.016 0.011 0.003
Table 6. Comparison of complications in the intensive care unit and hospital events between the control and beta-blocker groups.
Variables
Complications in the ICU - Inotropic agents > 24 hours - Temporary pacemaker - Intubation > 48 hours - ICU > 48 hours - Stroke
- Atrial ibrillation
- ICU deaths
- Total complications in the ICU Hospital events
- Hospital deaths - Total hospital events
Control Group n (%)
0 01 (03) 01 (03) 04 (12) 01 (03) 03 (09) 00 06 (18)
01 (03) 07 (21)
Beta-blocker Group n (%)
03 (09) 0 03 (09) 05 (14) 01 (03) 01 (03) 01 (03) 05 (14)
01 (03) 05 (14)
P-value
0.085 0.299 0.332 0.792 0.966 0.275 0.328 0.457
0.966 0.454
n= number of patients; ICU= Intensive Care Unit
Table 7. Results of the multivariate analysis of troponin I release at 12 hours.
Control group
Number of grafts performed Hospital events
Perfusion time
Postoperative complications
Expected Percentage Increase
1.22 1.33 1.65 1.00 0.64
CI 95%
1.02-1.46 1.01-1.77 0.97-2.80 0.99-1.01 0.36-1.14
P-value
mellituswitha third, more than70% with hypertension, more than50% withdyslipidemiaand all withventricular function regarded as good. This populationwas consideredlow risk (mean EuroSCORE 2.0). Clinical characteristics were dis-tributedequallyin both groups, except forpreoperativeheart rate, which was lower in thebeta-blockergroup(73.8 versus 68.2, P=0.035).
Themyocardial injuryis associatedwithcardiac surgery and can be causedby differentmechanisms, including: direct traumabysuturingandmanipulation of the heart; regional or globalischemiaby inadequate cardiac protection, coronary dis-section, microvascular eventsrelatedto reperfusionor failure toperform thegrafts[6].Moreover, nobiological markeris able to distinguishthe injurycausedbyinfarctionthatoccurs in small quantities in myocardial cells, which usually are associated with theprocedure itself[6].However, the higher the value for acardiacbiochemical markerafter the procedure, the greater the myocardial injury, regardless of the mechanism of injury.Despite the dificultiesin interpreting thetroponin levelafter aCABG, it is known that the higherthis value, the worse the prognosis[7,8].
In this study, patients who usedbeta-blockershad a signii-cant reductionin the levels ofcTnI(2.50ng/mlversus3.70ng/ ml, P=0.048), with a trendin the reductionofhospital events, despite notachievingstatistical signiicance(14% versus21%, P=0.454). It was also shown that the longer the perfusion time, the anoxic time, and the numberof grafts required, the higher levels of TnIat 12 hours postoperatively. However, in multivariate analysis, independent predictors of troponin releasewere the numberof grafts required and the fact of not using beta-blockers(control group).
The clinical signiicance of this minimum or expected TnI amounthas not yet beenelucidated. In thisstudy, despite thelower release in thebeta-blockergroup, there was no sig-niicant differencein relation toin-hospital events, probably because thestudy was not designedwith thisobjectiveand the sample sizewasinsuficient.
On the other hand, the main interestof this studywas to observethe behaviorchangesofTnIwith asingleprophylactic pharmacological intervention. Therefore, we excluded those who had aspeciicdiagnostic criteria for perioperative myo-cardial infarction (presence of new Q waves onpostoperative) known toelevate a lot the level of TnI. The useof asimple method of myocardial protection, as the use ofprophylactic oral metoprolol, combined with new advances in surgical techniques andpostoperative care, can further reduce the minimum expectedreleaseofmarkersof myocardial necrosis and thuspossiblyimprove prognosisinCABG.
The mechanismsof myocardial protectionof beta-blockers inCABGare not yetfully understood. Animal experiments suggestthat beta-blockade is cardioprotectiveduring reper-fusion, either by reduction ininfarct size, improvement of ventricular function, reduction in apoptosis or decrease of
myocardial edema[9,10]. The possiblemechanisms involved in thisprotectionincludereducing the releaseofoxygen free radicals and adhesionto endothelium nuclearpolymorphs (major source of inlammatory response) [11]. During cardiac surgerywithextracorporeal circulationthere isa signiicant increasein the levels ofcatecholamines, resulting in anacute desensitizationofbeta-adrenergic receptorsinduced by these agonists. It is a cause ofmyocardial depressionthat occurs after surgery [12]. Probablythe mechanismsof myocardial protectionwith the useof metoprololare related, in part, with reductions of some ischemic processor metabolic changes that occurafter surgery. There are no datain the literature to conirm whetherreduced levels ofTnIare the result ofminor traumastraight from the heartwith the useof beta-blockers, and what roleof this mechanisminmyocardial injuryandits clinical relevance.
Limitations of this study include being a single center, there is no standardization of the available tests for troponin, using intermittent clamping as surgical technique (and not be applied to other techniques) and cases of infarction without Q-wave in post-CABG are not identiied, since there is no deinition for diagnosis in clinical studies. This study used a low-risk population, and therefore with lower prevalence of hospital events, which may have contributed to no statistical differences between the groups. Finally, a larger sample of patients could extend the results obtained, but as the hospital morbidity and mortality are considered low in low-risk patients undergoing CABG surgery, multicenter clinical trials would be needed with a very large population to assess reduction of infarction postoperatively and hospital events with the use of prophylactic beta-blockers in addition to the impact of the minimum TnI changes in the possible risk factors and prognosis. There is a need to clarify whether changes of TnI in non-complicated patients with new Q waves on EKG have any clinical consequences after discharge, because this study was limited to in hospital follow up.
The clinical implications of this study allow us to assure that there is some degree of myocardial injuryeven in un-complicated patients and it becomes mandatory, therefore to deine which the minimum reference value of cTnI is after CABG and correlate the values with prognosis. The reduction of TnI in the beta-blocker group in this study may help to understand the beneits of this medication, since it is known that the higher the levels of troponin, the worse the prognosis of patients, regardless of the pathophysiological mechanisms involved [8,13].
CONCLUSION
Author’s roles & responsibilities
JMRN Protocol design, data collection, discussion of results and manuscript writing
CG Discussion of results RFR Discussion of results
AFSA Surgical procedures and discussion of results MI Surgical procedures and discussion of results VLA Data collection and discussion of results JJD Discussion of results
LSP Protocol design, discussion of results and manuscript writing
REFERENCES
1. Leal JCF, Braile DM, Godoy MF, Purini Neto J, Paula Neto A, Ramin SL, et al. Early evaluation of cardiac troponin I in patients submitted to myocardial revascularization. Rev Bras Cir Cardiovasc. 1999;14(3):247-53.
2. Califf RM, Abdelmeguid AE, Kuntz RE, Popma JJ, Davidson CJ, Cohen EA, et al. Myonecrosis after revascularization procedures. J Am Coll Cardiol. 1998;31(2):241-51.
3. Ong HT. Beta blockers in hypertension and cardiovascular disease. BMJ. 2007;334(7600):946-9.
4. Kaw R, Hernandez AV, Masood I, Gillinov AM, Saliba W, Blackstone EH. Short- and long-term mortality associated with
new-onset atrial ibrillation after coronary artery bypass grafting:
a systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2011;141(5):1305-12.
for at least 72 hours, allow us to conclude that there was less myocardial injury in the beta-blocker group, conferring myocardial protection.
5. Roques F, Michel P, Goldstone AR, Nashef SA. The logistic EuroSCORE. Eur Heart J. 2003;24(9):881-2.
6. Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et al. Third universal definition of myocardial infarction. J Am Coll Cardiol. 2012;60(16):1581-98.
7. Lurati Buse GA, Koller MT, Grapow M, Bolliger D, Seeberger M, Filipovic M. The prognostic value of troponin release after adult cardiac surgery: a meta-analysis. Eur J Cardiothorac Surg. 2010;37(2):399-406.
8. Domanski MJ, Mahaffey K, Hasselblad V, Brener SJ, Smith PK, Hillis G, et al. Association of myocardial enzyme elevation and survival following coronary artery bypass graft surgery. JAMA. 2011;305(6):585-91.
9. Usta E, Mustai M, Straub A, Ziemer G. The nonselective
beta-blocker carvedilol suppresses apoptosis in human cardiac tissue: a pilot study. Heart Surg Forum. 2010;13(4):E218-22.
10. Fannelop T, Dahle GO, Matre K, Moen CA, Mongstad A, Eliassen F, et al. Esmolol before 80 min of cardiac arrest with oxygenated cold blood cardioplegia alleviates systolic dysfunction. An experimental study in pigs. Eur J Cardiothorac Surg. 2008;33(1):9-17.
11. Geissler HJ. Reduction of myocardial reperfusion injury by high-dose beta-blockade with esmolol. Thorac Cardiovasc Surg. 2002;50(6):367-72.
12. Booth JV, Landolfo KP, Chesnut LC, Bennett-Guerrero E, Gerhardt MA, Atwell DM, et al. Acute depression of myocardial beta-adrenergic receptor signaling during cardiopulmonary bypass: impairment of the adenylyl cyclase moiety. Duke Heart Center Perioperative Desensitization Group. Anesthesiology. 1998;89(3):602-11.