TITLE PAGE
The immediate effects of acupuncture on the mechanosensitivity of the median nerve: an exploratory randomised trial
Nuno Moraisa, Henry Gretenb,c, Maria João Santosb, Jorge Machadob aPolytechnic Institute of Leiria, School of Health Sciences (ESSLei – IPL), Department of Health Technologies, Campus 2 – Morro Do Lena – Alto Do Vieiro, 2411-901 Leiria, Portugal
bUniversity of Porto, Instituto de Ciências Biomédicas Abel Salazar (ICBAS-UP), Rua de Jorge Viterbo Ferreira, 228, 4050-313, Porto, Portugal
cHeidelberg School of Traditional Chinese Medicine, Karlsruher Str. 12, 69126 Heidelberg, Germany
KEYWORDS: pain threshold; pain tolerance, peripheral nerves; upper limb neurodynamic test 1
Word count, excluding title page, references, figures and tables: 3324
Corresponding author: Nuno Morais
Rua Engenheiro Duarte Pacheco, 19C, Fração AC 3850-040 Albergaria-a-Velha, Portugal
Telephone: (+351) 919 528 026 Email: [email protected]
ABSTRACT
Introduction: Acupuncture appears to reduce the mechanosensitivity of peripheral nerves in animal models; yet, this possibility has not been demonstrated in humans. The main purpose of this exploratory trial was to evaluate the immediate effects of acupuncture on the mechanosensitivity of the median nerve, measured by the elbow extension range-of-motion (EE–ROM) at pain onset and maximum tolerance during the upper limb neurodynamic test 1 (ULNT1). Additional purposes were to test the effects of two different points in ULNT1 responses and critically appraise pre-/post-intervention changes for conducting future research.
Methods: Thirty-one asymptomatic individuals randomly assigned to group PC (n=14) or LU (n=17) by coin flip procedure, underwent acupuncture (leopard spot needling) in PC5 or LU5’’, respectively. Two mixed-model analysis of variance (ANOVA) with time (pre-intervention vs post-intervention) as the within-subject factor and group (PC vs LU) as the between-subject factor, plus time group interaction, were used to determine the effects of acupuncture therapy on EE–ROM at pain onset and maximum tolerance during ULNT1. Results: At baseline measurements there were no differences between groups (p > 0.05). After acupuncture, mean EE–ROM increased 3.1º at pain onset (p=0.029, η2
p=0.154) and 5.6º at maximum tolerance (p=0.002, η2p=0.277) with
no differences between groups (p>0.05, η2
p<0.01).
Discussion and Conclusion: Immediately after acupuncture, the
mechanosensitivity of the median nerve appears to be reduced as observed by an increase in EE–ROM during the ULNT1. Further studies are necessary to confirm these preliminary findings.
INTRODUCTION
Mechanosensitivity of neural tissues is a normal protective mechanism that allows nerves to respond to potentially harmful mechanical stress levels, i.e. repetitive stress or elevated changes in tension, shear and/or compression imposed upon them during body movements and postures. Responses include a mixture of sensory experiences (e.g., pain, stretching, tingling, burning
sensations) and movement control strategies (e.g., reflex muscle contraction, increased resistance to movement, restriction in range of motion)1, 2.
With injury or pathology of the neural structures (neuropathy) or the surrounding tissues and nervous system sensitization, the mechanosensitivity of nerves may increase (gain of somatosensory function), resulting in an elevated painful response to mechanical stimuli, i.e. hypersensitivity, hyperalgesia and in more severe cases allodynia, movement guarding and avoidance behaviour2. While this is advantageous in acute conditions to protect the body from further injury, there is growing evidence showing that, in non-acute conditions, increased neural mechanosensitivity may be related with chronicity and exacerbation of pain and disability in several musculoskeletal disorders, e.g., non-specific arm pain syndrome3-5, non-specific neck3, 6 and low back7, 8 pain disorders, carpal tunnel syndrome4, 9, or knee10 or thumb11
osteoarthritis. Assessing the mechanosensitivity of neural structures is thus of considerable value for clinicians and researchers to assist them in the
differentiation of mechanisms responsible for pain generation and/or maintenance and in the selection/study of appropriate therapies3, 6-9, 12.
Acupuncture has been shown to reduce the mechanosensitivity of peripheral nerves and improve nerve-related functional impairments after an injury in the peripheral nervous system13-15. However, these effects have only been demonstrated in animal models. In human subjects, acupuncture has shown positive results in nerve function and symptoms, including pain, in studies conducted in people with peripheral neuropathy16-18; however, it is unclear whether the effects could be associated with changes in the neural mechanosensitivity as no specific tests were used to measure it. Some authors have used electrophysiological tests to evaluate the effects of acupuncture on peripheral nerves function16-21; yet, the usefulness of such measures (e.g., nerve conduction studies) to assess increased neural mechanosensitivity is of
questionable value as they evaluate the conductivity or degree of injury in large-diameter nerve fibres, responsible for loss of somatosensory function (e.g., hypoesthesia), whereas increased mechanosensitivity is related with increased excitability of the small-diameter afferents, nociceptors of the nervi nervorum, and central nervous system pathways4, 7, 22, 23.
Neurodynamic tests are part of the clinical examination of patients with suspected neuropathy. These tests aim to asses the mechanosensitivity of the nervous system24, consisting of using a series of body movements to apply mechanical forces to a portion of the nervous system in order to evaluate how sensitive or tolerant nerves are to mechanical stimuli3. Although the concepts of neural mechanosensitivity and neurodynamics have been widely employed in research and non-pharmacological interventions for pain management25, these have not been yet applied in acupuncture research.
The main purpose of this exploratory trial was to test the feasibility of using a new approach (assessment of mechanosensitivity of neural tissues) to evaluate the effects of acupuncture in clinical practice and research.
Specifically, we aimed to determine whether the mechanosensitivity of the median nerve of human subjects, assessed by applying mechanical forces to the nerve (upper limb neurodynamic test 1 or ULNT1), was altered immediately after acupuncture. Because acupuncture has not been previously used to modulate the mechanosensitivity the median nerve we also aimed to explore whether stimulation of different points located in the territory supplied by the median nerve could result in different responses to the ULNT1, and to evaluate if pre-/post-intervention changes are sufficiently relevant to recommend further studies on the effects of acupuncture on nerve-related pain.
METHODS
The research protocol was approved by the Ethics Committee of the Institute of Biomedical Sciences Abel Salazar of University of Porto (ICBAS– UP, project# 064/2014) and registered in ClinicalTrials.gov with the ID
NCT02150915. The study is reported according to the Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA)26.
Study Design
This was an exploratory trial conducted in a sample of asymptomatic individuals randomly assigned to either one of the following groups, both
receiving true acupuncture therapy: PC group or LU group. The design and flow diagram of recruitment, participation, allocation and reassessment (follow-up) of this study is shown in Figure 1.
Participants
Healthy volunteers from a scholar community were recruited to
participate in the study, following announcement and invitation held across the campus. The aims, procedures and eligibility criteria of the study were provided in the announcement. Inclusion criteria included being ≥ 18 years old and able to move all upper body quadrant joints in a normal range of motion without any pain or movement restriction. Participants were excluded if they presented musculoskeletal abnormalities in the upper body quadrant, any complaints in that region over the past 3 months, health conditions that could disrupt nerve function (e.g., diabetes), leg length discrepancy of more than 1.5 cm27, cognitive impairment, or no mechanosensitive response to the ULNT1. All participants were informed about their right to withdraw at any time during the study. A physiotherapist with 17 years of clinical experience ensured that the participants met the eligibility criteria. The research was conducted at the same place of the recruitment, from June to August 2014. Written informed consent was obtained from each participant before data collection and their rights protected. Sample size was based on the maximum number of participants we could test during the study period.
Main Outcome Measures
Elbow extension range of motion (EE–ROM) at pain onset and maximum tolerance during the ULNT1 was the main outcome measure. The ULNT1 is a provocative test to the mechanosensitivity of the brachial plexus/median nerve, consisting of a sequence of movements of the body segments that
progressively moves and tensions those neural structures through elongation of the nerve bed1, 28, 29. In high mechanosensitive neural tissues, as in patients with
nonspecific neck and arm pain or carpal tunnel syndrome, it is expected that a greater sensory and/or motor response (i.e., hypersensitivity, hyperalgesia, or more resistance to motion due to muscle spasm) occurs which stops the EE– ROM at an earlier phase during the test and/or determines its end1, 6, 9.
Asymptomatic individuals show similar responses during the application of the ULNT1 as a protective mechanism of the neural structures, although not as early or as sharply as in symptomatic individuals4, 6, 9, providing a preliminary research framework to test this new approach of studying acupuncture effects before progressing to clinical trials with patients with nerve-related pain. Instruments
To assess EE-ROM, a smartphone (iPhone 4, iOS 7.2, Apple Inc., Cupertino, CA) with built-in motion sensors (triaxial accelerometer,
electromechanical gyroscope and magnetometer) that measure the position and orientation of the device in the 3-dimensional space was used. Measurements were acquired with a native application of the iPhone 4 operating system, the Compass app, in compass vision mode. Using this hardware/software set, previous research estimated measurement errors (SEM and MDC95) of 6.6–6.8º and 18.4–18.8º in EE–ROM at pain onset, and 4.2–4.8º and 11.7–13.2º at maximum tolerance during the ULNT130. These values are comparable to those of other measuring instruments used to assess EE–ROM during the ULNT14. Selection of acupuncture points
Point selection was based on a systematic review of randomized
controlled trials aiming to evaluate the effects of acupuncture in people suffering from dysfunction of the median nerve 18 and on authors’ consensus according to their clinical, teaching and research backgrounds. Researchers have been using the stimulation of acupuncture points located distally in the ipsilateral upper limb (hand and wrist), according to the principles of traditional Chinese Medicine (TCM), to test symptoms change, including pain, in people with median nerve dysfunction18. The most frequently stimulated points are distal points located in the so-called “pericardium or PC meridian”18. Given the positive trends found in the aforementioned systematic review18, the research team assumed that puncture of distal PC points could be clinically relevant for
first testing the effects of acupuncture on the mechanosensitivity of the median nerve. Nevertheless, in injury-free subjects, pain sensations and protective muscle responses associated with the ULNT1 are located closer to the elbow than near the wrist 1, 31. It was then speculated that the potential effects of acupuncture in pain sensation and performance during the ULNT1 could be enhanced by using points more proximal to the location where most subjects are expected to experience pain and restricted motion. Additionally, with needling of distal PC acupuncture points there is a risk, although small, of damaging the median nerve32. An alternative is therefore clinically relevant. Taking all this into consideration, the authors first conducted a preliminary study in 3 subjects to evaluate the effects of stimulation of other points located in the territory that is supplied by the median nerve hoping to select those that could potentially modulate better the mechanosensitivity of the median nerve. Three classical points (LU 8, LU 10, TE 5) and 1 new extraordinary point (LU 5’’) were tested (crossover design). LU 5’’ was proposed by one of the authors (H.G.) and is located 2 cun distally to LU 5, in the direction of LU 6. Based on changes in the location and type of sensory responses and the resistance to elbow extension movement during the ULNT1 after stimulation, LU 5’’ unveiled the most promising effects (unpublished data).
Randomisation and group selection
After completing the ULNT1 at baseline (pre-intervention), subjects were referred to the room where acupuncture was being conducted. Subjects’
randomisation and assignment to either one of the two intervention groups were performed in this room through coin flip procedure. Each subject was asked to launch a euro coin in the air, catch it and show the upper face to the specialist in TCM recruited for the application of the acupuncture. This face defined group allocation: common face of euro currency assigned the participant to PC5 group (active comparator), whereas the other side allocated the participant to the LU5’’ group (experimental).
Sociodemographic information (age, gender), height and body mass were first collected to characterize the sample.
ULNT1: assessment protocol pre- and post-intervention
An experienced physiotherapist (17 years of practice) in musculoskeletal and neurodynamic examination performed the ULNT1 before (pre-) and after (post-) acupuncture. The examiner was aware of the aims and design of this study; however, he was blinded to the allocation of participants to intervention groups and the actual value of the EE–ROM between measurements, , since only the initial and final angular position values displayed by the smartphone were registered during the assessment. The EE–ROM was calculated later as the difference between the initial angular position and final angular position values, at pain onset and maximum tolerance. For the assessment, participants were asked to remain in the supine position close to the border of a massage table, with the lower limbs straight, the body aligned and the upper limbs in neutral position. The head and neck were stabilized in maximum comfortable contralateral side-flexion using a 5kg sand bag in order to magnify the pain sensation over other potential sensory responses occurring with ULNT1 (e.g., stretching)31. The smartphone was coupled to the participant’s forearm using an armband with an extended Velcro strip to tightly adjust the smartphone. Before each test, the examiner assessed the quality of smartphone coupling to ensure consistency of the measurements. All participants underwent a practice trial in the non-dominant side prior to the first measurement. With this procedure, participants could become familiar with the mechanosensations (i.e., pain or paraesthesia, stretching) that may occur during the ULNT1 and could identify the sensory responses they should report during the test – the onset of pain and the maximal tolerance. ‘Onset of pain’ was described as ‘the moment when the least experience of discomfort/pain was recognized’ whereas ‘maximum
tolerance’ was defined as ‘the greatest level of discomfort/pain which the subject was prepared to tolerate’33. The ULNT1 was then performed in the dominant limb with following sequence: (1) maximal contralateral cervical side-flexion; (2) arm at 90° of shoulder abduction preventing scapular elevation; (3) 90° of shoulder external rotation and 90º of elbow flexion (this position defined the 0º or starting position of testing range of motion); (4) maximal forearm
supination; (5) extension of the wrist and fingers; and (6) elbow extension. From (1) to (5), movements were performed without causing discomfort or
compensatory movements in the adjacent segments to minimise potential contamination of sensory responses arising from non-neural tissues (e.g., muscle, fascia, or joint).
Acupuncture: treatment protocol
For the application of the acupuncture technique, a specialist in TCM with 5 years of clinical practice and tutoring was recruited. This specialist had
information about the aims and design of the study, however, she was blinded to measurement outcomes. For the intervention, participants sat comfortably in a chair with their back supported and their dominant exposed for the
intervention. To puncture PC 5 or LU 5’’, conventional sterile disposable stainless-steel needles were used (BD Micro-Fine, 0.30mm [30G] 8mm). The applied technique was the so-called leopard spot needling therapy, also known as sparrow-pecking technique, consisting of 5 fast penetrations into the skin in about 3 seconds to a depth of 0.5 cm, restricted by the shape of needles. This technique is believed to produce analgesic effects and improve muscle function by increasing the blood flow to the site of needling34. After the intervention, the specialist in TCM applied cloth sterile adhesive tape (3cm x 3cm) in both
acupuncture points to blind the site of intervention. Subjects were then referred to the room where a new ULNT1 would be conducted (Figure 1).
Statistical analysis
Analyses were conducted using SPSS v22.0 (IBM Corp., Armonk, NY).
Baseline measurements were compared between groups using independent t-test (age, mass, height, body mass index and pre-intervention EE-ROM during ULNT1) and Fisher’s exact test (gender and hand dominance). Two mixed-model analysis of variance (ANOVA) with time (pre-intervention vs
post-intervention) as the within-subject factor and group (PC vs LU) as the between-subject factor, plus time group interaction, were used to determine the effects of acupuncture on EE–ROM at pain onset and maximum tolerance during the ULNT1. The assumptions for the application of the statistical tests were
and esfericity (Mauchly’s) of the data. A p < 0.05 was considered statistically significant. Effect sizes, using eta square partial (η2
p), complemented the
inferential statistics. Cut-off values for interpreting η2
p have been defined
elsewhere35. RESULTS Participants
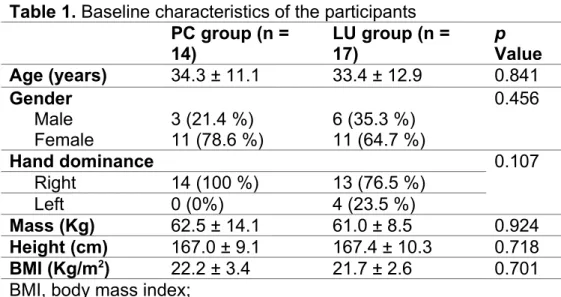
Thirty-two eligible individuals (n = 32) volunteered to participate in this research. One of the subjects, was excluded after the ULNT1 pre-intervention because no mechanosensitive response to the test was found (Figure 1), i.e., absence of pain/discomfort or sensation of stretching or paraesthesia in the anterior part of the forearm and first 3/4 fingers plus full range of elbow extension motion4. A total of 31 participants then composed the final sample size (PC5 group, n =14; L5’’ group, n =17). There were no statistical differences between groups at baseline measurements (Table 1), including EE-ROM at pre-intervention phase (pain onset, p = 0.615 and maximum tolerance, p = 0.483; mean and standard deviation values are provided in Table 2). Both assessment and intervention procedures were well accepted by the participants. No adverse effects of needling occurred except minor bleeding in 11 participants, which required no specific treatment.
Onset of Pain
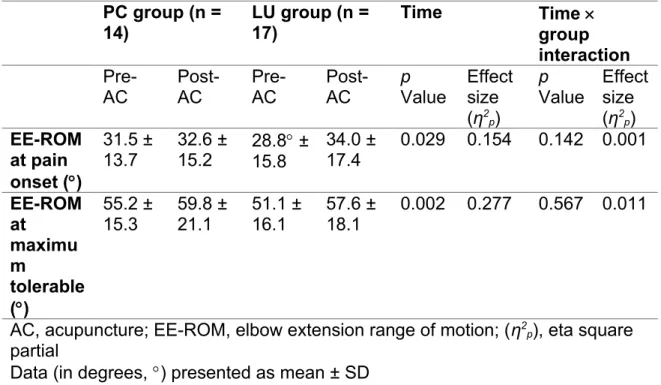
Within-subject factor analysis showed significant differences and a moderate effect size from pre- to post-intervention measurements (Table 2, factor time). The gain in EE–ROM after acupuncture was, on average, 3.1º (95% CI = 0.3º – 5.9º). No differences between groups were found and the effect size was negligible (p = 0.901, η2
p = 0.001). No time-by-group interaction
effect was found (Table 2).
Maximum tolerable pain
Significant differences were also found in pain tolerance from pre- to post-intervention (Table 2). The increment in EE–ROM was, on average, 5.6º (95%CI = 2.2º – 9.0º) after acupuncture, representing a large effect size of the
factor time (Table 2). No differences between groups were found and the magnitude of the effect size was negligible (p = 0.585, η2
p = 0.010). No
interaction effects were found (Table 2).
DISCUSSION
According to the authors’ knowledge, this was the first study evaluating the effects of acupuncture on the mechanosensitivity of peripheral nerves in human subjects. Using a new approach in acupuncture research, based on the concepts of mechanosensitivity of neural tissues and neurodynamics, it was found that immediately after its application, acupuncture may slightly reduce the mechanosensitivity of the median nerve as observed by a small increase in the EE–ROM during the ULNT1, particularly when considering the maximum tolerable pain. Although preliminary, our findings support pre-clinical research suggesting that acupuncture may be a feasible non-pharmacological
therapeutic modality in a wide range of disorders where nerve-related pain and increased sensitivity to mechanical stimuli is an important clinical feature13-15, 36.
This study found an average gain of 3.1º and 5.6º in EE–ROM,
respectively, at pain onset and maximum tolerance, respectively, from baseline to post-acupuncture ULNT1 measurements (within-subject factor analysis). Despite these interesting results, which encourages further studies on this topic, the relevance of such change is still difficult to establish. Acupuncture has shown a moderate to large effect size in EE-ROM (Table 2, factor time), meaning that the magnitude of the differences pre-post acupuncture was relatively important. Despite that, 3.1º is lower than the SEM previously
estimated for the condition ‘onset of pain’ (~7º) using a similar instrumental set-up in neurodynamic assessment30. This means that the observed change in EE-ROM might be due to measurement error. At ‘maximum tolerable pain’, the mean change in EE–ROM was higher than the estimated SEM for this condition (~4º)30. Nevertheless, the SEM was still within the 95%CI of the mean
differences (2.2º – 9.0º) pre-post acupuncture, precluding us from drawing further conclusions. A statistical change of 7.5º in EE-ROM has been suggested as meaningful in detecting improvements in patients’ performance in the ULNT1 5, 33. However, it is not evident whether this threshold value indicates an
important change from the patients’ or clinicians’ perspective. Further research is therefore warranted to determine the minimal clinical important
difference/change of EE–ROM during the ULNT1 in order to interpret with certainty the effects of acupuncture and other therapies in people with increased mechanosensitivity of the median nerve.
The stimulation of a point located more proximally to the elbow (LU 5’’) did not show greater gains in EE-ROM than the stimulation of a more distally point (PC 5). Thus, the hypothesis of obtaining enhanced needling effects at a more proximal point could not be verified. This suggests, nonetheless, that puncture of more distal points may not be necessary to modulate the
mechanosensitivity of the median nerve, reducing the potential risk of damaging the median nerve. Future research should take these findings into account when designing clinical studies.
Findings from this study should be interpreted in light of its limitations. Given its exploratory nature, no sample size calculation was conducted. Nevertheless, the results presented here may contribute to determine the sample size for larger scale studies. Generalizability is also limited because only asymptomatic subjects were tested in here. Studies in populations with nerve-related pain and disability are needed to evaluate the effects of acupuncture in peripheral nerves with evidence of increased
mechanosensitivity. Additionally, we only used a neurodynamic test to assess the mechanosensitivity of the median nerve as this was the most suitable procedure to be applied in this exploratory research. In future research, a battery of measurements, including quantitative sensory testing and patient-reported outcome measures37, should be considered to comprehensively capture the complexity of gain in somatosensory function phenomenon, characterise study participants, improve the interpretation of the potential effects of acupuncture in patients with nerve-related pain, and assess its effects in functioning and health-related quality of life.
CONCLUSIONS
Immediately after acupuncture, the mechanosensitivity of the median nerve appears to be reduced as observed by an increase in elbow extension
during the ULNT1. However, further studies are necessary to confirm these preliminary findings.
REFERENCES
1. Jaberzadeh S, Scutter S, Nazeran H. Mechanosensitivity of the median nerve and mechanically produced motor responses during Upper Limb
Neurodynamic Test 1. Physiotherapy. 6// 2005;91(2):94-100.
2. Nee RJ, Butler D. Management of peripheral neuropathic pain: Integrating neurobiology, neurodynamics, and clinical evidence. Physical Therapy in Sport. 2006;7(1):36-49.
3. Nee RJ, Vicenzino B, Jull GA, Cleland JA, Coppieters MW. Neural tissue management provides immediate clinically relevant benefits without harmful effects for patients with nerve-related neck and arm pain: a randomised trial. Journal of Physiotherapy. 2012;58:23-31.
4. Nee RJ, Jull GA, Vicenzino B, Coppieters MW. The validity of upper-limb neurodynamic tests for detecting peripheral neuropathic pain. J. Orthop. Sports Phys. Ther. 2012;42(5):413-424.
5. Costello M, Puentedura E, Cleland J, Ciccone CD. The immediate effects of soft tissue mobilization versus therapeutic ultrasound for patients with neck and arm pain with evidence of neural mechanosensitivity: a randomized clinical trial. J Man Manip Ther. Jul 2016;24(3):128-140.
6. López-de-Uralde-Villanueva I, Beltran-Alacreu H, Fernández-Carnero J, Gil-Martínez A, La Touche R. Differences in Neural Mechanosensitivity
Between Patients with Chronic Nonspecific Neck Pain With and Without Neuropathic Features. A Descriptive Cross-Sectional Study. Pain Med. 2016;17(1):136-148.
7. Baron R, Binder A, Attal N, Casale R, Dickenson AH, Treede RD.
Neuropathic low back pain in clinical practice. Eur. J. Pain. 2016;20(6):861-873. 8. Smart KM, Blake C, Staines A, Thacker M, Doody C. Mechanisms-based classifications of musculoskeletal pain: Part 2 of 3: Symptoms and signs of peripheral neuropathic pain in patients with low back (±leg) pain. Man. Ther. 8// 2012;17(4):345-351.
9. Jaberzadeh S, Zoghi M. Mechanosensitivity of the median nerve in patients with chronic carpal tunnel syndrome. Journal of Bodywork and Movement Therapies. 4// 2013;17(2):157-164.
10. Fingleton C, Smart K, Moloney N, Fullen BM, Doody C. Pain sensitization in people with knee osteoarthritis: a systematic review and meta-analysis. Osteoarthritis Cartilage. 2015;23(7):1043-1056.
11. Villafañe JH, Silva GB, Bishop MD, Fernandez-Carnero J. Radial Nerve Mobilization Decreases Pain Sensitivity and Improves Motor Performance in Patients With Thumb Carpometacarpal Osteoarthritis: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2012;93(3):396-403.
12. Nijs J, Apeldoorn A, Hallegraeff H, et al. Low back pain: guidelines for the clinical classification of predominant neuropathic, nociceptive, or central
sensitization pain. Pain physician. May-Jun 2015;18(3):E333-346.
13. Hoang N, Sar C, Valmier J, Sieso V, Scamps F. Electro-acupuncture on functional peripheral nerve regeneration in mice: a behavioural study. BMC Complement. Altern. Med. 2012;12(1):141.
14. Kim JH, Min B-I, Na HS, Park DS. Relieving effects of
electroacupuncture on mechanical allodynia in neuropathic pain model of inferior caudal trunk injury in rat: mediation by spinal opioid receptors. Brain Res. 2/20/ 2004;998(2):230-236.
15. Cidral-Filho FJ, da Silva MD, Moré AOO, Córdova MM, Werner MF, Santos ARS. Manual acupuncture inhibits mechanical hypersensitivity induced by spinal nerve ligation in rats. Neuroscience. 2011;193(0):370-376.
16. Schröder S, Liepert J, Remppis A, Greten JH. Acupuncture treatment improves nerve conduction in peripheral neuropathy. Eur. J. Neurol.
2007;14(3):276-281.
17. Schulman RA, Liem B, Alex Moro. Treatment of Carpal Tunnel Syndrome With Medical Acupuncture. Medical Acupuncture. 2008;20(3):163-167.
18. Sim H, Shin B-C, Lee MS, Jung A, Lee H, Ernst E. Acupuncture for Carpal Tunnel Syndrome: A Systematic Review of Randomized Controlled Trials. The journal of pain : official journal of the American Pain Society. 2011;12(3):307-314.
19. Yang C-P, Hsieh C-L, Wang N-H, et al. Acupuncture in Patients With Carpal Tunnel Syndrome: A Randomized Controlled Trial. The Clinical Journal of Pain. 2009;25(4).
20. Kumnerddee W, Kaewtong A. Efficacy of acupuncture versus night splinting for carpal tunnel syndrome: a randomized clinical trial. J. Med. Assoc. Thai. 2010;93(12):1463-1469.
21. Ural FG, #xfc, #xe7, et al. The Acupuncture Effect on Median Nerve Morphology in Patients with Carpal Tunnel Syndrome: An Ultrasonographic Study. Evid. Based Complement. Alternat. Med. 2017;2017:5.
22. Haanpää M, Attal N, Backonja M, et al. NeuPSIG guidelines on neuropathic pain assessment. PAIN®. 1// 2011;152(1):14-27.
23. Sauer SK, Bove GM, Averbeck B, Reeh PW. Rat peripheral nerve components release calcitonin gene-related peptide and prostaglandin E2 in response to noxious stimuli: evidence that nervi nervorum are nociceptors*. Neuroscience. 8// 1999;92(1):319-325.
24. Schmid AB, Nee RJ, Coppieters MW. Reappraising entrapment neuropathies – Mechanisms, diagnosis and management. Man. Ther. 2013/12/01/ 2013;18(6):449-457.
25. Basson A, Olivier B, Ellis R, Coppieters M, Stewart A, Mudzi W. The Effectiveness of Neural Mobilization for Neuro-Musculoskeletal Conditions: A Systematic Review and Meta-Analysis. J. Orthop. Sports Phys. Ther.
2017;0(0):1-76.
26. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA):
Extending the CONSORT Statement. PLoS Med. 2010;7(6):e1000261. 27. Hanada E, Kirby RL, Mitchell M, Swuste JM. Measuring leg-length
discrepancy by the “iliac crest palpation and book correction” method: Reliability and validity. Arch. Phys. Med. Rehabil. 7// 2001;82(7):938-942.
28. Nee RJ, Yang C-H, Liang C-C, Tseng G-F, Coppieters MW. Impact of order of movement on nerve strain and longitudinal excursion:A biomechanical study with implications for neurodynamic test sequencing. Man. Ther. 8// 2010;15(4):376-381.
29. Coppieters MW, Hough AD, Dilley A. Different Nerve-Gliding Exercises Induce Different Magnitudes of Median Nerve Longitudinal Excursion: An In
Vivo Study Using Dynamic Ultrasound Imaging. J. Orthop. Sports Phys. Ther. 2009/03/01 2009;39(3):164-171.
30. Cruz J, Morais N. Intrarater Agreement of Elbow Extension Range of Motion in the Upper Limb Neurodynamic Test 1 Using a Smartphone
Application. Arch. Phys. Med. Rehabil. 2016;97(11):1880-1886.
31. Lohkamp M, Small K. Normal response to Upper Limb Neurodynamic Test 1 and 2A. Man. Ther. 4// 2011;16(2):125-130.
32. Xu S, Wang L, Cooper E, et al. Adverse events of acupuncture: a systematic review of case reports. Evid. Based Complement. Alternat. Med. 20130410 DCOM- 20130704 2013;2013(12):1-15.
33. Coppieters M, Stappaerts K, Janssens K, Jull G. Reliability of detecting ‘onset of pain’ and ‘submaximal pain’ during neural provocation testing of the upper quadrant. Physiother. Res. Int. 2002;7(3):146–156.
34. Shinbara H, Okubo M, Sumiya E, Fukuda F, Yano T, Kitade T. Effects of manual acupuncture with sparrow pecking on muscle blood flow of normal and denervated hindlimb in rats. Acupuncture in Medicine. 2008;26(3):149.
35. Morais NV, Pascoal AG. Scapular positioning assessment: Is side-to-side comparison clinically acceptable? Man. Ther. 2013 2013;18(1):46-53.
36. Zhang R, Lixing Lao, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 20140122 DCOM- 20140311 2014;120(2):482-503.
37. Colloca L, Ludman T, Bouhassira D, et al. Neuropathic pain. Nature Reviews Disease Primers. 02/16/online 2017;3:17002.
Funding statement:
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing Interests: None declared.
Contributorship:
N Morais contributed to the conception and design of the work, acquisition, analysis, and interpretation of data, and drafted the manuscript. H Greten
contributed to the conception and design of the work and interpretation of data. MJ Santos contributed to the design of the work and acquisition of the data. J Machado contributed to the design of the work and acquisition of the data. All authors revised the work critically for important intellectual content, and approved the final version of the manuscript.
FIGURE LEGENDS
Figure 1. Design and flow of the participants through the trial.
TABLES
Table 1. Baseline characteristics of the participants PC group (n = 14) LU group (n = 17) p Value Age (years) 34.3 ± 11.1 33.4 ± 12.9 0.841 Gender 0.456 Male 3 (21.4 %) 6 (35.3 %) Female 11 (78.6 %) 11 (64.7 %) Hand dominance 0.107 Right 14 (100 %) 13 (76.5 %) Left 0 (0%) 4 (23.5 %) Mass (Kg) 62.5 ± 14.1 61.0 ± 8.5 0.924 Height (cm) 167.0 ± 9.1 167.4 ± 10.3 0.718 BMI (Kg/m2) 22.2 ± 3.4 21.7 ± 2.6 0.701
BMI, body mass index;
Table 2. Effects of acupuncture on elbow extension range of motion at pain onset and maximum tolerable during the ULNT1.
PC group (n = 14) LU group (n = 17) Time Time group interaction Pre-AC Post-AC Pre-AC Post-AC p Value Effect size (η2 p) p Value Effect size (η2 p) EE-ROM at pain onset () 31.5 ± 13.7 32.6 ± 15.2 28.8 ±15.8 34.0 ± 17.4 0.029 0.154 0.142 0.001 EE-ROM at maximu m tolerable () 55.2 ± 15.3 59.8 ± 21.1 51.1 ± 16.1 57.6 ± 18.1 0.002 0.277 0.567 0.011
AC, acupuncture; EE-ROM, elbow extension range of motion; (η2
p), eta square
partial