2019/2020
Maria Ribeiro Pereira
Anorexia nervosa as a genetically determined condition
Mestrado Integrado em Medicina
Área: Ciências médicas e da saúde – Medicina Clínica
Tipologia: Monografia
Trabalho efetuado sob a Orientação de:
Doutora Isabel Maria Boavista Vieira Marques Brandão
Trabalho organizado de acordo com as normas da revista:
International Journal of Clinical Neurosciences and Mental Health
Maria Ribeiro Pereira
Anorexia nervosa as a genetically determined condition
UC Dissertação/Projeto (6º Ano) - DECLARAÇÃO DE INTEGRIDADE
Eu, Maria Ribeiro Pereira, abaixo assinado, nº mecanográfico 201403828, estudante do 6º ano do Ciclo de Estudos Integrado em Medicina, na Faculdade de Medicina da Universidade do Porto, declaro ter atuado com absoluta integridade na elaboração deste projeto de opção.
Neste sentido, confirmo que NÃO incorri em plágio (ato pelo qual um indivíduo, mesmo por omissão, assume a autoria de um determinado trabalho intelectual, ou partes dele). Mais declaro que todas as frases que retirei de trabalhos anteriores pertencentes a outros autores, foram referenciadas, ou redigidas com novas palavras, tendo colocado, neste caso, a citação da fonte bibliográfica.
Faculdade de Medicina da Universidade do Porto, 12/04/2020
UC Dissertação/Projeto (6º Ano) – DECLARAÇÃO DE REPRODUÇÃO
NOME
Maria Ribeiro Pereira
NÚMERO DE ESTUDANTE E-MAIL
201403828 [email protected]
DESIGNAÇÃO DA ÁREA DO PROJECTO
Ciências médicas e da saúde – Medicina Clínica
TÍTULO DISSERTAÇÃO/MONOGRAFIA (riscar o que não interessa) Anorexia nervosa as a genetically determined condition
ORIENTADOR
Isabel Maria Boavista Vieira Marques Brandão
COORIENTADOR (se aplicável)
ASSINALE APENAS UMA DAS OPÇÕES:
É AUTORIZADA A REPRODUÇÃO INTEGRAL DESTE TRABALHO APENAS PARA EFEITOS DE INVESTIGAÇÃO, MEDIANTE DECLARAÇÃO ESCRITA DO INTERESSADO, QUE A TAL SE COMPROMETE.
É AUTORIZADA A REPRODUÇÃO PARCIAL DESTE TRABALHO (INDICAR, CASO TAL SEJA NECESSÁRIO, Nº MÁXIMO DE PÁGINAS, ILUSTRAÇÕES, GRÁFICOS, ETC.) APENAS PARA EFEITOS DE INVESTIGAÇÃO, MEDIANTE DECLARAÇÃO ESCRITA DO INTERESSADO, QUE A TAL SE COMPROMETE.
DE ACORDO COM A LEGISLAÇÃO EM VIGOR, (INDICAR, CASO TAL SEJA NECESSÁRIO, Nº MÁXIMO DE PÁGINAS, ILUSTRAÇÕES, GRÁFICOS, ETC.) NÃO É PERMITIDA A REPRODUÇÃO DE QUALQUER PARTE DESTE TRABALHO.
Faculdade de Medicina da Universidade do Porto, 12/04/2020
Anorexia nervosa as a genetically determined condition
1
2
Abstract
3
Anorexia nervosa (AN) is a psychiatric condition classically associated with an
4
extremely low body weight, a constant desire to be thin, with restriction of food intake
5
and a distorted self-perceived body image. This condition is potentially fatal and there
6
is still a lack of effective treatment options. In order to overcome this problem, the
7
scientific community is being encouraged to try to move this field into personalized
8
medicine. This can be achieved by deeply understanding the genetic and metabolic
9
pathways that contribute to the etiology of this disorder. Since the last century, there
10
has been evidence from twin and family studies supporting the existence of a genetic
11
basis for AN. In the past few years, the genetic investigation has entered a very precise
12
level, revealing nine genome-wide significant loci as well as significant genetic
13
correlations between AN, metabolic traits and psychiatric phenotypes. In this review,
14
we will summarize the most important findings on this field.
15
16
Keywords: anorexia nervosa; eating disorders; genetics; heritability
Introduction
18
According to the Diagnostic and Statistical Manual of Mental Disorders
(DSM-19
5), anorexia nervosa (AN) is a complex, severe and potentially life-threatening
20
condition and it can be categorized into two distinct subtypes, the restricting subtype
21
and the binge-eating subtype. [1]
22
AN is far more common in young adult or adolescent females than males [1-3]
23
and the onset of the disease is frequently correlated with a stressful experience. [1]
24
There is often delusional thinking and no insight about the seriousness of the
25
malnourished status, which often leads to several physiological disturbances, including
26
amenorrhea. [1, 4] These patients additionally present with other psychiatric traits, such
27
as depressive, obsessive-compulsive, obstinate thinking, and overly inhibited emotional
28
expression. [1, 5]
29
AN is still a widely misunderstood disorder since there is a noticeable
30
heterogeneity regarding the treatment response, generating a global concern. [6]
31
Pharmacotherapy has a secondary role in the treatment of eating disorders and it
32
should not be considered as a unique intervention. [7] Mortality is higher in AN than in
33
any other psychiatric disorder and the outcome is still unacceptably poor. The majority
34
of patients develop a relapsing course of the disease and only 25-30% fully recover. [8]
35
Most psychiatric disorders are known for having a very complex etiology,
36
including genetic, environmental and social factors. AN is no exception to this and it is
37
a very particular disease with characteristics that cannot be generalized for other types
38
of eating disorders. [9, 10] It is known that there is an increased risk of AN among
first-39
degree relatives of individuals with the disorder. However, until recently, there was not
40
enough evidence to show a clear genetic background of AN. This review aims to
41
provide the readers with an overview of the most relevant historical genetic findings in
42
anorexia nervosa, the most effective methods of genetic analysis as well as the most
43
recent and important discoveries on this matter and its possible clinical pertinence.
44
Methods
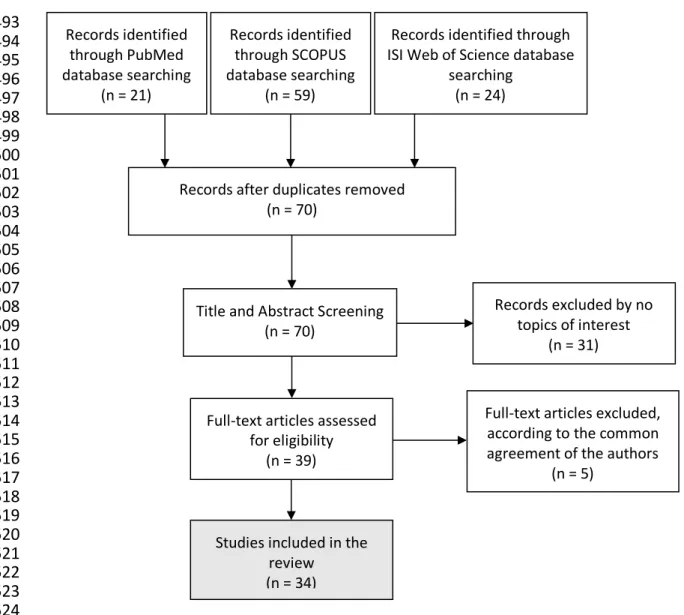
46
A literature search was made on PubMed using the query " "Anorexia
47
Nervosa/genetics"[Mesh] ", on SCOPUS using the query "KEY ( "Anorexia
48
Nervosa" AND "genetics" )" and on ISI Web of Science using the query
49
"TOPIC:(genetics) AND TOPIC: ("Anorexia Nervosa")". In this search, only articles
50
published during 2018 and 2019 were included. 21 results were found from the
51
PubMed data basis, 59 results from the SCOPUS data basis and 24 results from the
52
ISI Web of Science data basis, meaning a total of 104 results. Among these, 34
53
duplicates were found. After reading all the titles and abstracts from the 70 remaining
54
articles, 39 articles were considered to be the most relevant because of their
55
contribution to the subject. After full-text assessment for eligibility, 5 articles were
56
excluded by common agreement of the authors. A flow chart representing the methods
57
used is shown in figure 1.
58
59
Discussion
60
Historical background of Anorexia Nervosa
61
There is an intriguing general conception that AN is quite a recent social and
62
cultural phenomenon linked to the obsession with body image and the constant
63
promotion of slenderness amongst adolescent girls nowadays. [11] Nevertheless, this
64
condition is not believed to be that recent since, in 1983, Skrabanek summarized the
65
most important periods in the history of AN until then. [12]
66
AN is first described between the 5th and 13th centuries in theological literature
67
and it is interpreted as a "supernatural manifestation". Between the 16th and 18th
68
centuries, it was still associated with religion and beliefs, since medical descriptions
69
insisted on a phenomenon called "anorexia mirabilis" or "inedia prodigiosa", which
70
would be interpreted as an ability to perform self-discipline as a path to God. [12]
71
The first clinical report of AN as "a form of hypochondriacal delirium occurring
72
consecutive to dyspepsia and characterized by refusal of food" was only presented in
73
the 19th century by a French psychiatrist. [13]
74
Until the beginning of the 20th century, AN was believed to be a purely
75
psychiatric disorder and its potential biological and physiological mechanisms were not
76
being considered. The initial studies were mainly candidate gene analysis and provided
77
inconsistent and non-replicable results. [9]
78
In the 1960s, the advancement of genetic investigation mirrored the evolution of
79
technology. [14] Due to advances in human genetics investigations, metabolic and
80
neuroendocrine influences, as well as their genetic basis, are starting to be considered
81
as possible intermediaries of the abnormal reward pathway that appears to be seen in
82
AN patients, allowing a potential adjustment on the disorder’s etiology as we know it.
83
[11, 15]
84
Nowadays, due to the recent large scale successful studies we reviewed in this
85
paper, AN is considered a multifactorial psychiatric disorder which has several risk
86
factors, including genetic variations and its consequent metabolic impact, as well as
87
internal and external environmental factors.
88
89
Why do Genetic Research on Psychiatric disorders?
90
Some critics have reported that the findings on genetic variations of psychiatric
91
disorders are meaningless and will not have relevant implications on therapy. The
92
authors consider that there should not be put so much effort and resources into
93
something that constantly produces results with lack of clinical interest. [16]
94
However, medical research for eating disorders is still considered to be
95
underfunded when taking in consideration the advantages it brings to global disability
96
adjusted life-years. [17] There is a need to decipher the basic mechanisms underlying
97
these complex illnesses. [18] The main goal of genetic research on psychiatric
98
disorders is to provide clinically useful information in the future, to develop new
99
preventive strategies, to potentially guide new drugs development and to identify the
100
ones at risk of having a poor outcome, in order to provide personalized medical care.
101
[18]
102
103
Genetic Evidence on Anorexia Nervosa
104
Heritability is defined as the percentage of phenotypic variance due to
105
hereditary factors only. [18] Family and twins studies were among the first lines of
106
evidence confirming an increased genetic risk for AN, estimating heritability at
40%-107
60%. They still are the ones having the most replicable results among all genetic
108
studies on eating disorders. [19, 20] The consistency of this results has encouraged the
109
investment of the scientific community into studying the genetics of AN. [6]
110
Once we entered the era of the molecular genetics, a constant effort was made
111
to find significant results on this subject. However, the initial studies that were
112
developed did provide very disappointing results, examining only a few markers and
113
having very small samples. [9, 21, 22] The studies made on the epigenetics of eating
114
disorders were mostly investigating methylation patterns at candidate genes on very
115
small samples and also provided inconclusive results. [23]
116
Animal models have a big role on studying some metabolic pathways. However,
117
in AN they appear to be inadequate to replicate the human food intake and reward
118
process since it is not possible to reproduce the complex behavioral aspects and life
119
events that humans experience and have such a big role in the establishment of AN.
120
[24]
121
During the past decade, we have witnessed notable advances on the genetics
122
of psychiatric disorders and have been gifted with a virtual avalanche of data on the
123
human genome. It is now known that the genetic architecture of multiple psychiatric
124
disorders often overlaps. [14]
125
Evidence indicates that there may be an immense amount of genes contributing
126
to the increased risk, each one having a minor effect. [9, 19, 21, 25] This partly
127
explains the failure of the linkage and candidate gene studies, since the effects of each
128
genetic variant alone are probably too weak to be detected by those methods.
129
We now understand that it is essential to define the biology of the feeding
130
dysregulation process. [26] Multiple small studies focused on those pathways.
131
Serotonin is known for having a major role in appetite regulation. This led to the
132
development of studies testing if polymorphisms of the gene coding for the serotonin
133
receptors had any influence on the onset of AN. The 5-HT2A receptor coding gene had
134
some promising results linking its expression not only to AN, but also to
obsessive-135
compulsive disorder. [27, 28] Unfortunately, authors were unable to replicate those
136
results in posterior investigations. [27]
137
The dysregulation of the human neuronatin gene (NNAT) appears to have an
138
impact in multiple metabolic ways, including insulin secretion and energy homeostasis.
139
Lombardi et al. reported multiple variants of the NNAT to be associated with
140
susceptibility for eating disorders. However, this is a finding from a very small sample
141
study and it has not been replicated. [29]
142
There were also some authors trying to find a genetic correlation between the
143
brain volume and AN. Walton et al. reported weak evidence for an association between
144
common genetic variants linked to subcortical brain volumes and those variants linked
145
to AN. [30]
146
Even though we mainly look at gene alterations trying to find a cause for the
147
illness, it is also important to consider the possibility of the gene expression to be
148
altered due to the malnourished status that comes with AN. [31, 32] There is evidence
149
that an early onset of AN and a longer period with the disease can result in methylation
150
of gene pathways liked to anxiety, social awareness and even serotonin receptors. [33]
151
152
153
154
Novel methods to detect genetic correlation: Genome-wide Association Study and
155
Polygenic Risk Score
156
A brief explanation of how the genetic analysis is currently being made is
157
important to understand the latest results summarized in this review.
158
There are millions of common genetic variants identified in the human genome.
159
These variations are present in more than 1% of the population and the most common
160
are single-nucleotide polymorphisms (SNPs), where there is a single nucleotide
161
substitution at a specific location. [18]
162
We will now briefly define two major concepts in this field: Genome-wide
163
Association Study and Polygenic Risk Score.
164
A Genome-wide Association Study (GWAS) is an observational study that
165
typically focuses on trying to make an association between SNPs and a specific trait or
166
disease. GWAS is primarily focused on detecting common genetic variations, that
167
individually confer a very small risk but when added together may be responsible for a
168
considerable portion of the disease’s heritability. [9] A GWAS compares cases and
169
controls, similarly to the candidate-gene association studies. However, they do it using
170
a hypothesis-free approach and, therefore, not limiting the amount of information we
171
can obtain from a study. [21]
172
On the other side, a Polygenic Risk Score (PRS) is a statistical technique that
173
aggregates effects of variants across the genome to estimate heritability, to infer
174
genetic overlap between traits and to predict phenotypes based on a genetic profile.
175
[16] According to Bogdan R. et. al, the PRSs shouldn’t yet be interpreted as diagnostic
176
tools, but as simple predictors of risk. [16]
177
Since the GWAS are often used to calculate PRS, we can infer that as GWAS
178
sample sizes get larger and better described, PRSs are likely to become more precise
179
and, therefore, have a very important role in the future of personalized medicine.
180
181
182
AN samples and international cooperation
183
Since the genetic architecture of the psychiatric disorders appears to be so
184
complex, large samples of cases and controls were gathered in order to perform
185
validated analysis through GWAS. This was achieved due to the existence of two main
186
data basis, one developed by the Eating Disorders Working Group of the Psychiatric
187
Genomics Consortium (PGC-ED) and, more recently, the Anorexia Nervosa Genetics
188
Initiative (ANGI).
189
ANGI is an international collaboration that was developed because there was a
190
need for a bigger sample size than the one provided previously by the PGC-ED. ANGI
191
recruited over 13,000 individuals from the United States of America, Australia, New
192
Zealand, Sweden and Denmark, making it the largest sample of AN cases and controls
193
and the most rigorous genetic research on eating disorders ever made. [21, 34] The
194
recruitment was made via national registers, treatment centers and social media. Each
195
participant was submitted to a questionnaire and provided either peripheral blood or
196
saliva samples, which were then genotyped. ANGI has the goal to globally provide
197
validated and easy access information to encourage the development of more studies
198
on this subject. [34]
199
200
Genome-wide significant loci
201
GWAS has been used since 2005 and it brought a revolutionary vision on how
202
to study AN, since it apparently does not follow the principles of the Mendelian pattern
203
of inheritance. Since then, multiple GWASs about AN were developed. However, only
204
two of them provided genome-wide significant results. [21]
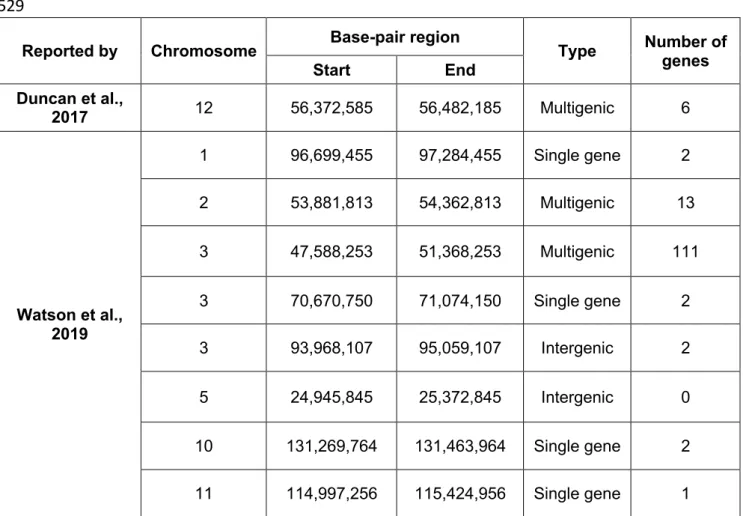
205
The first significant locus to be identified in AN via GWAS was reported by
206
Duncan et al. in 2017 in a study that included 3495 cases and 10982 controls. This is a
207
broad and multigenic locus, located on chromosome 12, in a region that had been
208
previously studied by its relation to autoimmune disorder and type 1 diabetes. This
209
study also reported significant positive and negative genetic correlations between AN
210
and other phenotypes, such as other psychiatric disorders and multiple metabolic traits,
211
summarized on table 2. [6, 35]
212
In 2019, even bigger advances on the knowledge of genetic architecture of the
213
AN were made. Watson et al. developed the biggest GWAS ever made on this subject,
214
combined both the PGC-ED and ANGI samples, making a total of 16 992 AN cases
215
and 55 525 controls, the largest sample ever studied. [36] This study provided robust
216
significant findings, having identified eight independent genome-wide significant loci,
217
listed on table 1, and multiple genetic correlations between anorexia nervosa and other
218
phenotypes, listed on table 2. [6, 36]
219
220
From GWAS to genetic correlations to multiple traits
221
The two studies mentioned above provided very comparable information about
222
the significant positive and negative genetic correlations to several traits, as we can
223
see on table 2.
224
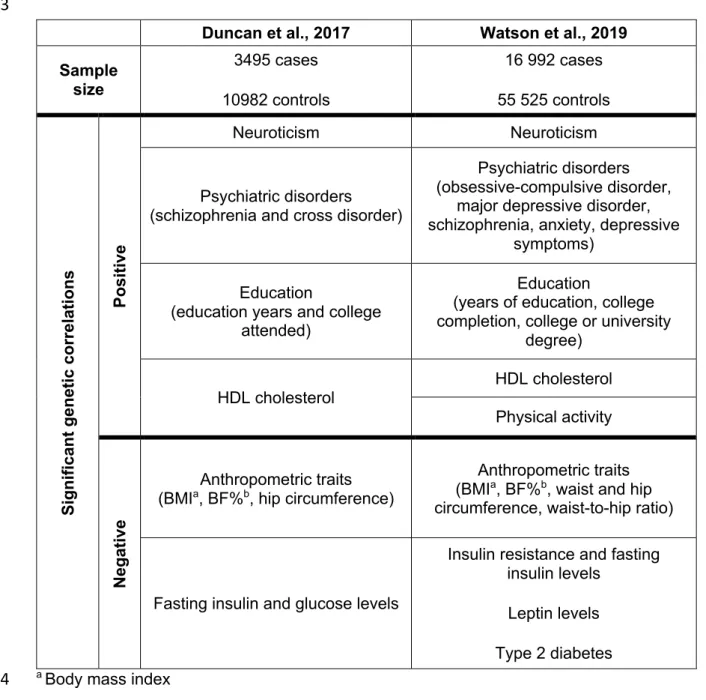
The significant positive genetic correlation of AN with neuroticism and other
225
psychiatric traits and disorders is supported by epidemiological evidence of AN patients
226
often presenting other psychiatric traits. This correlation reinforces that there is a
227
shared genetic risk among several psychiatric disorders. [35, 36] Additionally, some of
228
this personality traits can be present before the onset of AN and, therefore, signal the
229
individuals who are at higher risk of developing it. [37]
230
Both studies reported a significant positive genetic correlation between AN and
231
education factors, such as the number of education years and the attendance to
232
college. With that in mind, we could look at this as an effect of a higher pressure for
233
academic success in highly educated families, resulting in increased anxiety levels that
234
could be associated to the onset of AN. However, these results are now revealing that
235
there is also a genetic influence for this linkage. [35, 36]
236
Regarding the metabolic phenotypes, we can group the findings into two distinct
237
groups. The “favorable” phenotypes, that include HDL cholesterol, have a significant
238
positive correlation to AN, as opposed to the “unfavorable” phenotypes, that include
239
insulin and glucose levels, and have a significant negative genetic correlation.
240
Finally, the anthropometric measures, such as extreme body mass index (BMI),
241
hip and waist circumference and body fat percentage, have a significant negative
242
genetic correlation to AN. This data could be the first step to a better understanding of
243
the shared biological mechanisms of extreme weight conditions. The same genetic
244
factors influencing normal BMI, body shape and composition variations can also be
245
responsible by the dysregulation of this measures in AN and obesity. [38, 39]
246
247
Does the in utero environment influence AN liability?
248
Placenta plays a central part when modeling the environment in which the fetus
249
is developing. Using an activity-based anorexia (ABA) rat model, Schroeder et al.
250
successfully demonstrated, for the first time, a possible mechanism of ABA in utero
251
programming. This mechanism could be explained by the alterations of placental gene
252
expression, such as placental miR-340 methylation, when submitted to stress. It is well
253
known that maternal stress during pregnancy can lead to a series of negative
254
consequences for the baby. Controversially, they reported that chronic exposure to
pre-255
natal stress can result in a resistance mechanism for the fetus, since the susceptibility
256
to AN seems to be downregulated by the placental miR-340 methylation. [40]
257
258
Sex differences – could genetics play a role?
259
It is well known that AN is around nine times more frequent in female than in
260
males [3] and, even though the environmental factors and the body image concerns
261
are more propitious for women to develop this kind of disorder, the biological cause for
262
such an evident difference is yet to be found. There are reports of subtle sex
263
differences on signs and symptoms presentation of eating disorders as well as
264
differences on their motivations for the weight loss. Even though some features are still
265
unclear, males appear to engage more on physical activity as a compensatory behavior
266
and they seem to be more focused on their muscle definition as opposed to the
267
females who mainly report the desire of thinness. [41]
268
Hubel et al. extended the research on the GWAS performed by Duncan et al.
269
and Watson et al. and tried to find a connection between the sex specific genomic
270
effects on body fat percentage (BF%) and AN. This investigation showed us that
271
female-specific genomic effects on BF% is significantly greater than the one observed
272
in males. This data suggests that there might be a specific group of genetic variations
273
that are differentially active in females and can contribute to the AN susceptibility. [35,
274
36, 42]
275
Since the onset of puberty apparently increases the genetic risk of developing
276
eating disorders, we understand that sex hormones can possibly have an important
277
role here. [41] This increase is more preeminent in females, and it is independent from
278
the environmental factors, raising the possible role of estrogen in activating or
279
modulating the genetic risk. [41, 43]
280
Neurotensin is a peptide discovered in the human brain over forty years ago
281
and it is known to be linked to the regulation of body temperature, locomotor activity,
282
metabolic rate and feeding rate. Schroeder et al., reported that females have four times
283
more neurotensin-expressing cells in certain parts of the brain comparing to males.
284
Estrogen modulates the expression of these cells, since the quantity of neurotensin
285
expressing cells vary according to estrogen levels during the menstrual cycle. This
286
means that the roles of those two systems can be intertwined, contributing to a bigger
287
liability for AN in females and supports the importance of future investigation on how
288
the estrogen level impacts the development of AN. [26]
289
There is also the possibility that some Y chromosome gene expressions could
290
have a protective effect against AN. [22] However, most of the genetic studies
291
performed did not have access to the information of the sex chromosomes, which
292
would be essential to include in future investigations. [42]
293
Evidence shows that it could be much easier to access the influence of genetics
294
in AN in a sample of male individuals. In this group, the environment appears to have a
295
smaller influence on AN development. Taking this into account, we can suppose that a
296
stronger genetic influence can be necessary for the onset of AN in males. [44]
297
However, due to the low prevalence of this condition in males and the small size
298
samples, it was not possible to perform a robust investigation until now. [45]
299
300
Future perspectives
301
Even though the future on this area seems very promising, in a short period of
302
time, it would only be reasonable to expect this data to help a better understanding of
303
familiar risk. [46] Imprecise interpretations and overly optimistic report could lead to
304
distortion of results and inappropriate investments. [18]
305
In the context of psychiatric disorders, where bad adherence to treatment due
306
to lack of insight is often a problem, it would probably be useful to provide the patient
307
and the people around them some explicit medical data, for example, the identification
308
of genetic variations known to be related to the condition.
309
It is probably too early to assume that these new discoveries would now be able
310
to guide us, for example, on how to choose the best medication for each patient. [46]
311
However, giving the reconceptualization of AN not only as a psychiatric disorder, but
312
also as a metabolic and immune related condition [35, 36], we can expect future
313
pharmacological agents to act primarily in these systems. [47]
314
In the future, genetic studies comparing the patients who experience relapse
315
after treatment to those who maintain the weight gained during treatment, could be an
316
important source of information and could lead us to an early identification of the most
317
treatment resistant cases by characterizing biomarkers of diagnosis and prognosis. [6,
318
48] Another important relation to be investigated in the future is the possible genetic
319
and metabolic shared risk factors between AN and suicidality in order to work towards
320
the prevention of this tragic outcome. [49]
321
322
Conclusion
323
Over the past decade, we started to comprehend that psychiatric disorders are
324
polygenic and may have the contribution of hundreds or thousands of genetic
325
variations, each having a small effect. [9, 19, 21, 25] We understand that the external
326
environment triggers cannot be ignored since this disorder has an extremely high social
327
burden, but we have no doubt that there is an interplay between genetics, the brain and
328
metabolism supporting the etiological mechanisms of AN.
329
It is challenging to extract information for our understanding on pathophysiology
330
from the results we have so far, but we know that this is a very promising area of
331
research. We need to have a deeply understanding of the different phenotypes existent
332
in this illness in order to be able to connect gene expression to behavior alterations in
333
the future. [14]
334
This is a disorder for which we still do not have very effective treatment options.
335
Therefore, an early identification of the patients suffering from AN could allow a more
336
successful medical intervention. Also, given the larger brain plasticity in younger
337
patients, an early treatment may be linked to minimize the neurocognitive damages
338
that can be provoked by AN. [50]
339
The genetic studies on AN have some important limitations that need to be
340
overcome. Although the sample size is now growing due to the international
341
collaborations mentioned above, the question of how big is big enough is still pertinent
342
to be discussed. [18] Furthermore, the investigations developed until now, include
343
mostly female populations of European ancestry and the male samples are still not
344
adequate to test male-specific genetic variations. The same problem exists for
345
individuals of other ancestral backgrounds. [6]
346
The most promising type of research studies seems to be the GWAS, since the
347
two analyzed in this review provided the strongest evidence ever found on the genetics
348
of AN. There are, until now, nine genome-wide significant loci identified in AN. [35, 36]
349
Taking this into account, the scientific community is now being encouraged to gather
350
even larger samples, to develop new GWASs to try to replicate previous results and
351
find new significant loci.
352
References
353
1.
American Psychiatric Association. Diagnostic and statistical manual of mental
354
disorders. 5th ed2013.
355
2.
Hudson JI, Hiripi E, Pope HG, Jr., Kessler RC. The prevalence and correlates of
356
eating disorders in the National Comorbidity Survey Replication. Biol Psychiatry.
357
2007;61(3):348-58.
358
3.
Bulik CM, Sullivan PF, Tozzi F, Furberg H, Lichtenstein P, Pedersen NL.
359
Prevalence, heritability, and prospective risk factors for anorexia nervosa. Arch Gen
360
Psychiatry. 2006;63(3):305-12.
361
4.
Behar R, Arancibia M, Gaete MI, Silva H, Meza-Concha N. The delusional
362
dimension of anorexia nervosa: Phenomenological, neurobiological and clinical
363
perspectives. Revista de Psiquiatria Clinica. 2018;45(1):15-21.
364
5.
Lee PH, Anttila V, Won H, Feng YCA, Rosenthal J, Zhu Z, et al. Genomic
365
Relationships, Novel Loci, and Pleiotropic Mechanisms across Eight Psychiatric
366
Disorders. Cell. 2019;179(7):1469-82.e11.
367
6.
Bulik CM, Flatt R, Abbaspour A, Carroll I. Reconceptualizing anorexia nervosa.
368
Psychiatry and Clinical Neurosciences. 2019;73(9):518-25.
369
7.
Zipfel S, Schmidt U. Psychobiology of eating disorders – A gateway to precision
370
medicine. Current Neuropharmacology. 2018;16(8):1100-1.
371
8.
Bulik CM, Blake L, Austin J. Genetics of Eating Disorders What the Clinician
372
Needs to Know. Psychiatric Clinics of North America. 2019;42(1):59-+.
373
9.
Breithaupt L, Hübel C, Bulik CM. Updates on genome-wide association findings
374
in eating disorders and future application to precision medicine. Current
375
Neuropharmacology. 2018;16(8):1102-10.
376
10.
Dinkler L, Taylor MJ, Råstam M, Hadjikhani N, Bulik CM, Lichtenstein P, et al.
377
Association of etiological factors across the extreme end and continuous variation in
378
disordered eating in female Swedish twins. Psychological Medicine. 2019.
379
11.
Duriez P, Ramoz N, Gorwood P, Viltart O, Tolle V. A Metabolic Perspective on
380
Reward Abnormalities in Anorexia Nervosa. Trends in Endocrinology and Metabolism.
381
2019;30(12):915-28.
382
12.
Skrabanek P. Notes towards the history of anorexia nervosa. Janus.
1983;70(1-383
2):109-28.
384
13.
Marcé L-V. Note sur une forme de délire hypocondriaque consécutive aux
385
dyspepsies et caractérisée principalement par le refus d'aliment. Ann Med-Psychol.
386
1860;6:15-28.
387
14.
Sullivan PF, Geschwind DH. Defining the Genetic, Genomic, Cellular, and
388
Diagnostic Architectures of Psychiatric Disorders. Cell. 2019;177(1):162-83.
389
15.
Gorwood P, Blanchet-Collet C, Chartrel N, Duclos J, Dechelotte P, Hanachi M, et
390
al. New Insights in Anorexia Nervosa. Front Neurosci. 2016;10:256.
391
16.
Bogdan R, Baranger DAA, Agrawal A. Polygenic Risk Scores in Clinical
392
Psychology: Bridging Genomic Risk to Individual Differences. Annual Review of Clinical
393
Psychology: Annual Reviews Inc.; 2018. p. 119-57.
394
17.
Murray SB, Pila E, Griffiths S, Le Grange D. When illness severity and research
395
dollars do not align: are we overlooking eating disorders? World Psychiatry.
396
2017;16(3):321-.
397
18.
Hubel C, Leppa V, Breen G, Bulik CM. Rigor and reproducibility in genetic
398
research on eating disorders. Int J Eat Disord. 2018;51(7):593-607.
399
19.
Bulik CM, Kleiman SC, Yilmaz Z. Genetic epidemiology of eating disorders. Curr
400
Opin Psychiatry. 2016;29(6):383-8.
401
20.
Yilmaz Z, Hardaway JA, Bulik CM. Genetics and Epigenetics of Eating Disorders.
402
Adv Genomics Genet. 2015;5:131-50.
403
21.
Himmerich H, Bentley J, Kan C, Treasure J. Genetic risk factors for eating
404
disorders: an update and insights into pathophysiology. Therapeutic Advances in
405
Psychopharmacology. 2019;9.
406
22.
Mayhew AJ, Pigeyre M, Couturier J, Meyre D. An Evolutionary Genetic
407
Perspective of Eating Disorders. Neuroendocrinology. 2018;106(3):292-306.
408
23.
Subramanian S, Braun PR, Han S, Potash JB. Investigation of differential HDAC4
409
methylation patterns in eating disorders. Psychiatr Genet. 2018;28(1):12-5.
410
24.
Maussion G, Demirova I, Gorwood P, Ramoz N. Induced Pluripotent Stem Cells;
411
New Tools for Investigating Molecular Mechanisms in Anorexia Nervosa. Frontiers in
412
Nutrition. 2019;6.
413
25.
Smoller JW, Andreassen OA, Edenberg HJ, Faraone SV, Glatt SJ, Kendler KS.
414
Psychiatric genetics and the structure of psychopathology. Molecular Psychiatry.
415
2019;24(3):409-20.
416
26.
Schroeder LE, Leinninger GM. Role of central neurotensin in regulating feeding:
417
Implications for the development and treatment of body weight disorders. Biochimica
418
et Biophysica Acta - Molecular Basis of Disease. 2018;1864(3):900-16.
419
27.
Gorwood P, Lanfumey L, Viltart O, Ramoz N. 5-HT2A receptors in eating
420
disorders. Receptors: Humana Press Inc.; 2018. p. 353-73.
421
28.
Plana MT, Torres T, Rodriguez N, Boloc D, Gasso P, Moreno E, et al. Genetic
422
variability in the serotoninergic system and age of onset in anorexia nervosa and
423
obsessive-compulsive disorder. Psychiatry Res. 2019;271:554-8.
424
29.
Lombardi L, Blanchet C, Poirier K, Lebrun N, Ramoz N, Rose Moro M, et al.
425
Anorexia nervosa is associated with Neuronatin variants. Psychiatr Genet.
426
2019;29(4):103-10.
427
30.
Walton E, Hibar D, Yilmaz Z, Jahanshad N, Cheung J, Batury VL, et al. Exploration
428
of Shared Genetic Architecture Between Subcortical Brain Volumes and Anorexia
429
Nervosa. Mol Neurobiol. 2019;56(7):5146-56.
430
31.
Yan X, Zhao X, Li J, He L, Xu M. Effects of early-life malnutrition on
431
neurodevelopment and neuropsychiatric disorders and the potential mechanisms.
432
Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2018;83:64-75.
433
32.
Kesselmeier M, Putter C, Volckmar AL, Baurecht H, Grallert H, Illig T, et al.
High-434
throughput DNA methylation analysis in anorexia nervosa confirms TNXB
435
hypermethylation. World J Biol Psychiatry. 2018;19(3):187-99.
436
33.
Booij L, Casey KF, Antunes JM, Szyf M, Joober R, Israel M, et al. DNA
437
methylation in individuals with anorexia nervosa and in matched normal-eater
438
controls: A genome-wide study. Int J Eat Disord. 2015;48(7):874-82.
439
34.
Thornton LM, Munn-Chernoff MA, Baker JH, Jureus A, Parker R, Henders AK, et
440
al. The Anorexia Nervosa Genetics Initiative (ANGI): Overview and methods. Contemp
441
Clin Trials. 2018;74:61-9.
442
35.
Duncan L, Yilmaz Z, Gaspar H, Walters R, Goldstein J, Anttila V, et al. Significant
443
Locus and Metabolic Genetic Correlations Revealed in Genome-Wide Association Study
444
of Anorexia Nervosa. Am J Psychiatry. 2017;174(9):850-8.
445
36.
Watson HJ, Yilmaz Z, Thornton LM, Hubel C, Coleman JRI, Gaspar HA, et al.
446
Genome-wide association study identifies eight risk loci and implicates
metabo-447
psychiatric origins for anorexia nervosa. Nat Genet. 2019;51(8):1207-14.
448
37.
Kaye WH, Bulik CM, Thornton L, Barbarich N, Masters K. Comorbidity of anxiety
449
disorders with anorexia and bulimia nervosa. Am J Psychiatry. 2004;161(12):2215-21.
450
38.
Hinney A, Kesselmeier M, Jall S, Volckmar AL, Focker M, Antel J, et al. Evidence
451
for three genetic loci involved in both anorexia nervosa risk and variation of body mass
452
index. Mol Psychiatry. 2017;22(2):192-201.
453
39.
Bulik-Sullivan B, Finucane HK, Anttila V, Gusev A, Day FR, Loh PR, et al. An atlas
454
of genetic correlations across human diseases and traits. Nat Genet.
2015;47(11):1236-455
41.
456
40.
Schroeder M, Jakovcevski M, Polacheck T, Drori Y, Luoni A, Roh S, et al.
457
Placental miR-340 mediates vulnerability to activity based anorexia in mice. Nat
458
Commun. 2018;9(1):1596.
459
41.
Timko CA, DeFilipp L, Dakanalis A. Sex Differences in Adolescent Anorexia and
460
Bulimia Nervosa: Beyond the Signs and Symptoms. Curr Psychiatry Rep. 2019;21(1):1.
461
42.
Hübel C, Gaspar HA, Coleman JRI, Finucane H, Purves KL, Hanscombe KB, et al.
462
Genomics of body fat percentage may contribute to sex bias in anorexia nervosa.
463
American Journal of Medical Genetics, Part B: Neuropsychiatric Genetics.
464
2019;180(6):428-38.
465
43.
Klump KL, Keel PK, Sisk C, Burt SA. Preliminary evidence that estradiol
466
moderates genetic influences on disordered eating attitudes and behaviors during
467
puberty. Psychol Med. 2010;40(10):1745-53.
468
44.
Lilenfeld LR, Kaye WH, Greeno CG, Merikangas KR, Plotnicov K, Pollice C, et al. A
469
controlled family study of anorexia nervosa and bulimia nervosa: psychiatric disorders
470
in first-degree relatives and effects of proband comorbidity. Arch Gen Psychiatry.
471
1998;55(7):603-10.
472
45.
Huckins LM, Hatzikotoulas K, Southam L, Thornton LM, Steinberg J,
Aguilera-473
McKay F, et al. Investigation of common, low-frequency and rare genome-wide
474
variation in anorexia nervosa. Mol Psychiatry. 2018;23(5):1169-80.
475
46.
Curtis D, Adlington K, Bhui KS. Pursuing parity: Genetic tests for psychiatric
476
conditions in the UK National Health Service. British Journal of Psychiatry.
477
2019;214(5):248-50.
478
47.
Himmerich H, Treasure J. Psychopharmacological advances in eating disorders.
479
Expert Review of Clinical Pharmacology. 2018;11(1):95-108.
480
48.
Ramoz N, Gorwood P. Epigenetics, genetics and physiology in anorexia nervosa
481
and remission. European Neuropsychopharmacology. 2019;29:S3-S.
482
49.
Smith AR, Ortiz SN, Forrest LN, Velkoff EA, Dodd DR. Which Comes First? An
483
Examination of Associations and Shared Risk Factors for Eating Disorders and
484
Suicidality. Current Psychiatry Reports. 2018;20(9).
485
50.
Brown M, Loeb KL, McGrath RE, Tiersky L, Zucker N, Carlin A. Executive
486
functioning and central coherence in anorexia nervosa: Pilot investigation of a
487
neurocognitive endophenotype. Eur Eat Disord Rev. 2018;26(5):489-98.
488
51.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred Reporting Items
489
for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Medicine.
490
2009;6(7):e1000097.
491
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
Figure 1. Graphical representation of this reviews’ methodological approach for
525
its bibliography selection (adapted from “The PRISMA Statement” [51])
526
Records identified through PubMed database searching
(n = 21)
Records after duplicates removed (n = 70)
Title and Abstract Screening (n = 70)
Records excluded by no topics of interest
(n = 31)
Studies included in the review (n = 34) Records identified through SCOPUS database searching (n = 59)
Records identified through ISI Web of Science database
searching (n = 24)
Full-text articles assessed for eligibility
(n = 39)
Full-text articles excluded, according to the common agreement of the authors
Table 1. List of all genome-wide significant loci identified in anorexia nervosa until now
527
and their main characteristics. [35, 36]
528
529
Reported by Chromosome Base-pair region Type Number of
genes Start End Duncan et al., 2017 12 56,372,585 56,482,185 Multigenic 6 Watson et al., 2019 1 96,699,455 97,284,455 Single gene 2 2 53,881,813 54,362,813 Multigenic 13 3 47,588,253 51,368,253 Multigenic 111 3 70,670,750 71,074,150 Single gene 2 3 93,968,107 95,059,107 Intergenic 2 5 24,945,845 25,372,845 Intergenic 0 10 131,269,764 131,463,964 Single gene 2 11 114,997,256 115,424,956 Single gene 1
Table 2. Simplified list of significant positive and negative genetic correlations between
530
anorexia nervosa and other phenotypes reported by Duncan et al. and Watson et al..
531
[35, 36]
532
533
a Body mass index
534
b Body fat percentage
535
Duncan et al., 2017 Watson et al., 2019
Sample size 3495 cases 10982 controls 16 992 cases 55 525 controls Si gni fi ca nt ge ne ti c cor re la ti ons Pos it iv e Neuroticism Neuroticism Psychiatric disorders (schizophrenia and cross disorder)
Psychiatric disorders (obsessive-compulsive disorder,
major depressive disorder, schizophrenia, anxiety, depressive
symptoms)
Education (education years and college
attended)
Education (years of education, college
completion, college or university degree) HDL cholesterol HDL cholesterol Physical activity Ne ga ti ve Anthropometric traits (BMIa, BF%b, hip circumference)
Anthropometric traits (BMIa, BF%b, waist and hip
circumference, waist-to-hip ratio)
Fasting insulin and glucose levels
Insulin resistance and fasting insulin levels
Leptin levels Type 2 diabetes
Instructions for Authors 1 INTERNATIONAL JOURNAL OF AND
CLINICAL NEUROSCIENCES
MENTAL HEALTH
INSTRUCTIONS FOR AUTHORS
1. Aims and Scope
The International Journal of Clinical Neurosciences and Mental Health is an open-access peer-reviewed journal published by ARC Publishing.
Our goal is to provide high-quality publications in the areas of Psychiatry and Mental Health, Neurology, Neurosurgery and Medical Psychology. Expert leaders in these medical areas constitute the international editorial board.
The journal publishes original research articles, review articles, drug reviews, case reports, case snippets, viewpoints, letters to the editor, editorials and guest editorials.
The International Journal of Clinical Neurosciences and Mental Health follows the highest scientific standards, such as the CONSORT / STROBE guidelines and the Uniform Requirements for Manuscripts Submitted to Biomedical Journals (ICJME).
The journal offers:
• Trusted peer review process
• Fast submission-to-publication time
• Open-access publication without author fees • Multidisciplinary audience and global exposure
Contents
1. AIMS AND SCOPE 1
2. TYPES OF PAPERS 2
2.1. Original research 2
2.2. reviewsand drug reviews 2
2.3. case repOrtsand case snippets 2
2.4. viewpOints 3
2.5. letterstOthe editOr 3
2.6. editOrialsand guest editOrials 3
3. MANUSCRIPT SUBMISSION 3
3.1. cOver letter 3
3.2. Manuscript preparatiOn 3
3.3. suppOrting infOrMatiOn 6
3.4. subMissiOn checklist 6
4. OVERVIEW OF THE EDITORIAL PROCESS 6
Instructions for Authors 2 INTERNATIONAL JOURNAL OF AND
CLINICAL NEUROSCIENCES
MENTAL HEALTH
2. Types of papers
The International Journal of Clinical Neurosciences and Mental Health publishes scientific articles in the following categories:
• Original Research. • Reviews. • Drug Reviews. • Case Reports. • Case Snippets. • Viewpoints.
• Letters to the Editor.
• Editorials and Guest Editorials.
As an open-access, online-only publication, the International Journal of Clinical
Neurosciences and Mental Health does not enforce arbitrary word count or illustration limits. The journal a provides a recommendation on the length of manuscripts, but authors are welcome to submit manuscripts outside those recommendations if deemed appropriate.
2.1. Original Research
The International Journal of Clinical Neurosciences and Mental Health welcomes original clinical or translational research related with psychiatry, mental health, medical psychology, neurosurgery and neurology.
Reports of randomised clinical trials should follow the CONSORT Guidelines and reports of observational studies should follow with STROBE Guidelines.
Original Research articles are recommended to have up to 4000 words (excluding title page, abstract, acknowledgements, references and tables) and up to 8 illustrations (figures or tables). Submission of supplementary material is encouraged. This may include additional illustrations of study results (both figures and/or tables), video files presenting study results or procedures, study protocol, study database and statistical analysis plan.
2.2. Reviews and Drug Reviews
Review articles on current topics related to psychiatry, mental health, medical psychology, neurosurgery and neurology, as well as CNS-related drugs are welcome. Both invited and unsolicited submissions are accepted.
Review articles are recommended to have up to 5000 words (excluding title page, abstract, acknowledgements, references and tables.). Inclusion of newly designed figures and tables to summarise key points is encouraged. The used of previously published material is subject to the licence agreement of the original publisher, and should generally be avoided. If previously published materials are, nonetheless, included in the illustrations, the authors should procure appropriate authorisation for use from the original publisher prior to submission.
2.3. Case Reports and Case Snippets
Highly meaningful Case Reports are accepted, presenting major educational content or major clinical findings. Case Snippets should describe a diagnosis or therapeutic challenge.
Case Reports and Case Snippets are recommended to have 750–1000 words (excluding title page, abstract, acknowledgements, references and tables) and up to 2 figures or tables.
Instructions for Authors 3 INTERNATIONAL JOURNAL OF AND
CLINICAL NEUROSCIENCES
MENTAL HEALTH
2.4. ViewpointsViewpoints should provide an expert opinion on important topics for medical research or practice, with possibility for covering social and policy aspects. This section encourages dialogue and debate on relevant issues with expert views based on evidence.
Viewpoints are recommended to have 1500–3000 words (excluding title page, abstract,
acknowledgements, references and tables) and can include figures or tables, as deemed appropriate.
2.5. Letters to the Editor
Letters to the Editor should share views on published articles, any findings insufficient for a research article or present ideas on any subject within the scope of the journal.
Letters to the Editor are recommended to have up to 1500 words (excluding title page, abstract, acknowledgements, references and tables) and can include figures or tables, as deemed appropriate.
2.6. Editorials and Guest Editorials
Authors are invited by the Editor-in-Chief to comment on specific topics and express their opinions in the form of Editorials. Nonetheless, interested authors are encouraged to contact the Editor-in-Chief with proposals for writing Editorials.
3. Manuscript Submission
These instructions advise on how the manuscript should be prepared and submitted.
Manuscripts that do not comply with the guidelines will be returned to the authors before being considered for peer-review.
All manuscripts should be prepared in A4-size or US-letter size, in UK or US English throughout the manuscript, a mixture of UK and US English will not be accepted.
Manuscripts should be submitted in *.doc and *.pdf formats, in the appropriate section of the journal website: IJCNMH online submission.
3.1. Cover Letter
A cover letter should be submitted together with the manuscript, in *.doc or *.pdf format, addressed to the Editor-in-Chief, and signed by the author submitting the manuscript.
A template for the cover letter is available for download.
The cover letter should contain statements about originality of your publication, Ethics Committee approval and informed consent (if applicable), conflicts of interest and why in your opinion your manuscript should be published.
3.2. Manuscript Preparation
The manuscript must be divided in 2 files: the Title page (submitted in *.doc format and *.pdf formats) and the Manuscript body (submitted in *.doc and *.pdf formats).
Submitting these 2 files is essential to ensure double-blind peer-review. Failure to provide these 2 files will result in delay in the peer-review process, since the manuscript will be returned to the authors for adjustment.
Instructions for Authors 4 INTERNATIONAL JOURNAL OF AND
CLINICAL NEUROSCIENCES
MENTAL HEALTH
Title pageThis should be submitted as a separate file from your manuscript (to ensure anonymity in the peer review process) and should include:
• Article title.
• Authors’ names, titles (e.g. MD, PhD, MSc, etc.) and institutional affiliations.
• Corresponding author: name, mailing address, telephone and fax numbers, email address. • Keywords (maximum of 10), according to MeSH terms, whenever possible.
• A short title (running head) (up to 70 characters). • Abstract word count (up to 250 words).
• Disclosure of conflicts of interest. Any conflict of interests should be declared. If authors have no declaration it should be written: “The authors declare no conflict of interest”.
Manuscript body:
The Manuscript body must be anonymous, not containing the names or affiliations of the authors. It must be structured in the following order: title, abstract, body text,
acknowledgements, references, tables, and figures captions/legends. The manuscript body should contain the title and the abstract, since the title page is not sent to reviewers during peer-review.
• The text must be formatted as follow: • Arial fonts, size: 11 points.
• Double line spacing (see paragraph menu). • Aligned to the left (not justified).
Showing continuous line numbers on the left border of the page. For MS Word you can add line numbers by going to: Page Layout -> Line Numbers -> select “Continuous”; for OpenOffice: Tools -> Line Numbering -> tick “Show numbering”.
Title
A descriptive and scientifically accurate article title should be provided. Abstract (250 words maximum)
An abstract should be prepared for all types of manuscript, except Editorials.
Abstracts of Original Research articles should be structured as: background/objective, methods, results, and conclusions. If the publication is associated with a registered clinical trial, the trial registration number should be referred at the end of the abstract.
Case-reports should be structured as background/introduction, case report, discussion. Systematic review articles should have a structured abstract with generally the same headings as Original Research articles, whereas narrative review articles can have a structured or
unstructured abstract, as deemed appropriate by the authors.
Abstracts for Viewpoint articles and Letters to the Editor, can have a structured or unstructured abstracts, as deemed appropriate by the authors.
Body text
Original research articles
Original research articles should be structured as follows:
Introduction: Should present the background for the investigation and justify its relevancy. Claims should be supported by appropriate references. Introduction should end by stating the objectives of the study.
Methods: Should allow the reproduction of results and therefore must provide enough detail. Appropriate subheadings can be included, if needed.
Results: Should include detailed descriptions of generated data. This section can be separated into subsections with concise self-explanatory subheadings.
Instructions for Authors 5 INTERNATIONAL JOURNAL OF AND
CLINICAL NEUROSCIENCES
MENTAL HEALTH
the main findings, their clinical relevance, the strengths and limitations of the study, future perspectives with suggestion of experiments to be addressed in the future.
Review articles and Drug Reviews
These types of articles should be organised in sections and subsections, as deemed appropriate by the authors
Case Reports and Case Snippets
These types of articles should be organised in the general following sections: Introduction/ Background, Case Report, Discussion. Subsections should be used as deemed appropriate by the authors
Acknowledgements
This section should name everyone who has contributed to the work but does not qualify as an author. People mentioned in this section must be informed and only upon consent should their names be included along with their contributions. Financial support (with grant number, if applicable) should also be stated here.
References
References citation in the text should be numbered sequentially along the text, within square brackets. The use of a reference management tool (such as Endnote or Reference Manager) is recommended. References must be formatted in Vancouver style.
Only published or accepted for publication material can be referenced. Personal communications can be included in the text but not in the references list.
Tables
Tables should be smaller than a page, without picture elements or text boxes. Tables should have a concise but descriptive title and should be numbered in Arabic numerals. Table footnotes should explain any abbreviations or symbols that should be indicated by superscript lower-case letters on the body table.
Figures
Figures should have a concise but descriptive title and should be numbered in Arabic numerals. If the article is accepted for publication, the authors may be asked to submit higher resolution figures. Copyright pictures shall not be published unless the authors submit a written consent from the copyright holder to allow publishing.
Figures should be tested and printed on a personal printer prior to submission. The printed image, resized to the intended dimensions, is almost a replication of how the picture will look online. It shall be clearly perceived, non-pixelated nor grainy. Only flattened versions of layered images are allowed. Each figure can only have a 2-point white space border, thus cropping is strongly advised. For text within figures, Arial fonts between 8 to 11 points should be used and must be readable. When symbols are used, the font information should be embedded.
Photographs should be submitted as *.eps at high-resolution (300 dpi or more), *.tif or *.pdf. Graphics should be submitted in *.eps or *.pdf format, to allow proper reproduction. MS Office graphics are also acceptable, if submitted in their original, editable formats.
Lines, rules and strokes should be between 0.5-1.5 points for reproducibility purposes. Nomenclature
All units should be in International System (SI). Drugs should be designated by their International Non-Proprietary Name (INN).
Instructions for Authors 6 INTERNATIONAL JOURNAL OF AND
CLINICAL NEUROSCIENCES
MENTAL HEALTH
3.3. Supporting InformationCode of Experimental Practice and Ethics
The minimal ethics requirements are those recommended by the Code of Ethics of the World Medical Association (Declaration of Helsinki). Authors should provide information regarding ethics on patient informed consent, data privacy as well as competing interests. If the authors have submitted a related manuscript elsewhere, they should disclose this information prior to submission.
3.4. Submission Checklist
Please ensure you have addressed the following issues prior submission: • Details for competing interests.
• Details for financial disclosure. • Details for authors contribution.
• Participants informed consent statement.
• Authorisation for use of figures included in the manuscript, not produced by the authors and subject to copyright.
• Authorship, affiliations and email addresses are correct. • Cover letter addressed to the Editor-in-Chief.
• Identification of potential reviewers and their email addresses (to be introduced at the online submission platform).
• Manuscript, figure and tables comply with the author guidelines, including the correct format, SI units and standard nomenclature.
• Separated files for Title page (*.doc+*.pdf) and Manuscript body (*.doc+*.pdf)—4 in total. • Manuscript body does not contain the names or affiliations of the authors, or other
direct-ly identifying information, and contain the title and the abstract.
If you have any questions, please contact the editorial office at [email protected]
4. Overview of the Editorial Process
The International Journal of Clinical Neurosciences and Mental Health aims to provide an efficient and constructive view of the manuscripts submitted to achieve a high quality level of publications. The editorial board is constituted by expert leaders in several areas of medicine particularly in Clinical Neuroscience and Mental Health.
Once submitted, the manuscript is assigned to an editor which evaluates and decides whether the manuscript is accepted for peer-review. At this initial phase, the editor evaluates if the manuscript fulfils the scope of the journal according to the content and minimum quality standards. For peer-review, one or two additional expert field editors will comment on the manuscript and decide on whether it is accepted for publishing with minor corrections or not accepted for publishing. The editor may ask authors to resubmit after revision (minor or major). Decision is based on technical and scientific merits of the work. Reviewers can be asked to be disclosed or stay anonymous. Authors can exclude specific editors or reviewers from the process, upon submission, a rational should be provided.
Upon evaluation, an email is sent to the corresponding author with the decision. If accepted, the manuscript enters the production process. It takes approximately 2-4 weeks for the
Instructions for Authors 7 INTERNATIONAL JOURNAL OF AND
CLINICAL NEUROSCIENCES
MENTAL HEALTH
4.1. Appeal ProcessThe editors will respond to appeals from authors which manuscripts were rejected. Their interests should be sent to the Editor.
Two directions can be followed:
• If the Editor does not accept the appeal, further right to appeal is denied.
• If the Editor accepts the appeal, a further review will be asked. After the new review, the editor can reject or accept the appeal. If rejected, nothing else can be done, if accepted the author is able to resubmit the manuscript.
The reasons for not accepting a manuscript for consideration can be: • The manuscript does not follow the scope of the journal.
• The manuscript has potential interest but there are methodological concerns after peer-re-view or editorial examination.
![Síntese e caracterização do carbeto misto de nióbio e tântalo nanoestruturado a partir da columbita [(Fe,Mn)(Nb,Ta)2O6]](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)