DOI:10.1590/2317-1782/20162015253
CoDAS 2016;28(5):640-645
Systematic Review
Revisão Sistemática
What we know of the central auditory
disorders in children exposed to alcohol
during pregnancy? Systematic review
O que sabemos das alterações auditivas
centrais em crianças expostas ao álcool na
gestação? Revisão sistemática
Humberto de Oliveira Simões1
Sthella Zanchetta1
Erikson Felipe Furtado1
Keywords
Speech, Language and Hearing Sciences
Hearing
Electrophysiology
Auditory Perception Alcohol-related disorders
Descritores
Fonoaudiologia
Audição Eletroisiologia Percepção Auditiva
Transtornos Relacionados ao Uso de Álcool
Correspondence address: Sthella Zanchetta
Departamento de Oftalmologia, Otorrinolaringologia e Cirurgia de Cabeça e Pescoço, Hospital das Clínicas, Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo – USP
Avenida Bandeirantes, 3900, 12º andar, Monte Alegre, Ribeirão Preto (SP), Brazil, CEP: 14049-900. E-mail: [email protected]
Received: October 14, 2015
Accepted: March 01, 2016 Study carried out at “Faculdade de Medicina de Ribeirão Preto – FMRP, Universidade de São Paulo – USP” -
Ribeirão Preto (SP), Brazil.
1 Universidade de São Paulo – USP - Ribeirão Preto (SP), Brazil.
Financial support: Conselho Nacional de Desenvolvimento Cientíico e Tecnológico – CNPq, Process: 162123/2014-0.
Conlict of interests: nothing to declare. ABSTRACT
Purpose: To identify the effects of alcohol intake during pregnancy on the central auditory nervous system in relation to their possible diagnosis, Fetal Alcohol Syndrome, partial Fetal Alcohol Syndrome, Alcohol-Related Birth Defects and Alcohol-Related Neurodevelopmental Disorder, his extension and the hearing assessment method. Research strategy: Systematic and integrative review searched the databases PubMed, LILACS and SciELO, with terms in Portuguese and English “fetal alcohol syndrome”, “alcohol-related disorders” associated with “hearing”. Selection criteria: We identiied 123 abstracts, six were selected and published until May 2015. Data analysis: Were listed topics to be answered, characterization of the sample; the diagnosis result of fetal exposure; method of hearing assessment and described results. Results: Among the behavioral assessments, Verbal Dichotic Tests with syllables and sentences and Speech in Noise Test, were used. Among the electrophysiological tests, the Brainstem Auditory Evoked Potential was detected change neural synchrony, and Long-Latency Auditory Evoked Potential – P300, early latency values. Conclusion: There is evidence that children exposed to alcohol in utero present central auditory nervous system involvement signals, but it was not possible to identify the inluence of different subtypes and their losses. Cortical auditory pathways were the most investigated and the electrophysiological method as used with an unexpected result in two of them, early N2 and P300 latency.
RESUMO
INTRODUCTION
The diagnosis of the effects of alcohol intake during pregnancy at birth or during child development is still a challenge(1,2).
The events described by Jones and Smith in the early 1970s(3)
included changes in pre- and/or post-natal development such
as facial dysmorphia (undeined philtrum, palpebral issures, thin upper lip, lattened face) and dysfunction of the central
nervous system (CNS) (intellectual disabilities and/or attention
deicit). The aforementioned authors(3) named this set of signs
Fetal Alcohol Syndrome (FAS), and some of these events had been described earlier by Lemoine et al(4).
With the documentation of new cases of FAS, it was observed that the signs initially described were not always present all together and, when they were present, severity levels varied, thus the term Fetal Alcohol Spectrum Disorder (FASD) was proposed(5). Manifestations of this condition
include neurological abnormalities characterized by behavioral disorders, neuropsychomotor development delay, intellectual impairment, and sensory and perceptual changes(6-9). There
are other labels under the umbrella term FASD owing to the heterogeneity of manifestations: Partial Fetal Alcohol Syndrome (pFAS), Alcohol-Related Birth Defects (ARBD), and Alcohol-Related Neurodevelopmental Disorder (ARND)(1).
Therefore, it is possible to infer that the impact of FAS/FASD on child development results from the extension and severity of manifestations which, in turn, can be related to the dose and time of maternal exposure to the drug(10).
Sensory damages described in the population with FAS/FASD include conductive and sensorioneural hearing losses, which occur in 70% - 77% and 29% of cases, respectively(11-14). The signiicant presence of conductive hearing loss may be
associated with the occurrence, in the same population, of craniofacial deformities, including cleft palate(15), which are
known etiologies for this type of loss(16).
Central auditory nervous system (CANS) impairment in
FAS was irst described in the 1990s by means of auditory,
behavioral and electrophysiological assessments(12). Altered
results were found in 15% of children in the Brainstem Auditory Evoked Potential (BAEP) and in 100% of children in behavioral assessments such as Verbal Dichotic Tests.
The occurrence of an abnormal neurophysiological representation of the sound stimulus in the CANS is named Auditory Processing Disorder (APD)(17). Currently, it is
recommended that its diagnostic evaluation be conducted through a set of electrophysiological and behavioral tests, with verbal and nonverbal stimuli(12). These recommendations are
supported by a better understanding of the neural mechanisms involved in behavioral and electrophysiological tests, including component P300 and Mismatch Negativity (MMN).
Considering the variability of FAS/FASD manifestations and their severity, the diagnostic assessment of auditory potentials can be useful because it describes the origin and extension of the APD, and this characterization is essential
to the management of an individual therapeutic intervention program.
OBJECTIVE
In view of the harmful impact of FAS/FASD on child development, the present literature review aims to identify the effects of alcohol intake during pregnancy on the CANS in relation to the possible different diagnoses of the condition, the hearing assessment method, and event-related characterization.
RESEARCH STRATEGY
A systematic, integrative search was conducted at the PubMed, LILACS, and SciELO databases using the following terms in Portuguese: “síndrome fetal do álcool”, “desordens relacionadas ao uso do álcool”, “audição”; and in English: “fetal alcohol syndrome”, “alcohol-related disorders” associated with “hearing”.
SELECTION CRITERIA
In the irst phase, the following criteria were established
for the reading of abstracts: inclusion: a) studies in humans, b) children, adolescents, and young adults with a history of fetal alcohol exposure, c) studies without a time limit published until May 31, 2015, d) available abstract, e) citation of hearing assessment in the same abstract, and f) publication in English, Portuguese, or Spanish; exclusion: a) literature reviews, b) letters and editorials, and c) case reports. In the second phase, the following new exclusion criteria were established for the reading in full of the selected works: absence of one of the possible diagnoses for fetal alcohol exposure (FASD, FAS, pFAS, ARBD, ARND) and absence of description of the hearing assessment procedure.
DATA ANALYSIS
The selected papers were analyzed by two speech-language
pathologists. After analysis, they illed in a spreadsheet with
the following information: a) author and year; b) type of study and level of evidence; c) sample description; d) diagnosis of fetal alcohol exposure; e) description of the auditory
function assessment method and its classiication: behavioral
vs. electrophysiological; f) hearing assessment outcomes; and g), in the presence of abnormal results, impairment extension: subcortical vs. cortical. To underpin the interpretation regarding
the methodological design of each of the articles, a classiication
criterion of evidence levels, from 1 to 5, was adopted according to the Oxford Centre for Evidence-based Medicine – Levels of Evidence (March 2009)(18). Subsequently, to identify the possible
generalization of the results found, each text was also rated according to grade of recommendation(18). The spreadsheets
CoDAS 2016;28(5):640-645
Simões HO, Zanchetta S, Furtado EF 642
was read in full by both examiners. If disagreement persisted, a third health professional was consulted.
RESULTS
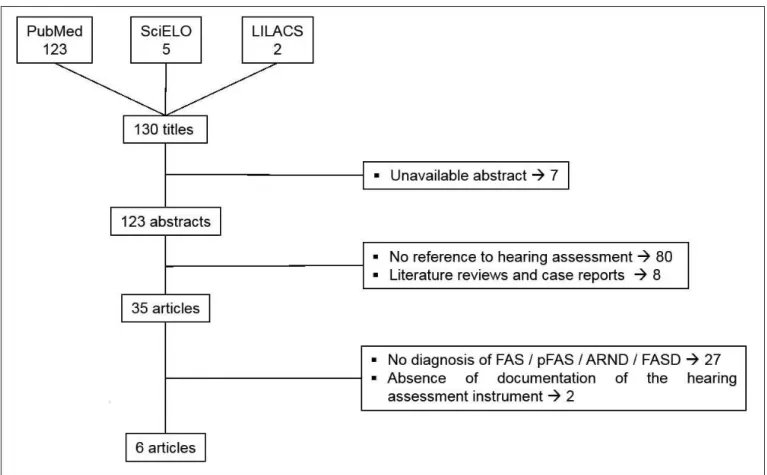
Based on the selected search terms, 130 titles were identiied,
from those 123 abstracts were found. After reading and application of the inclusion and exclusion criteria, 35 articles, 26.9% (35/130) of the total, were selected. Upon reading the abstracts, the examiners found that 27 (79%) articles did not present a description of the diagnosis of the individual exposed to alcohol during pregnancy, only a reference to it, and that two (0.5%) articles used auditory cognitive assessment subtests for the outcome of the auditory processing disorder; therefore, these 29 articles were excluded from the study.
Figure 1 shows a lowchart of the search conducted at the
scientiic databases.
Eventually, six articles were identiied and summarized according to the survey questions (Chart 1).
FAS/FASD AND ITS SUBTYPES AND LEVELS OF EVIDENCE
The six selected studies addressed the diagnostics of individuals exposed to alcohol during pregnancy, four of them(12,13,19,20) exclusively on FAS, one of them(21) on FAS and
pFAS, and one(22) on FAS, pFAS and ARND. Of the four studies
that addressed diagnostics exclusively on FAS, three were from the 1990s(12,13,19), and the two studies that used the sub-labels
of the FAS/FASD (21,22) were published in the year or after the
guiding publications, with guidelines on the theme(23-24).
All six papers used a sample of individuals with partial or
complete FAS, which represent a proile of greater clinical severity
within FASD(21). Although children with the complete syndrome are associated with proiles of higher alcohol consumption during
pregnancy(21), the respective articles did not report information
on the characteristics of alcohol use by the mother.
All selected studies were conducted using the cross-sectional design. None of them presented longitudinal and/or cohort characteristics, but four of them(19-22) used control groups for
comparison with the study groups. The cross-sectional study with a control group shows level of evidence “3” and grade of recommendation “B”(19-22). The other two papers(12,13) show level
of evidence “4” and grade of recommendation “C”. It is worth mentioning that 66.6% (4/6) of the articles, those with grade of recommendation “B” (19-22), presented credible outcomes, that is,
their results can be generalized for the studied conditions and should be used for clinical decision making. The studies with grade of recommendation “C”(12,13) suggest that conditions may
be clinically different from those used in the study(19).
Caption: FAS = Fetal Alcohol Syndrome; pFAS = Partial Fetal Alcohol Syndrome; ARND = Alcohol-Related Neurodevelopmental Disorder; FASD = Fetal Alcohol Spectrum Disorder
CoD
A
S
2016;
28(5):
640-645
l a
udi
tory pa
thw
ays
a
nd a
lc
ohol
e
xpos
ure
643
Chart 1. Characterization of the studies that investigated the central auditory pathways in children exposed to alcohol during pregnancy
Author/Year Study design Sample Diagnostics
Levels of evidence and grades of recommendation*
Diagnostic evaluation: behavioral vs. electrophysiological
vs. electroacoustic
Subcortical vs.
cortical Outcomes
Stephen et al.(22) - Cross-sectional - Case control
10 children exposed to alcohol
15 control children Age: 3 - 6 years
FASD (FAS, pFAS, ARND)
Level of evidence: 3b Grade of
recommendation: B
Electromagnetic technique with Oddball paradigm
Cortical Increased latency between the groups.
Steinmann et al. (21)
- Cross-sectional - Case control
24 children exposed to alcohol
20 control children Age: 11 - 15 years
FAS and pFAS
Level of evidence: 3b Grade of
recommendation: B
Electrophysiological with Oddball paradigm
Complex P2-N2-P3
Cortical
N2 with greater latency in frequent stimulus in the study group Frequent vs. rare stimuli; the study group presented earlier N2 in the rare stimulus; this outcome was not observed in the control group.
Damelöf et al.(20) - Cross-sectional - Case control
11 children exposed to alcohol
14 control children Age: 8 - 17 years
FAS
Level of evidence: 3b Grade of
recommendation: B
Behavioral
Verbal dichotic test Cortical
Children with FAS presented right ear advantage less frequently (considering the pairing of hand dominance).
Church et al.(12) - Cross-sectional
22 children exposed to alcohol
Age: 3 - 26 years
FAS
Level of evidence: 4 Grade of
recommendation: C
Electrophysiological and behavioral BAEP
Test of everyday attention and speech-in-noise test
Subcortical and Cortical
15% of the 22 assessed individuals presented altered BAEP outcomes. 100% of the 12 individuals who underwent behavioral assessment presented altered outcomes.
Kaneko et al.(19) - Cross-sectional - Case control
18 children exposed to alcohol
18 children with Down Syndrome
18 control children Age: 8 years (mean)
FAS
Level of evidence: 3b Grade of
recommendation: B
Electrophysiological
N1 and P3 Cortical
The P300 with lowest values of amplitude and latency in the study group with the active electrode in the active electrode in the frontal region.
Rössig et al.(13) - Cross-sectional 36 children exposed to
alcohol FAS
Level of evidence: 4 Grade of
recommendation: C
Electrophysiological
BAEP Subcortical
21% with altered outcomes due to the changes in the neural structures of the auditory pathway.
More frequent alteration, greater latency of the V wave, or even absence, and increased latency of the III wave. *Oxford Centre for Evidence-based Medicine – Levels of Evidence (March 2009)(18)
CoDAS 2016;28(5):640-645
Simões HO, Zanchetta S, Furtado EF 644
EVALUATION OF CENTRAL AUDITORY PATHWAYS
Only one study(12) used both behavioral and electrophysiological techniques on the hearing assessment. For the other selected
works, one article(20) used behavioral evaluation and three
papers(13,19,20) applied electrophysiological measurement.
There was another only study(22) in which the authors chose
magnetoencephalography (MEG) with Oddball paradigm to investigate the cortical activation of auditory stimuli.
The following behavioral assessments were used: verbal dichotic listening test (VDT) with syllables(20), competing
sentence test (CST) in contralateral mode, and speech-in-noise test (SNT)(12). Verbal dichotic listening tests are commonly
associated with cortical auditory disorders, whereas the SNT is susceptible to both cortical and subcortical disorders(25,26);
nevertheless, there are signs that noise attenuation begins at the superior olivary complex(27). VTD(20) was employed to investigate
the right ear advantage (REA), a sign commonly present in right-handed individuals(25) that relects the dominance of the
left hemisphere for linguistic sounds. The authors(20) reported that REA occurred less frequently compared with the control
group pairing the number of right-handed individuals in both groups. Changes in the outcomes of CST and SNT(12) were
found in 100% of the individuals assessed (n=12), with an initial sample of 22 individuals; the authors reported that only 12 of the 22 study participants attended the behavioral hearing
assessment, with no further speciications.
Four of the six selected articles used auditory evoked potentials(12,13,19,21). Brainstem Auditory Evoked Potential (BAEP)
was chosen in two studies(12,13), both addressed the diagnosis
of FAS, with the outcomes suggesting that alteration in neural synchrony was similar between them, 21%(13) and 15%(12).
The two studies also described increasing interpeak latencies involving waves III and V as a suggestive sign of abnormality, that is, dysfunction involving the superior olivary complex and lateral lemniscus/inferior colliculus(28).
The other two studies used the recording of late or long latency potentials(19,21): the irst survey(19) analyzed components
N1 and P300 and observed that children with FAS presented smaller amplitude and latency at P300 compared with those of the control group with the active electrode in the frontal position; whereas the latter article(21) used the recording of
components P2, N2 and P300 and observed that the children exposed to alcohol during pregnancy presented greater latency
at N2 in the recording of the frequent stimulus compared with
those of the control group. They also compared the variables
in each group with respect to the frequent and rare stimuli and veriied that component N2 presented difference in the latencies,
with early latency in the rare stimulus - a result not observed for the control group.
The sites generated by the long-latency auditory evoked potentials (LLAEP) are not accurate; however, it has been accepted that component P2 have its origin, not only but also, in the thalamic region, with extensions of the limbic and reticular systems(29,30). P300 is considered an endogenous component
dependent on the attentional process, considering that it demands
a mental or motor task for a given sound stimulus, called rare. Its multiple generators are located in the thalamus, hippocampus, and frontal cortex(29,30).
Only one study associated the different types and diagnoses of fetal alcohol exposure with the assessment outcome(22). The authors
recorded the sound stimuli by means of magnetoencephalography (MEG) with Oddball paradigm and observed that children exposed to alcohol during pregnancy presented increased latency compared with those of the control group, but the subtypes of the spectrum (FAS, pFAS and ARND) were not included in
the analysis. Increased latency was identiied in components
M1 and M2, which correspond to the superior temporal gyrus area. An important aspect for consideration of the hearing assessment of CANS is that, in addition to intrauterine exposure to alcohol, there are other known risk factors for its dysfunction(16). These
factors include, but are not limited to, hyperbilirubinemia with levels for exchange transfusion, Apgar score, and bacterial or viral infections. Although the selected articles report the occurrence of other risk factors for these types of alterations, they did not identify them, and did not mention the possibility of risk factor overlapping(12,13,19).
CONCLUSION
Children and young adults exposed to alcohol in utero present central auditory nervous system (CANS) impairment
signs, but no inluence of the different FAS/FASD subtypes on these losses was identiied. The cortical auditory pathways were
the most investigated and the electrophysiological assessment was the most used method, with unexpected results for early N2 and P300 latencies. Only one study associated behavioral
and electrophysiological techniques on the hearing assessment.
REFERENCES
1. Hoyme HE, May PA, Kalberg WO, Kodituwakku P, Gossage JP, Trujillo PM, et al. A practical clinical approach to diagnosis of fetal alcohol spectrum
disorders: clarification of the 1996 institute of medicine criteria. Pediatrics. 2005;115(1):39-47. PMid:15629980.
2. Benz J, Rasmussen C, Andrew G. Diagnosing fetal alcohol spectrum disorder: history, challenges and future directions. Paediatr Child Health.
2009;14(4):231-7. PMid:20357921.
3. Jones KL, Smith DW. Recognition of the fetal alcohol syndrome in early
infancy. Lancet. 1973;302(7836):999-1001. PMid:4127281. http://dx.doi. org/10.1016/S0140-6736(73)91092-1.
4. Lemoine P, Harousseau H, Borteyru JP, Menuet JC. Les enfants des parents alcoholiques: anomalies observées, a propos de 127 cas. Quest Med. 1968;21:476-82.
5. Streissguth AP, O’malley K. Neuropsychiatric implications and long-term consequences of fetal alcohol spectrum disorders. Semin Clin Neuropsychiatry. 2000;5(3):177-90. PMid:11291013. http://dx.doi.org/10.1053/scnp.2000.6729.
6. Momino W, Sanseverino MT, Schüler-Faccini L. Prenatal alcohol exposure as a risk factor for dysfunctional behaviors: the role of the pediatrician. J Pediatr (Rio J). 2008;84(4):S76-9. PMid:18758654. http://dx.doi.org/10.1590/
7. Cancino FT, Zegarra J. Síndrome alcohólico fetal. Rev Neuropsiquiatr. 2003;66(4):302-12. http://dx.doi.org/10.20453/rnp.v66i4.1556.
8. Burd L, Cotsonas-Hassler MT, Martsolf JT, Kerbeshian J. Recognition and management of fetal alcohol syndrome. Neurotoxicol Teratol. 2003;25(6):681-8. PMid:14624967. http://dx.doi.org/10.1016/j.ntt.2003.07.020. 9. Cohen-Kerem R, Bar-Oz B, Nulman I, Papaioannou VA, Koren G. Hearing
in children with fetal alcohol spectrum disorder (FASD). Can J Clin Pharmacol. 2007;14(3):e307-12. PMid:18025546.
10. Coles CD, Kable JA, Keen CL, Jones KL, Wertelecki W, Granovska IV, et al. Dose and Timing of prenatal alcohol exposure and maternal
nutritional supplements: developmental effects on 6-month-old infants. Matern Child Health J. 2015;19(12):2605-14. PMid:26164422. http://
dx.doi.org/10.1007/s10995-015-1779-x.
11. Church MW, Abel EL. Fetal alcohol syndrome: hearing, speech, language, and vestibular disorders. Obstet Gynecol Clin North Am. 1998;25(1):85-97. PMid:9547761. http://dx.doi.org/10.1016/S0889-8545(05)70359-4.
12. Church MW, Eldis F, Blakley BW, Bawle EV. Hearing, language,
speech, vestibular, and dentofacial disorders in fetal alcohol syndrome. Alcohol Clin Exp Res. 1997;21(2):227-37. PMid:9113257. http://dx.doi. org/10.1111/j.1530-0277.1997.tb03754.x.
13. Rössig C, Wässer S, Oppermann P. Audiologic manifestations in fetal alcohol
syndrome assessed by brainstem auditory-evoked potentials. Neuropediatrics. 1994;25(5):245-9. PMid:7885533. http://dx.doi.org/10.1055/s-2008-1073029.
14. Church MW, Gerkin KP. Hearing disorders in children with fetal alcohol syndrome: findings from case reports. Pediatrics. 1988;82(2):147-54.
PMid:3399287.
15. Cone-Wesson B. Prenatal alcohol and cocaine exposure: influences on cognition, speech, language, and hearing. J Commun Disord. 2005;38(4):279-302. PMid:15862811. http://dx.doi.org/10.1016/j.jcomdis.2005.02.004. 16. Joint Committee on Infant Hearing. Year 2007 Position statement: principles
and guidelines for early hearing detection and intervention programs. Pediatrics. 2007;120(4):898-921. PMid:17908777. http://dx.doi.org/10.1542/
peds.2007-2333.
17. AAA: American Academy of Audiology. Clinical practice guidelines:
diagnosis, treatment and management of children and adults with central auditory processing disorder [Internet]. Reston: AAA; 2010 [citado em 2014
Fev 18]. Disponível em: http://audiology.org/resources/documentlibrary/ Pages/CentralAuditoryProcessingDisorder.aspx
18. Phillips B, Ball C, Sackett D, Badenoch D, Straus S, Haynes B, et al. Oxford Centre for Evidence-Based Medicine levels of evidence. Oxford: Centre
for Evidence-Based Medicine; 2009 [citado em 2014 Fev 18]. Disponível em:
http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/
19. Kaneko WM, Ehlers CL, Philips EL, Riley EP. Auditory event-related
potentials in fetal alcohol syndrome and Down’s syndrome children. Alcohol Clin Exp Res. 1996;20(1):35-42. PMid:8651459. http://dx.doi. org/10.1111/j.1530-0277.1996.tb01040.x.
20. Domellöf E, Rönnqvist L, Titran M, Esseily R, Fagard J. Atypical functional lateralization in children with fetal alcohol syndrome. Dev Psychobiol.
2009;51(8):696-705. PMid:19768741. http://dx.doi.org/10.1002/dev.20404.
21. Steinmann TP, Andrew CM, Thomsen CE, Kjær TW, Meintjes EM, Molteno CD, Jacobson JB, Jacobson SW, Sorensen HB. An auditory Go/No-Go
study of event-related potentials in children with fetal alcohol spectrum
disorders. In: Conference of the IEEE Engineering in Medicine and Biology
Society; 2011; Boston. Piscataway: Engineering in Medicine and Biology
Society; 2011. p. 789-92.
22. Stephen JM, Kodituwakku PW, Kodituwakku EL, Romero L, Peters
AM, Sharadamma NM, et al. Delays in auditory processing identified in
preschool children with FASD. Alcohol Clin Exp Res. 2012;36(10):1720-7.
PMid:22458372. http://dx.doi.org/10.1111/j.1530-0277.2012.01769.x.
23. Stratton KR, Howe CJ, Battaglia FC, editors. Fetal Alcohol syndrome:
diagnosis, epidemiology, prevention, and treatment. Washington, DC:
National Academy Press: 1996.
24. Chudley AE, Conry J, Cook JL, Loock C, Rosales T, LeBlanc N. Fetal
alcohol spectrum disorder: Canadian guidelines for diagnosis. CMAJ :
Canadian Medical Association Journal. 2005;172(5, Supl Suppl):S1-21. PMid:15738468. http://dx.doi.org/10.1503/cmaj.1040302.
25. Kimura D. Cerebral dominance and the perception of verbal stimuli. Can
J Psychol. 1961;15(3):166-71. http://dx.doi.org/10.1037/h0083219.
26. Musiek FE, Chermak GD, organizadores. Handbook of (Central) auditory
processing disorder. San Diego: Plural Publishing; 2007. (Auditory
Neuroscience and Diagnosis; 1).
27. Boer J, Thornton AR, Krumbholz K. What is the role of the medial olivocochlear
system in speech-in-noise processing? J Neurophysiol. 2012;107(5):1301-12. PMid:22157117. http://dx.doi.org/10.1152/jn.00222.2011.
28. Möller AR, Jannetta P, Bennett M, Möller MB. Intracranially recorded
responses from human auditory nerve: new insights into the origin of brainstem
evoked potentials. Electroencephalogr Clin Neurophysiol.
1981;52(1):18-27. PMid:6166449. http://dx.doi.org/10.1016/0013-4694(81)90184-X.
29. Hall JW. New handbook of auditory evoked responses. Boston: Ally &
Bacon; 2006.
30. McPherson DL. Long latency auditory evoked potentials. In: McPherson
DL. Late potentials of the auditory system. San Diego: Singular Publishing
Group; 1996. p. 7-21.
Author contributions