Revist a de Saúde Pública
I SSN 0034- 8910 versão im pressaRev Saúde Pública 2003; 37(6)
WH O Q O L- OLD Project: m ethod and focus group results in Braz i l
Mar celo P A Flecka, Eduar do Chacham ov icha and Clarissa M Trent inib,*
aGrupo WHOQOL- OLD Cent ro Brasileiro. Port o Alegre, RS, Brasil. bDepartam en t o de Psiquiat r ia e Medicina Legal da Universidade Federal do Rio Grande do Sul. Port o Alegre, RS, Brasil
ABSTRACT
Ba ckground
Ex plor ing t he condit ions t hat allow sat isfact or y qualit y of life in old age is an issue of scient ific and social r elev ance.
Objectives
T o descr ibe a qualit y of life assessm ent m et hod for t he elder ly and pr esent t he r esult s fr om focus groups conduct ed am ong old people in good healt h and ill healt h, as w ell as t heir caregivers.
M ethods
Results
A t endency t ow ar ds m ak ing an associat ion bet w een qualit y of life and w ellbeing and feeling w ell w as obser v ed. The r esponses spont aneously included t he 6 dom ains proposed in WHOQOL- 100, t hus cor r obor at ing t he m ult idim ensional nat ur e of t his const r uct ion. Ninet een out of t he 24 or iginal facet s of t his inst r um ent w er e cit ed as r elev ant , and t he fiv e facet s not spont aneously r em em ber ed w er e not concent r at ed in a single dom ain. When quest ioned about t he im por t ance of each of t he 24 facet s of WHOQOL- 100, t he gr oups consider ed all of t hem t o be r elev ant . How ev er , suggest ions for m odificat ions t o fiv e facet s w er e m ade. Addit ional it em s w er e also ex am ined and considered relevant for assessing qualit y of life am ong t he elder ly , by bot h t he old people and t he car egiv er s.
Conclusions
The r esult s cor r obor at e t he hy pot hesis t hat old people const it ut e a par t icular gr oup and, as such, t hey hav e r elev ant specific char ac t er ist ics. Thus, an appr opr iat e inst r um ent for assessing qualit y of life am ong t he elder ly needs t o consider such m at t er s.
Keywords
Aged. Qualit y of life. Focus gr oups. Car egiv er s. Old people’s healt h.
I N TRODUCTION
The aging of t he populat ion is a r elat iv ely new phenom enon all ar ound t he w or ld. Accor ding t o dat a fr om t he Wor ld Healt h Or ganizat ion ( WHO) , life ex pect ancy for t he w hole w or ld, w hich t oday is 66 y ear s, w ill becom e 73 y ear s by 2025.5 I n Br azil, t he pr ospect for t he y ear 2030 is t hat t her e w ill be a populat ion of around 25 m illion old people.1 0 Prelim inary dat a from t he lat est dem ographic census7 ( I BGE, 2000) show t hat around 10 m illion people am ong t he Brazilian populat ion are over 65 year s old.
Wit hin t his r ealit y , t her e is a need for specific st udies am ong adv anced age gr oups by healt hcar e pr ofessionals.
From t he beginning of t he 1990s, t he WHO observed t hat qualit y of life m easur em ent s t ook on par t icular im por t ance in healt h assessm ent s, bot h fr om t he indiv idual and social per spect iv es.9 Ther e ar e sev er al scales for assessing qualit y of life. How ev er , t hey differ in r elat ion t o t heir under ly ing co n cep t ual aspect s and t he im por t ance giv en t o subj ect iv it y , t o t he det r im ent of obj ect iv it y in choosing r esponses t o t he it em s inv est igat ed. They also differ r egar ding t he nat ur e and w eight of each dom ain for assessing qualit y of life as a r esour ce for gener at ing con cept s per t in en t t o t h e populat ion in quest ion, for subsequent v er ificat ion v ia a psy chom et r ic focus.6 , 3 , 1 1 Becau se of su ch par t icular aspect s, t he im por t ance of ut ilizing qualit at ive m et hods has been highlight ed.
The Wor ld Healt h Or ganizat ion Qualit y of Life Group ( WHOQOL Group) has developed a scale w it hin a cr oss- cult ur al per spect iv e for m easur ing qualit y of life am ong adult s. The subj ect iv e char act er of qualit y of life ( encom passing bot h posit iv e and negat iv e aspect s) and it s m ult idim ensional nat ur e hav e been consider ed fundam ent al char act er ist ics. Ther e is now int er est w it hin t he WHOQOL Gr oup in developing an inst rum ent for evaluat ing qualit y of life am ong elderly adult s. Such int erest is j ust ified by t h e fact t h at it is n ot possible t o assu m e t h at inst r um ent s t hat ar e suit able for assessing t he field of physical healt h am ong young adult s, for exam ple, are t he sam e or appropriat e for populat ions of elder ly adult s. Specific m at t er s pr obably need t o be addr essed for each age gr oup. I n addit ion t o t his, t he m agnit ude of t he aging phenom enon, t oget her w it h t he scar cit y of inst r um ent s for ev aluat ing su ch qu est ion s, st r en gt h en s su ch in t er est .
The pr esent st udy for m s par t of a w ider pr oj ect t hat inv olv es 16 ot her cent er s: Scot land ( coor dinat ing cent er ) , England, Germ any, Spain, Denm ark, France, Czech Republic, Hungary, Finland, Canada, Aust r alia, Unit ed St at es, I sr ael, Japan, Sw eden, China and also t he Eur opean office of t he WHO, as well as t he Brazilian cent er of WHO’s Qualit y of Life Group.
The WHOQOL- OLD proj ect has t w o m ain obj ect iv es:
To develop an inst rum ent for assessing qualit y of life am ong elderly adult s ( WHOQOL- OLD) , from t he st art ing point of qualit y of life m easurem ent s for younger adult s ( WHOQOL- 100) , recent ly published in it s original version ( WHOQOL Group,1 2 1998) and also in t he form of t he Brazilian version.4
To ut ilize WHOQOL- OLD in an innovat ory cross- cult ur al pr oj ect t hat w ill com par e t he aging t hat t ak es place w it h good healt h and ill healt h.
For t his, t he m et hodology and act ion st r at egy for t he pr oj ect w ill follow a ser ies of clear ly defined st eps t hat have alr eady been ut ilized in t he developm ent of ot her m odules w it hin WHOQOL. I n sum m ar y , t hese st eps include: 1) r ev iew of t he WHOQOL inst r um ent ; 2) conduct ing of focus gr oups; 3) pilot m odule for WHOQOL- OLD; 4) collect ion of dat a for t he pilot ; 5) analy sis of t he pilot dat a; 6) m odule for t he field t est ; 7) pr oduct ion of a quest ionnair e for ev aluat ing " At t it udes in r elat ion t o aging" ; 8) field t est ; 9) analy sis of t he dat a fr om t he field t est ( t est ing t he possibilit y for an abbreviat ed version of WHOQOL- OLD) ; 10) publicat ion and dissem inat ion of t he result s.
The inv olv em ent of each cent er , t hr ough w or k ing w it h t his m et hod and apply ing it in t he differ ent languages of t he par t icipat ing count r i es, w ill allow w ide- ranging developm ent of WHOQOL for elderly adult s.
Thus, t he pr esent ar t icle has t he obj ect iv e of descr ibing t he m et hod for conduct ing focus gr oups on qualit y of life am ong t he elderly in Brazil, and t he result s from t his.
Fiv e f ocus gr oups w er e conduct ed in Br azil, and t hese follow ed an int er nat ionally st andar dized m et hodology ( WHOQOL Gr oup, 1995) . I n addit ion t o t his, four pr ofessionals w ho w er e par t icular ly involved in car ing for t he elder ly w er e int er view ed individually. Thus, t he gr oups fur nished concept s fr om dist inct angles r egar ding v ar ious aspect s of qualit y of life am ong t he elder ly . The fiv e focus gr oups w er e com posed as follow s: healt hy old people aged 60- 80 years, sick old people aged 60- 80 y ear s, healt hy old people aged over 80 year s, sick old people aged over 80 year s, and car egiver s.
Subjects
The sam pling of subj ect s w as done accor ding t o conv enience, w hile follow ing select ion cr it er ia t hat encom passed differ ent subpopulat ions of t he elder ly . The healt hy old people in bot h age gr oups w er e r ecr uit ed fr om a com m unit y choir for t he elder ly t hat is par t of a univ er sit y ex t ension pr oj ect . On t he ot her hand, t he sick old people aged 60- 80 years were select ed during t heir int ernm ent in a universit y gener al hospit al. The sick old people aged over 80 years were recruit ed from an old people’s hom e t hat ser v es as a t r aining ar ea for m edical st udent s. The gr oup of car egiv er s w as m ade up of individuals connect ed w it h t he old people’s hom e or r ecom m ended by it . The cr it er ion for choosing t he r ecr uit m ent locat ions w as t heir ease of access r esult ing fr om t heir link w it h univ er sit y ser v ices.
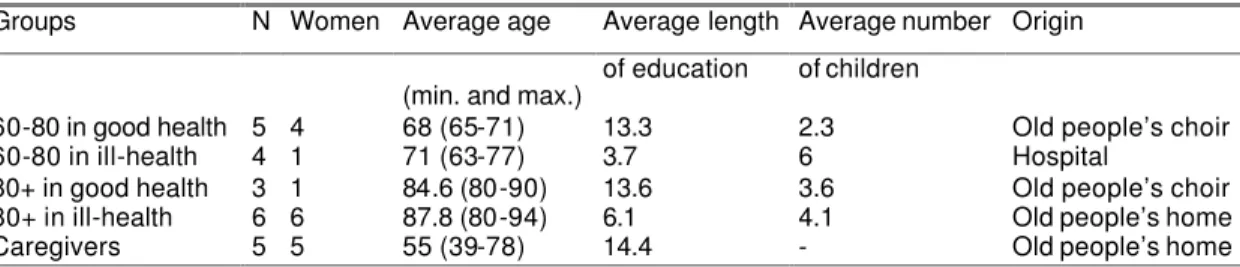
Thus, 18 elder ly people and fiv e car egiv er s par t icipat ed in t he focus gr oups, as show n in Table 1. The cr it er ion of t he indiv idual’s subj ect iv e opinion of his or her healt h w as ut ilized as t he m eans for classify ing t his per son as healt hy or sick . This choice w as based especially on t he subj ect iv e pr inciple t hat t he WHO qualit y of life assessm ent inst r um ent s ar e based on. The elder ly people w as ask ed dir ect ly w het her t hey consider ed t hem selv es t o be healt hy or sick , j ust befor e conduct ing t he focus gr oups, and t heir r esponses defined w hich gr oup t hey w ould be allocat ed t o.
Table 1 – Description of the characteristics of focus group participants.
Groups N Women Average age Average length Average number Origin
of education of children (min. and max.)
60-80 in good health 5 4 68 (65-71) 13.3 2.3 Old people’s choir 60-80 in ill-health 4 1 71 (63-77) 3.7 6 Hospital
80+ in good health 3 1 84.6 (80-90) 13.6 3.6 Old people’s choir 80+ in ill-health 6 6 87.8 (80-94) 6.1 4.1 Old people’s home
Caregivers 5 5 55 (39-78) 14.4 - Old people’s home
Pr ocedur es for conduct ing t he focus gr oups
All t he gr oups obser v ed t he pr e - est ablished m et hodology d escr ibed in t he follow ing:
Et hical aspect s: t he pr oj ect w as ex am ined and appr ov ed by t he Et hics Com m it t ee of Hospit al de Clínicas de Por t o Alegr e. All t he par t icipant s inv olv ed in t he st udy w er e adequat ely infor m ed and agr eed in adv ance t o t ak e par t in it . Even when inform ed of t he possibilit y of int errupt ion during t he gr oup, none of t hem gav e up or r efused t o par t icipat e.
Coor dinat ion: t his w as done by a pr ofessional w it h ex per ience of conduct ing gr oups, accom panied by an assist ant . The lat t er w as r esponsible for t ape- r ecor ding t he gr oup discussions and t yping t he cont ent of w hat t he par t icipant s w er e ex pr essing, in a com put er at t hat locat ion.
Recor dings: at t he end of each gr oup discussion t her e w as a com put er ized r ecor d of t he cont ent of t he gr oup discussion and a com plet e audio r ecor d, fr om t he beginning t o t he end of each gr oup. The t ap e- r ecor der w as sw it ched on r ight at t he st ar t of t he gr oup discussion and w as only sw it ched of f aft er all par t icipant s had left t he locat ion. Such obser v at ion allow ed t he r ecor ding of any m anifest at ion t hat m ight have been m ade aft er t he for m al t er m inat ion of t he gr oup discussion.
Dur at ion: t he av er age dur at ion of t he gr oup discussions w as 120 m inut es. This lengt h of t im e allow ed all t he t hem es t o be adequat ely dealt w it h, but w it hout causing fat igue, loss of at t ent ion or disper sion of t h e par t icipan t s.
Descr ipt ion of t he act iv it ies dur ing t he gr oup discussion: t o begin w it h, t he coor dinat or used open quest ions t o put for w ar d t he concept , i. e. w hat can im pr ov e or w or sen qualit y of life and w hat is m ost im por t ant for it . This st age of t he discussion last ed 20 m inut es on av er age. Follow ing t his, t he gr oup r ead and exam ined t he definit ion of each dom ain and each of t he it em s in WHOQOL- 100,4 guided by t he coor dinat or . The r elev ance of t hese dom ains for t he par t icipant s’ liv es and t he suit abilit y of t he for m ulat ion of t he quest ions ( such as clar it y , v ocabular y and conciseness) w er e inv est igat ed. This st ag e of dev eloping t he gr oup discussion last ed ar ound 60 m inut es. The t hir d st age of conduct ing t he gr oups w as dedicat ed t o suggest ions of ot her t opics consider ed r elev ant for qualit y of life t hat w er e not dealt w it h in t he original quest ionnaire original. The obj ect iv e of t h is st age w as t o gen er at e n ew it em s t hat could be added t o t hose alr eady under st ood by t he par t icipant s as being r elev ant . The best w ay of for m ulat ing quest ions on such it em s w as also exam ined w it h t he elder ly par t icipant s.
RESULT S
Th e gr oup discussions r an t heir cour se in an at m ospher e of am icable and calm cooper at ion. The par t icipant s show ed sat isfact ion about being able t o discuss specific aspect s of qualit y of life for t heir age gr oups. They ex pr essed t heir cont ent m ent in seeing t hat t he ir experiences w ould be t aken int o account and t hat t her e w as int er est in st udy ing old people. Ther e had been a cer t ain appr ehensiv eness am ong t he r esear cher s t hat t he elder ly people, especially t hose aged ov er 80 y ear s, w ould not be w illing or be in a condit ion t o par t icipat e in an act iv it y t hat r equir ed a high lev el of concent r at ion and abst r act ion for ar ound t w o hour s, w hich w as not bor ne out . The old people k ept up t heir int er est and par t icipat ion t hr oughout t he gr oup discussions.
A sum m ar y of t he cont ribut ions t hat em er ged fr om t he focus gr oups is pr esent ed in Tables 2 t o 4.
Table 2 – Summary of focus group discussions – responses to general questions on quality of life: positive and negative aspects.
Focus groups Definition of quality of life
What is important for quality of life?
What harms your wellbeing?
What would improve your quality of life?
60-80 in ill-health Wellbeing, money, feeling well.
Health, giving social support to others.
Not being allowed to help, health problems.
60-80 in good health Having happiness in life, love and friendship.
Having voluntary activities, religion, health, good relationships with the family, an activity, support from others, activities with other old people, learning, reading and eating well.
Lack of work opportunities, politics, lack of respect towards the elderly, lack of attention to the health and education systems, lack of sense of humor.
80+ in ill-health Independence, the head working well, freedom and health.
Health (especially mental), motivation, contact with the children and grandchildren, eating well, money.
Illness, pain, anxiety. Eating well, walks, friendship, prayers, being capable of helping others and obtaining gratitude, health, being in a good physical condition, having the possibility of sharing feelings. 80+ in good health Health, spirituality,
having good living conditions.
Participating in some social organization, feeling happy.
Lack of interest, marital problems, not having a good relationship with the family.
Having the desire to do things.
Caregivers Living well (without illnesses), having intellectual activities, expectations for the future, being respected.
Lack of attention and love, difficulties in keeping up with technological
advances.
Being valued, preparation of the young for dealing with old age, love and contact from the family, motivation for learning.
The r esponses t o t he gener al quest ions pr esent ed in Table 2 cam e fr om open quest ions r elat ed t o t he definit ion and posit iv e and negat iv e aspect s of qualit y of life. The idea t hat qualit y of life consist s of a m ult idim ensional const r uct ion becam e ev ident fr om t he het er ogeneit y of t he v ar ious m at t er s cont ained in t he r esponses. Ther e w as a t endency t o m ak e an associat ion bet w een qualit y of life and w ellbeing or feeling w ell. Aspect s of qualit y of life consider ed im por t ant by all t he gr oups of elder ly people w er e also highlight ed, such as healt h, sociabilit y , social suppor t , phy sical act iv it y , t he possibilit y of giving support and t he feeling of usefulness. Som e groups indicat ed religious belief, st able financial condit ions and good liv ing condit ions as im por t ant fact or s in qualit y of life.
The r esponses spont aneously cov er ed all t he six dom ains pr oposed in WHOQOL- 100, t hus dem onst r at ing t hat t hey ar e gener ically appr opr iat e for invest igat ing t he qualit y of life am ong t he elder ly . Of t he 24 or iginal facet s of t his inst r um ent , 19 w er e cit ed as being r elev ant t o t he int er view ees’ qualit y of life. The it em s “ sleep and r est ” ( phy sical dom ain) , “ body im age and appear ance” ( psy chological dom ain) , “ sex ual act iv it y ” ( social r elat ionship dom ain) , “ t r anspor t at ion” ( environm ent al dom ain) and “ dependence on m edicat ion or t reat m ent ” ( level of independence dom ain) w er e not spont aneously r emem ber ed by t he old people. Thus, t hese unr em em ber ed facet s w er e not cent er ed on a single dom ain.
Table 3 – Revision of the items in WHOQOL-100. Synthesis of the comments from the old people and caregivers’ focus groups.
Groups Domain 1: Domain 2: Domain 3: Domain 4: Domain 5: Domain 6: Physical Psychological Level of
independence Social relationships
Environment Spirituality, religious belief and personal beliefs 60-80 in
ill-health Body image and appearance: it was suggested that the elderly should accept the changes in body image secondary to aging. Dependence on medication or treatment: medication was regarded as a factor for improvement in quality of life.
60-80 in good health
Energy and fatigue: it was suggested that the point to which the physical limitations can be tolerated should be evaluated.
Sleep and rest: it was emphasized that the need for sleep diminishes among the elderly. Memory and concentration: some participants indicated that this item is no longer relevant. Dependence on medication or treatment: medication was regarded as a factor for improvement in quality of life.
80+ in ill-health Pain and discomfort: it was indicated that the tolerance of pain is greater among the elderly.
Capacity for work: this was not
considered so important for the elderly. The possibility for recreation is more relevant than work. Sexual activity: there were divergences in relation to the relevance of this item for the elderly.
80+ in good health Pain and discomfort: it was suggested that the importance that pain takes on in individuals’ lives should be evaluated. Negative feelings: it was suggested that the term depression is too specific and does not substitute for negative feelings. Dependence on medication or treatment: the predominant opinion was that taking medications worsens the quality of life.
Sexual activity: the group did not reach a consensus regarding the importance of this item. Transportation : this item was not
be evaluated. feelings.
Caregivers
Energy and fatigue: it was suggested that this item is even more important among the elderly than among the young. Body image and appearance: it was suggested that physical signs like wrinkles are not as important as eyesight problems, for example. Dependence on medication or treatment: there is an impression that medications have a positive connotation for the elderly.
Capacity for work: it was indicated that difficulty in working affects men more than women. Sexual activity: it was observed that the question assumes that there is sexual activity, which is not always true among the elderly.
Physical environment: there was a special observation regarding noise. Spirituality/reli gion/personal beliefs: it was observed that some old people begin to give more importance to religion in their old age, especially when they have some serious illness.
When quest ioned about t he im por t ance of each of t he 24 facet s of WHOQOL- 100, t he groups consider ed t hem all t o be r elev ant . How ev er , fiv e facet s m er it ed m odificat ion for applicat ion t o t he elderly: a) body im age and appear ance; b) capacit y for w or k ; c) negat iv e feelings; d) sex ual act iv it y ; and e) dependence on m edicat ion or t r eat m ent . I n t he facet body im age and appear ance, t her e w er e t w o fundam ent al differences in relat ion t o t he original form ulat ion of WHOQOL- 100 for adult s: an em phasis on t he accept ance of t he m odificat ions r esult ing fr om t he age and giv ing v alue t o good bodily funct ioning t o t he det r im ent of it s appear ance. Wit h r egar d t o t he facet capacit y for w or k , t he old people’s em phasis was on t ak ing adv ant age of t he t im e t hr ough useful or enj oy able act iv it ies. The hy pot hesis w as r aised t hat t his facet w ould be m or e per t inent t o m en t han t o w om en. I n t he facet negat iv e feelings, t he em phasis on depr ession as a negat iv e feeling, t o t he det r im ent of ot her feelings t hat w er e also negat iv e and could be pr esent , w as consider ed ex cessiv e. The facet sex ual act iv it y w as t he m ost polem ical and gener at ed m ost cont r ov er sy . Som e par t icipant s consider ed t his t o be irrelevant for old people, w hile ot hers cons ider ed it t o be v er y r elev ant . I t w as suggest ed t hat t he quest ion should be for m ulat ed in such a w ay as t o not pr esuppose t hat sex ual act s w er e necessar ily t ak ing place, but t hat act iv it ies such as car essing and phy sical cont act ( k isses and hugs) should also be consider ed. The facet dependence on m edicat ion or t r eat m ent w as cr it icized because dependence on m edicat ion or t r eat m ent could be seen bot h as a fact or in t he w or sening of qualit y of life, due t o t he dim inut ion of aut onom y, and also as an im provem ent t hr ough t he beneficial effect t hat som e m edicat ion and/ or t r eat m ent pr ovide.
Table 4 – Additional items proposed that were considered relevant by the focus groups.
Sensory function (e.g. eyesight, hearing);
Communication: opportunity to talk to other people;
Memory; capacity to think, concentrate and make decisions;
Relationships – with friends and family;
Opportunity for social contact (going out and meeting people);
Housing situation;
Feeling of social isolation;
Financial matters;
Work satisfaction: paid or voluntary work;
Facing up to losses: friends or members of the family;
Significant life events (e.g. retirement or becoming a grandparent);
Importance of eating well/having a good appetite;
Opportunity for leisure activities/recreation;
Importance of having achievements recognize d.
D ISCUSSION
Accor ding t o Ner i,8 it w as only in t he 1 9 9 0 s t hat old age “ w it h disease” ceased t o be r egar ded as sy nony m ous w it h old age as a w hole, bot h by science and cult ur e. Recent epidem iological t r ends, su ch as t h e gr ow t h in t h e n u m ber s of h ealt h y old people, ar e for cing a change in t he t heor et ical pr esupposit ion t hat old age is sy nony m ous w it h disease.
Accor ding t o Br ow ne et al,2 each populat ion of elder ly people w ill giv e par t icular v alue t o cer t ain dom ains. Nonet heless, old people hav e quest ions t hat can be gener alized but differ fr om t hose of t he general adult populat ion. Bowling,1 w it h an int erest in asking old people w hat t hey deem ed im port ant in det erm ining qualit y of life, int erviewed a populat ion from a com m unit y of different ages, wit h and w it hout illnesses. This aut hor found t hat t he elder ly only differ ed fr om t he ot her age groups in at t r ibut ing lesser im por t ance t o phy sical w or k act iv it ies and gr eat er w eight t o healt h t han y ounger people did.
I n t he pr esent st udy , t he per cept ion of t he need for addit ional it em s t hat w as obser v ed in t he focus gr oups cor r obor at es t he hy pot hesis t hat t he elder ly const it ut e a par t icular gr oup and, as such, pr esent r elev an t specific ch ar act er ist ics.
REFEREN CES
1 . Bowling A. What t hings are im port ant in people's lives? A survey of t he public's j udgem ent s t o infor m scales of healt h r elat ed qualit y of life. Soc Sci Med 1995; 41: 1447- 62.
2 . Browne JP, O'Boyle CA, McGee HM, Joyce CR, McDonald NJ, O'Malley K et al. I ndividual qualit y of life in t he healt hy elder ly. Qual Life Res 1994; 3: 235- 44.
3 . Farquar M. Elderly people's definit ions of qualit y of life, 1995. Soc Sci Med 1995; 41: 1439- 46.
4 . Fleck MPA, Fachel O, Louzada S, Xav ier M, Chacham ov ich E, Vieir a G, et al. Desenv olv im ent o da v er são em por t uguês do inst r um ent o de av aliação de qualidade de v ida da Or ganização Mundial da Saúde ( WHOQOL- 100) , 1999. Rev ABP/ APAL 1999; 21: 19- 28.
5 . Forlenza OV, Caram elli P. Neur opsiquiat r ia ger iát r ica. São Paulo: Edit or a At heneu; 2000.
6 . Fundação I nst it ut o Br asileir o de Geogr afia e Est at íst ica ( 2000) . Av ailable at h t t p: / / w w w . ibge. gov . br [ Accessed 20 Jan 2003]
7 . George LK, Bearon LB. Qualit y of life in older per sons: m eaning and m easur em ent . New Yor k : Hum an Sciences Press; 1980.
8 . Neri AL. Qualidade de v ida e idade m adur a. Cam pinas: Papirus; 1993.
9 . Orley J, Kuyken W, edit ors. Qualit y of life assessm ent : int er nat ional per spect iv es, 1994. Heidelberg: Springer Verlag; 1994. p. 41 - 60.
11. The WHOQOL Gr oup. The w or ld healt h or ganizat ion qualit y of life assessm ent : posit ion paper from t he World Healt h Organizat ion, 1995. Soc Sci Med 1995; 41: 1403 - 9 .
12. The WHOQOL Group. The World Healt h Organizat ion qualit y of life assessm ent ( WHOQOL) : developm ent and general psychom et ric propert ies, 1998. Soc Sci Med 1998; 46: 1569- 85.
Address to correspondence
Mar celo PA Fleck
Depart am ent o de Psiquiat ria e Medicina Legal da UFRGS Rua Ram iro Barcelos, 2.350 4º andar
90035 - 003 Port o Alegre, RS, Brazil E- m ail: m fleck .v oy @t er r a.com .br
Financed by FI PE. Hospit al de Clínicas de Port o Alegre
( Pr oj ect n. 0 1 .3 7 4 )
* Post gr aduat e st udent at doct or at e lev el. Post gr aduat e psy chiat r y pr ogr am of t he Feder al Univ er sit y of Rio Grande do Sul.
Received on 13/ 9/ 2002. Review ed on 4/ 7/ 2003. Approved on 14/ 7/ 2003.
© 2 0 0 3 Fa cu lda de de Sa ú de Pú blica da Un ive r sida de de São Paulo
Ave n ida D r . Ar n a ldo, 7 1 5 0 1 2 4 6 - 9 0 4 Sã o Pa u lo SP Br a zil
Te l./ Fa x : + 5 5 1 1 3 0 6 8 - 0 5 3 9