www.jped.com.br
ORIGINAL
ARTICLE
Analysis
of
contextual
variables
in
the
evaluation
of
child
abuse
in
the
pediatric
emergency
setting
夽
Ana
Nunes
de
Almeida
a,
Vasco
Ramos
a,∗,
Helena
Nunes
de
Almeida
b,
Carlos
Gil
Escobar
b,
Catarina
Garcia
baUniversidadedeLisboa,InstitutodeCiênciasSociais,Lisboa,Portugal
bHospitalProfessorDoutorFernandodaFonseca,DepartamentodePediatria,UnidadedeUrgênciaeCuidadosIntensivos,
Amadora,Portugal
Received3June2016;accepted14September2016 Availableonline27April2017
KEYWORDS Physicalviolence; Sexualviolence; Children; Portugal; Hospitalurgency
Abstract
Objective: This article comprises a sample of abuse modalities observed in a pediatric emergencyroomofapublichospitalintheLisbonmetropolitanareaandamultifactorial char-acterizationofphysicalandsexualviolence.Theobjectivesare:(1)todiscusstheimportance ofsocialandfamilyvariablesintheconfigurationofbothtypesofviolence;(2)toshowhow physicalandsexualviolencehavesubtypesandinternaldiversity.
Methods: A statistical analysis was carried outin a database (1063 records of childabuse between2004and2013).Aformwasappliedtocaseswithsuspectedabuse,containingdataon thechild,family,abuseepisode,abuser,medicalhistory,andclinicalobservation.Afactorial analysisofmultiplecorrespondencewasperformedtoidentifypatternsofassociationbetween socialvariablesandphysicalandsexualviolence,aswellastheirinternaldiversity.
Results: Theprevalenceofabuseinthispediatricemergencyroomwas0.6%.Physicalviolence predominated(69.4%),followedbysexualviolence(39.3%).Exploratoryprofilesofthesetypes ofviolencewereconstructed.Regardingphysicalviolence,thegenderoftheabuserwasthe firstdifferentiatingdimension;thevictim’sgenderandagerangewerethesecondone.Inthe caseofsexualviolence,theageoftheabuserandco-residencewithhim/hercomprisedthe firstdimension;thevictim’sageandgendercomprisedtheseconddimension.
Conclusion: Patternsofassociationbetweenvictims,familycontexts,andabuserswere iden-tified.Itisnecessarytoalertcliniciansabouttheimportanceofsocialvariablesinthemultiple facetsofchildabuse.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
夽
Pleasecitethisarticleas:AlmeidaAN,RamosV,AlmeidaHN,EscobarCG,GarciaC.Analysisofcontextualvariablesintheevaluation ofchildabuseinthepediatricemergencysetting.JPediatr(RioJ).2017;93:374---81.
∗Correspondingauthor.
E-mail:[email protected](V.Ramos). http://dx.doi.org/10.1016/j.jped.2016.09.005
PALAVRAS-CHAVE Violênciafísica; Violênciasexual; Crianc¸as; Portugal;
Urgênciahospitalar
Análisedasvariáveiscontextuaisnaavaliac¸ãodosmaus-tratosinfantisapartir
darealidadedeumaurgênciapediátrica
Resumo
Objetivo: Esteartigoapresentaumacasuísticademodalidadesdemaus-tratosnumaUrgência Pediátrica(UP)deumhospitalpúbliconaÁreaMetropolitanadeLisboaeumacaracterizac¸ão multifatorialdaviolênciafísicaeviolênciasexual.Osobjetivossão:1)discutiraimportância devariáveissociaisefamiliaresnaconfigurac¸ãodeambos;2)mostrarcomoviolênciafísicae violênciasexualapresentamsubtiposediversidadeinterna.
Métodos: Realizou-seumaanáliseestatísticadeumabasededados(1063registosde maus-tratosinfantis, entre2004-2013).Utilizou-seoformulárioaplicadoacasos comsuspeitade maus-tratos, comdadossobreacrianc¸a,família,episódiodemaus-tratos, agressor,história médicaeobservac¸ãoclínica.Foirealizadaumaanálisefatorialdecorrespondênciasmúltiplas paraidentificarpadrõesdeassociac¸ãoentrevariáveissociaiseviolência,físicaesexual,bem comosuadiversidadeinterna.
Resultados: Aprevalênciademaus-tratosnestaUPfoide0,6%.Predominamaviolênciafísica (69,4%)eaviolênciasexual(39,3%).Perfisexploratóriosdestestiposforamconstruídos.Quanto à violênciafísica,osexo do agressorestruturaaprimeira dimensãodiferenciadora; sexoe grupoetáriodavítimaestruturamasegunda.Nocasodaviolênciasexual,aidadedoagressor ecoresidênciacomeleestruturamaprimeiradimensão;idadeesexodasvítimasorganizama segundadimensão.
Conclusão: Identificaram-sepadrõesdeassociac¸ãoentrevítimas,contextosfamiliarese agres-sores.Énecessário alertarosclínicos paraaimportânciadasvariáveissociais nasmúltiplas facesqueosmaus-tratosassumem.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
In its several forms, child abuse remains a characteristic thataffectscontemporarychildhoodonaworldwidescale. Itoccursinavarietyofcontexts,particularlythosewhere thechildshouldbesaferandmoreprotected(family,home, school,institutionswherecare isprovided).1Itis amajor
causeofchildhoodmorbidity andmortality,andits
conse-quencesforthedevelopmentandwell-beingofchildrenare
devastating.1,2
It is estimated that 4---16% of children in high-income
countriesarephysicallyabusedandoneintensuffers
psy-chological violence or neglect.3 According to the World
HealthOrganization(WHO),18millionchildreninEuropeare
victimsofsexualviolence,44million,ofphysicalviolence,
and55million,ofpsychologicalviolence;approximately850
childrendieeachyearasaresultofthesetypesofabuse.4
Theactualityandseverityofthisproblempersists,3despite
child protection policies developed internationally since
the 1970s.5 In a scenario of greater social intolerance to
such situations,6 the contribution of researchersand
pro-fessionals is crucial so that decision-makers can promote
adjustedpublicpolicies(forinformationregistration,
train-ingoftechnicians,prevention,intervention,andfollow-up
inthefield).
In the last decade, Portugal has implemented specific
policiesonchildsafety,allowingthecountrytomake
signif-icantprogressinthisarea.However,reliablenationaldata
arenotyetavailabletoallowafullandaccurateassessment
ofthesituation.
Aimingtoovercomethelackofstudiesinthearea,this
article presents a seriesof maltreatment modalities in a
pediatricemergencyroom(PER)unitofapublichospitalin
Lisbonandamultifactorialcharacterizationofthetwomost
frequenttypes,physicalviolence,andsexualviolence.The
objectivesare(1)todiscusstheimportanceof familyand
socialvariables(e.g.,gender ofvictimsandabusers,type
ofrelationship,time)intheconfigurationofbothtypesof
abuse;(2) toshowhowphysical andsexualviolence have
subtypesandinternaldiversity.
Definitions
Inline withthe ConventionontheRightsof theChild,an individualyoungerthan18yearsisconsidereda‘‘child’’.In 1999,theWHOdefinedchildabuseasallformsofphysical oremotional abuse,sexualviolence, neglect,or commer-cialexploitationthatresultsinactualorpotentialharmto thechild’shealth,survival,development,ordignityinthe contextofarelationshipofresponsibility,trust,orpower.6It
considersasphysicalviolenceanactionbyanycaregiverthat
causesactualorpotentialphysicalharmtothechild.Sexual
violenceisanactinwhichthecaregiverusesthechildfor
hisorhersexualgratification. Emotionalviolenceincludes
the failure by the caregiver to provide a child-friendly
environment(e.g.,restrictingmovement,threatening,
ridi-culing, intimidating, discriminating, rejecting, and other
non-physicalformsofhostiletreatment),7whichadversely
impactsthechild’sdevelopmentandemotionalhealth.
intimidationand continuousabuseofachild overanother
whohasnochancetodefendhimorherself.8,9
Neglectorabandonmentisdefinedasthecaregiver’s
fail-uretoensurethechild’sdevelopmentinareasconsideredto
bevital,suchashealth,education,emotionaldevelopment,
nutrition,shelter,andsafety.8
Methods
Participants
Thisstudyincludedrecordsof1063childrenoveraten-year period(from2004 toOctober 2010, aged 0---16 yearsand fromthelastdateuptoage18),identifiedasallegedvictims ofsomeformofchildabuse(bythepatienthimorherself, his/hercaregiver,ortheattendingphysician),whocameto, orwerereferencedtothePERunitofthehospital.
Tools
Asdatacollectioninstrument,aspecificformwasusedfor caseswithsuspectedabuse,filledoutbythemedicalteam during the emergency episode. This is a semi-structured questionnairethat contains dataon thechild and his/her family,theabuseepisode,theabuser,medicalhistoryand clinicalobservation,andthesubsequentrecommendations forthesituation.Thecollectiondependedontheinterview andobservationperformedbytheattendingclinicianinthe PERunitand,thus,thereissomeheterogeneityinthe com-pletionofthesocialfields.
Procedures
The variables ofthe collectiontool, ona paperform(up to 2011) and computer file (from 2011 onwards), were retrospectivelyinserted intoa computerizeddatabase for posterior analysis by the multidisciplinary team (Hospi-tal Support Center for at-Risk Child and Youth). Data includedthevictim’scharacteristics(gender,age,household composition,personalhistoryofchronicdiseases,domestic violenceintheusualdomicile),theabuser’scharacteristics (genderand age,relationship withthe victim),and abuse (dateofoccurrence,typeofabuse),aswell asthe subse-quentlyimplementedmeasures.
Statistical
analysis
Firstly,thestudysamplewasbrieflydescribed.Exploratory models were then constructed, containing the two most frequent types of abuse in the sample: physical violence (64.2%)andsexualviolence(39.3%).Themodelsarebased onthemultiplecorrespondencefactorialanalysis,usingthe optimal scaling method.10,11 This technique aims to
ana-lyze associationsbetween variables in a multidimensional
space, summarizing informationabout a large number of
category variables, facilitating the understanding of how
they organize themselves into specific patterns. For the
numerical variables with normal distribution, the means
andthestandarddeviationswerecalculated.Forthe
varia-bles without normal distribution, the median, minimum
andmaximumvalueswerecalculated.Thechi-squaredtest
wasusedforthecomparativeanalysesincategorical
varia-bles. This technique does not replace any predictive or
riskmodel.StatisticalanalyseswereperformedusingSPSS
Statistics®(IBMSPSSStatisticsforWindows,Version24.0.NY,
USA).
Ethicalconsiderations
Thedatacollectionduringtheclinicalprocessisperformed bytheclinicianafterverbalconsentprovidedbythechild’s oradolescent’scaregiverinthePERunit,accordingtothe law.Theproceduresforcollecting,processing,and analyz-ingdatawereapprovedbytheHospitalEthicsCommitteeof thePERunit.
Results
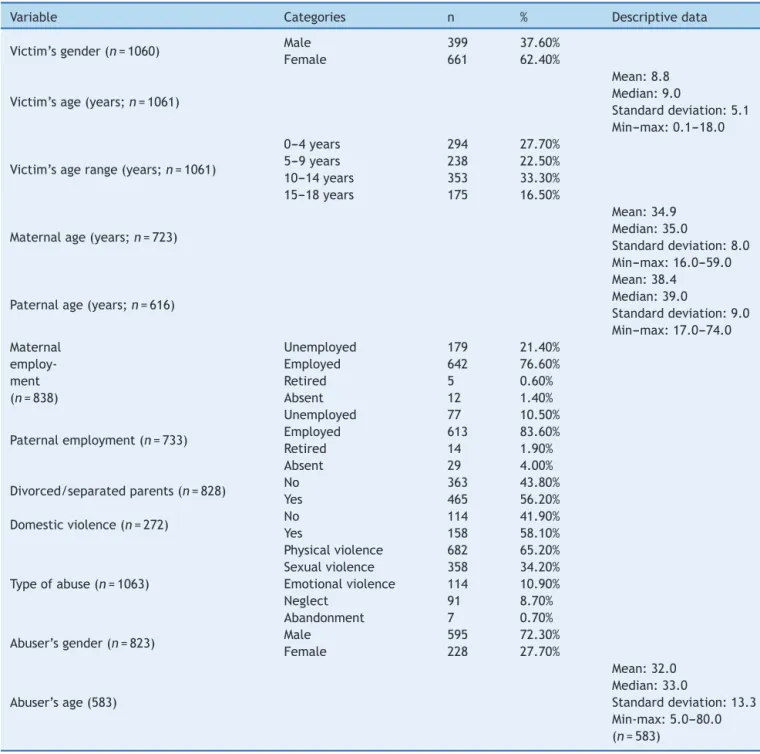
Duringthestudyperiod,1063casesofabusewererecorded, corresponding to 0.6% of occurrences in this PE. Most of thevictimswerefemale(62.4%)andthemeanagewas8.8 years(SD±5.1).Overall,mostepisodesoccurredinchildren aged10---14years(32.7%).Femalevictimstendedtobeolder (mean=9.4,SD±5.0).Mostofthemalevictimswereaged 0---4yearsold(32.5%).Regardingthevictims’parents,the meanageofthemotherswas35years(SD±8),whereasthe meanage ofthefatherswas38years(SD±9).Mostwere employed(83.6%offathersand76.6%ofmothers)andmore thanhalf(56.2%)weredivorcedorseparated.In158cases, therewasa reportof domestic violence in thehousehold wherethechildusuallylived.
Physicalviolence wasthe most common typeof abuse (69.4%),followedbysexual(39.3%)andemotionalviolence (22.2%). In 8.7% of the cases,the assessed children were victims of neglect and in 0.7% of cases, they had been abandoned.Mostoftheabusersaremales(72.3%),witha meanageof 32years(SD±13.3).Withslightvariationsin theirrelativeweight,thisisthepatterntypicallyseenina PERunit,12,13differentfromwhatisfound,forinstance,at
theChildandYouthProtectionCommissions(Comissõesde
Protec¸ãodeCrianc¸aseJovens [CPCJ]),whereneglectand
emotionalviolencearethemostfrequentlyrecordedtypes
(Table1).14
Timeintroducesothercharacterizationpatterns.Despite
theannualvariations(thelongitudinalanalysisdidnot
con-sider theyear2004, sincetheformwasnotin useonthe
beginningofthatyear),therewasanincreasingtrendinthe
numberofcasesdetected.Buttheannualevolutionpertype
ofabuseisdifferentiated.Thenumberofcasesofsexual
vio-lencehasremainedstable,withpeaksin2007and2012.As
forthecasesofemotionalviolence,theyhaveincreasedin
recentyears(Fig.1).
The analysis of the monthly distribution of reported
episodes of violence indicates a cumulative mean of 83
occurrences. The monthly variation, which refersto
sea-sonalrhythmsofsociallife,issignificant:thereweremore
casesinthespringandsummermonths(March,May,June,
July, September, and October) and fewer cases in late
autumn and winter (November, December, and January).
Physical violence was the most common type of abuse
Table1 Samplecharacteristics.
Variable Categories n % Descriptivedata
Victim’sgender(n=1060) Male 399 37.60%
Female 661 62.40%
Victim’sage(years;n=1061)
Mean:8.8 Median:9.0
Standarddeviation:5.1 Min---max:0.1---18.0
Victim’sagerange(years;n=1061)
0---4years 294 27.70%
5---9years 238 22.50%
10---14years 353 33.30%
15---18years 175 16.50%
Maternalage(years;n=723)
Mean:34.9 Median:35.0
Standarddeviation:8.0 Min---max:16.0---59.0
Paternalage(years;n=616)
Mean:38.4 Median:39.0
Standarddeviation:9.0 Min---max:17.0---74.0 Maternal
employ-ment (n=838)
Unemployed 179 21.40%
Employed 642 76.60%
Retired 5 0.60%
Absent 12 1.40%
Paternalemployment(n=733)
Unemployed 77 10.50%
Employed 613 83.60%
Retired 14 1.90%
Absent 29 4.00%
Divorced/separatedparents(n=828) No 363 43.80%
Yes 465 56.20%
Domesticviolence(n=272) No 114 41.90%
Yes 158 58.10%
Typeofabuse(n=1063)
Physicalviolence 682 65.20%
Sexualviolence 358 34.20%
Emotionalviolence 114 10.90%
Neglect 91 8.70%
Abandonment 7 0.70%
Abuser’sgender(n=823) Male 595 72.30%
Female 228 27.70%
Abuser’sage(583)
Mean:32.0 Median:33.0
Standarddeviation:13.3 Min-max:5.0---80.0 (n=583)
Source:Emergencysignformfortheabusedchild(2004---2013).
inDecember(monthsthatcoincidewithschoolholidaysand children staying at home).Emotional violence cases were morecommoninthelasttwomonthsoftheyear(November andDecember).
Exploratory
profiles
of
physical
violence
and
sexual
violence
Exploratoryprofilesoftheassociationbetweensocial varia-blesandthemostcommontypesofabuseweredelineated usingtheFAMC.TheresultsareshowninFigs.2and3.
Varia-blesassociatedwiththevictimandwiththeabuser(gender
andagegroup)andfamilycontext(divorced/separated
par-ents)wereincluded.
Asforphysicalviolence,theabuser’sgenderconstitutes
thefirstdimension,whilethevictim’sgenderandagegroup
constitutesthesecond one (Fig. 2).The abuser’s ageis a
factorthatmediatesthesetwoelements.
Afirstprofileofphysicalviolencewasidentified,inwhich
victimsandabusersareadolescents(lowerright-hand
cor-ner),insituationsofpeerviolence(i.e.,bullying)occurring
bothinsideandoutside theschoolsettings.Asecond
pro-file(lowerleft-handcorner)correspondstomaleabusers,
tendingtobeolder,whoattackvictims,especiallyfemales,
96 95 89 128 132 115 111 107 128
1 1 0 2 1 0 0 2 0
30 24 34 44 45 36 31 55 45
12 10 10 9 11 11 5 6 11
15
4 6 8 2 6
24 15 29 58 70 61 86 85 76 75 61 79 0 20 40 60 80 100 120 140
2005 2006 2007 2008 2009 2010 2011 2012 2013
Total Neglect Abandonment Emotional violence Sexual violence Physical violence 66 77 109 80 113 102 99 86 96 91 63 61
0 1 0 1 0 0 1 0 1 1 1 1
16 27 29 22 43 33 38 43 31 32 26 9 2 8
11 8 11
5 8 4 10 6 5 8 11 10 7 9
13 6 15 5 16 9 47 53 80 56 77 70 61 48 61 55 41 30 0 20 40 60 80 100 120
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Total
Neglect
Abandonment Sexual abuse
Physical violence Emotional violence
Figure1 Annualandmonthlyevolution(totalandpertypeofcase).
Source:Emergencysignformfortheabusedchild(2004---2013).
together.Athirdprofile(upperleft-handcorner)highlights femaleabusers,separated,ordivorced,betweentheages of20and 39.Here,thevictimstend tobemaleandvery young(between5and9yearsofage)andlivinginpartial co-residencewiththeabuser.Thereisafourthprofile,less defined,intheupperright-handcorner,inwhichthevictims areverysmall,malechildren;informationabouttheabuser andthemaritalstatusoftheparentsisscarce.
Regardingsexual violence,the dataarestructured dif-ferently.The ageofthe abuserandco-residencewiththe aggressor constitute thefirst dimension.The victims’age andgender constitute the second one. The abuser’s gen-der and recent separation/divorce are the elements that connectthetwodimensions.
There is an association between male aggressor and femalevictims (bottomof the chart). In this profile, vio-lence occurs in situations where the victim comes from familiesin whichtheparents arenotseparated/divorced. Thesearemaleabuserswhoattackpre-adolescentor ado-lescentfemalevictims.Asecondprofile(upperpartofthe chart)associatesfemaleabusersbetweentheagesof30and 39withyoungervictims,whocomefromsettingsinwhich theparentshaveseparated.Thequalityofthedatapresents somebiashereduetothelackofinformationontheidentity andage oftheabuser,whichcompromisesthedescription oftheothertwoquadrants.Thissignsuggeststherelative
opacity thatsurroundssexualviolence situationsinvolving veryyoungchildren,inadditiontothefactthattheymaybe practicedbywomenorthroughtheirconnivance/protection oftheabuser/partner.
Discussion
Thepresentseries,obtainedfromthecontextofaPERunit doesnotdifferfromothersfoundintheliterature,namely Portuguesestudies.8,9Thedescriptivestatisticsshowedthat
thetypeofabusemostfrequentlyobservedinthePER
(phys-ical and sexual violence) are, therefore, forms of active
maltreatment, asopposed to neglect(typically identified
through social work services and technicians),1 and their
relativeweightfollowcommonpatterns.15
This sample showed signs of physical violence among
peers, especially among older children. If, in other
countries,bullyinghasacquiredsomestatisticalvisibility,as
wellasinpediatricnewspapers,5,16inPortugaltheapproach
ofthesubjectremainsincipient.Thisiscertainlyduetothe
disregard or lack of notificationof thesesituations in the
currentprotocolsofinformationcollection.
The gender of the child and of the abuser were
considered inthe analysis.Thegender variablehada
Category Point Graph
Co-residence Abuser’s age range Abuser’s age range Family events Abuser’s gender Victim’s gender
Dimension 2
2.0
1.5
1.0
0.5
0.0
–0.5
–1.0
–1.5
–2.0
–2 –1 0 1 2
Dimension 1
Partial co-residence
Abuser 20-29
Recent separation/divorce
Victim 0-4
Unknown
Victim 5-9
Male victim
Abuser’s age unknown
No data on parents
Abuser’s gender unknown
Victim 10-14
Victim 15-18 No recent separation/divorce
Abuser 40-49 Abuser 50+
Abuser <19 Female abuser
Male abuser
Total co-residence Female victim Abuser 30-39
Normalization variable
Figure2 Factorialanalysisofmultiplecorrespondence:physicalviolencea.
Category Point Chart
2.5
2.0
1.5
1.0
0.5
0.0
–0.5
–1.0
–1.5
–2.0
–2.5
–2.5 –2.0 –1.5 –1.0 –0.5 –0.0 –0.5 –1.0 –1.5 –2.0 –2.5
Dimension 2
Dimension 1
Co-residence Abuser’s age range Abuser’s age range Family events Abuser’s gender Victim’s gender
Unknown
Abuser’s gender unknown
Victim 0-4
Female abuser
Male victim
Partial co-residence
Abuser 30-39 Recent separation/divorce
Victim 5-9
Victim 15-18
Victim 10-14Abuser <19
Abuser 50+
Abuser 40-49
Total co-residence Abuser’s age unknown
Abuser 20-29 Male abuser Female victim No data on parents
No recent separation/divorce
literature,17 as follows: abusers are mostly males (72%),
with mainly female victims (62%); gender was important
in structuring the closeness or distance between
illustra-tivevariablesintheconstructionofbothtypesofviolence,
physicalorsexual.
Comparedtoothers,this studytested theintroduction
ofsocialvariablesthatareseldomusedintheanalysisand
characterizationofchildabuse.Time,ontheonehand,and
themaritalrelationshipbetweenthechild’sparents,onthe
otherhand,showedinnovativeresults.
The seasonal pattern of abuse has become apparent:
springandsummershowmaximumpeaks,whereaslatefall
andwintershowminimumvalues.The relativestabilityof
physical violence throughout the year contrasts with the
concentrationofsexualviolenceinthesummermonthsand
in December. Further researchwill allow a better
under-standingofthis variability;but therhythms of schoollife
(with children staying at homefor longerperiods of time
orexclusivelyunderthecustodyofthefamilyduringschool
vacation)maybepartoftheexplanation.
Conversely, the nature of the marital
relation-ship between the child’s parents (married parents vs.
divorced/separatedparents) wasan explanatory variable.
Itisaresultthatstandsoutfromthedominantapproachin
theliteratureonchildabuse,whichfavors---inthe
charac-terizationofthecouple’srelationship---thequestionofthe
presence of violence.18 Thus, the parents’ marital status
(whethertheyaretogetherorseparated),initself,playsa
roleintheconfigurationoftwosubtypesofsexualviolence:
between male abusers and pre-adolescent or adolescent
female victims and between female abusers and younger
children.Thefirstscenarioisassociatedwithparents who
livetogether;thesecond,withseparated/divorcedparents.
The data refersprimarily tosuspected cases of violence;
sometimes,at ayoungage,theyaredifficulttoproveand
dependonthe(biased?)reportoftheparentaccompanying
thechildtothePERunit,whomaybeinvolvedinasituation
oflitigiousseparation.
Thisarticlealsoattemptedtoapplyamultidimensional
methodology, not commonly employed in the literature,
whichallowedthe discoveryof other subtypesof physical
andsexualviolence.Genderplaysanimportantroleinthe
structuringoftheseprofiles:thegenderofthechildandof
theabuserinphysicalviolence,aswellasthechild’sgender
inthedifferentformsofsexualviolence.Itisalsoworth
not-ingtheexistence,incasesofsexualviolence,ofthewoman
asthe abuserofa youngerchild, whichis areality rarely
identifiedordiscussedinsimilarstudies,19buttowhichthe
interventionmustbeattentive.
Thelimitationsofthisstudyoriginate,toagreatextent,
fromthegapsinthefillingoutofdatabytheprofessionalsof
thePERunit,asituationenhancedbythecircumstancethat,
todate,protocolcompletionisnotmandatory.Thefactthat
itis filledoutduringthe busyhospitalworking hoursalso
contributestothelowerprecisionandattentiongiventothis
process.Thesefactorsexplainthelowerqualityorevenlack
ofdataonthechild’ssocialbackground,particularlyevident
inthe caseof parents ofsexual violencevictims (levelof
education,occupation,andemployment,amongothers).
ItisknownthatthesituationsreportedinaPERunitare
onlyafractionof casesofchild abuse,evenamongthose
where the child is taken to the hospital20; andthat such
abuse is often only detected after multiple visits.21 The
expansion and improvement of the questions usedin the
formanditsconversionintoamandatoryplatform,attached
tothehospitalfile,willcontributetoovercomethe
prob-lemsofdataincompletion,aswell astoincreasetherate
ofdetectionofsituationsofviolence,inthewakeof
docu-mentedgoodpractices.15,22
Betterawarenessoftheimportanceofsocialandfamily
variables,aswellasoftheschoolcontextonthemultiple
facetsofabuse,willinevitablybeusefultohealthcare
pro-fessionals,trainedmainlyfortheassessmentoforganicor
psychologicalriskfactors.Thisstudyintendstocontribute
inthissense.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
TheauthorswouldliketothanktheteamofthePediatrics DepartmentofHospitalFernandoFonseca,EPE,for provid-ingtheinformationandforthesupportprovidedduringthis study.They wouldalso liketothankDéboraTerra for the reviewofthemanuscriptinBrazilianPortuguese.
References
1.RadfordL,CorralS,BradleyC,FisherHL.Theprevalenceand impactofchildmaltreatmentandothertypesofvictimization intheUK:findingsfromapopulationsurveyofcaregivers, chil-dren and young people and young adults. ChildAbuse Negl. 2013;37:801---13.
2.UNICE.F.Hiddeninplainsight---astatisticalanalysisofviolence againstchildren.NewYork:UNICEF;2014.
3.GilbertR,WidomCS,BrowneK,FergussonD,WebbE,JansonS. Burdenandconsequencesofchildmaltreatmentinhigh-income countries.Lancet.2009;373:68---81.
4.WHO. European report on preventing child maltreatment. Copenhagen:WorldHealthOrganization;2013.
5.GilbertR,FlukeJ,O’DonnellM,Gonzalez-IzquierdoA,Brownell M,GulliverP,etal.Childmaltreatment:variationintrendsand policiesinsixdevelopedcountries.Lancet.2012;379:758---72. 6.WHO. Report ofthe consultationon childabuse prevention.
Geneva:WorldHealthOrganization;1999.
7.RunyonD,WattamC,IkedaR,HassanF,RamiroL.Childabuse and neglectbyparents and othercaregivers.Geneva: World HealthOrganization;2002.
8.FanteC.Fenômenodebullying:comopreveniraviolêncianas escolaseeducarparaapaz.Campinas:Verus;2005.
9.RodriguezNE.Bullying,guerranaescola.Lisboa:SinaisdeFogo; 2004.
10.GreenacreMJ.Correspondence analysisin practice. 2nd ed. BocaRaton:Chapmann&Hall/CRC;2007.
11.MeulmanJJ.Optimalscalingmethodsformultivariate categor-icaldataanalysis.Leiden,TheNetherlands:LeidenUniversity; 1998.
12.CruzME,Gonc¸alvesE,BarbosaMC,VianaV,IlharcoMJ,Sequeira F,etal.Crianc¸asmaltratadas:apontadoicebergue.Acta Pedi-atrPort.1997;28:35---9.
14.NascimentoJ,FerreiraI,ZilhãoC,PintoS,FerreiraC,CaldasL, etal.Oimpactodoriscosocialnuminternamentopediátrico. ActaPediatrPort.2013;44:15---9.
15.Louwers EC, Korfage IJ, Affourtit MJ, Scheewe DJ, van de MerweMH,Vooijs-MoulaertFA,etal.Detectionofchildabusein emergencydepartments:amulti-centrestudy.ArchDisChild. 2011;96:422---5.
16.deOliveiraWA,SilvaMA,daSilvaJL,deMello FC,doPrado RR,Malta DC. Associationsbetween thepractice of bullying andindividual and contextual variablesfrom theaggressors’ perspective.JPediatr(RioJ).2016;92:32---9.
17.May-ChahalC.Genderand childmaltreatment:theevidence base.SocWorkSoc.2006;4:53---68.
18.Mills LG, Friend C, Conroy K, Fleck-Henderson A, Krug S, Magen RH, et al. Woman abuse and child protection: a
tumultuousmarriage(PartII)Childprotectionanddomestic vio-lence:training,practice,andpolicyissues.ChildYouthServRev. 2000;22:315---32.
19.BarthJ,BermetzL,HeimE,TrelleS,ToniaT.Thecurrent preva-lenceofchildsexualabuseworldwide:asystematicreviewand meta-analysis.IntJPublicHealth.2013;58:469---83.
20.Flaherty E, Sege R. Barriers to physician identification and reportingofchildabuse.PediatrAnn.2005;34:349---56. 21.RavichandiranN,SchuhS,BejukM,Al-HarthyN,ShouldiceM,
AuH,et al.Delayedidentificationofpediatricabuse-related fractures.Pediatrics.2010;125:60---6.