w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
Small
cell
variant
of
anaplastic
large
cell
lymphoma
with
leukemic
presentation:
a
diagnostic
challenge
Tomás
Zecchini
Barrese
a,∗,
Carlo
Sagramoso
b,
Francesco
Bacci
b,
Elena
Sabattini
baFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil
bBolognaUniversityMedicalSchool,Bologna,Italy
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25May2015 Accepted18May2017 Availableonline27June2017
Introduction
Anaplasticlymphomakinase(ALK)-positiveanaplasticlarge cell lymphomas (ALCLs) are recognized as a distinct clini-copathologicentityintheWorldHealthOrganization(WHO) classificationofhematopoieticneoplasms.1Basedonthe
mor-phologic features,mainly characterizedbyanaplastic large cells,and onthe expressionofthe Ki-1antigen(CD30), it wasfirstdescribedin1985.2From1990onwardsstudieshave
shownthatmanyALCLsareassociatedwiththet(2;5)(p23;q35) responsibleforthe upregulation oftheALK protein.ALCLs accountfor2–8%ofnon-Hodgkinlymphomasinadultsand approximately10–30%oflymphomas inchildren;the ALK-positive (ALK+) ALCLs largely occur within the first three decadesoflife.3Morphologically,ALK+ALCLsarecomposed
ofavariableamountofsocalled‘hallmarkcells’illustratedby largeelementswitheccentric,horseshoe-orkidney-shaped nuclei.Thesecellscanbeadmixedwithsmallerlymphocytes, HodgkinandReed-Sternberg-likeneoplasticcells aswell as withreactiveinflammatorycells,resultinginabroadrange ofhistologicpatterns recognized bythe WHOas common,
∗ Correspondingauthorat:DepartamentodeCiênciasPatológicas,Dr.CesárioMotaJúnior,112,VilaBuarque,01221-020SãoPaulo,SP,
Brazil.
E-mailaddress:[email protected](T.ZecchiniBarrese).
lymphohistiocytic,smallcellandHodgkin-liketypes,though compositeorotherunusualtypescanbeencountered.1Most
patients(70%)presentwithadvancedstagediseaseand sys-temic symptoms (75%), particularly high fever. Extranodal involvementiscommonandmainlycomprisesskin,bone,soft tissue,lungandliver.3–5Wehereinreportacaseofanadult
womanpresentingwithrapidlyprogressiveneoplasticsmall celllymphocytosis:onlyrarecaseswithleukemic presenta-tionhavebeendescribed.6–14
Case
report
A37-year-oldwomanpresentedwithathree-weekhistoryof fever,asthenia,nightsweats,anddyspnea.Imagingstudies with computed tomography (CT)revealed slightly enlarged superficialanddeeplymphnodes,thelargestoneofwhich was 35mmindiameter ataninguinal site. The craniocau-dal length of the spleenwas 14.5cm. The complete blood countrevealedleukocytosis(39.0×109/L)withrapiddoubling time(80.0×109/Lafteroneweek)withmarked lymphocyto-sis(90%)thatshowedaT-cellphenotypeatflowcytometry
http://dx.doi.org/10.1016/j.bjhh.2017.05.009
flowcytometrydetected4%ofresidual neoplasticcellsand a higher CD8+ lymphoid component that was interpreted as a virus-mediated reaction and supported by cytological evidenceoflarge“lympho-mononuclear”circulatingcells.A secondbonemarrowbiopsywasunabletoconfirmresidual diseasewhileshowingrichnessinmyeloidprecursors,plasma cellsandsomeCD8+cellsthatconfirmedwhatwasobservedin theperipheralblood.Someweekslater,shedevelopedascites and, on cytologic examination, largecells withclear cyto-plasm, irregular horseshoe-shaped nuclei and conspicuous nucleolicouldbeobserved.Immunocytochemicaltestswere positiveforCD30,CD4,EMA,PERFORINandALKcandnegative forCD3,CD8andPAX-5(Figure1).Theresultswereinterpreted asanALK+anaplasticlargecelllymphomaandthepatient startedchemotherapy(methotrexate,doxorubicin, cyclophos-phamide,vincristine,prednisone,andbleomycin–MACOP-B scheme)withimprovementoftheclinicalconditions.Neither lymphnodeenlargementatCTnorresidualtumorinthebone marrowweredetected.Nomoleculardetectionofthe t(2;5) wascarriedout.Althoughthisanalysiswasnotperformed, ALKstaining,bothnuclearand cytoplasmic,asseeninthis case,usuallycorrelateswiththet(2;5)translocationinvolving ALKand NPM.Varianttranslocationswilldisplay membra-nousorcytoplasmicstaining.15,16Basedonthesefindingswe
reviewedthefirstbonemarrowbiopsyperformingadditional immunohistochemistryfortheALKcproteinwhichrevealed positivityinsomeoftheCD4+smalllymphocytesaswellas inraredispersedpreviouslyunrecognizedatypicallargecells whichalsoturnedouttobeCD30+.Thisprompteda diagno-sisofperipheralblood and bonemarrowinvolvementbya smallcellcomponentofanALK+ALCLofthecomposite vari-ant(showingcommontypefeaturesintheserosa)presenting inleukemicphase(Figure2).
Discussion
ALK+ALCLisaT-celllymphomacharacterizedbycellsthat are generallylargewithabundantcytoplasmand pleomor-phic,oftenhorseshoe-shapednuclei,wideCD30expression andwithatranslocationinvolvingtheALKgenewhichleadsto overexpressionoftheALKprotein.1Nodalandextranodalsites
arecommonlyinvolved,withapproximately40%ofpatients showingtwoor moreextranodalsites ofthedisease.3 The
smallcellvariantofALCL,firstreportedbyKinneyetal.in
H&E
ALKc
CD30
EMA
PERFORIN
Figure1–Peritonealcellblockshowingatypicallymphoma cellswitheccentric,horseshoe-nuclei(hematoxylinand eosin:400×).ALKc,CD30,EMAandPERFORINwere
detectedbyimmunohistochemicalstaininginthe AnaplasticLargeCellLymphomacells(400×).
1993,17 accountsfor5–10%ofcasesand moreoftenoccurs
in pediatricages.1 Thisvariant,which displaysa
predomi-nanceofsmallcellsadmixedwithraresparsemedium/large elements3hasalsobeenreportedinassociationwiththeother
histologic variants, suchcases corresponding to the ‘com-positetype’ALCL.10AlthoughCD30expressionisadefining
characteristicofallALCLvariants,itcharacteristicallyshows alowerdegreeofintensityinthesmallcellcomponentas com-paredtothestrongstainingonmediumandlargesizecells; immunopositivityforALKispresentinallreportedcasesof smallcellvariantALCL.18
LeukemicpresentationinALCLishighlyunusualbutmost oftenreportedinthesmallcellvariantcases.9,18Sofaratotal
GIEMSA
CD30
ALKc
CD3
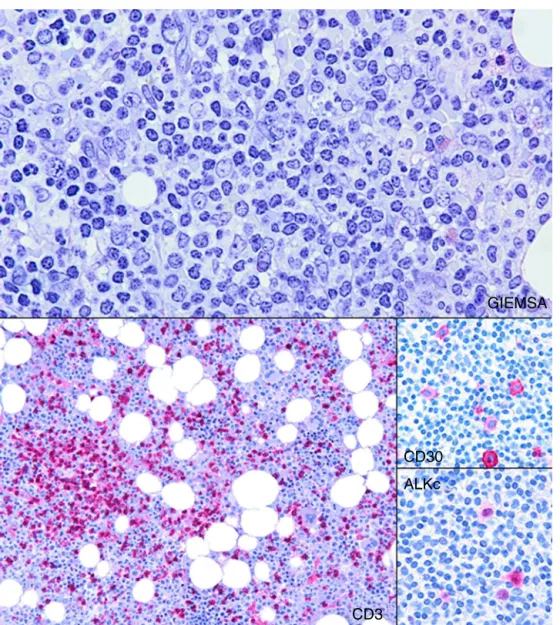
Figure2–Histologicsectionfromthebonemarrowbiopsysampleshowingmildnodularandinterstitialinfiltrationby smalllymphocytes(Giemsa:200×).CD3highlightstheselymphocytes(100×).CD30andALKcaredetectedby
immunohistochemicalstaininginsomeoftheatypicallymphocytesandbecomeofessentialimportancetothedifferential diagnosiswithT-cellprolymphocyticleukemia(400×).
<100×109/L).6,8–10,12–14,17,19–28 Clinically, most patients pre-sentedwithB-typesymptoms,withfeverbeingreportedmost (85.18%). The age of affected patients ranged from seven monthsto63years,butwith70%beingyoungerthan30years ofage.Thereisaslightmalepredominance(55.5%).9,13,26–28As
observedbyNguyenetal.mostcases(85%)ofleukemicphase ALK+ALCLshowedthet(2;5)(p23;q35)translocation,although thisobservationcannotberegardedasstatisticallysignificant sincet(2;5)occursinapproximately80%ofALK+ALCL regard-lessofthevarianttype.9
Thediagnosis ofasmallcell variantALCLinadultscan bechallenging6,18,29particularlyintheabsenceofalargecell
componentsinceitcanalsobemistakenforaninfectiousor inflammatoryprocess.Infact,althoughtheneoplasticcells doshowirregular nuclearcontours,the smallsizeand the inconspicuousnucleoliareoftenmisleading.Inthiscase,the massivelymphocytosisand minororganomegalyprompted clinicianstosearchfordiagnosisinthebonemarrowbiopsy
wheretheinfiltratewasquantitativelymild,organizedinrare fociandinsinglyscatteredsmallsizecellswithoutfrank cyto-logicalatypia.Consideringtheclinical presentation,aTPLL and alargegranularlymphocyte lymphoma/leukemiawere consideredaspossiblediagnoses:uponCD4positivityasmall cellvariantTPLL1wasfavoredinspiteoffewunusualfeatures
Conclusion
Ourcaseconfirmsthehighvariabilityinclinicalpresentation ofALCLs whichmayhaveuncommonfeatures,andshould makehematologistsandpathologistsawareoftheimportance oftakingasmallcellvariantALCLintoconsiderationalsoin adults,whenfacedwithunusualT-celllymphocytosisand/or TPLL-likepresentations.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SwerdlowSH,CampoE,HarrisNL,JaffeES,PileriSA,SteinH, etal.WorldHealthOrganizationClassificationofTumorsof HaematopoieticandLymphoidTissues.4thed.Lyon:IARC Press;2008.p.312–6.
2. SteinH,MasonDY,GerdesJ,O’ConnorN,WainscoatJ, PallesenG,etal.TheexpressionoftheHodgkin’sdisease associatedantigenKi-1inreactiveandneoplasticlymphoid tissue:evidencethatReed–Sternbergcellsandhistiocytic malignanciesarederivedfromactivatedlymphoidcells. Blood.1985;66(4):848–58.
3. SteinH,FossHD,DurkopH,MarafiotiT,DelsolG,PulfordK, etal.CD30(+)anaplasticlargecelllymphoma:areviewofits histopathologic,genetic,andclinicalfeatures.Blood. 2000;96(12):3681–95.
4. FaliniB,PileriS,ZinzaniPL,CarboneA,ZagonelV, Wolf-PeetersC,etal.ALK1lymphoma:clinico-pathological findingsandoutcome.Blood.1999;93(8):2697–706.
5. FaliniB.Anaplasticlargecelllymphoma:pathological, molecularandclinicalfeatures.BrJHaematol. 2001;114(4):741–60.
6. BayleC,CharpentierA,DuchayneE,ManelAM,PagesMP, RobertA,etal.Leukaemicpresentationofsmallcellvariant anaplasticlargecelllymphoma:reportoffourcases.BrJ Haematol.1999;104(4):680–8.
7. ChhanabhaiM,BrittenC,KlasaR,GascoyneRD.t(2;5)positive lymphomawithperipheralbloodinvolvement.Leuk
Lymphoma.1998;28(3–4):415–22.
8. TakahashiD,NagatoshiY,NagayamaJ,InagakiJ,ItonoagaN, TakeshitaM,etal.Anaplasticlargecelllymphomain leukemicpresentation:acasereportandareviewofthe literature.JPediatrHematolOncol.2008;30(9):696–700.
13.HeR,ViswanathaDS.LeukemicphaseofALK-positive anaplasticlargecelllymphoma.Blood.2013;121(11):1934.
14.OnciuM,BehmFG,RaimondiSC,MooreS,HarwoodEL,Pui CH,etal.ALK-positiveanaplasticlargecelllymphomawith leukemicperipheralbloodinvolvementisaclinicopathologic entitywithanunfavorableprognosis.Reportofthreecases andreviewoftheliterature.AmJClinPathol.
2003;120(4):617–25.
15.BenharrochD,Meguerian-BedoyanZ,LamantL,AminC, BrugièresL,Terrier-LacombeMJ,etal.ALK-positive lymphoma:asinglediseasewithabroadspectrumof morphology.Blood.1998;91(6):2076–84.
16.SooKL,ShustikD,MohdYusoffLZ,TanL.Analgorithmic approachtothediagnosisofNKandTcelllymphomas. Pathology.2011;43(7):673–81.
17.KinneyC,CollinsRD,GreerJP,WhitlockJA,SioutosN,Kadin ME.Asmall-cell-predominantvariantofprimaryKi-1(CD30)– T-celllymphoma.AmJSurgPathol.1993;17(9):859–68.
18.SummersTA,MoncurJT.Thesmallcellvariantofanaplastic largecelllymphoma.ArchPatholLabMed.
2010;134(11):1706–10.
19.AndersonMM,RossCW,SingletonTP,SheldonS,SchnitzerB. Ki-1anaplasticlargecelllymphomawithaprominent leukemicphase.HumPathol.1996;27(10):1093–5.
20.AwayaN,MoriS,TakeuchiH,MoriS,SuganoY,KamataT, etal.CD30andtheNPM-ALKfusionprotein(p80)are differentiallyexpressedbetweenperipheralbloodandbone marrowinprimarysmallcellvariantofanaplasticlargecell lymphoma.AmJHematol.2002;69(3):200–4.
21.KongSY,ChoHJ,SukJH,TakEY,KoYH,KimK,etal.Anovel complext(2;5;13)(p23;q35;q14)insmallcellvarianttype anaplasticlargecelllymphomawithperipheralinvolvement. CancerGenetCytogenet.2004;154(2):183–5.
22.MeechSJ,McGavranL,OdomLF,LiangX,MeltesenL,GumpJ. Unusualchildhoodextramedullaryhematologicmalignancy withnaturalkillercellpropertiesthatcontainstropomyosin 4-anaplasticlymphomakinasegenefusion.Blood.
2001;98(4):1209–16.
23.SanoF,TasakaT,NishimuraH,AkiyamaT,KuboY,
MatsuhashiY,etal.Smallcellvariantofanaplasticlargecell lymphomadiagnosedbyanovelchromosomalabnormality t(2;5;3)(p23;q35;p21)ofbonemarrowcells.PatholInt. 2008;58(8):494–7.
24.DalalBI,ChhanabhaiM,HorsmanDE,LeHuquetJ,Coupland R.Anaplasticlarge-celllymphomapresentingasacute leukemia.AmJHematol.2005;79(June(2)):164–5.
26.ImamuraR,MouriF,NomuraK,NakamuraT,OkuE, MorishigeS,etal.Successfultreatmentofsmallcellvariant anaplasticlargecelllymphomawithallogeneicperipheral bloodstemcelltransplantation,andreviewoftheliterature. IntJHematol.2013;97(1):139–43.
27.GrigoropoulosRL,WrightP,vant’VeerMB,ScottMA,Follows GA.Pitfallsinthediagnosisofanaplasticlargecelllymphoma withasmallcellpattern.CaseRepHematol.
2013;2013:840253.
28.GadageVS,SubramanianPG,GalaniKS,SehgalKK,JohariSP, GhogaleVS,etal.Leukemicphaseofanaplasticlymphoma kinasepositive,anaplasticlargecelllymphoma.IndianJ PatholMicrobiol.2011;54(3):599–602.