Pelvic floor muscle function and quality of life in
postmenopausal women with and without pelvic floor
dysfunction
ISABELLA PARENTE RIBEIRO FROTA1 , ADRIANA BOMBONATO OLIVEIRA ROCHA2, JOSE ANANIAS VASCONCELOS NETO 1 , CAMILA TEIXEIRA MOREIRA VASCONCELOS3 , THAIS FONTES DE MAGALHAES1 , SARA ARCANJO LINO KARBAGE1,
KATHIANE LUSTOSA AUGUSTO1, SIMONY LIRA DO NASCIMENTO4, JORGE MILLEM HADDAD2& LEONARDO ROBSON PINHEIRO SOBREIRA BEZERRA1
1Department of Surgery, Maternidade Escola Assis Chateaubriand and Department of Maternal-Child Health, Federal
University of Ceara, Fortaleza, CE, 2Department of Gynecology, Faculty of Medicine, University of Sao Paulo, Sao Paulo,~
SP,3Departament of Nursing, Faculty of Pharmacy, Odontology and Nursing, Federal University of Ceara, Fortaleza, CE,
and4Department of Physical Therapy, Faculty of Medicine, Federal University of Ceara, Fortaleza, CE, Brazil
Key words
Pelvic floor, postmenopause, prolapse, quality of life, urinary incontinence
Correspondence
Leonardo Robson Pinheiro Sobreira Bezerra, Department of Surgery, Maternidade Escola Assis Chateaubriand and Department of Maternal-Child Health, Federal University of Ceara, General Tertuliano Potiguara St. 272/ 1800 CEP 60135280, Fortaleza, Ceara, Brazil. E-mail:[email protected]
Conflict of interest
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Please cite this article as: Frota IPR, Rocha ABO, Neto JAV, Vasconcelos CTM, De Magalhaes TF, Karbage SAL, et al. Pelvic floor muscle function and quality of life in postmenopausal women with and without pelvic floor dysfunction. Acta Obstet Gynecol Scand 2018; https://doi.org/10.1111/aogs. 13305
Received: 10 July 2017 Accepted: 27 December 2017
DOI: 10.1111/aogs.13305
Abstract
Introduction. This study aims to compare pelvic floor muscle (PFM) function in postmenopausal women with and without pelvic floor dysfunction (PFD) and the relationship between PFM function and quality of life.Material and methods. A case–control study with 216 postmenopausal women with (n =126) and
without (n= 90) PFD. PFM function was assessed by digital vaginal palpation using the PERFECT scale. Specific quality of life was evaluated using the King’s Health Questionnaire for women with urinary incontinence and the Prolapse Quality-of-Life Questionnaire for women with pelvic organ prolapse. We analyzed women with PFD into two categories: Oxford’s grade≤2 or≥3 using a chi-squared test. Results.Out of 126 womem with PFD 44 (34.9%) presented stress urinary incontinence, 21 (16.6%) had pelvic organ prolapse and 61 (48.4%) had urinary incontinence + pelvic organ prolapse. Strength had a median value 2 (0–5) in all women studied and most of them had insufficient
strength, reduced endurance and repetition without statistical difference between groups. Incontinent women with strength ≤2 had worse perception of
general health domain of King’s Health Questionnaire (p=0.007). No association was found between PFM function and Prolapse Quality-of-Life Questionnaire. Conclusions. PFM function assessed by bidigital palpation in postmenopausal women was not sufficiently sensitive to differentiate between women with vs. women without PFM dysfunction and was not related with specific quality of life in women with urinary incontinence and pelvic organ prolapse, respectively. These data should be used to reinforce the widespread recommendation that PFM training is essencial in PFD treatment.
Introduction
Pelvic floor dysfunctions (PFD) are common gynecologi-cal disorders that affect roughly one-third of adult women (1). Urinary incontinence (UI) and fecal inconti-nence are included in this group, as well as pelvic organ prolapse (POP), sexual dysfunctions and lower urinary tract syndromes.
Urinary incontinence is defined as the involuntary loss of urine (2). POP, in turn, is anatomically defined as the descent of the anterior vaginal wall, posterior vaginal wall, uterus and/or apex of the vagina (2). Despite not generating significant morbidity or mortality, these func-tional and anatomic changes may cause social, psycholog-ical, physical and sexual dysfunction, and can dramatically reduce the quality of life (QoL) of affected women (3,4).
PFD, especially UI and POP, have multiple causes and develop gradually over years. Although the relative importance of each cause is unknown (5), vaginal delivery is the most commonly cited risk factor. Collagen changes, reduced urethral vascularization and reduced skeletal muscle volume are associated with postmenopausal hypoestrogenism (6). The resulting urogenital atrophy is also presumed to be one of the causes of the endopelvic fascia disturbances and urinary sensory symptoms that occur after menopause (7).
Pelvic floor muscles (PFM) function has a decisive role in maintaining continence and pelvic organ support and several authors have studied pelvic muscle training and its role in the treatment and prevention of PFDs (8). Dif-ferent methods of PFM function evaluation were devel-oped, such as vaginal palpation, manometry, electromyography, dynamometry and ultrasonography. Despite this, however, none of them seems able to fully assess the complexity of PFM function (9).
Conversely, QoL measurements in women with PFD have been increasingly valued and have been recom-mended by the International Continence Society since 1997. The subjective perception of healing is now consid-ered as important as the objective evaluation. QoL mea-sures should be included in all clinical trials, as a complement to traditional clinical parameters. Hence, PFM evaluation and QoL are important, but there are still gaps in the differences in their function between women with PFD and women without such dysfunction. We can find these gaps especially when we study the impact of PFM function, as assessed by digital palpation, in the gen-eral and disease-specific QoL of such patients. To answer these issues, we aimed to assess pelvic floor muscle func-tion in postmenopausal women with and without PFD, relating these results to the QoL of the women involved.
Material and methods
This observational case–control study followed the
guideli-nes of the STROBE Statement (10), and took place in the Urogynecology outpatient services of two tertiary hospitals in Fortaleza, Brazil, from October 2012 to October 2013.
Selection of participants
Postmenopausal women who have visited a gynecology outpatient clinic were recruited for the study. Acoording to their symptoms and gynecological examination they were divided into two groups: Group 1 (Control group) with women without PFD, and Group 2 (Case group) with women with PFD.
To be included in the case group the woman had to pre-sent an objective diagnostic of PFD of stress or mixed UI and/or symptomatic POP. The diagnosis of PFD was based on the presence of suggestive findings on the gynecological examination (physical examination for genital prolapse; POP-Q stage≥2) (11) and urodynamic studies and on the presence of typical clinical symptoms (a dragging or heavy sensation, the feeling of a lump in the vagina and voiding difficulties; or symptoms indicating stress-related involun-tary loss of urine). Women with uninhibited detrusor con-tractions on urodynamic testing, who had not undergone hormone replacement therapy in the past 6 months, with a history suggestive of neurogenic bladder, gynecological cancer, collagen disease, psychiatric comorbidities and/or cognitive impairment were excluded from this study.
Sample size
Sample size was calculated based on the original study by Devreese et al. (12), which evaluated the function of PFM through vaginal palpation in women with and without UI. We calculated a sample size of 88 per group was required to achieve a study strength of 80% and signifi-cance level of 5%, using an unpaired two-tailedt-test.
Data collection
Data were collected through clinical gyneacological evalu-ations for inclusion, using standardized clinical evaluation
Key message
forms available in both locations, assessment of general and specific quality of life and PFM function evaluation as described bellow.
Quality of life measurements
Since generic instruments are not able to fully evaluate the impact of a particular condition on patients’ QoL, several disease-specific questionnaires have been created (13). We used the Brazilian version of the King’s Health Questionnaire (KHQ) for patients with UI (n=44) (14) and the Brazilian version of the Prolapse Quality of Life Questionnaire (P-QoL) for patients with POP (n =21) (15). If patients showed simultaneous UI and POP, both specific questionnaires were applied (n=61).
Pelvic floor function assessment
Pelvic floor function was assessed by a trained specialized physiotherapist. The researcher (IPRF) initially provided explanations with a brief overview on PFM anatomy and function using three-dimensional models and illustrations through informal conversation. Patients were taught what the PFM are, their location and their contribution to pel-vic organ support and urinary continence. This was done to develop women’s self-awareness regarding their body and the muscles that would be evaluated.
Finally, the researcher evaluated pelvic floor function through vaginal palpation according to the PERFECT scheme (16), which examines power (P), endurance (E), number of timed repetitions (R), and number of timed, fast contractions (F). A rest interval of 30 s was allowed between contractions, to avoid fatigue (12). Power (P) was graded by an Oxford adapted scale from zero (Nil) to five (Strong) (16). Strength was considered insufficient when grading was less than or equal to 2 (17). When effective, contraction results in an upward lift of the per-ineum. If no contractions were visualized or felt through palpation, with a strength grading equal to zero, we con-sidered there to be no perineal awareness (18).
Data analysis
Women from group 1 vs. group 2 were tested for homo-geneity regarding age, body mass index, number of preg-nancies, parity, number of cesarean sections, number of vaginal deliveries and score in the Criterio de Classificacß~ao Economica Brasil (CCEB) questionnaire, an instrument used to assess socio-economic status in the Brazilian pop-ulation. The CCEB is based on the evaluation of house-hold income, schooling and amount of durable goods owned by the patient.
The Kolmogorov–Smirnov test was used to verify if
quantitative data were normally distributed. The variables age, body mass index and part of the SF-36 domains (physical functioning, general health perceptions, vitality and mental health) showed Gaussian distribution and so were analyzed using Student’s t-test. The Mann–Whitney U-test was used when variables were not normally dis-tributed. Correlations between groups were calculated using Pearson’s coefficient. Multiple logistic regression analyses were used with Wald test and the Hosmer–
Lemeshow test to search the association between depen-dent and independepen-dent variables like age, years of study, number of gestations and parity. We considered statistical significance when p<0.05 (5%). Analyses were per-formed using the Statistical Package for Social Science 15.0. (SPSS Inc., Chicago, IL, USA).
Ethical approval
The Ethics Committee of both hospitals approved this sur-vey under numbers 499/2011 and 156/2012, and all partici-pants signed a consent form. This project was registered in Clinical Trials under the identifier NCT01891162.
Results
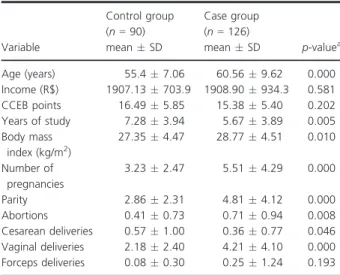
The final sample of this study comprised 216 women, of which 90 did not have PFD (group 1) and 126 (group 2) had PFD. Age range was 36–89 years (mean
58.09.0 years), and all participants belonged to the low-income socio-economic stratum (C). Women with PFD were older, had more deliveries, greater body mass index and fewer years of study (p<0.005). (Table 1).
The median PFM strength score according to the Oxford scale was 2 (range: 0–5). In the control group, we
found a normal distribution in strength grading scores, and observed a predominance of grade 2 in 35.8% of par-ticipants, followed by grade 3 (17.8%), 1 (17.8%), 0 (14.4%), 4 (11.1%) and 5 (3.3%) scores. Likewise, a nor-mal distribution was also seen in the PFD group, with the same predominance of grade 2 in 39.7% of partici-pants, followed by grade 3 (23.8%), 1 (11.1%), 0 (12.7%), 4 (8.7%) and 5 (4%) scores.
Women were also analyzed according to presence or absence of PFM contractions. Those with strength zero were considered to lack perineal awareness and those with power equal to ≥1 were considered to have present per-ineal awareness, there were also no significant differences between groups. When we compared the PFM strength between the case and control groups using the Pearson’s coefficient we did not find statistically significant differ-ence (p=0.514). Although, the majority of women with or without PFD presented PFM contractions when
requested (Table 2). When we performed multiple logistic regression analyses using Wald test and the Hosmer–
Lemeshow test, we did not find association to be statisti-cally significant between variables like age (0.746), years of study (0.501), number of gestations (0.584) and parity (0.350).
According to the presence of UI and POP, 44 (34.9%) women had only UI, 21 (16.7%) had only POP, and 61 (48.4%) presented both dysfunctions. When these groups were compared, no difference in PFM function was demonstrated (Table 3).
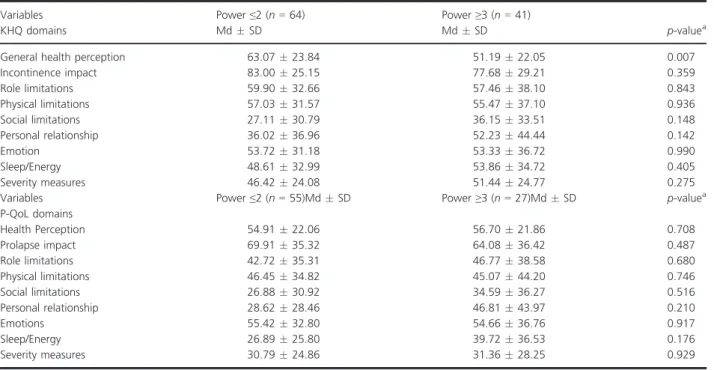
In patients with UI, the association between PFM func-tion and specific QoL measured by the KHQ demon-strated a significant difference only in the General Health Perception domain (p=0.007); those with more effective contractions had more favorable QoL scores. On the other hand, no association was demonstrated between PFM function and quality of life measured by the P-QoL in women with POP (Table 4).
Discussion
We observed no statistically significant differences between women with PFD and the control group regard-ing PFM evaluation usregard-ing the PERFECT scheme, suggest-ing that PFM strength may not be the unique determining factor of PFD. As the studied group is of postmenopausal women, this result might suggest that postmenopausal status may play an important role in the etiology of PFD.
We recognize that the use of vaginal palpation to assess PFM function has limitations. Most studies in PFD actu-ally use manometry, dynamometry and ultrasound (19,20). However, the Oxford standardized scale is proba-bly the most frequently used worldwide in physical ther-apy and routine clinical evaluation (1,9,21,22). It has both good reproducibility, inter-examiner and test–retest
reliability, and internal and external validity (22,23). Therefore, we decided to use vaginal palpation to assess PFM function because of its feasibility in daily clinical settings. In this sense, our study sought to answer daily routine physiotherapist-related questions.
Assessment of PFM function and strength is a crucial step in the clinical evaluation of PFD, several studies have investigated the role of PFM function in different life cycles (19,24–26). Henderson et al. (25) found a
differ-ence between correct PFM contraction on the first attempt in women with POP and SUI vs. without PFD (85.8%) (p=0.01). Also, there was no association between ability to contract PFM and age. Fitzgerald et al. found that the physiological aging of continent women per se does not correlate with lower PFM strength (26). Sartori et al. were also unable to find associations
Table 2. Comparison of pelvic floor muscle strength between postmenopausal women with and without pelvic floor dysfunction. (n =216).
Variables
Control group (n=90)
Case group
(n=126) p-value Odds ratio
Perfect
Strength≤2,n(%) 61 (67.8%) 80 (63.5%) 0.307a 0.82 Strength≥3,n(%) 29 (32.2%) 46 (36.5%)
Strength, meanSD
2.031.30 2.171.24 0.369b
Endurance, meanSD
2.502.17 2.232.03 0.428b
Repetition, meanSD
1.542.61 1.062.17 0.721b
Fast, meanSD 5.574.20 5.404.35 0.725b Perineal awareness
Strength 0,n(%) 13 (14.4%) 16 (12.7%) 0.430a 0.86 Strength≥1,n(%) 77 (85.6%) 110 (87.3%)
aChi-squared test. bMann
–WhitneyU-test.
Table 1. Characterization of demographic data between postmenopausal women with and without pelvic floor dysfunction. Fortaleza, 2014 (n=216).
Variable
Control group (n=90) meanSD
Case group (n=126)
meanSD p-valuea
Age (years) 55.47.06 60.569.62 0.000 Income (R$) 1907.13703.9 1908.90934.3 0.581 CCEB points 16.495.85 15.385.40 0.202 Years of study 7.283.94 5.673.89 0.005 Body mass
index (kg/m2)
27.354.47 28.774.51 0.010
Number of pregnancies
3.232.47 5.514.29 0.000
Parity 2.862.31 4.814.12 0.000 Abortions 0.410.73 0.710.94 0.008 Cesarean deliveries 0.571.00 0.360.77 0.046 Vaginal deliveries 2.182.40 4.214.10 0.000 Forceps deliveries 0.080.30 0.251.24 0.193
CCEB,Criterio de Classificacßao Economica Brasil~ questionnaire. aMann
between PFM strength, age and number of vaginal deliv-eries, upon studying 150 continent women ranging from 30 to 67 years of age. However, they did not have a group with PFD for comparison nor did they include women of all ages (19).
Interestingly, in both of our studied groups, most women had a mean muscle strength score of ≤2 in the
Oxford scale (PERFECT scheme), which is considered low. Patients’ low reponsiveness with digital palpation and their inability to separate between high- or low-func-tion seems to be very common in this populalow-func-tion
(18,27). This is consistent with a previous epidemiological study investigating 1732 women who had PFM strength assessed with the Oxford scale, and also found scores≤3
(1). Albrich et al. also evaluated 114 women with PFD using the PERFECT scheme, and found a mean grading of 2.211.06 in the Power section (vs. 2.17 1.24 found in our results) (28). Finally, Roza et al. measured PFM through the PERFECT scheme in nulliparous women (continent vs. incontinent participants), and did not find significant differences between the two groups (20).
Table 3. Pelvic floor muscles function according to the clinical complaints and gynecological examination in women with and without pelvic floor dysfunction (n=216).
Variables
UI group (n=44) MdSD
POP group (n=21) MdSD
UI+POP group (n=61) MdSD
Control (group 1) (n=90)
MdSD p-valuea
Strength≤2 25 (56.8%) 61 (67.8%) 39 (63.9%) 61 (67.8%) 0.358
Strength≥3 19 (43.2%) 5 (23.8%) 22 (36.1%) 29 (32.2%)
Strength 2.321.25 1.621.32 2.251.17 2.031.30 0.148
Endurance 2.612.00 1.621.71 2.162.13 2.502.17 0.222
Repetition 1.412.17 1.052.13 1.002.22 1.542.61 0.313
Fast 6.394.19 4.104.38 5.154.37 5.574.20 0.180
MdSD, medianstandard deviation; POP, pelvic organ prolapse; UI, urinary incontinence. a
Kruskal–Wallis test.
Table 4. Association between specific quality of life using the King’s Health Questionnaire (KHQ) (for women with urinary incontinence) and the Prolapse Quality-of-Life Questionnaire (P-QoL) (for women with pelvic organ prolapse) vs. the pelvic floor function (PERFECT scheme) of women with pelvic floor dysfunction (n=126).
Variables KHQ domains
Power≤2 (n=64) MdSD
Power≥3 (n=41)
MdSD p-valuea
General health perception 63.0723.84 51.1922.05 0.007
Incontinence impact 83.0025.15 77.6829.21 0.359
Role limitations 59.9032.66 57.4638.10 0.843
Physical limitations 57.0331.57 55.4737.10 0.936
Social limitations 27.1130.79 36.1533.51 0.148
Personal relationship 36.0236.96 52.2344.44 0.142
Emotion 53.7231.18 53.3336.72 0.990
Sleep/Energy 48.6132.99 53.8634.72 0.405
Severity measures 46.4224.08 51.4424.77 0.275
Variables P-QoL domains
Power≤2 (n=55)MdSD Power≥3 (n=27)MdSD p-valuea
Health Perception 54.9122.06 56.7021.86 0.708
Prolapse impact 69.9135.32 64.0836.42 0.487
Role limitations 42.7235.31 46.7738.58 0.680
Physical limitations 46.4534.82 45.0744.20 0.746
Social limitations 26.8830.92 34.5936.27 0.516
Personal relationship 28.6228.46 46.8143.97 0.210
Emotions 55.4232.80 54.6636.76 0.917
Sleep/Energy 26.8925.80 39.7236.53 0.176
Severity measures 30.7924.86 31.3628.25 0.929
aMann
In our study, participants had not undergone previous PFM strength assessment or treatment, which may par-tially account for the insufficient PFM strength that we found. Ferreira et al. (23) observed significant increases in Power measurements using the Oxford scale after 30 days of the first assessment in nulliparous women. In addition Henderson et al. (25) have reported that simple explanations could make patients contract PFM effec-tively. Those authors believed that women without UI and POP would be more capable of correctly contracting this muscle group; however, women in that study were in the menacme. We can infer that, perhaps, post-menopausal status alone causes low levels of perineal awareness due to tissue atrophy, resulting in low grading scores in the Oxford scale even when PFD is not present.
A study showed that PERFECT scheme scores were not able to distinguish between genital prolapse stages or degrees of severity of UI. This may happen because PFM function does not progressively worsen once PFD has taken place, or because the Oxford scale is not accurate enough to show a clear association between PFM func-tion and PFD (21). Moreover, weaker PFM do not neces-sarily imply the existence of PFD, as women may not have adequate perineal awareness until muscles are stimu-lated to contract voluntarily. A limitation of our study is that we did not analyze pelvic floor function according to IU severity, which can interfere in the results.
We also studied the association between PFM function and validated general QoL evaluation questionnaires. We found that women with PFD presented with worse QoL, using SF-36, than control groups. Barentsen et al. (29) found that severe UI also diminishes the generic quality of life compared with slight UI, although there is no effect of moderate severity on QoL as compared with slight severity of urine loss. In our population, PFD seems to have an impact that is more significant in general quality of life. Some social or cultural factors could explain this strong impact of the PFD on the overall qual-ity of life of our women. It appears that to our popula-tion, PFD is a greater predictor for a decreased quality of life.
When we evaluated the impact of UI and/or POP on QoL, we found no differences between Oxford and P-QoL scores. Participants with UI were evaluated through the KHQ and only the General Health Percep-tion domain was statistically different (p<0.007). Maybe the disease-specific QoL questionnaires used do not have the same sensitivity as the SF-36 in our population. This may indicate difficulties in perceiving QoL variations by participants as most women studied had low educational levels (mean of 6.6 years of formal education). Struggles over understanding or interpreting questions are likely to cause altered scores, so lowering the reliability of the use
of QoL questionnaires in such evaluations. To avoid this bias, the validation of instruments that contemplate edu-cational limitations and cultural singularities is needed.
In 2007, Borello-France et al. assessed PFM strength by the Brink scale in groups of women with POP, but no stress UI (21). They observed differences between POP stages and PFM strength; the lowest stage had the best PFM force. The same authors did not find significant dif-ferences when comparing muscle strength assessment and disease-specific QoL scores. In addition, they also ana-lyzed sex-related QoL in patients with PFD, and found that scores were not associated with PFM strength either. Chevalier et al. (2014) (22) assessed PFM function in 218 women using the PERFECT scheme and a perineometer. In similarity with our study, they did not find a correla-tion between Power measurements using the Oxford scale and QoL measured by the SF-12. They concluded that there was no association between PFM Power, the general health status of women and their perceived QoL. This corroborates the hypothesis that PFM strength cannot infer whether postmenopausal patients with PFD have better or worse QoL.
There are some limitations regarding the significance of extrapolating Oxford scores to other disturbances involved in PFD. In our setting, we must take into account cultural characteristics, income and educational levels, which influence an individual’s perception of her own health and well-being. Women with lower socio-eco-nomic profiles tend to have higher chances of needing medical attention because they are more commonly exposed to health hazards; and have delayed perception and recognition of PFD (27,30). Such phenomena may also present as low genital awareness and struggle over understanding physical examination instructions.
There were no differences in PFM strength between the studied groups. Regarding PFM function and QoL in postmenopausal women with UI, as measured by the KHQ, a statistically significant difference was only found in the General Health Perception domain. When we assessed PFM function and specific QoL as measured by the P-QoL in postmenopausal women with POP, statisti-cally significant differences were not found in any domain.
this purpose need further validation. We believe that other instruments, such as manometers and dynamome-ters that determine pressure and force, respectively, may be used, further studies are necessary to reach consensus on this matter. Several authors researched the digital pal-pation correlation with other methods considered as objective; nevertheless its reproducibility remains ques-tionable. However, currently, there is no evaluation tool that is considered the reference standard; that way, the International Continence Society Committee strongly rec-ommends that the assessment of PFM has to be per-formed through vaginal palpation and perineometry (1). To better investigate these associations, further studies in the area are needed.
Finally, variables such as perimenopausal status, demo-graphic data, etiology and psychosocial aspects play a more important role in the expression of PFD symptoms and, as a result, in the perceived QoL than they do in the PFM function (22). Our results support the perception that PFD and its related symptoms are complex and not fully understood. However, although there is no differ-ence in PFM function between women with and without PFD in our study, we strongly believe that these data should be used to reinforce the level A1 evidenced base and the widespread recommendation that PFM training is essential in PFD elaboration of adequate treatment and is essential for the monitoring of the results (1–3).
Acknowledgements
We acknowledge to Interdisciplinary Cearense Group of Urogynecology and Pelvic Floor Dysfunctions.
References
1. Parden AM, Griffin RL, Hoover K, Ellington DR, Gleason JL, Kathryn L, et al. Prevalence, awareness, and
understanding of pelvic floor disorders in adolescent and young women. Female Pelv Med Reconstruc Sur. 2016;22:346–55.
2. Haylen BT, Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, et al. An international urogynecological association (IUGA)/international continence society (ICS) joint report on the terminology for female pelvic floor dysfunction International Urogynecological Association; International Continence Society. Neurourol Urodyn. 2010;29:4–20.
3. Botelho S, Pereira LC, Marques J, Lanza AH, Amorim CF, Palma P, et al. Is there correlation between
electromyography and digital palpation as means of measuring pelvic floor muscle contractility in nulliparous, pregnant, and postpartum women? Neurourol Urodynam. 2013;32:420–3.
4. Stanford EJ, Cassidenti A, Moen MD. Traditional native tissue versus mesh-augmented pelvic organ prolapse repairs: providing an accurate interpretation of current literature. Int Urogynecol J. 2012;23:19–28.
5. Schorge JO, Halvorson LM, Bradshaw KD, Schaffer JI, Hoffman BL, Cunningham G. Prolapso deorg~ao pelvico. In: Schorge JO, et al. (eds). Williams Gynecology, 2nd edn. New York: McGraw Hill Medical, 2011. pp. 532–55.
6. Carlile A, Davies I, Rigby A, Brocklehurst JC. Age changes in the human female urethra: a morphometric study. J Urol. 1988;139:532–5.
7. Raz R, Stamm WE. A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections. N Engl J Med. 1993;329:753.
8. Petrus PE, Ulmsten UI. An integral theory and its method for the diagnosis and management of female urinary incontinence. Scand J Urol Nephrol Suppl. 1993;153:1–93.
9. Marijke C, Hove S, Pool AL, Eijkemans MJC, Bruger CW. Pelvic floor muscle function in a general female
population in relation with age and parity and the relation between voluntary and involuntary contractions of the pelvic floor musculature. Int Urogynecol J. 2009;20:1497–
504.
10. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): guidelines for reporting observational studies. Ann Intern Med. 2007;147:573–7.
11. Bump RC, Mattiasson A, Bo K, Brubaker L, DeLancey JOL, Klarskov P, et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor
dysfunction. Am J Obstet Gynecol. 1996;175:10.
12. Devreese A, Staes F, De Weerdt W, Feys H, Van Assche A, Penninckx F, et al. Clinical evaluation of pelvic floor muscle function in continent and incontinent women. Neurourol Urodynam. 2004;23:190–7.
13. Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al. The standardization of terminology of lower urinary tract function: report from the
Standardization Sub-committee of the International Continence Society. Am J Obstet Gynecol. 2002;187:116–
26.
14. Reese PR, Pleil AM, Okano GJ, Kelleher CJ. Multinational study of reliability and validity of the King’s Health Questionnaire in patients with overactive bladder. Qual Life Res. 2003;12:427–42.
15. Oliveira MS, Tamanini JT, de Aguiar Cavalcanti G. Validation of the Prolapse Quality-of-Life Questionnaire (P-QoL) in Portuguese version in Brazilian women. Int Urogynecol J Pelvic Floor Dysfunct. 2009;20:1191–202.
16. Laycock J, Jerwood D. Pelvic floor muscle assessment:the PERFECT scheme. Physiotherapy. 2001;87:631–42.
in patients with stress urinary incontinence. Clinics. 2011;66:785–91.
18. Bo K, Sherburn M. Evaluation of female pelvic-floor muscle function and strength. Physical Ther. 2005;85:269–82.
19. Sartori DVB, Gameiro MO, Yamamoto HA, Kawano PR, Guerra R, Padovani CR, et al. Reliability of pelvic floor muscle strength assessment in healthy continent women. BMC Urol. 2015;15:29.
20. Roza T, Mascarenhas T, Araujo M, Trindade V, Jorge RN. Oxford Grading Scale vs manometer for assessment of pelvic floor strength in nulliparous sports students. Physiotherapy. 2013;99:207–11.
21. Borello-France DF, Handa VL, Brown MB, Goode P, Kreder K, Scheufele LL, et al. Pelvic-floor muscle function in women with pelvic organ prolapse. Phys Ther. 2007;87:399–407.
22. Chevalier F, Fernandez-Lao C, Cuesta-Vargas AI. Normal reference values of strength in pelvic floor muscle of women: a descriptive and inferential study. BMC Women’s Health. 2014;14:143.
23. Ferreira CHJ, Barbosa PB, Souza FO, Antonio FI, Franco MM, Bo K. Inter-rater reliability study of the modified Oxford Grading Scale and the Peritron manometer. Physiotherapy. 2011;97:132–8.
24. Vermandel A, Wachter S, Beyltjens T, Hondt DD. Pelvic floor awareness and the positive effect of verbal instructions in 958 women early postdelivery. Int Urogynecol J. 2015;26:223–8.
25. Henderson JW, Wang S, Egger MJ, Masters M, Nygaard I. Can women correctly contract their pelvic floor muscle without formal instruction? Female Pelvic Med Reconstr Surg. 2013;19:8–12.
26. FitzGerald MP, Tennstedt SL, Nager CW, Xu Y, Zimmem P. Quality of life in women with stress urinary
incontinence. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18:543–9.
27. Bo K, Finckenhagen HB. Vaginal palpation of pelvic floor muscle strength: inter-test reproducibility and comparison between palpation and vaginal squeeze pressure. Acta Obstet Gynecol Scand. 2001;80:883–7.
28. Albrich S, Steetskamp J, Knoechel SL, Porta S, Hoffmann G, Skala C. Assessment of pelvic floor muscle contractility: digital palpation versus 2D and 3D perineal ultrasound. Arch Gynecol Obstet. 2016;293:839–43.
29. Barentsen JA, Visser E, Hofstetter H, Maris AM, Dekker JH, Bock GH. Severity, not type, is the main predictor of decreased quality of life in elderly women with urinary incontinence: a population-based study as part of a randomized controlled trial in primary care. Health Qual Life Outcomes. 2012;10:153.