www.jped.com.br
ORIGINAL
ARTICLE
Coenzyme
Q10
and
pro-inflammatory
markers
in
children
with
Down
syndrome:
clinical
and
biochemical
aspects
夽
Moushira
E.
Zaki
a,
Hala
T.
El-Bassyouni
b,
Angie
M.S.
Tosson
c,∗,
Eman
Youness
d,
Jihan
Hussein
daNationalResearchCentre,MedicalResearchDivision,BiologicalAnthropologyDepartment,Cairo,Egypt
bNationalResearchCentre,HumanGeneticsandGenomeResearchDivision,ClinicalGeneticsDepartment,Cairo,Egypt cCairoUniversity,FacultyofMedicine,PediatricsDepartment,Cairo,Egypt
dNationalResearchCentre,MedicalResearchDivision,MedicalBiochemistryDepartment,Cairo,Egypt
Received28February2016;accepted27April2016 Availableonline19October2016
KEYWORDS
CoenzymeQ10;
Downsyndrome
children; Interleukin6; Oxidativestress; Tumornecrosis factor␣
Abstract
Objective: EvidenceofoxidativestresswasreportedinindividualswithDownsyndrome.There isagrowinginterestinthecontribution oftheimmune systeminDownsyndrome. Theaim ofthisstudyistoevaluatethecoenzymeQ10andselectedpro-inflammatorymarkerssuchas interleukin6andtumornecrosisfactor␣inchildrenwithDownsyndrome.
Methods: Eighty-sixchildren(5---8yearsofage)wereenrolledinthiscase-controlstudyfrom twopublicinstitutions.Atthetimeofsampling,thepatients andcontrolssufferedfromno acuteorchronicillnessesandreceivednotherapiesorsupplements.Thelevelsofinterleukin 6, tumornecrosisfactor ␣,coenzymeQ10,fastingbloodglucose,andintelligence quotient
weremeasured.
Results: Forty-threeyoung Down syndromechildren andforty-threecontrols wereincluded overaperiodofeightmonths(January---August2014).Comparedwiththecontrolgroup,the Downsyndromepatientsshowedsignificantincreaseininterleukin6andtumornecrosisfactor␣
(p=0.002),whilecoenzymeQ10wassignificantlydecreased(p=0.002).Also,bodymassindex andfasting bloodglucosewere significantlyincreasedinpatients.Therewas asignificantly positivecorrelationbetweencoenzymeQ10andintelligencequotientlevels,aswellasbetween interleukin6andtumornecrosisfactor␣.
夽
Pleasecitethisarticleas:ZakiME,El-BassyouniHT,TossonAM,YounessE,HusseinJ.CoenzymeQ10andpro-inflammatorymarkersin childrenwithDownsyndrome:clinicalandbiochemicalaspects.JPediatr(RioJ).2017;93:100---4.
∗Correspondingauthor.
E-mail:[email protected](A.M.Tosson). http://dx.doi.org/10.1016/j.jped.2016.04.012
Conclusion: Interleukin6andtumornecrosisfactor␣levelsinyoungchildrenwithDown
syn-dromemaybeusedasbiomarkersreflectingtheneurodegenerativeprocessinthem.Coenzyme Q10mighthavearoleasagoodsupplementinyoungchildrenwithDownsyndrometoameliorate theneurologicalsymptoms.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
PALAVRAS-CHAVE
CoenzimaQ10; Crianc¸ascom síndromedeDown; Interleucina6; Estresseoxidativo; Fatordenecrose tumoral␣
CoenzimaQ10emarcadorespró-inflamatóriosemcrianc¸ascomsíndromedeDown: aspectosclínicosebioquímicos
Resumo
Objetivo: Foramrelatadasevidênciasdeestresseoxidativoemindivíduoscomasíndromede Down.Háuminteressecadavez maiornacontribuic¸ãodosistemaimunológiconasíndrome deDown.OobjetivodesteestudoéavaliaracoenzimaQ10emarcadorespró-inflamatórios selecionados,comointerleucina6efatordenecrosetumoral␣,emcrianc¸ascomasíndrome
deDown.
Métodos: 86crianc¸as(5-8anosdeidade)deduasinstituic¸õespúblicasforaminscritasneste estudodecaso-controle.Nomomentodaamostragem,ospacienteseoscontrolesnãosofriam denenhumadoenc¸aagudaoucrônicaenãorecebiamnenhumaterapiaousuplementos.Foram medidososníveisdeinterleucina6,fatordenecrosetumoral␣,coenzimaQ10,glicemiade
jejumequocientedeinteligência.
Resultados: 43crianc¸ascomsíndromedeDowne43controlesforamincluídosemumperíodode 8meses(janeiro-agosto2014).Emcomparac¸ãoaogrupodecontrole,ospacientescomsíndrome deDownmostraramaumentosignificativonainterleucina6enofatordenecrosetumoral␣
(p=0,002),ao passoqueacoenzimaQ10 apresentousignificativareduc¸ão(p=0,002).Além disso,oíndicedemassacorporaleaglicemiadejejumeramsignificativamentemaioresnos pacientes.Houveumacorrelac¸ãosignificativamentepositivaentreosníveisdecoenzimaQ10 edoquocientedeinteligência,bemcomoentreainterleucina6eofatordenecrosetumoral
␣.
Conclusão: Osníveisdeinterleucina6efatordenecrosetumoral␣emcrianc¸asmaisnovas
comsíndromedeDownpodemserutilizadoscomobiomarcadores,refletindooprocesso neu-rodegenerativoneles.AcoenzimaQ10podeterumpapelcomobomsuplementoemcrianc¸as comsíndromedeDownparamelhorarossintomasneurológicos.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Trisomy21isthemostfrequentchromosomalabnormality, which characteristicallyhassignificant cognitive disability andneurologicdeficiencies.Itaffects1/700to1/1000live births.1 Excess inhibition in the brain of patients withan
extra chromosome 21 could be responsible for cognitive
deficitsnoticedthroughout theirlives.2 Oxidativestressis
knowntohaveasubstantialroleinthepathologybecauseof
geneticandepigenetic factors,which suggeststhat
oxida-tiveimbalancecontributestotheclinicalmanifestationsin
Downsyndrome(DS).3InDownsyndrometheoxidative
dam-agehasamajorroleintheneurodegenerative processes.4
CoenzymeQ10(CoQ10)worksasareactiveoxygenspecies
(ROS)scavenger.Possibly,inaddition,itstimulatesoxidative
damagerepairenzymesandhasaroleintheregulationof
geneexpression.Italsomight workasamodulatorofDNA
repairmechanisms.5,6TheeffectofCoQ10hasbeenstudied
in some neurological disorders where mitochondrial
dys-functionwasdetected.7Thiscouldexplainthebiochemical
processbywhich exogenousCoQ10 improves the
bioener-geticimpairmentinsomemitochondrialmyopathiesandin
cardiomyopathy.8,9CoenzymeQ10hasbeenadministeredin
patientsaffectedbyDS,attemptingtocounteractthe
oxida-tiveimbalancepresentduetoitssecondarydeficiency,with
promisingresults.10,11IndividualshavingDSaremoreprone
toinfectionsandautoimmunedisorders.Ineffectiveimmune
responsesinDSleadtorecurrentviral/bacterialinfections
andcontributetothedevelopmentofvarious
pathophysio-logicalsymptoms,includingcognitiveimpairment.12
The dysfunctionof the immune system in DShas been
attributed to decreased number of B-lymphocytes, T-cell
subset modifications, as well as changes in the levels of
anti-andpro-inflammatorycytokines.Tumornecrosisfactor
␣(TNF␣)andinterleukin6(IL-6)havebeenimplicatedaskey
componentsofimmuneandalsoinflammatoryprocesses.13
Animproved andbetter understanding ofthe relationship
betweenthesedifferentelementsmayhelpinthediscovery
ofnewapproachestoamelioratetheprogressionof
Theaimofthestudywastoevaluatethelevelofsome
pro-inflammatorymarkers(IL-6andTNF␣)andCoQ10in5---8
year-oldchildrenwithDS.
Methods
ThisprospectivestudyincludedallDownsyndromepatients presentingtotheClinicalGeneticsClinic,NationalResearch Centre,and outpatient clinic of New Children’s Hospital, whomettheinclusioncriteriaoveraperiodofeightmonths. Both the centre and hospital are general governmental establishmentsservingmiddle-andlow-incomepatients.
Thepatients’inclusioncriteria
CytogeneticallyprovenDownsyndromepatients,havingno congenitalanomalies or chronic diseases, aged5---8 years old,whoconsentedtoparticipateinthisinvestigation,were enrolledinthestudy.Theagegroup5---8yearswasselected, accordingtothefrequencyofyoungDScasesfulfillingthe inclusioncriteria. Atthetimeofbloodsampling,theyhad noacuteillnessesandwerenotonanytypeofmedications or supplements for at least one month. The study period wasdetermined by availabilityof kits. The control group consistedofhealthychildrenofsimilarageandsexfulfilling theinclusioncriteria.
IQassessmentanddeterminationofplasmaCoQ10 andcytokineslevels
Thisstudy wasblinded. Allsampleswerecodedand num-bered by the investigator responsible for collection of clinical data and only she had access tothe full data on the subjects. Intelligence quotient (IQ) assessmentswere done using the 4thedition of Wechsler Intelligence Scale forChildren(WISC-IV).14LevelsofCoQ10wereassayedbya
dedicatedhigh-performanceliquidchromatography(HPLC)
system with electrochemical detector (ECD) produced by
Shiseido Co. Ltd. (Tokyo, Japan). CoQ10 levels in plasma
weremeasuredasmol/L.Cytokinequantificationwas
con-ducted by ELISA using commercial kits for human TNF␣
and IL-6 (eBio-Science, CA, USA), according to the
man-ufacturer’s instructions. The presence and concentration
of cytokineswere identified by the intensity of the color
measuredbyspectrometryinamicroELISAreader.Plasma
levelsofhumanTNF␣andIL-6wereexpressedinpg/mL.An
OlympusAU400automaticanalyzer(OlympusCorporation,
Tokyo,Japan) wasusedto measure fastingblood glucose
withcommercialkits(RocheDiagnostics,IN,USA).
Therecruitmentandexperimentalprotocolsofthestudy
were conducted in compliance with the Declaration of
Helsinki (as revised in Edinburgh, 2000) and approved by
localethicalcommittee.Alllegalguardiansofparticipants
consentedtothestudy.
Statisticalanalysis
All data are expressed as mean±standard deviation. Correlation analyses were performed by calculating the Pearsoncorrelationcoefficient(r)toassesstherelationships
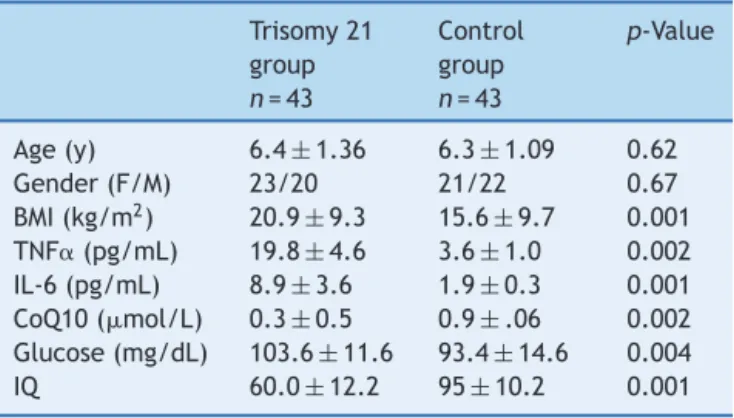
Table1 ClinicaldataandinvestigationsofstudiedDS chil-drenandcontrols.
Trisomy21 group n=43
Control group n=43
p-Value
Age(y) 6.4±1.36 6.3±1.09 0.62 Gender(F/M) 23/20 21/22 0.67 BMI(kg/m2) 20.9±9.3 15.6±9.7 0.001
TNF␣(pg/mL) 19.8±4.6 3.6±1.0 0.002
IL-6(pg/mL) 8.9±3.6 1.9±0.3 0.001 CoQ10(mol/L) 0.3±0.5 0.9±.06 0.002
Glucose(mg/dL) 103.6±11.6 93.4±14.6 0.004 IQ 60.0±12.2 95±10.2 0.001
BMI,bodymassindex; CoQ10,coenzyme Q10;DS, Down syn-drome; IL-6, interleukin 6; IQ, intelligence quotient; TNF␣, tumornecrosisfactor␣.
between the studied parameters. Statistical analysis was performedusingSPSSStatistics20.0forwindows(IBMSPSS StatisticsforWindows,Version20.0,NY,USA).The results wereconsideredstatisticallysignificantatthe0.05 signifi-cancelevel.
Results
Forty-threeDownsyndromepatientsand43controls were enrolledinaprospectivestudyfromJanuary2014toAugust 2014.Table1summarizesclinicaldata,BMI,and
investiga-tionsonthestudiedindividuals.
DSpatientshadsignificantlyhigherbodymassindex(BMI)
thancontrols(p=0.001).Also,TNF␣andIL-6levelswere
sig-nificantlyhigherinDSpatientscomparedtocontrols,with
p-valuesof0.002and0.001,respectively. TheCoQ10level
was significantly lower DS patients (p=0.002). The redox
statusof CoQ10 (%ofoxidized/total CoQ10) wasfoundto
be in the range of 28---35% in the plasma of DS children
comparedto8---12%in controls.The leveloffastingblood
glucose wassignificantlyhigher in DSpatients (p=0.004),
while theIQscoresignificantlylower(p=0.001) than
con-trols. The mean IQscore of DSpatients wasin the range
of mild mental disability. Table 2 summarizes the results
of Pearsoncorrelationcoefficients rbetweenCoQ10,
pro-inflammatory cytokines, and BMI. There was a significant
positivecorrelationbetweenCoQ10levelsandIQscores,as
wellasbetweenIL-6andTNF␣levels.
Discussion
It has been postulated that a triplicatedchromosome 21 causesa50%increaseintheexpressionoftrisomicgenesas aprimarydosageeffect,whichtranslatesdirectlyinto bio-chemicalaberrations.13,15Anumberofstudieshaveshown
thattrisomy21relatedincreaseofoxidativestressmightbe
involvedindifferentaspectsofDSphenotypes.4,16
In this study the inflammatory markers and oxidative
stress mechanisms in children with Down syndromes are
evaluatedandcomparedtocontrols.Inthepresentstudy,
allpatientsshowedsignificantdecreaseinplasmaCoQ10,a
Table2 CorrelationmatrixofCoQ10,pro-inflammatorycytokines,andvariousparametersinDSchildren.
CoQ10 TNF␣ IL-6 IQ BMI Glucose
CoQ10 1 −0.2 −0.2 0.4a 0.01 −0.3
TNF␣ 1 0.9b −0.2 −0.2 0.03
IL-6 1 −0.04 −0.2 0.04
IQ 1 0.2 −0.2
BMI 1 −0.09
Glucose 1
BMI,bodymassindex;CoQ10,coenzymeQ10;DS,Downsyndrome;IL-6,interleukin6;IQ,intelligencequotient;TNF␣,tumornecrosis factor␣.
a SignificantpositivecorrelationbetweenCoQ10levelsandIQscores. b SignificantpositivecorrelationbetweenIL-6andTNF
␣levels.
factorassociatedwithoxidativeimbalanceinchildrenwith trisomy21.Milesetal.6foundsignificantdecreaseofCoQ10
inDSpatients.AnotherstudybyTianoetal.17concludedthat
lymphocyteandplatelet CoQ10contentwere significantly
lowerinDSpatients,afactwhichprobablyunderlie
oxida-tiveimbalanceat thecellularlevel.However,thepresent
study included a larger number of patients, with an age
rangeof4years(5---8yearsofage).TheCoQ10redox
mech-anismispossiblyrelatedtomaintainingthemitochondrial
homeostasisandpreventionoffreeradicalproduction.
How-ever,studiescomparingdataonoxidativeDNAdamageand
systemicoxidative stress parametersin CoQ10-treated DS
patientsconcludedthatCoQ10doesnotsimplyworkasan
ROSscavenger.Thisisbecauseoftheabsenceofa
measur-ableplasmaantioxidantresponse,whichcouldbemasked
by the hyperuricemia usually found in DS, together with
unchangedDNAlevels.7
The cytokines IL-6 and TNF␣ are considered major
orchestratorsofbothimmuneandinflammatoryresponses.18
Thepresentstudy’sdatashowedsignificantincreaseinthe
pro-inflammatorymarkersIL-6andTNF␣levelinserum
col-lected from DS subjects, when compared to the control
group,asimilarfindingtootherstudies.13,19
High rates of overweight and obesity among children
worldwideandtherangeofhealthproblemsassociatedwith
themfrompsychosocialtoadversemetabolicfindings
war-rantdevelopmentofanumberofaction plansandsetting
of global targetsfor the preventionof obesity inchildren
andadolescents.Newpreventivestrategies,highlightingthe
importantroleofphysicalactivityandnutritioneducation,
arenecessary.Individual,family,andcommunityvariations
canaffecthavingahealthylifestyle.20,21
High BMI is associated with a specific pattern of
low-gradeimmuneactivation.22Thepresentstudy’sdataconfirm
previously described associations between DS and high
BMI.23,24The meanIQscoreofthestudiedDSpatientswas
60.0±12.2. Gardiner,in 2014,25 delineatedthat although
intellectualdisabilityinDScanbeonlymilddelay,themost
frequentlyreportedIQisintherangeof40---50(mildto
mod-eratedelay). Shuklaetal.26 reportedthattheIQscoreof
theDSpatientshadmoderatementaldisabilityin31%and
mild mental disability 52% of their patients. The
correla-tionofCoQ10levelstoIQscoresinDSpatientssignifiesthe
CoQ10effectonneurodevelopmentthatmaybeduetoits
protectiveroleagainstnuclearDNAdamage,inadditionto
itsredoxrole.5Itiswell-knownthatdiabetesmellitushasa
higherprevalenceinDSthaninthegeneralpopulation,27,28
while in the present findingsthe blood glucose level was
withinnormal,whichmaybeexplainablebytheyoungage
ofthepatients.Theimportanceoftheseresultsfrom
clini-calandtherapeuticpointsofviewisthatitemphasizesthe
importanceof a proper follow-up strategy for DS
individ-uals,andaidstooutlinenovelstrategiesforthetreatment
ofpatientswithDS.
In conclusion, the levels of Il-6, TNF␣, and CoQ10 in
youngDSpatients mightrepresent akey-contributing
fac-tortotheneurodegenerativeprocessthatculminatesinDS.
CoenzymeQ10shouldbeconsideredagoodsupplementin
youngchildrenwithtrisomy21toamelioratethe
neurolog-icalsymptoms.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.PerluigiM,PupoG,TramutolaA,Cini C,CocciaR,BaroneE, etal.NeuropathologicalroleofPI3K/Akt/mTORaxisinDown syndromebrain.BiochimBiophysActa.2014;1842:1144---53. 2.Martínez-Cué C, Delatour B, Potier MC. Treating enhanced
GABAergic inhibition in Down syndrome: use of GABA ␣5-selective inverse agonists. Neurosci Biobehav Rev. 2014;46:218---27.
3.Tiano L, Carnevali P, Padella L, Santoro L, Principi F, Brugè F,etal.Effect ofcoenzyme Q10inmitigating oxidativeDNA damageinDownsyndromepatients,adoubleblindrandomized controlledtrial.NeurobiolAging.2011;32:2103---5.
4.PerluigiM,ButterfieldDA.OxidativestressandDownSyndrome: aroutetowardAlzheimer-likedementia.CurrGerontolGeriatr Res.2012;2012:724904.
5.Tiano L, Padella L, SantoroL, Carnevali P,Principi F, Brugè F, et al. Prolonged coenzyme Q10 treatment in Down syn-drome patients: effect on DNA oxidation. Neurobiol Aging. 2012;33:626,e1---8.
6.MilesMV,PattersonBJ,Chalfonte-EvansML,HornPS,HickeyFJ, SchapiroMB,etal.CoenzymeQ10(ubiquinol-10) supplemen-tationimproves oxidativeimbalanceinchildrenwithtrisomy 21.PediatrNeurol.2007;37:398---403.
8.NainiA,LewisVJ,HiranoM,DiMauroS.PrimarycoenzymeQ10 deficiencyandthebrain.Biofactors.2003;18:145---52. 9.MortensenSA.OverviewoncoenzymeQ10asadjunctivetherapy
in chronicheartfailure. Rationale,designand end-pointsof ‘‘Q-symbio’’---amultinationaltrial.Biofactors.2003;18:79---89. 10.Littarru GP, Tiano L. Clinical aspects of coenzyme Q10: an
update.Nutrition.2010;26:250---4.
11.MuchováJ, ˇZitˇnanováI, ˇDuraˇckováZ.OxidativestressandDown syndrome.Doantioxidantsplayaroleintherapy?PhysiolRes. 2014;63:535---42.
12.Nateghi Rostami M, Douraghi M, Miramin Mohammadi A, NikmaneshB.Alteredserumpro-inflammatorycytokinesin chil-drenwithDown’ssyndrome.EurCytokineNetw.2012;23:64---7. 13.Rodrigues R, Debom G, Soares F, Machado C, Pureza J, Peres W, et al. Alterations ofectonucleotidases and acetyl-cholinesterase activities in lymphocytes of Down syndrome subjects: relation with inflammatory parameters. Clin Chim Acta.2014;433:105---10.
14.WechslerD.WechslerIntelligenceScaleforChildren: adminis-trationandscoringmanual.4thed.SanAntonio,TX,USA:The PsychologicalCorporation;2003.
15.Abdel-SalamE,Abdel-MeguidI,KorraaS.Assessmentofimmune functioninDownsyndromepatients.EgyptJMedHumGenet. 2013;14:307---10.
16.Garrido-Maraver J, Cordero MD, Oropesa-Ávila M, Fernández VegaA,delaMataM,DelgadoPavónA,etal.CoenzymeQ10 therapy.MolSyndromol.2014;5:187---97.
17.Tiano L, Padella L, Carnevali P, Gabrielli O, Bruge F, Prin-cipi F, et al. Coenzyme Q10 and oxidative imbalance in Downsyndrome:biochemicalandclinicalaspects.Biofactors. 2008;32:161---7.
18.AureliA, Sebastiani P,Del BeatoT, Marimpietri AE,Graziani A, Sechi E, et al. Involvement of IL-6 and IL-1 receptor
antagonistonintellectualdisability.ImmunolLett.2014;162: 124---31.
19.ShimadaA,HayashiY,OgasawaraM,ParkMJ,KatohM,Minakami H,etal.Pro-inflammatorycytokinemiaisfrequentlyfoundin Down syndrome patients withhematological disorders. Leuk Res.2007;31:1199---203.
20.deOnisM.Preventingchildhoodoverweightandobesity.J Pedi-atr(RioJ).2015;91:105---7.
21.GuerraPH,da Silveira JA,Salvador EP. Physicalactivityand nutritioneducationattheschoolenvironmentaimedat pre-ventingchildhoodobesity:evidencefromsystematicreviews.J Pediatr(RioJ).2016;92:15---23.
22.MagroneT,JirilloE.Childhoodobesity:immuneresponseand nutritionalapproaches.FrontImmunol.2015;6:76.
23.RealdeAsuaD,ParraP,CostaR,MoldenhauerF,Suarez C.A cross-sectionalstudyofthephenotypesofobesityandinsulin resistancein adultswithDown syndrome.Diabetes MetabJ. 2014;38:464---71.
24.AfifiHH,AglanMS,ZakiME, ThomasMM,TossonAM.Growth charts of Down syndrome in Egypt: a study of 434 chil-dren 0---36 months of age. Am J Med Genet A. 2012;158A: 2647---55.
25.Gardiner KJ. Pharmacological approaches to improving cog-nitive function in Down syndrome: current status and considerations.DrugDesDevTher.2014;9:103---25.
26.ShuklaD,Bablani D,ChowdhryA,Thapar R,Gupta P,Mishra S.Dentofacialand cranialchangesinDownsyndrome.Osong PublicHealthResPerspect.2014;5:339---44.
27.Roizen NJ, Patterson D. Down’s syndrome. Lancet. 2003;361:1281---9.