w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Rituximab
as
an
alternative
for
patients
with
severe
systemic
vasculitis
refractory
to
conventional
therapy:
report
of
seven
cases
and
literature
review
Leonardo
Sales
da
Silva
a,
Karla
Valéria
Miranda
de
Campos
b,
Ana
Karla
Guedes
de
Melo
b,
Danielle
Christinne
Soares
Egypto
de
Brito
b,c,d,
Alessandra
Sousa
Braz
b,c,d,
Eutilia
Andrade
Medeiros
Freire
b,c,d,∗aMedicineSchool,UniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil
bDepartmentofRheumatology,HospitalUniversitárioLauroWanderley,UniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil cMedicalCourse,UniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil
dDepartmentofInternalmedicine,MedicalSciencesCenter,UniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14November2014 Accepted1July2015
Availableonline12September2015
Keywords:
Rituximab
Systemicvasculitides
Granulomatosiswithpolyangiitis Microscopicpolyangiitis Polyarteritisnodosa
a
b
s
t
r
a
c
t
Thegreaterunderstandingofpathophysiologyandbehaviorofsystemicvasculitis,together with thedevelopmentoftherapeuticregimens withincreasinglybettersafety and effi-cacyprofiles,dramaticallychangedtheprognosisofpatientsdiagnosedwiththeseclinical entities.Recently,theuseofrituximabinthetreatmentofpatientswithANCA-associated vasculitisinrandomizedclinicaltrialsshowedanimportantalternativeinselectedcases, especially patientsrefractoryor intoleranttostandardtherapy withcyclophosphamide andcorticosteroids.Thisarticlepresentsthereportofsevencasesofsystemicvasculitis successfullytreatedwithrituximab.
©2015ElsevierEditoraLtda.Allrightsreserved.
O
rituximabe
como
uma
opc¸ão
para
pacientes
com
vasculite
sistêmica
grave
refratária
à
terapia
convencional:
relato
de
sete
casos
e
revisão
de
literatura
Palavras-chave:
Rituximabe
Vasculitessistêmicas
r
e
s
u
m
o
O maior entendimento das bases fisiopatológicas e do comportamento das vasculites sistêmicas,aliadoaodesenvolvimentoderegimesterapêuticoscomperfildeseguranc¸a e eficácia cada vezes melhores,modificou drasticamente o prognóstico dos pacientes
∗ Correspondingauthor.
E-mailaddresses:eutiliafreire@hotmail.com,leonrd0@hotmail.com(E.A.MedeirosFreire). http://dx.doi.org/10.1016/j.rbre.2015.07.016
Granulomatosecompoliangeíte Poliangeítemicroscópica Poliarteritenodosa
diagnosticados com essas entidades clínicas.Recentemente, oemprego do rituximabe no tratamentode pacientescom vasculitesANCAassociadas em ensaiosclínicos ran-domizados se mostrou uma opc¸ão importante em casos selecionados, especialmente pacientesrefratáriosouintolerantesàterapia-padrãocomciclofosfamidaecorticosteroides. Opresenteartigotrazorelatodesetecasosdevasculitessistêmicascomtratamento bem-sucedidocomrituximabe.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Theintroductionofglucocorticoidsand,later,of cyclophos-phamide(CYC)ininducingremissionofsystemicvasculitis (SV) dramaticallychanged the prognosis ofthese patients, resultinginsymptomaticimprovement,highratesof remis-sion and in increased survival.1,2 However, a significant
portionofpatientsremains refractoryor intolerantto con-ventionaltherapies,3justifyingthegrowing interestinnew
saferandmoreeffectivetherapeuticoptions.Recentevidence pointstoacrucialroleofBlymphocytesinthedevelopment ofSV.4Rituximab(RTX)isachimericanti-CD20+Bcell
mono-clonalantibodywidelyusedinBcelllymphomas,andmore recentlyhasbeenusedforvariousautoimmuneconditionsin selectedcases.
We report seven cases of patients diagnosed with SV treatedsuccessfullywithRTX.
Case
report
Patient1
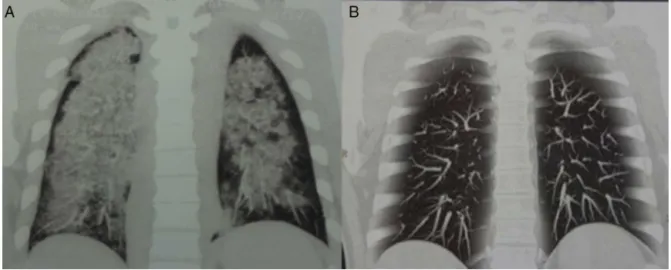
Male,46,withfever,weightloss,severepulmonary vasculi-tis(Fig.1),pauci-immuneglomerulonephritisandneuropathy of lower limbs, with Birmingham Vasculitis Activity Score (BVAS)=20andANCA-negative.Treatedunderadiagnosisof microscopic polyangiitis (MPA), subjected to pulse therapy withmethylprednisolone(MP)followedbycyclophosphamide associatedwithprednisone40mg/day.Thepatientdeveloped hyperglycemia and liver toxicity; thus, this treatment was suspended, with the introduction of weekly doses of RTX 375mg/m2for4weeks.Afterayearoftreatment,thepatient
achievedcompleteremissionwithoutmaintenancetherapy.
Patient2
Female,31,presentingedemaandfixedcyanosisof extremi-ties,polyarthralgia,subcutaneousnodules,limbischemiaand acuterespiratoryfailure(BVAS=15),withadiagnosisof pol-yarteritisnodosa(PAN)andHBsAgpositivefor6years.Skin biopsyshowedfibrinoidnecrosisandmedium-calibervessel infiltration.SubjectedtopulsetherapywithMPandCYCwith poorresponse. Treatmentwas started withtwo fortnightly dosesofRTX1g,withdramaticimprovement.Treatedwith amaintananceinfusionofRTXafter6months,maintaining completeremissionwithoutsteroids.
Patient3
Male, 56,admittedwith arthritis,nephritis,retinal vasculi-tis,pulmonarynodulesandperipheralneuropathy(BVAS=17). Withadiagnosisofgranulomatosiswithpolyangiitis(GPA)for 3years withcANCA 1/40,refractoryto7pulsesofMP and CYC. Afterrescue therapy with 4weekly infusions ofRTX 375mg/m2,thepatientshowedcompleteremissionofthe
dis-easeforthreeyears,withmaintenancetherapywithRTXevery 6months.
Patient4
Female,47,withongoingfever,weightloss,hearingloss, pal-pable purpura, glomerulonephritis and hemoptysis for the duration of 3 years (BVAS=38 at admission), with a diag-nosisofGPA.AchestCTscanrevealedmultiplepulmonary cavitations.Ancillaryandtherapeutictestsnegativefor tuber-culosis,withsubsequentweeklyRTXinfusionfor4weeks.The patientremainsincompleteremissionafter1year,without maintenancetherapy.
Patient5
Male,26,withanearlyweightloss,arthritis,sinusitis, conjunc-tivitisandabdominalpainfor5months(BVAS=12),pANCA 1/20.Afterrulingoutdifferentialdiagnoses,thepatientwas treatedaswithGPA,beginningwithtwobiweeklyinfusions ofRTX.Amaintenanceschedulewithhalf-yearlyinfusionsof RTXwaschosen.
Patient6
Male,24,withmanifestationsofnephritisandwithabiopsy revealingpauci-immuneglomerulonephritis,compatiblewith adiagnosisofMPA,refractorytomultiplepulsesofMPand CYCover5years.Aschemeof4weeklyinfusionsofRTXwas started,withearlyBVAS=12,achievingcompleteremission; asmaintenance,half-yearlyinfusionswerescheduled.
Patient7
Fig.1–ChestCTcoronalreconstructionofpatient1.(A)Viewpriortotreatment,showingdiffuseopacitiescompatiblewith diffusealveolarhemorrhageandpulmonarycapillaritis.(B)Viewafterrituximabtherapy,showingregressionoflesions.
Discussion
Systemic vasculitides (SV) are a heterogeneous group of conditions whose main landmark is a primary inflamma-tion and damage to blood vessels with subsequent tissue ischemiaand/orvascularhemorrhage.Manyare the condi-tionsthatfitthisclinical-pathologicalprofile,affectingvessels ofdifferentsizesindifferentorganicsystemswithvariable intensity.5
Amongthecasesdescribed,adiagnosisofMPAforpatients 1, 6 and 7 were proposed, and patients 3, 4 and 5 were diagnosedwithGPA,whilepatient2wastreatedunderthe hypothesis of PAN. Although GPA and MPA are classically referredtoasANCA-associatedvasculitides(AAV),patients1, 4and6hadanegativeANCA,aphenotypealsoreferredtoas seronegativevasculitisbysomeauthors,withinvolvementof 10%ofcases.5
SVsare wellrecognizedfortheir potentialseverity, with anoftenacceleratedevolutionandresultingindeathifnot treatedproperly.Priortotheintroductionofeffectivetherapies forSV,thefive-yearsurvivalratewasaround10%,incontrast toover80%reportedintheliteratureaftertheintroductionof CYCandcorticosteroids.1,2
Thetreatment with CYC, however, is not without seri-ousadverseevents,suchasmyelosuppression(2%),infections (46%),neoplasms(2.8%),andinfertility(57%).6 Furthermore,
the5-yearrecurrenceriskforpatientstreatedappropriatelyis 38%.3Thecurrentscenariohasmotivatedagrowinginterestin
newtherapeuticagentsforSVasdrugsofchoiceoralternative medicationsincarefullyselectedcases.
Evidencesupportsawell-establishedpathogenicroleofB cellsinthedevelopmentofautoimmunediseases.Amongthe proposedmechanisms,isthefactthatBcellsareprecursors ofANCA-producing plasmacells,besidestheproductionof cytokinescriticalforthedevelopmentofT-cellhyperactivity andstimulatingproliferationandactivationofneutrophils.4
Thesefactorsconstitutedthepremiseforexperimental stud-ies evaluatingthetherapeuticresponseofpatientswithSV undergoinginfusionofRTX.
RTX is a chimeric anti-CD20+ B-cell monoclonal anti-body,whichselectivelyinducesdepletionofBcellsthrough direct stimulation of apoptosis, antibody-dependent cyto-toxicity and complement-dependent cytotoxicity.7 Thefirst
report onthe use ofRTXin inducingremissionof SVwas publishedin2001bySpecketal.8 Sincethen,multiplecase
reports and studies were published, including two large, controlled trials (RITUXVAS and RAVE) that demonstrated non-inferiority ofinduction therapywithRTXcomparedto conventionaltherapywithCYC.9,10TheRITUXVASstudywas
publishedin2010byJonesetal.,including44patientswith newlydiagnosedAAVwithrenalinvolvementwithoutprior treatment;thesepatientswererandomizedintotwogroups, CYCandRTX.9TheresultsoftheRAVEstudywererecently
published by Specks et al. and included 197 patients in a multicenter,randomized,double-blindnon-inferioritystudy that compared RTX with daily oral CYC for induction of remissionofAAV.10Theauthorsconcludedfornon-inferiority
ofRTX versusCYC forinductionofremission,9,10 and RTX
appearstobemoreeffectiveincasesofrelapse.10However,
contrary towhatwasanticipated,therewere nosignificant differencesinseriousadverseeventratesbetweenthesetwo groups.10
Recommendations about indicationtime forRTX as an inducer ofSV remission vary.Themain recommendations refer to AAV; thus, it is still uncertain whether these can be extrapolated to ANCA-disease negative phenotypes in patients with GEPA, GPA and MPA or other forms of SV. Therearenocomparativedataoncost-effectivenessbetween RTX and CYC. In general, RTX is indicated as first choice whenthetreatmentaimistryingtoavoidtheadverseevents relatedtoCYC,especiallyinyoungpatientswith reproduc-tiveaspirations.3,11Thismatterwasdecisiveforthedefinition
wasinitiallytreatedwithRTX.OthersituationsinwhichCYC mustbeavoidedincludeahighcumulativedose, hypersen-sitivityand high riskofmalignancy.3,11 Another consistent
indicationofRTXisforrescuetherapyinpatientsrefractory to conventional therapy due to intolerance or unsatisfac-tory response; this occurs in 13–30% of cases,11 including
patients1,2,3and7describedinthispaper,withthefirst ofthemduetopharmacologicalschemeintoleranceandthe other due to poorresponses. patient 4 receivedher initial treatment with a two-week corticoid pulse and an empir-ical regimen for tuberculosis, with severe evolution; thus, thispatientwassubjectedtoaninductionwithRTX. Appar-ently RTX shows better results in patients with relapsing disease and can be recommended as first choice in these cases.11
Patients1,3,4,6and7weresubjectedtofourinfusionsof RTX,375mg/m2perdose,at1-weekintervals,whilepatients2
and5receivedtwobiweeklyinfusionsof1g.Differentinfusion schemesmaybeusedforinductionofremissioninpatients with SV.The mainevidence refers to lymphoma protocol, 375mg/m2/weekfor4weeks,usedbymoststudies,including
RITUXVASandRAVE.9,10 Aminorityofauthorsoptedbythe
schemecommonlyusedinrheumatoidarthritis,withan infu-sionoftwodosesof1gintravenouslyatanintervalof15days. Theprotocolsusedforlymphomaand rheumatoidarthritis appeartobeequallyeffectiveinAAV,beingnon-inferiorto conventionaltherapy.11Aretrospectivemulticenterstudyof
65patientsconductedbyJonesetal.showednosignificant differencebetweentheremissionratesforbothschemes(81% withlymphomaprotocolversus75%withrheumatoidarthritis protocol).11
AlthoughthereisconvincingevidencethatRTXisan effec-tivealternativeforinductionandmaintenanceofremissionof AAV,itsroleinpatientswithANCA-negativeSVisstill uncer-tain.Thefactthatevenpatients1,4and6describedinthis paper,besidespreviousreports,12,13 allwithANCA-negative
subjects,haveshownsatisfactoryresponsesduringinduction therapysuggeststhatRTXmayplayaroleevenintheabsence ofsuchantibodies,actingthroughother pathogenic mech-anismsrelatedtoBcells,forinstance, apossibleinfluence ontheprocessofantigenpresentationandco-stimulationof B-celldependentTcells.7
Lesssignificantevidencehasbeenpresentedastotherole ofRTXinthetreatmentofpatientswithPAN.Studiessuggest thatinmost casesthepathogenesisofPAN are associated withcirculatingimmunecomplexdepositionand/or vascu-larformationinsitu,comprisedbyHBeantigenandspecific antibodies.Thesefactorsthen inducethecomplement cas-cadeactivationandmonocyteandneutrophilrecruitment.5
Thus,theintroductionofRTXasapossibletherapeuticagent forpatientswithPANisbasedonthedepletionof antibody-producingB-cells.7 Thereisnoinformationavailableinthe
literatureonrandomizedtrialscomparingstandardinduction therapyversusRTXinpatientswithPAN, althoughisolated reportspointtosatisfactoryresultsinselectedcases,14,15such
aswithpatient2,whoreachedcompleteremissiondespitethe severeactivityofadiseaserefractorytoconventionaltherapy, requiringherintensivecareunitadmissionforventilatoryand hemodynamicsupport.
Current knowledgeinvolving therapiesforSVremission inductionpointstoaconstant needtodevelopincreasingly effectiveandsafetherapeuticregimens.Withtheintroduction ofRTXasanalternativetoCYCinrefractorycases,orinthose patientswhomconventionaltherapyshouldbeavoided,there was a significant increase in published rates ofsuccessful inductionofremission.However,shortandlongtermadverse eventsassociatedwithavailableschemescontinuecausinga majorconcern.Thecasesdescribedinthispapercorroborate the dataintheliterature,andRTXisagoodalternativefor inductionofremissioninrefractorypatientsorinthosewitha contraindicationtoCYCscheme.Randomizedtrialswith rep-resentativesamplesareneededtoconfirmassumptionsabout theefficacyandsafetyofRTXinpatientswithPANorGPAand ANCA-negativeMPA.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.LhoteF,CohenP,GuillevinL.Polyarteritisnodosa, microscopicpolyangiitisandChurg-Strausssyndrome. Lupus.1998;7:238–58.
2.FauciAS,WolffSM.Wegener’sgranulomatosis:studiesin eighteenpatientsandareviewoftheliterature.Medicine (Baltimore).1994;73(6):315–24.
3.AlbericiF,JayneDR.Impactofrituximabtrialsonthe treatmentofANCA-associatedvasculitis.NephrolDial Transpl.2014;29(6):1151–9.
4.DornerT,JacobiAM,LipskyPE.Bcellsinautoimmunity. ArthritisResTher.2009;11(5):247–56.
5.LangfordCA,FauciAS.Thevasculitissyndromes.In:Longo DL,etal.,editors.Harrison’sprinciplesofinternalmedicine. 18thed.NewYork:McGraw-Hill;2012.
p.2785–801.
6.HoffmanGS,KerrGS,LeavittRY,HallahanCW,LebovicsRS, TravisWD,etal.Wegenergranulomatosis:ananalysisof158 patients.AnnInternMed.1992;116(6):488–98.
7.WeinerGJ.Rituximab:mechanismsofaction.SeminHematol. 2010;47:115–23.
8.SpecksU,FervenzaFC,McDonaldTJ,HoganMC.Responseof Wegener’sgranulomatosistoanti-CD20chimericmonoclonal antibodytherapy.ArthritisRheum.2001;44:2836–40.
9.JonesRB,TervaertJW,HauserT,LuqmaniR,MorganMD,Peh CA,etal.Rituximabversuscyclophosphamidefor
ANCA-associatedrenalvasculitis.NEnglJMed. 2010;363(3):211–20.
10.SpecksU,MerkelPA,SeoP,SpieraR,LangfordCA,Hoffman GS,etal.Efficacyofremission-inductionregimensfor ANCA-associatedvasculitis.NEnglJMed.2013;369(5): 417–27.
11.GuerryMC,BroganP,BruceIN,D’CruzDP,HarperL,Luqmani R,etal.Recommendationsfortheuseofrituximabin anti-neutrophilcytoplasmantibody-associatedvasculitis. Rheumatology.2012;51(4):634–43.
13.KhanA,LawsonCA,QuinnMA,IsdaleAH,GreenM. SuccessfultreatmentofAnca-negativeWegener’s granulomatosiswithrituximab.IntJRheumatol. 2010;2010:846063.
14.SonomotoK,MiyamuraT,WatanabeH,TakahamaS, NakamuraM,AndoH,etal.Acaseofpolyarteritisnodosa
successfullytreatedbyrituximab.NihonRinshoMeneki GakkaiKaishi.2008;31(2):119–23.