especialidade de Cardiologia
Júri:
Presidente: Doutor José Augusto Gamito Melo Cristino, Professor Catedrático e Presidente do Conselho Científico da Faculdade de Medicina da Universidade de Lisboa.
Vogais:
- Doutor Lino Manuel Martins Gonçalves, Professor Catedrático da Faculdade de Medicina da Universidade de Coimbra;
- Doutor Henrique José Cyrne de Castro Machado Carvalho, Professor Convidado do Instituto de Ciência Biomédicas Abel Salazar da Universidade do Porto;
- Doutor Fausto José da Conceição Alexandre Pinto, Professor Catedrático da Faculdade de Medicina de Lisboa (Orientador);
- Doutor António Cândido Vaz Carneiro, Professor Associado com Agregação da Faculdade de Medicina de Lisboa;
- Doutora Ana Maria Gomes de Almeida, Professora Associada com Agregação da Faculdade de Medicina da Universidade de Lisboa;
- Doutora Dulce Alves Brito, Professora Auxiliar Convidada da Faculdade de Medicina da Universidade de Lisboa.
The texts published in this thesis had the authorization by the editors where they were originally published, to be here reproduced.
Learning is a treasure that will follow its owner everywhere.
Chinese proverb
At this stage of my medical journey, I take this opportunity to reflect on the motivation behind my PhD. At the beginning of my career as a specialist, I had the opportunity to be involved in an academic project. By then, though, all my efforts were focused on achieving the greatest possible experience on interventional cardiology and in the desire to expand it to regional hospitals which had hardly any access to it. By that time, in the late eighties, early nineties of the past century, intervention cardiology was a discipline concentrated in a few hospitals and with scarce possibilities of access by young cardiologists. After the initial training with Professors Amadeo Betriu and António Serra in Barcelona, it was in Santa Cruz Hospital, with professor Seabra Gomes, that I found a place where clinical practice, teaching and research live together in a way that I felt I could be identified with. Taking into account that experience which ultimately boosted my development project of intervention cardiology at Hospital Garcia de Orta. Innovation and new technologies are essential for the development of healthcare systems. But without efficient integration, they represent only a rise in costs without health results. It’s important that, in their training, health professionals can acquire management skills which enable them to have instruments to maximize resource management.
Acute coronary syndromes in recent years have been targeted by major innovation both in medical devices and pharmaceuticals. Because treatment is heavily dependent on the time in which it is administered, and because resources are not available in a well-distributed manner, there is a need for optimisation of all stages in the chain - from diagnosis to treatment.
I have always had a great interest in myocardial infarction. Not only on the disease and all the complexity in the physiopathology involved and possibilities of therapeutic improvement, but also in preventive measures, on clearly identified risk factors and the best ways to improve patient rehabilitation. It was within the scientific community, the Portuguese Society of Cardiology - initially within the Working Group of Interventional Cardiology and subsequently in the Portuguese Association of Cardiovascular Intervention - that I found the main instruments which enabled me to help the improvement of the performance in the national approach to acute coronary syndromes. From an early stage in my career, I was aware that physicians devoted much of their time on “what to do” then “how to do”. The acute myocardial infarction is a paradigm of this phenomenon.
Technological developments have allowed a great improvement in clinical results. At the same time, detailed guidelines that indicate the best ways to achieve these results have been published. The bottom line is that, in daily practice, many patients are still not treated in accordance with the guidelines.
Although every one of us give our best to treat the patient according to leges artis, the complexity involved in the entire chain, mostly on the organizational level - particularly in communication - led to worst results than expected. Knowing that I needed a better knowledge of these organizational processes led me to attend a post-graduation and a master`s degree in management in health organizations. The master´s thesis, which I discuss in 2009, under the theme “Risk management in primary angioplasty”, aimed to identify the main “failures” in the treatment of myocardial infarction and the search for solutions to overcome them. It was on that same year that we saw the birth of a project of the European Society of Cardiology (ESC): “Stent for Life” (SFL). This matched what I was already looking for some time: an initiative to allow the registration and the characterization of primary angioplasty in Portugal, as well as to investigate the main obstacles to good system performances, along with the implementation of specific programmes that would enable the improvement of the entire chain of events involved in the complexity of acute coronary syndromes in general, and STEMI in particular. Since its beginning, in 2002, we have given the greatest attention and tried to contribute to the success of the registries of the Portuguese Society of Cardiology. A project so complete as SFL, looks not only to the moment of the myocardial infarction, but its
prevention and rehabilitation. For that, it is necessary to monitor and assess tools which allow us to understand where we came from, where we are at the moment, and where we want to go. Given the fact that PSC registries are continuous, unaudited and volunteer dependent, we obtained an authorization from the National Data Collection Centre in Cardiology (CNPD), to collect the data in a prospective way, once a year, during a month period. We essentially collect the data related to the performance of the treatment of myocardial infarction, particularly the data related to the primary angioplasty access and time delays in the circuit. All cardiology centres in Portugal mainland participated in this annual survey, which allow us to get a very reliable perspective of primary angioplasty and the main barriers to its performance.
SFL international had precise objectives, obtained quantitatively, with focus on the number of primary angioplasties per year and per million inhabitants. Since the beginning, we consider that this quantitative target was also important to gather qualitative elements. In myocardial infarction, it is not only important to treat more patients, but to treat them as quickly as possible. On the other side, we must be aware that these projects required the help of experts in management of health organizations. We found that help at ISCTE, having received the support of Professor Luís Martins. Under this collaboration, we conducted a market survey, on a national level, which allowed us to perceive that an important percentage of the Portuguese population still ignores heart attack symptoms. We find out a clear need for rapprochement between the medical pragmatic approach of the main barriers to the good performance of the healthcare organizations with the specialized vision of management schools. At present, there are paths of research based on theoretical contributions of studies on the impact of certain projects as “change agents” of the healthcare institutions. The analysis of success factors, the evaluation of leadership, compliance of the participants, the role of professional associations, the so called “relation coordination” are key elements of analysis that in our opinion should be further integrated in this project soon.
I would like to thank all who, directly or indirectly, contributed to the realization of this project.
To Prof. Fausto Pinto for his full support, availability and precious advice. To Prof. Luis Martins, who gave me a wider vision of healthcare organizations and new lines of research.
A very special thanks to Dr. Sofia de Mello, who embraces SFL initiative since the beginning with great enthusiasm and further contribute to its success. Since the first moment, Sofia was a project enthusiast. She and I discussed almost every day and in detail, all the programs that we were building and planning tasks that were far beyond the moment of primary angioplasty, and included primary prevention, rehabilitation and education.
A very special thanks to Dr. Ernesto Pereira, for his encouragement and his cooperation in data collection, and for his friendship.
To Dr. Silvia Vitorino, and to Dr. Rita Calé for their cooperation in data collection and analysis.
To APIC presidents: Dr. Leitão Marques for having supported the candidacy of SFL process, and to Dr. Rui Campante Teles, who supported the continuation of the program. I’m also thankful to Dr. Lidia de Sousa, Dr. Manuel Almeida and Dr Marco Costa for supporting the project and great help in all organizational APIC and tasks. To Dr. Silvia Monteiro, Dr. Pedro Jerónimo de Sousa, Dr. Jorge Mimoso, Dr. Jorge Marques and Dr. Renato Fernandes for the organization of regional and educational SFL programs.
To Dr. Pedro Coelho dos Santos for his help in the communication campaigns and to Dr. João Ferreira for inspiring ideas and support for the project.
To INEM presidents, particularly to Dr. Miguel Oliveira and to Dr. Luis Meira, who have always been partners, and for their help in our efforts to find new ways to improve treatment of myocardial infarction. Dr. Raquel Ramos for all the availability and operational assistance between the interventional intervention centers and the pre-hospital medical emergency.
To all the” Stent for Life” ambassadors in Portugal, who unselfishly collaborated in the information campaign “Não Perca Tempo - Salve uma Vida” (Act Now - Save a Life), highlighting the collaboration of José Carlos Malato.
To all the doctors, nurses and technicians, in hospitals, who have given their best so that primary angioplasty is offered in time, to patients with myocardial infarction. This work is dedicated to my wife Dinora, my daughters Ana Luísa and Filipa and my mother Lina, for their support over the years.
Preface . . . I acknowledgements . . . IV lIst of abbreVIatIons . . . IX
abstract . . . 1
resumo . . . 7
CHAPTER I: GEnERAl InTRoduCTIon, objECTIvEs And METHods 1 .1 Introduction . . . 13
1 .2 general study objective . . . 17
1 .3 specific objectives . . . 17
1 .4 methods . . . 18
CHAPTER II: PoRTuGuEsE REGIsTRY oF InTERvEnTIonAl CARdIoloGY 2 .1 the 2002 Portuguese Interventional cardiology registry . . . 25
2 .2 the Portuguese Interventional cardiology registry from 1992 to 2003 . . . 33
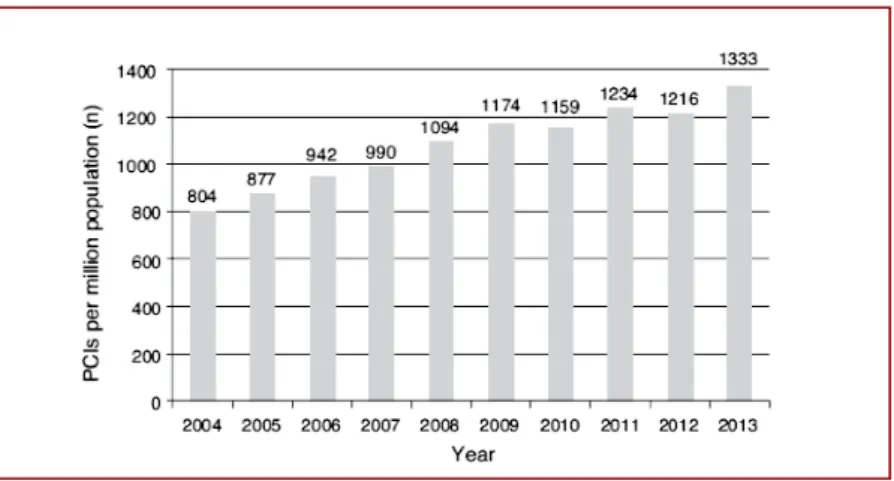
2 .3 trends in Percutaneous coronary Intervention from 2004 to 2013 according to the Portuguese national registry of Interventional cardiology . . . 47
2 .4 elective and Primary angioplasty at Hospitals without on-site surgery versus with on-site surgery: results from a national registry . . . 66
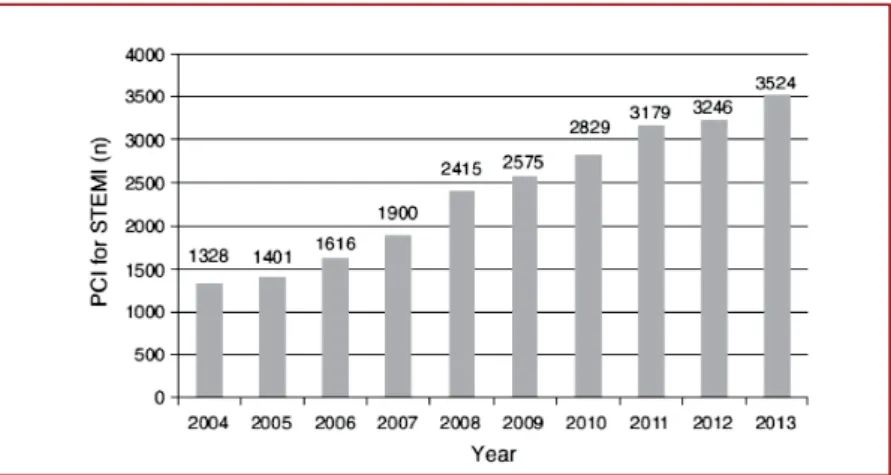
CHAPTER III: PRIMARY AnGIoPlAsTY In PoRTuGAl 3 .1 trends in Primary angioplasty in Portugal from 2002 to 2013 according to the Portuguese national registry of Interventional cardiology . . . 81
CHAPTER Iv: THE ‘sTEnT FoR lIFE’ InITIATIvE 4 .1 stent for life in Portugal: this initiative is here to stay . . . 95
4 .2 Primary angioplasty in Portugal: door-to-balloon time is not a good performance index . . . 110
CHAPTER v: PREdICToRs oF PATIEnT And sYsTEM dElAYs
5 .1 factors Influencing the Patient delay to Primary angioplasty in myocardial Infarction with st-segment elevation (stemI):
the stent for life Initiative in Portugal . . . 121
5 .2 stent for life Initiative: Predictive factors of system delay in Patients with st-segment elevation myocardium Infarction . . . 144
CHAPTER vI: ovERAll dIsCussIon And ConClusIons 6 .1 overall discussion and conclusions . . . 163
6 .2 limitations of the study . . . 178
6 .3 conclusions and future Perspectives . . . 179
acc – american college of cardiology aHa – american Heart association
amI – acute myocardial infarction
aPIc – Portuguese association of cardiovascular Intervention bls – basic life support
cabg – coronary artery bypass graft
cards – cardiology audit and registration data standards cI – confidence interval
cncdc – national center for data collection in cardiology codu – referral center for emergency Patients
cVd – cardiovascular disease des – drug-eluting stents
dgs – directorate-general of Health dm – diabetes mellitus
d2b – door-to-balloon d2d – door-to-door
eaPcI – european association of Percutaneous cardiovascular Interventions ecg – electrocardiogram
ems – emergency medical service esc – european society of cardiology fmc – first medical contact
Ils – Immediate life support
Inem – national Institute for medical emergencies IVus – Intravascular ultrasound
IQr – Interquartile ranges
merV – major emergency response vehicle mI – myocardial infarction
nstemI – non st-segment elevation myocardial infarction oct – optical coherence tomography
oHca – out of hospital cardiac arrest PcI – Percutaneous coronary intervention
P-PcI – Primary percutaneous coronary intervention Psc – Portuguese society of cardiology
rncI – national registry of Interventional cardiology sfl – stent for life
stemI – st-segment elevation myocardial infarction
Keywords: Patient delay; system delay; Predictive factors;
st-segment elevation myocardial infarction; stent for life;
Portuguese registry; Primary angioplasty; stemI .
IntroductIon
Geoffrey Hartzler was the pioneer of primary angioplasty (P-PCI) when he treated the first patient with acute ST-segment elevation myocardial infarction (STEMI) in 1981. It would be about a decade before Cindy Grines and Bill O’Neill demonstrated that P-PCI was superior to fibrinolysis and would take nearly two decades until the guidelines considered P-PCI as a class I indication for the treatment of STEMI.
Since the beginning of fibrinolysis studies it is widely known that the time from the onset symptoms to reperfusion was decisive for the success of the therapy. Also in P-PCI, the total ischemia time span has an impact on the results. Since this technique is much more demanding both from the logistic point of view and the availability of trained teams, the time factor plays a fundamental role in the results. Despite the scientific evidence of the benefits of reperfusion in STEMI, a significant proportion of patients worldwide still remain out of revascularization. Even in the Western more developed countries, many patients do not have access to P-PCI. In Europe there is an important heterogeneity in the practice of P-PCI, with high performance levels in the north and suboptimal levels in the south. The “Stent for Life Initiative” (SFL) was created in this context to reduce the differences among the various countries through measures to increase patient access to P-PCI. Identical initiatives were developed in the United States of America.
Although in Portugal there is an interventional cardiology network that covers almost the whole country, and a good network of roads which allow a reasonable access (less than two hours) to P-PCI, in the middle of the last decade, it was one of the European countries with one of the lowest P-PCI rates. It was also observed that in Portugal only a small percentage of STEMI patients asked for help through 112. Most of them travelled to secondary hospitals, without primary angioplasty, therefore requiring secondary transportation, with a meaningful impact on treatment delay. Given the strong prognostic implications of total ischemia time (between the onset of symptoms and the time of reperfusion therapy), it is important not only to monitor all these timings, but also to identify where the main barriers to a good system performance are and to plan actions in order to improve quality indicators of the P-PCI in Portugal. The rapid technical progress in the areas of medical devices and pharmacology, along with the strong growth in the number of procedures, increased the need for recording data from the real world. The implementation in 2002 of the registries of the Portuguese
Society of Cardiology (PSC), allowed a wide scrutiny of interventional cardiology practice and the management of acute coronary syndromes. The continuous recording of interventions, and the benchmark between national and international centres, are fundamental tools for the knowledge of the current situation of interventional cardiology and for the decision making. No less important is the scientific potential which the Portuguese Society of Cardiology registries program really represent.
objectIves
The main objectives were:
1. To evaluate the trends of P-PCI overtime in Portugal together with evaluation of performance indicators.
2. To identify quality indicators of P-PCI in Portugal, particularly the conundrum of delay in P-PCI access, in both the patient and the system delay components.
Methods
1. A retrospective study based on the data of questionnaires distributed to Portuguese interventional cardiology centres (1992-2003) was performed in order to assess the earlier trends of PCI in Portugal.
2. The period of 2002/2003 was a landmark in the Portuguese interventional cardiology due to the beginning of the National Registries of the Portuguese Society of Cardiology. Retrospective evaluations of prospectively collected data from the National Registry of Interventional Cardiology (ClinicaTrials.gov identifier NCT01867801) and from the National Registry of Acute Coronary Syndromes (ClinicaTrials.gov identifier NCT01642329) from 2002 to 2013 were performed in order to assess the evolution of PCI in Portugal and particularly P-PCI. These data were complemented with official data from the General Directorate of Health for the years under review. 3. In-hospital mortality as a surrogate of quality indicators among centres. The presence
(or absence) of cardiac surgery was also compared.
4. In order to assess the patient and system delay components, a prospective cross-sectional study (Momentos) was carried out during one month per year (2011-2014),
in all interventional cardiology centres in Mainland Portugal and integrated in the “Via Verde Coronaria”. Data of 994 patients suspected of having STEMI with less than 12 hours of evolution and proposed to P-PCI, who were admitted to 18 Portuguese centres of interventional cardiology were collected for a one-month period, every year from 2011 to 2014.
Patient delay was defined as the time from symptom onset to first medical contact (FMC). It was considered a continuous variable and was expressed in minutes.
System delay was defined as the time from first contact with the health care system to the initiation of reperfusion therapy. This variable was analysed as continuous or categorical variable (cut-off value 90 minutes). “Door-to-Balloon time” (D2B) was defined as the time from entrance at the P-PCI centre to the moment of reperfusion and was evaluated as well as continuous or categorical variable (cut-off value of 60 min).
Following the “Momento Zero” study (2011) a public awareness campaign for the
symptoms of heart attack and to how to call for help in order to improve the patient delay (“Act Now – Save a Life”, from the SFL initiative). Educational programs were implemented for professionals aimed at improving the performance on Acute Coronary Syndromes management and treatment.
Univariate analysis and logistic regression models of multivariate analysis were used to determine the predictors of “patient delay” and “system delay” overtime. Exponential beta coefficients (exp (beta)), and 95% confidence intervals (CIs) were reported for continuous variables. Odds Ratio (OR) and 95% confidence intervals (CIs) were reported for categorical variables. The analysis was conducted at a 5% level of significance.
results
1. From 1992 to 2001 the evaluation questionnaires distributed in Portuguese interven-tional cardiology centres showed an increase of 1,193% in coronary interventions in comparison to 1992, with a total of 8,465 procedures and a rate of coronary inter-ventions of 848 per million population in 2003. During this period, this PCI rate per million population in Portugal was lower than the mean European rate (848 vs. 1194). 2. According to the prospective and multicenter evaluation of the RNCI and the official
representing an increase of 315% compared to 2002. In 2002, P-PCI represented 16% of the total number of PCI, and in the years 2012-2013 they represented 25%. Between 2002 and 2013 the number of procedures per million inhabitants increased from 106 to 338 and rescue angioplasty decreased from 71%, in 2002, to 16%, in 2006, and to 2%, in 2013. During the study period, the use of drug eluting stents increased from 10% to 70%. After 2008, there was an increased use of aspiration thrombectomy, reaching 47% in 2013. The use of glycoproteins IIb / IIIa inhibitors decreased from 73% in 2002 to 24% in 2013. The radial access increased from 8% in 2008 to 55% in 2013.
3. Between 2002 and 2006, hospital mortality from coronary angioplasty in hospitals without cardiac surgery compared to hospitals with surgery 0.3% in both cases among patients with chronic angina; 1.5% and 1.0% (ns) respectively in patients with acute coronary syndromes; 4.0% and 5.0% (ns) in patients with acute ST-segment elevation myocardial infarction and no cardiogenic shock; 50.9% and 53.4% (ns) in patients with cardiogenic shock.
4. In the study “Momentos”, conducted monthly between 2011 and 2014, there were no significant differences in patient delay (114 min in 2011 and 119 min in 2015). The multivariable analysis identified five predictors of patient delay: age $ 75 (Exp(beta) 1.28; CI95% 1.10-1.50; p=0.001), onset symptoms during the night (Exp(beta) 1.26; CI95% 1.10-1.45; p=0.001), and primary healthcare unit before first medical contact (Exp(beta) 1.75; CI95% 1.41-2.16; p<0.001) were indicators of longer time and call 112-EMS (Exp(beta) 0.84; CI95% 0.71-1.00; p=0.045) and transportation by National Institute of Medical Emergency (INEM) to the P-PCI facility (Exp(beta) 0.71; CI95% 0.59-0.84; p<0.001) were indicators of a shorter patient delay.
There were also no significant changes in the “system delay” (115 min in 2011 and 127 min in 2014) and D2B (54 min in 2011 and 64 min in 2014) during the study period. Only 27% of patients had a system delay # 90 min. The system delay of less than 90 min was achieved in only 13% of patients undergoing secondary transportation versus 33% of cases where no transfer was required. The multivariate analysis identified four predictors of “system delay”: age $ 75 years (OR 2.57, CI 95% 1.50-4.59, p = 0.001), attendance a unit without P-PCI (OR 4.08; CI 95% to 2.75-6.10, p <0.001), call 112 (OR 0.47, CI95% 0.32-0.68, p <0.001) and “Centro” region (OR 3.43, CI 95% 1.60-8.31, p = 0.003).
conclusIons
The registries of Portuguese Society of Cardiology (PSC) allow a better knowledge of the activity of Portuguese cardiology in general and primary angioplasty in particular. The data collected allowed us to characterize the Portuguese intervention practice in Portugal and to plan a strategy to improve the performance. It was possible to verify that the practice of elective and primary coronary angioplasty performed in hospitals without on-site surgery is a safe practice, with results similar to those obtained in hospitals with surgery. The implementation of centres in peripheral regions, without cardiac surgery, allowed the P-PCI to be a reality in practically the entire national territory.
Although at the beginning of this millennium both the Portuguese distribution of P-PCI centres and the road network were satisfactory, Portugal was one of the European countries with lower P-PCI implementation, which led PSC to join the SFL initiative. Despite the weak initial implementation, between 2002 and 2013 the rate of coronary angioplasty per million people increased by a factor of 3. Rescue angioplasty was overcome by primary angioplasty in 2006. New trends in the treatment of acute myocardial infarction with ST-segment elevation were observed, with the use of drug eluting stents and radial access, with rates similar to the European average.
Despite a public awareness campaign for the symptoms of myocardial infarction and the need for calling the emergency number 112 in such circumstances (“Act Now – Save a Life” SFL initiative), in the four years the patient’s delay was not significantly reduced. Given the difficulty in achieving significant progress in reducing time to first medical contact through classic campaigns, it is important to analyse which factors are strongly associated with longer delays and to try to build campaigns and actions that are more focused on these more difficult populations. In our study, it was observed that the elderly and the onset of symptoms during the night period was associated with an increase in “patient delay”. Inversely, asking for help through 112 and being transported by national Institute for medical emergencies (Inem) was associated with a shorter time.
The “Door-to-Balloon” time (D2B) represents only a small part of the total ischemic time. In Portugal the D2B is within the values recommended by the guidelines but unfortunately most patients did not have access to an earlier reperfusion, mainly as a
result of the need for secondary transportation (about half of them entered hospitals without interventional cardiology). There were also no significant changes in the “system delay” during the study period. A higher percentage of patients achieved a system delay of less than 90 min when no secondary transportation was required. Four predictors of system delay were identified: age greater than 75 years, attending hospitals without P-PCI, no call to 112, and living in the “Centro region”.
Ideally, patients should be treated with P-PCI but it will be mandatory to evaluate and monitor system delays in order for patients to have access to the best therapy that in each case requires and to see if P-PCI is used in a timely manner (where it may clearly be superior to fibrinolysis). The data collected throughout the SFL initiative was associated with the implementation of a number of specific educational programs for patients and professionals aimed at improving system-wide performance.
Introdução
Geoffrey Hartzler foi pioneiro na angioplastia primária (P-PCI) quando tratou o primeiro paciente com enfarte agudo do miocárdio com elevação do segmento ST (STEMI) em 1981. Passaria cerca de uma década antes de Cindy Grines e Bill O’Neill demonstras-sem que a P-PCI era Superior à fibrinólise e levaria quase duas décadas até que as
guidelines considerassem a P-PCI como uma indicação de classe I para o tratamento
de STEMI.
Desde o início dos estudos de fibrinólise, que se verificou que o tempo desde o início dos sintomas até o momento da reperfusão era decisivo para o sucesso da terapêutica. Também na P-PCI, o tempo de isquemia total tem um impacto nos resultados. Uma vez que esta técnica é muito mais exigente tanto do ponto de vista logístico como da disponibilidade de equipes treinadas, o fator tempo desempenha um papel fundamental nos resultados. Apesar da evidência científica dos benefícios da reperfusão no STEMI, uma proporção significativa de doentes, em todo o mundo, ainda não é revascularizada. Mesmo em países ocidentais e mais desenvolvidos, muitos doentes não têm acesso à P-PCI. Na Europa existe uma importante heterogeneidade na prática da P-PCI, com níveis de desempenho elevado nos países do norte e sub-óptimo nos do sul. Foi neste contexto que a Iniciativa “Stent for Life” (SFL) foi criada para reduzir as diferenças entre países, através de medidas que se propõem aumentar o acesso dos doentes à P-PCI. Iniciativas idênticas também se desenvolveram nos Estados Unidos da América.
Embora Portugal seja um país com uma rede de cardiologia de intervenção que abrange praticamente todo o país, dispor de uma boa rede de estradas que permite um razoável acesso (menos de duas horas) à angioplastia primária, em meados da última década, era um dos países europeus com uma das mais baixas taxas de P-PCI. Também se observou que apenas uma pequena percentagem de doentes com STEMI pedia ajuda por meio do 112 e que a maioria deles se deslocava para hospitais secundários sem angioplastia primária com necessidade de transporte secundário, com um impacto significativo no atraso do tratamento.
Dado o tempo total de isquemia (entre o início dos sintomas e o momento da terapia de reperfusão) poder ter fortes implicações prognósticas, é importante não apenas monitorizar todos esses tempos, mas também identificar quais os principais obstáculos ao bom desempenho do sistema de forma a planear ações que permitam melhorar os indicadores de qualidade da P-PCI em Portugal.
O rápido progresso técnico nas áreas de dispositivos médicos e na farmacologia, juntamente com o forte crescimento do número de procedimentos, aumentou a necessidade de registar os dados da atividade. A implementação, em 2002, dos registos da Sociedade Portuguesa de Cardiologia (PSC) permitiu um amplo escrutínio da prática da cardiologia de intervenção e da gestão das síndromes coronárias agudas. O registo contínuo das intervenções, com benchmark entre os centros nacionais e internacionais, são ferramentas fundamentais para o conhecimento da atividade de cardiologia de intervenção e para a tomada de decisões com base no mundo real. Não menos importante é o potencial científico que os registos da PSC representam.
objetIvos
Os objectivo principais foram o seguintes:
1. Avaliar a evolução da intervenção coronária na P-PCI em Portugal, bem como os indicadores de desempenho.
2. Identificar os indicadores de qualidade da P-PCI em Portugal, particularmente no atraso ao acesso, tanto nos componentes de atraso do doente como do sistema.
Métodos
1. Realizou-se um estudo retrospectivo com base nos dados dos questionários distribuídos aos centros de cardiologia de intervenção portugueses (1992-2003) para avaliar a evolução de angioplastia em Portugal durante este período.
2. O período 2002/2003 foi um marco na cardiologia intervencionista portuguesa devido ao início dos Registos Nacionais da Sociedade Portuguesa de Cardiologia. Foram realizadas avaliações retrospectivas de dados prospectivamente coletados do Registro Nacional de Cardiologia de Intervenção (ClinicaTrials.gov NCT01867801) e do Registro Nacional de Síndromes Coronárias Agudas (ClinicaTrials.gov NCT01642329) de 2002 a 2013, a fim de avaliar a evolução da PCI Portugal em geral e da P-PCI em particular. Esses dados foram complementados com dados oficiais da Direção-Geral de Saúde para os anos em análise.
3. Comparou-se também a mortalidade intra-hospitalar como indicador de avaliação comparativa de qualidade entre centros com e sem cirurgia cardíaca.
4. Para avaliar os componentes do atraso do doente e do sistema, foi realizado um estudo transversal prospectivo (Momentos) durante um mês por ano (2011-2015), em todos os centros de cardiologia de intervenção do Continente e integrados na Via Verde Coronária. Os dados de 994 doentes com suspeita de STEMI com menos de 12 horas de evolução e propostos para P-PCI, admitidos em 18 centros portugueses de cardiologia de intervenção, foram coletados por um período de um mês por ano, de 2011 a 2015.
O atraso do doente foi definido como o tempo desde o início dos sintomas até o primeiro contacto médico (FMC). Foi considerada uma variável contínua e foi expressa em minutos.
O atraso do sistema foi definido como o tempo desde o primeiro contato com o sistema de saúde até o início da terapêutica de reperfusão. Esta variável foi analisada como variável contínua ou categórica (valor de corte de 90 minutos). O tempo “Porta--Balão” (D2B) foi definido como o tempo desde a entrada no centro P-PCI até o momento da reperfusão e foi avaliado como variável contínua ou categórica (valor de corte de 60 min).
Após o Momento Zero (2011), deu-se início a uma campanha de sensibilização pública para os sintomas de enfarte do miocárdio e como pedir ajuda com o objectivo de melhorar o atraso do doente (“Não Perca Tempo – salve uma Vida”, da iniciativa SFL). Foram também implementados programas educativos para profissionais com o objetivo de melhorar o desempenho na gestão e tratamento das Síndromes Coronárias Agudas. A análise univariada e modelos de regressão logística de análise multivariada foram utilizados para determinar os preditores de “atraso do doente” e “atraso do sistema”. Os coeficientes beta exponenciais (exp (beta)) e os intervalos de confiança (IC) de 95% foram relatados para variáveis contínuas. Razão de Odds (OR) e intervalos de confiança de 95% (ICs) foram relatados para variáveis categóricas. A análise foi realizada com um nível de significância de 5%.
resultados
1. De 1992 a 2001, os questionários de avaliação distribuídos nos centros de cardiologia intervencionista portuguesa mostraram um aumento de 1.193% nas intervenções coronárias em relação a 1992, com um total de 8.465 procedimentos
e uma taxa de intervenções coronárias de 848 por milhão de habitantes em 2003. Em Portugal, nesse ano, a taxa de PCI por milhão de habitantes foi inferior à taxa média europeia (848 vs. 1194).
2. De acordo com a avaliação prospectiva e multicêntrica do RNCI e os dados oficiais da Direcção-Geral da Saúde, em 2013, foram realizadas 3.524 angioplastias primárias, representando um aumento de 315% em relação a 2002. Em 2002, a P-PCI representou 16% do número total de PCI, representando 25% nos anos 2012-2013. Entre 2002 e 2013, o número de procedimentos por milhão de habitantes aumentou de 106 para 338 e a angioplastia de recurso diminuiu de 71% em 2002 para 16% em 2006 e 2% em 2013. Durante o período em estudo, o uso de stents farmacoactivos aumentou de 10% para 70%. Após 2008, houve um aumento do uso da trombectomia por aspiração, atingindo 47% em 2013. Os inibidores das glicoproteínas IIb/IIIa diminuíram a utilização de 73% em 2002 para 24% em 2013. O acesso radial aumentou de 8% em 2008 para 55% em 2013.
3. Entre 2002 e 2006, a mortalidade hospitalar por angioplastia coronária em hospitais sem cirurgia cardíaca, em comparação com hospitais com cirurgia, não foi significati-vamente diferente com taxa de mortalidade de 0,3% em ambos os anos nos doentes com angina crónica; 1,5% e 1,0% (ns) nas síndromes coronárias agudas; 4,0% e 5,0% (ns) em doentes com STEMI e sem choque cardiogénico; 50,9% e 53,4% (ns) no choque cardiogénico, respectivamente nos centros sem e com cirurgia.
4. No estudo “Momentos”, realizado mensalmente entre 2011 e 2015, não houve diferenças significativas no atraso do doente (114 min em 2011 e 119 min em 2015). A análise multivariada identificou cinco preditores de atraso do doente: idade $75 (Exp (beta) 1,28, IC 95% 1,10-1,50; p = 0,001), início dos sintomas durante a noite (Exp (beta) 1,26; CI 95% 1,10-1,45; p = 0,001) e recorrer a um centro de saúde antes do primeiro contato médico (Exp (beta) 1,75, IC 95% 1,41-2,16, p <0,001) foram indicadores de maior tempo e ligar para o 112 (Exp (beta) 0,84; IC 95% 0,71-1,00; p = 0,045) e transporte pelo Instituto Nacional de Emergência Médica (INEM) para o centro de P-PCI (Exp (beta) 0,71; IC 95% 0,59-0,84, p <0,001) com menor atraso do doente.
Também não houve alterações significativas no “atraso do sistema” (115 min em 2011 e 127 min em 2015) e D2B (54 min em 2011 e 64 min em 2015) durante o período do estudo. Apenas 27% dos doentes tiveram um atraso do sistema #90
min. O atraso do sistema de menos de 90 minutos foi atingido em apenas 13% dos doentes submetidos a transporte secundário versus 33% dos casos em que não foi necessária transferência. A análise multivariada identificou quatro preditores de “atraso do sistema”: idade $ 75 anos (OR 2,57, IC 95% 1,50-4,59, p = 0,001), atendimento numa unidade sem P-PCI (OR 4,08; IC 95% a 2,75-6,10, P <0,001), não pedir ajuda através do 112 (OR 0,47, CI 95% 0,32-0,68, p <0,001) e procedência da região Centro (OR 3,43, CI 95% 1,60-8,31, p = 0,003).
conclusões
Os registos da PSC permitem um melhor conhecimento da atividade da cardiologia portuguesa em geral e da angioplastia primária em particular. Os dados recolhidos permitiram enquadrar a intervenção portuguesa e planear uma estratégia para melhorar o desempenho da P-PCI. Foi possível verificar que a prática de angioplastia coronária eletiva e primária realizada em hospitais sem cirurgia é uma prática segura, com resultados semelhantes aos obtidos em hospitais com cirurgia. A implantação de centros em regiões mais periféricas, sem cirurgia cardíaca, permitiu que a P-PCI fosse uma realidade em praticamente todo o território nacional.
Embora no início deste milénio a distribuição portuguesa dos centros P-PCI e a rede rodoviária fossem satisfatórias, Portugal era um dos países europeus com a menor implementação de P-PCI, o que levou a PSC a associar-se à iniciativa SFL. Não obstante esse números inicias, entre 2002 e 2013 a taxa de angioplastia coronária por milhão de habitantes triplicou. A angioplastia de recurso foi superada pela angioplastia primária em 2006. Observaram-se novas tendências no tratamento do STEMI, com a generalização do uso de stents farmacoactivos e o acesso radial, com taxas semelhantes à média europeia.
Apesar de uma campanha de sensibilização pública para os sintomas de enfarte do miocárdio e a necessidade de pedir ajuda através do número de emergência 112 em tais circunstâncias (“Não Perca Tempo – Salve uma Vida”, iniciativa SFL), o atraso do doentes não se reduziu significativamente ao longo dos quatro anos de campanha. Dada a dificuldade de alcançar progressos significativos na redução do tempo até ao primeiro contato médico através de campanhas clássicas, é importante analisar quais os fatores que estão mais fortemente associados com este atraso e tentar construir
campanhas e ações focadas nessas populações mais difíceis. No nosso estudo, observou-se que os idosos e quando o início dos sintomas decorria durante o período noturno, estiveram associados a um aumento no “atraso do doente”. Inversamente, a solicitação de ajuda por meio do 112 e o transporte pelo Instituto Nacional de Emergência Médica (INEM) estiveram associados a um tempo menor.
O tempo “Porta-Balão” (D2B) representa apenas uma pequena parte do tempo total de isquemia. Em Portugal, o D2B está dentro dos valores recomendados pelas guidelines, mas a maioria dos doentes entrou no sistema muito mais cedo, principalmente devido ao facto de cerca de metade deles ter recorrido a hospitais sem cardiologia de intervenção e necessitando de transporte secundário. Também não houve mudanças significativas no “atraso do sistema” durante o período em estudo. Uma maior percentagem de doentes atingiu um atraso do sistema inferior a 90 minutos quando não foi necessário um transporte secundário. Foram identificados quatro preditores de atraso do sistema: idade superior a 75 anos, entrada inicial num hospital sem P-PCI, não ligar para o 112 e procedência da região Centro.
Idealmente, os doentes devem ser tratados por P-PCI, mas será necessário avaliar e monitorar os tempos do sistema para que os dentes obtenham o melhor benefício da terapia mais apropriada em cada caso e para ver se a P-PCI não está a ser realizada para além da barreira temporal em que demonstrou ser superior à fibrinólise. Os dados coletados ao longo da iniciativa SFL possibilitaram a implementação de um conjunto de programas educacionais específicos para doentes e profissionais com o objetivo de melhorar o desempenho de todo o sistema.
1.1 IntroductIon
Geoffrey Hartzler was one of the pioneers of interventional cardiology and presented the first results of his research in animals, at Miami in 1976, and at the same event he met Andreas Gruentzig. Hartzler made his training at Mayo Clinic and, in this institution, he performed his first coronary angioplasty. However, in 1980, he moved to St. Luke’s Hospital Mid America Institute, in Kansas City, where he found a less conservative environment which allowed him to continue the development of coronary angioplasty. There he became a pioneer of primary angioplasty (P-PCI) when, in 1981, he treated the first patient with acute myocardial infarction with ST segment elevation (STEMI). The patient previously presented a focal lesion of the right coronary artery detected by diagnostic cardiac catheterization, and already in the ward, suffered an acute myocardial infarction. Hartlzer took him to the hemodynamics room and, with a balloon angioplasty, he managed to successfully reopen the occluded right coronary. In 1984, he published a series on the first 43 patients treated.1,2 In Europe, Felix Zijlstra,
having moved to Zwolle after his graduation in Rotterdam, had an important role in the implementation and promotion of primary angioplasty.
Nevertheless in spite of the signs of success, it would take almost two decades until the American guidelines to consider P-PCI as class I treatment for STEMI.3
In Portugal, the first coronary angioplasty was performed by Ricardo Seabra Gomes at Santa Cruz Hospital,4 after being with Andreas Gruentzig at Emory, in the University
School of Medicine, Atlanta, where he also met Bernhard Meir. With the unconditional support of the cardiothoracic surgery director, Machado Macedo, managed to gather the conditions for starting with the cardiology coronary intervention. Using a grant awarded by the Calouste Gulbenkian Foundation, he managed to acquire balloons to treat the first patient in May 31, 1984, with the surgery backup support by Queirós e Melo. Vasco da Gama Ribeiro - who just arrived from Rotterdam - witnessed this event. The second Hospital to perform a coronary angioplasty was S. João (1987), followed by the Hospitals of the University of Coimbra (1988) and Santa Marta (1988). The first primary angioplasty in Portugal was performed by Seabra Gomes in April 16, 1987.5,6
It has been a long road, in order to reach P-PCI. The American doctor, James Herrick, who lived between the American Civil War and World War Two, made a famous presentation in the Association of American Physicians in May 4, 1912.7 He considered
the hypotheses that the acute necrosis observed in the left ventricle, revealed in autopsies of patients who died of myocardial infarction, could be caused by coronary thrombosis. He also considered that the thrombosis was not always fatal. This presentation wasn´t well accepted by his peers, and in the following decades this subject continued to be controversial. Many physicians considered that thrombosis was the consequence and not the cause of myocardial infarction. Previously, in 1880, a German pathologist, Carl Weigert, had proposed coronary occlusion as the ethology of myocardial infarction,8
but was Herrick who persisted with it, not only with clinical bases but also supported in animal experimentation. Herrick’s publication is considered today a “landmark article”.9
It was also Herrick who began to use ECGs, invented by Einthoven in 1902, which remain until today the gold standard to STEMI diagnosis.10 Up to the beginning of the
1960s, in the absence of the perfect knowledge of myocardial infarction pathogenesis, the treatment consisted on prolonged rest in bed, oxygen therapy, fluid therapy and morphine.
It was during early 60s of the twentieth century, which Desmond Julian, from the United Kingdom, who promoted the first major step forward in STEMI mortality reduction, by creating the coronary units. These allowed the monitoring and treatment of life-threatening arrhythmias, reducing mortality in the early hours from 30 to 15%.11
In 1980, DeWood presented a series of 322 patients, where he showed that patients had a high rate of occlusion of the artery involved in the myocardial infarction, especially when the coronary angiography was performed earlier (87% of the occlusions in the first 24 hours). This article, published in 1980, was another important “landmark”, because it not only proved that the coronary occlusion occurs especially in the early hours, but also reported that it is possible to perform coronary angiography in patients with acute myocardial infarction - something that was once considered a contraindication.12
Streptokinase was isolated in 1933 by Tillet and Garner,13 however, only the discovery of
coronary angiography in late sixties and the following use of this procedure in STEMI12
proved the presence of thrombosis in the arteries responsible for the heart attack. It was the Russian Evgeny Chazov, doctor of the elites of the former Soviet Union and later Nobel laureate, which showed that the coronary infusion of streptokinase had dissolved a thrombus in a coronary artery.14 Probably because the article was
published in a Russian magazine, it did not have the necessary disclosure. The same didn´t happened with Peter Rentrop15 when he published a series of five cases, followed
by a European study with a random design, which showed a significantly reduction in mortality within 6 months (15.5% in the intracoronary streptokinase group vs 30.6% in the control group; p<0.01).16
However, the intracoronary administration of a fibrinolytic was a major logistical hurdle. The real beginning of the fibrinolysis era came with a publication of the GISSI study in 1986,17 confirmed by the ISIS-2.18 These two studies showed a relative mortality
reduction between 19 and 25% with the use of intravenous fibrinolysis. ISIS-2 also showed the importance of aspirin in the reduction of STEMI related mortality.
Fibrinolysis had been a breakthrough in STEMI treatment, not only for the mortality reduction, but for the ease logistics of intravenous administration. However, its use was related to higher risks of haemorrhagic stroke, particularly in the elderly. Besides it was contraindicated in some situations: uncontrolled blood pressure, previous surgery, recent trauma, haemorrhagic disease and previous stroke. Re-occlusions and failure rates were also important.19,20
Given the limitations of fibrinolysis, in which 15% of the cases the vessel remains occluded,21,22 and the fact that new occlusions occur in 25% of the patients after 3
months,23 it made perfect sense to perform angioplasty after fibrinolysis, not only to
treat the residual stenosis, but also to improve the TIMI grade flow (in cases where this has not yet happened). However, three randomised controlled trials carried out in this context, reported that this strategy was not advantageous, and it was abandoned.24-26
These results were later explained by an inadequate adjuvant antithrombotic therapy. As mentioned previously, despite Hartzler having performed the first P-PCI in 1981, it took about a decade until Cindy Grines and Bill O’Neill finally proved the superiority of P-PCI over fibrinolysis.27 The study PAMI27 randomised 395 patients for P-PCI vs
fibrinolysis. There was a significant reduction in the primary end-point of in-hospital death and myocardial re-infarction (5.1% vs 12.0%; p=0.02) in the P-PCI group, a trend towards mortality reduction (2.6% vs 6.5%; p=0.06) and a reduction in intracranial haemorrhage (0% vs 2.0%; p=0.05). Finally, a meta-analysis performed by Keeley and published in 2003, with 23 randomised controlled trials included, which compared P-PCI vs fibrinolysis, came to prove the reduction in early mortality (7 vs 9%; p=0.02), non-fatal myocardial re-infarction (3 vs 7%; p<0.001) and stroke (1 vs 2%; p=0.004).28
It’s been known, from the first fibrinolysis studies, that the time from onset symptoms until the administration of the drug, was crucial to the success of the therapy. Reimer studies with experimental models showed a phenomenon called “wave-front”, which correlates the myocyte mortality and ischemic time.29,30 Fifty percent of the myocytes
died in the first 90 minutes from the coronary occlusion, followed by a less pronounced reduction in the hours following coronary occlusion. These observations led to the “golden hour” concept: if we reopen the artery in the first hour, we can recover a high percentage of the myocardium at risk. These experimental studies agree with clinical results. Both random clinical studies31 and registries,32 showed that the delay from
onset symptoms to fibrinolysis was associated with increased mortality. These data led to creation of the concept “door to needle”: timeframe between first medical contact and fibrinolytic administration. The guidelines pointed out that “door to needle” must be less than 30 minutes.33
Even with its documented superiority, P-PCI is much more demanding, concerning both on logistic level and on the availability of well-trained teams. In P-PCI, as in fibrinolysis, the time factor is crucial in the success of the therapy. The study GUSTO IIb reported that the mortality at 30 days was 1% when P-PCI was performed in the first hour and 6.4% when performed after 90 minutes.34,35 This led to the concept “door-to-balloon”
(D2B), that evaluate the elapsed time between the entry of the patient in the hospital until the time when the injury is crossed with the medical device, which in this case is the “balloon”.
It is not well established yet, what the temporal distance from which the performance of P-PCI loses its benefit to fibrinolysis.36-38 A meta-analysis indicates that this temporal
distance is about 110 minutes.39 Randomised controlled trials show that the patients’
transference to a cardiology centre, if carried out in a time frame window of 2 hours, is superior to the strategy of performing fibrinolysis in place.40 When is no impossible
to provide P-PCI in a timely manner, fibrinolysis still maintains an important role in reperfusion of STEMI. In such cases, it is necessary to follow a pharmaco-invasive strategy.41-43 Although in an ideal situation most of the patients should be treated with
P-PCI, it is mandatory to assess and monitor the system times, by allowing the patients to receive the best benefit of the therapy, which should be adequate to each case, and to understand if P-PCI is being performed beyond the time barrier in which is clearly superior to fibrinolysis.
It is important to notice that P-PCI proved to be superior to fibrinolysis when performed in high-volume centres and with experienced operators. If performed in low-volume centres, with inexperienced operators, with long delays, the results are inferior.44
Despite all the scientific evidence of the benefits of reperfusion in STEMI, an important proportion of patients worldwide remain out of revascularization. Even in the western and most developed countries, many patients don’t have access to P-PCI. In Europe, there is an important heterogeneity in the practice of P-PCI, with high performance levels in the North and suboptimum levels in the South.45 It was in this context that the
Initiative “Stent for Life (SFL) was created, to reduce the differences between various countries, through measures to increase the access of patients to P-PCI.46-47 Similar
initiatives were also developed in the United States of America.48-49
Despite Portugal being a country with an intervention Cardiology network that covers virtually the entire territory, and with a good network of roads and motorways, allowing the access in a reasonable time (less than 2 hours) to primary angioplasty, it was, in the middle of the last decade, one of the countries with the lowest rates of P-PCI.45 At
the same time, it was observed that only a small percentage of patients with STEMI asked for help through the 112 and that most of them went by their own means to secondary hospitals without primary angioplasty requiring secondary transportation, with an important impact on the treatment delay.45
The total ischaemic time (from onset symptoms to reperfusion) has implications on the prognosis.50-53 For this reason, it’s important not only to monitor all these time delays,
but also to find the major obstacles to a good system performance and to plan actions to improve all the quality parameters of P-PCI in Portugal.
1.2 General study objectIve
Using information from the National Registry of Interventional Cardiology and from the National Registry of Acute Coronary Syndromes, from the Portuguese Society of Cardiology, to characterise the evolution of the coronary angioplasty in Portugal and to identify the main barriers to access to interventional cardiology, on a timely basis, in order to contribute to an improvement in the performance of primary angioplasty.
1.3 specIfIc objectIves
To monitor the performance and quality indicators of primary angioplasty in Portugal, both in quantitative terms (number of primary angioplasty per year per million inhabitants) and in qualitative terms (the various components of the patient and system delays). To identify the main predictors of “patient delay” in the access to primary angioplasty, in order to develop specific action programmes, in particular to raise the awareness of the Portuguese population to the acute coronary syndromes.
To identify the major predictors of the system delay, in the access to primary angioplasty, to design specific action programmes, with focus on the pre-hospital and hospital emergency service, as well as all stakeholders involved in the system.
To characterise the regional performance of primary angioplasty, to plan specific actions for each region, as well as exerting influence in strategic decision-making for these regions with a view to combat the iniquity.
To meet general and specific objectives, data of this research were collected from the National Registry of Cardiology (RNCI) and the National Registry of Acute Coronary Syndromes (RNSCA), scientific property of the Portuguese Society of Cardiology. This information was supplemented by a cross-sectional study carried out during one month per year, in all centres of interventional cardiology in Portugal mainland, and integrated into the “Via Verde Coronária” (Coronary Green Way fast track). These surveys obtained express consent from the Coordinator of the National Data Collection Centre in Cardiology. The collection of information for the CNCDC is authorized by the National Data Protection Commission and the ethics committees from the respective hospitals.
1.4 Methods
1. A retrospective study based on the data of questionnaires distributed to Portuguese interventional cardiology centres (1992-2003) was performed in order to assess the earlier trends of PCI in Portugal.
2. The period of 2002/2003 was a landmark in the Portuguese interventional cardiology due to the beginning of the National Registries of the Portuguese Society of Cardiology. Retrospective evaluations of prospectively collected data from the National Registry
of Interventional Cardiology (ClinicaTrials.gov identifier NCT01867801) and from the National Registry of Acute Coronary Syndromes ClinicaTrials.gov identifier NCT01642329) from 2002 to 2013 were performed in order to assess the evolution of PCI in Portugal and particularly P-PCI. These data were complemented with official data from the General Directorate of Health for the years under review. 3. In-hospital mortality, as a surrogate of quality indicators between centres with and
without cardiac surgery, was also compared.
4. In order to assess the patient and system delay components, a prospective cross-sectional study (Momentos) was carried out for one month per year (2011-2015), in all interventional cardiology centres in Mainland Portugal and integrated in the Via Verde Coronaria. Data of 994 patients suspected of having STEMI with less than 12 hours of evolution and proposed to primary percutaneous coronary intervention, who were admitted to 18 Portuguese centres of interventional cardiology were collected for a one-month period, every year from 2011 to 2015.
Patient delay was defined as the time from symptom onset to first medical contact (FMC). It was considered a continuous variable and was expressed in minutes.
System delay was defined as the time from first contact with the health care system to the initiation of reperfusion therapy. This variable was analysed as continuous or categorical variable (cut-off value 90 minutes). “Door-to-balloon time” (D2B) was defined as the time from entrance at the P-PCI centre to the moment of reperfusion and was evaluated as well as continuous or categorical variable (cut-off value of 60 min). Following the Momento Zero study (2011) a public awareness campaign for the symptoms of heart attack and for how to call for help in order to improve the patient delay (Act Now – Save a Life, from the SFL initiative). Educational programs were implemented for professionals aimed to improve the performance on Acute Coronary Syndromes management and treatment.
Univariate analysis and logistic regression models of multivariate analysis were used to determine the predictors of “patient delay” and “system delay” overtime. Exponential beta coefficients (exp(beta)), and 95% confidence intervals (CIs) were reported for continuous variables. Odds Ratio (OR) and 95% confidence intervals (CIs) were reported for categorical variables. The analysis was conducted at a 5% level of significance.
references
11. Hartzler GO, Rutherford BD, McConahay DR, et al. Percutaneous transluminal coronary angioplasty with and without thrombolytic therapy for treatment of acute myocardial infarction. Am Heart J 1983;106:965–73.
12. Hartzler GO, Rutherford BD, McConahay DR. Percutaneous transluminal coronary angioplasty: application for acute myocardial infarction. Am J Cardiol. 1984;53:117C–21.
13. Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC Jr. ACC/ AHA guidelines for the management of patients with ST-elevation myocardial infarction: executive summary: a report of the ACC/AHA Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines on the Management of Patients With Acute Myocardial Infarction). Circulation. 2004;110: 588 – 636.
14. Seabra-Gomes R, Silva A, Aleixo A et al. Angioplastia coronária. Experiência inicial do Hospital de Santa Cruz. Rev Port Cardiol 1985;4:309-311.
15. Seabra-Gomes R. Cardiologia de Intervenção no Enfarte Agudo do Miocárdio. Rev Port Cardiol 1990;9:315-358.
16. Seabra-Gomes Ricardo. Vinte anos de Angioplastias Coronárias no Hospital de Santa Cruz (1984-2004). Ideias Lounge.Com impresso na Krispress; 2005 ISBN: 972-9060-53-3.
17. Herrick JB: certain clinical features of sudden obstruction of the coronary arteries. Trans Assoc Am Phys 1912;27:100.
18. Weigart C. Ueber die pathologiische Gerinnugs-Vorgange. Arch Path Anat (Virchow). 1880;79:87–123.
19. Herrick JB. Landmark article (JAMA). Clinical features of sudden obstruction of the coronary arteries. JAMA. 1983;250:1757–65.
10. Braunwald E. Evolution of management of acute myocardial infarction: 20th century saga. Lancet 1998;352:1771-4.
11. Julian DG. Treatment of cardiac arrest in acute myocardial ischaemia and infarction. Lancet. 1961;2:840–4.
12. DeWood MA, Spores J, Notske R, et al. Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction. N Engl J Med. 1980;303:897–902.
13. Tillett WS, Garner RL. The fibrinolytic activity of hemolytic streptococci. J Exp Medi. 1933; 58: 485–502.
14. Chazov EI, Matveeva LS, Mazaev AV, et al. Intracoronary administration of fibrinolysin in acute myocardial infarct. Ter Arkh. 1976;48:8.
15. Rentrop KP, Blanke H, Karsch KR, et al. Acute myocardial infarction: intracoronary application of nitroglycerin and streptokinase. Clin Cardiol. 1979;2:354–63.
16. Streptokinase in acute myocardial infarction. European Cooperative Study Group for Streptokinase Treatment in Acute Myocardial Infarction. N Engl J Med 1979, 301:797–802.
17. Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Gruppo Italiano per lo Studio della Streptochinasi nell’Infarto Miocardico (GISSI). Lancet 1986, 1:397–402.
18. Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Lancet 1988, 2:349–360.
19. An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. The GUSTO investiga- tors. N Engl J Med 1993, 329:673–682.
20. Ohman EM, Califf RM, Topol EJ, et al. Consequences of reocclusion after successful reperfusion therapy in acute myocardi- al infarction. TAMI Study Group. Circulation. 1990;82:781–91.
21. The GUSTO Angiographic Investiga- tors. The effects of tissue plasminogen activator, streptokinase, or both on coronary-artery patency, ventricular function, and survival after acute myocardial infarction. N Engl J Med 1993;329:1615-22. [Erratum, N Engl J Med 1994;330:516.]
22. Anderson JL, Karagounis LA, Becker LC, Sorensen SG, Menlove RL. TIMI perfusion grade 3 but not grade 2 results in improved outcome after thrombolysis for myocardial infarction: ventriculographic, enzymatic, and electrocardiographic evidence from the TEAM-3 Study. Circulation 1993; 87:1829-39. 23. Gibson CM, Karha J, Murphy SA, et al. Early and long-term clinical outcomes associated with
reinfarction following fibrinolytic administration in the Thrombolysis in Myocardial Infarction trials. J Am Coll Cardiol 2003;42:7-16.
24. Simoons ML, Arnold AE, Betriu A, et al. Thrombolysis with tissue plasminogen activator in acute myocardial infarction: no additional benefit from immediate percutaneous coronary angioplasty. Lancet. 1988;1:197–203.
25. Immediate vs delayed catheterization and angioplasty following thrombolytic therapy for acute myocardial infarction. TIMI II A results. The TIMI Research Group. JAMA 1988, 260:2849–2858. 26. Topol EJ, Califf RM, George BS, et al. A randomized trial of immediate versus delayed elective
angioplasty after intravenous tissue plasminogen activator in acute myocardial infarction. N Engl J Med. 1987;317:581–8.
27. Grines CL, Browne KF, Marco J, et al. A comparison of immediate angioplasty with thrombolytic therapy for acute myocardial infarc- tion. The Primary Angioplasty in Myocardial Infarction Study Group. N Engl J Med. 1993;328:673–9.
28. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13– 20. 29. Reimer KA, Lowe JE, Rasmussen MM, Jennings RB. The wavefront phenomenon of ischemic cell
death. 1. Myocardial infarct size vs duration of coronary occlusion in dogs. Circulation. 1977; 56: 786–94.
30. Reimer KA, Vander Heide RS, Richard VJ. Reperfusion in acute myocardial infarction: effect of timing and modulating factors in experimental models. Am J Cardiol. 1993;72:13G–21.
31. Boersma E, Maas AC, Deckers JW, Simoons ML. Early thrombolytic treatment in acute myocardial infarction: reappraisal of the golden hour. Lancet. 1996;348:771–5.
32. Goldberg RJ, Mooradd M, Gurwitz JH, et al. Impact of time to treatment with tissue plasminogen activator on morbidity and mortality following acute myocardial infarction (The second National Registry of Myocardial Infarction). Am J Cardiol. 1998;82:259–64.
33. Steg PG, James SK, Atar D, Badano LP, Blomstrom-Lundqvist C, Borger MA, Di Mario C, Dickstein K, Ducrocq G, Fernandez-Aviles F, Gershlick AH, Giannuzzi P, Halvorsen S, Huber K, Juni P, Kastrati A, Knuuti J, Lenzen MJ, Mahaffey KW, Valgimigli M, van ’t Hof A, Widimsky P, Zahger D. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2012;33(20):2569–2619.
34. A clinical trial comparing primary coronary angioplasty with tissue plasminogen activator for acute myocardial infarction. The Global Use of Strategies to Open Occluded Coronary Arteries in Acute Coronary Syndromes (GUSTO IIb) Angioplasty Substudy Investigators. N Engl J Med 1997, 336:1621–1628.
35. Berger PB, Ellis SG, Holmes Jr DR, et al. Relationship between delay in performing direct coronary angioplasty and early clinical outcome in patients with acute myocardial infarction: results from the global use of strategies to open occluded arteries in Acute Coronary Syndromes (GUSTO-IIb) trial. Circulation. 1999;100: 14–20.
36. Boersma E; Primary Coronary Angioplasty vs. Thrombolysis Group. Does time matter? a pooled analysis of randomized clinical trials comparing primary percutaneous coronary intervention and in-hospital fibrinolysis in acute myocardial infarction patients. Eur Heart J. 2006;27(7):779-788. 37. Terkelsen CJ, Christiansen EH, Sørensen JT, et al. Primary PCI as the preferred reperfusion therapy
in STEMI: it is a matter of time. Heart. 2009;95(5): 362-369.
38. Pinto D, Kirtane A, Nallamothu B et al. Hospital Delays in Reperfusion for ST Elevation Myocardial Infarction: Implications When Selecting a Reperfusion Strategy. Circulation. 2006;114:2019-25. 39. Betriu A, Masotti M. Comparison of mortality rates in acute myocardial infarction treated by
percutaneous coronary intervention versus fibrinolysis. Am J Cardiol. 2005;95:100–101.
40. Dalby M, Bouzamondo A, Lechat P, Montalescot G. Transfer for primary angioplasty versus immediate thrombolysis in acute myocardial infarction: a meta-analysis. Circulation. 2003;108:1809-14. 41. Armstrong PW; WEST Steering Committee. A comparison of pharmacologic therapy with/without
timely coronary intervention vs. primary percutaneous intervention early after ST-elevation myocardial infarction: the WEST (Which Early ST-elevation myocardial infarction Therapy) study. Eur Heart J. 2006;27:1530-8.
42. Bonnefoy E, Steg PG, Boutitie F, Dubien PY, Lapostolle F, Roncalli J, Dissait F, Vanzetto G, Leizorowicz A, Kirkorian G; CAPTIM Investigators, Mercier C, McFadden EP, Touboul P. Comparison of primary angioplasty and pre-hospital fibrinolysis in acute myocardial infarction (CAPTIM) trial: a 5-year follow-up. Eur Heart J. 2009;30:1598-606.
43. Armstrong PW, Gershlick AH, Goldstein P, Wilcox R, Danays T, Lambert Y, Sulimov V, Rosell Ortiz F, Ostojic M, Welsh RC, Carvalho AC, Nanas J, Arntz HR, Halvorsen S, Huber K, Grajek S, Fresco C, Bluhmki E, Regelin A, Vandenberghe K, Bogaerts K, Van de Werf F; STREAM Investigative Team. Fibrinolysis or primary PCI in ST-segment elevation myocardialinfarction. N Engl J Med. 2013;368:1379-87.
44. Nallamothu BK, Wang Y, Magid DJ, et al. Relation between hospital specialization with primary percutaneous coronary intervention and clinical outcomes in ST-segment elevation myocardial infarction: National Registry of Myocardial Infarction- 4 analysis. Circulation 2006;113:222-9.
45. Widimsky P, Wijns W, Fajadet J, et al. Reperfusion therapy for ST elevation acute myocardial infarction in Europe: description of the current situation in 30 countries. Eur Heart J. 2010;31:943-57. 46. Widimsky P, Fajadet J, Danchin N, et al. ‘‘Stent 4 Life’’ targeting PCI at all who will benefit the most. A
joint project between EAPCI, Euro-PCR, EUCOMED and the ESC Working Group on Acute Cardiac Care. EuroIntervention. 2009;4:555-7.
47. Widimsky P, Wijns W, Kaifoszova Z. Stent for Life: how this initiative began? EuroIntervention. 2012;8:P8-10.
48. Jacobs AK, Antman EM, Faxon DP, Gregory T, Solis P. Development of systems of care for ST-elevation myocardial infarction patients: executive summary. Circulation 2007; 116:217-30. [Erratum, Circulation 2007;116(2): e77.]
49. Bradley EH, Nallamothu BK, Herrin J, Ting HH, Stern AF, Nembhard IM, et al. National efforts to improve door-to-balloon time results from the door-to balloon alliance. J Am Coll Cardiol 2009;54:2423–9.
50. De Luca G, Suryapranata H, Zijlstra F,et al. Symptom-onset-to-balloon time and mortality in patients with acute myocardial infarction treated by primary angioplasty. J Am Coll Cardiol 2003;42:991-7. 51. De Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time delay to treatment and mortality
in primary angioplasty for acute myocardial infarction every minute of delay counts. Circulation. 2004;109:1223–1225.
52. Nallamothu BK, Bradley EH, Krumholz HM. Time to treatment in primary percutaneous coronary intervention. N Engl J Med 2007; 357: 1631–38
2.1 the 2002 portuGuese InterventIonal cardIoloGy reGIstry
Rev Port Cardiol 2004; 23 (1): 7-14
Hélder Pereira on behalf of researchers from Registo Nacional de Cardiologia de Intervenção
abstract
The 2002 Portuguese Interventional Cardiology Registry
The Portuguese Interventional Cardiology Registry was created by the Portuguese Society of Cardiology with the aim of documenting prospectively and continually the characteristics of the patients and procedures carried out in Portugal.
We studied 5250 patients, from 19 centers, with a mean age of 63±11 years, 76% male. Twenty-five per cent of the patients had a previous history of acute myocardial infarction, 16.4% of percutaneous angioplasty and 6.7% of coronary artery bypass graft. The procedure was performed for acute myocardial infarction in 18.2%. In total 7685 lesions were treated and 52% of the patients had single-vessel disease. The intervention was multi-vessel in 16%. Stents were implanted in 85.5%, of which 45.1% were direct stenting. In 23% of cases drug-eluting stents were used. Glycoprotein inhibitors were used in 50%. Vascular access was femoral in 98.3%, of which 37% used closure devices. Hospitalization without complications in 90%, with better outcomes in men (90.5% male vs. 86.8% female). Total mortality was 2.2%.
KEy woRDs
Portuguese registry; Interventional cardiology; PTCA.
IntroductIon
The Portuguese Interventional Cardiology Registry was created by the Portuguese Society of Cardiology with the aim of documenting on a prospective and continuous basis the characteristics of the patients and procedures carried out in Portugal.
This article presents the results of the Registry for the period January 1 to December 31 of 2002. The registry is observational and continuous, and is coordinated by the Working Group on Hemodynamics and Interventional Cardiology and the National Cardiology Data Collection Center (CNCDC) of the Portuguese Society of Cardiology.