w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Depressive
and
anxiety
symptoms
and
social
support
are
independently
associated
with
disease-specific
quality
of
life
in
Colombian
patients
with
rheumatoid
arthritis
Heather
L.
Rogers
a,∗,
Hardin
T.
Brotherton
a,
Silvia
Leonor
Olivera
Plaza
b,
María
Angélica
Segura
Durán
b,
Marvín
Leonel
Pe ˜na
Altamar
caDepartmentofMethodsandExperimentalPsychology,UniversityofDeusto,Bilbao,Spain
bGrupodeInvestigaciónCarlosFinlay,FacultaddeSalud,UniversidadSurcolombiana,Neiva,Colombia cClínicaSaludcoopNeiva,Neiva,Colombia
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13February2014 Accepted11January2015 Availableonline13July2015
Keywords:
Rheumatoidarthritis Qualityoflife Depression Anxiety Socialsupport
a
b
s
t
r
a
c
t
Objective:Toexaminetherelationshipbetweendisease-specificqualityoflife(QOL)and socio-demographic,medical,andpsychosocialfactorsinColombianpatientswith Rheuma-toidArthritis(RA).
Methods:One hundred and three RA patients recruited from ambulatory centers in Neiva,ColombiawereadministeredtheDiseaseActivityScale28(DAS-28),QOL-RA,Zung Self-RatingDepressionScale,State-TraitAnxietyInventory(STAI),InterpersonalSupport EvaluationList-12(ISEL-12),andSymptomChecklist-90Revised(SCL-90R).
Results:LowerQOL-RAwasassociatedwithlowersocio-economicstatus(r=0.26,p<0.01), higherlikelihoodofusingopioids(t=−2.51,p<0.05), higherlikelihoodofcomorbid pul-monarydisease(t=−2.22,p<0.05),andlowerISEL-12sub-scales(r’s=0.41–0.31,p’s<0.001). Lower QOL-RA was associated with higher DAS-28 (r=−0.28, p<0.01), Visual Analog Scale(VAS;r=−0.35,p<0.001),ZungDepression(r=−0.72,p<0.001),STAI-State(r=−0.66,
p<0.001),STAI-Trait(r=−0.70,p<0.001),SCL-90RGlobalSeverityIndex(r=−0.50,p<0.001), SCL-90RPositiveSymptomTotal(r=−0.57,p<0.001),andallSCL-90Rsub-scales(r’s=−0.54to −0.21,p’s<0.01).AmultivariatelinearregressionmodelindicatedthatSES(B=2.77,p<0.05), ZungDepression(B=−0.53,p<0.001),STAI-State(B=−0.26,p<0.05),andISEL-12Belonging (B=1.15,p<0.01)wereindependentlyassociatedwithQOL-RA,controllingforsignificant associations.
Conclusions:Moredepressiveandanxietysymptomswereindependentlyassociatedwith lower disease-specific QOL, while higherperceptions ofhaving people to doactivities with(belongingsocialsupport)andhigherSESwereindependentlyassociatedwithhigher
∗ Correspondingauthor.
E-mail:[email protected](H.L.Rogers). http://dx.doi.org/10.1016/j.rbre.2015.01.005
disease-specificqualityoflife.PsychosocialfactorsimpactQOLinRAaboveandbeyond diseaseactivity.Additionalresearchintothebenefitsofpsychosocial assessmentofRA patientsandprovisionofcomprehensivecaretoimproveQOLiswarranted.
©2015ElsevierEditoraLtda.Allrightsreserved.
Sintomas
depressivos
e
de
ansiedade
e
apoio
social
estão
associados
de
modo
independente
à
qualidade
de
vida
específica
da
doenc¸a
em
pacientes
colombianos
com
artrite
reumatoide
Palavras-chave: Artritereumatoide Qualidadedevida Depressão Ansiedade Apoiosocial
r
e
s
u
m
o
Objetivo: Analisararelac¸ãoentreaqualidadedevida(QV)específicadadoenc¸aefatores sociodemográficos,clínicosepsicossociaisempacientescolombianoscomartrite reuma-toide(AR).
Métodos: Recrutaram-se103pacientescomARem centrosambulatoriais deNeiva, na Colômbia. Eles responderam ao Disease ActivityScale28 (DAS-28),QOL-RA, Escala de Autoavaliac¸ãodaDepressãodeZung,InventáriodeAnsiedadeTrac¸o-Estado(Idate), Inter-personalSupportEvaluationList-12(Isel-12)eSymptomChecklist-90Revised(SCL-90R). Resultados: Escoresmaisbaixosde QOL-RAestiveram associadosa umapiorcondic¸ão socioeconômica (CSE; r=0,26, p<0,01), maiorprobabilidade de usar opioides (t=−2,51, p<0,05), maior probabilidade de doenc¸a pulmonar comórbida (t=−2,22, p<0,05) e pontuac¸õesinferioresnassubescalasdoISEL-12(r’s=0,41–0,31,p’s<0,001).Uma menor pontuac¸ão no QOL-RA esteveassociadaa escoresmais elevados no DAS-28(r=−0,28, p<0,01), Escala Analógica Visual (EVA; r=−0,35, p<0,001),Escala de Autoavaliac¸ãoda Depressão de Zung (r=−0,72, p<0,001), Idate-Estado (r=−0,66, p<0,001), Idate-Trac¸o (r=−0,70,p<0,001),SCL-90RÍndicedeGravidadeGlobal(r=−0,50,p<0,001),SCL-90RTotal de SintomasPositivos (r=−0,57,p<0,001)etodas assubescalas doSCL-90R(r’s=−0,54 a−0,21,p’s<0,01). UmmodeloderegressãolinearmúltiplaindicouqueaCSE(B=2,77, p<0,05),aEscaladeAutoavaliac¸ãodaDepressãodeZung(B=−0,53,p<0,001),oIdate-Estado (B=−0,26,p<0,05)eoIsel-12Pertencimento(B=1,15,p<0,01)estavamindependentemente associadosàpontuac¸ãonoQOL-RA,mesmoquandocontroladosporassociac¸ões significa-tivas.
Conclusões: Maissintomasdepressivosedeansiedadeestiveramindependentemente asso-ciadosaumamenorQVespecíficadadoenc¸a,enquantoapercepc¸ãoaumentadadeter pessoas comquemfazeratividades(pertencimento,apoio social)e CSEmaiselevados estiveramindependentementeassociadosaumamaiorQVespecíficadadoenc¸a.Osfatores psicossociaisimpactamnaQVnaARacimaealémdaatividadedadoenc¸a.Énecessária pesquisaadicionalacercadosbenefíciosdaavaliac¸ãopsicossocialdopacientecomAReda prestac¸ãodecuidadosabrangentesparamelhoraraQV.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
RAisa debilitatingautoimmune disease whosesymptoms cause increased difficulty in carrying out normal, every-dayactivities. RAhasa worldwideprevalenceof0.5–1% of thepopulation, affectingwomenmorethan menataratio of 3:1 and increasing with age.1 The prevalence of RA in
LatinAmerica isestimated at0.4%,2 while inColombia, it
may be evenlower, at0.1%.3 Thepublic health burden of
the disease is quite high.Approximately 10 years ago, RA was the second cause of loss ofworking years in women between ages 15 and 44 in Colombia.4 Subjective patient
and physician measures are important predictors of RA treatment response and future health outcomes,5 making
accurate measurementsindomainsofquality oflife,pain, andpsychologicalfactorsvaluableforaccurateandimproved prognoses.
Qualityoflife(QOL)inindividualswithRAispoorerthan healthy controls.Comparedtothosewithout arthritis, peo-ple with RA were 40% more likely to report fair or poor generalhealth,30%morelikelytoneedhelpwithpersonal care, and twice as likely to have a health-related activity limitation.6 General measures of QOL, such as the Health
Assessment Questionnaire Disability Index (HAQ) and the Short-Form36(SF-36),aswellasdisease-specificmeasures, suchastheRAQOLandtheQOL-RA,allindicatepoorerQOL thancontrols.7–11
Depressive symptoms and depression have been associ-atedwithworseQOLinpatientswithRAincross-sectional studies12–15andfoundtobeanindependentpredictorofQOL
attwo-year follow-up.16 Anxietyhasalsobeenfoundtobe
associatedwithpoorerQOL.12,13,17RApatientswitha
comor-bidpsychiatricdisorderhadlowerQOL,18andsomatization,
inparticular, was found tobe associatedwith worseQOL, independentofanxietyanddepression.14Positivesocial
sup-port hasbeen associatedwith betterQOL inpatients with RAin somecross-sectional studies,19 whereas problematic
socialinteractions,criticism,and/oralackofsocialsupportis associatedwithpoorerQOL.20,21Highersatisfactionwith
emo-tionalsupportindependentlypredictedimprovedQOLinRA patients,22thoughthisbufferingeffectappearedtodecrease
overtime.23
Muchofthepriorresearchhasfocusedonsamplesfrom Anglo-Saxon cultures and the importance of psychosocial factors(includingdepressivesymptoms,anxiety,other psy-chopathology,andsocialsupport)onQOLinLatinAmericans with RA has been less studied.24 The aim of the present
studyistodeterminethepsychosocialfactorsassociatedwith disease-specificQOL inasampleofpatients withRAfrom Colombia and examine their independent contributions to QOLinRA.Afocusontheroleofsocialsupportina Colom-biansamplewithRAisnovel,anditishypothesizedthatsocial support, in particular, may influence QOL differently than inpriorresearchinprimarilyAnglo-Saxonculturesbecause LatinAmericanvaluestendtoalign withcollectivistideals andfamililism.25
Patients
and
methods
Participants
The sample consisted of 103 individuals diagnosed with Rheumatoid Arthritis (RA) according to the American Col-legeofRheumatology/EuropeanLeagueAgainstRheumatism (ACR/EULAR)CollaborativeInitiative2010Rheumatoid Arthri-tis ClassificationCriteria.26 All patients aged18 to 79 who
visited ambulatory centers in Neiva, Colombia between December2012andJune2013tobeevaluatedbya rheumatolo-gistorinternalmedicinespecialistandwerecognitivelyableto participateinthestudywereincluded.Anypatientcurrently hospitalized,withacomorbidneurologicalorpsychiatric dis-order interfering with independent decision making, with terminalillness(definedbyasurvivaltimeoflessthan six months),orwithahistoryofalcoholorotherdrugabusewas excludedfromthisstudy.
Procedure
Patients were assessed by a rheumatologist or internal medicine specialist to determine eligibility. After sign-ing an informed consent, the Disease Activity Scale-28 (DAS28)27 was administered, followed by a session with a
trained research assistant to complete demographic and psychologicalscales. Thisstudy received ethics committee approval.
Measures
DiseaseActivityScale-28(DAS28)
TheDiseaseActivityScale-28(DAS28)isacompositemeasure thatconsistsofphysical,emotional,andserological evalua-tion.Measurementsinthisstudyincluded:(a)a28tenderjoint countanda28swollenjointcount,(b)theerythrocyte sedi-mentationrate(ESR)asameasureofinflammation,and(c)a VisualAnalogScale(VAS)ratingofdiseaseactivityoverthe priorweekfrom0(notatallactive)to10(extremelyactive). A total score is calculated, with higher scores represent-inggreaterextentofdiseaseactivity.27Thefollowingcut-off
pointshavebeenestablished:lessthan2.6indicatesdisease remission,2.6–3.2indicateslowdiseaseactivity,3.2–5.1 indi-catesmoderatediseaseactivity,andgreaterthan5.1indicates high disease activity. TheDAS28 is highly correlated with theoriginalDAS(r>0.94)andwell-correlatedwithdisability asmeasuredbytheHealthAssessmentQuestionnaire(HAQ; r=0.49)andtheShortForm-36(SF-36;r=−0.46).28
QualityOfLife-RheumatoidArthritis(QOL-RA)
TheQualityofLife-RheumatoidArthritis(QOL-RA)isan eight-itemself-reportquestionnairethatevaluatesphysicalability, interaction, pain, tension, overall health, arthritis-specific QOL,socialsupport,andmoodonaLikertscalefrom1(very poor)to10(excellent).29 Highertotalscoresindicatehigher
disease-specificQOL.TheSpanishversionoftheQOL-RAis commonlyusedinColombiaandhasgoodreliability,witha Cronbach’salphaof0.89,veryclosetotheEnglishversionof 0.90.29
State-TraitAnxietyInventory(STAI)
The State-Trait Anxiety Inventory (STAI) measures Trait Anxiety(STAI-Trait),orstableanxiety,andStateAnxiety (STAI-State),ormomentaryanxiety.Eachsub-scaleconsistsof20 symptomsevaluatedona4-pointLikertscalefrom1(notat all or almost never) to 4(verymuchso or almost always). Someitemsreflectabsenceofanxietyandarereversecoded inscoring.Highertotalscoresoneachsub-scalereflectgreater anxiety.30TheSpanishmeasurehasgoodtoexcellent
reliabil-ity(STAI-Traitalpha=0.86,STAI-Statealpha=0.91).31
InterpersonalSupportEvaluationList(ISEL-12)
TheInterpersonalSupportEvaluationList(ISEL-12)isa short-ened version of a 40 item scale.32 The ISEL-12 assesses
ZungSelf-RatingDepressionScale
TheZungSelf-RatingDepressionScalewasdesignedto eval-uate the level of depression in patients diagnosed with a depressivedisorder.34 TheZungconsistsof20 items
repre-sentingtheaffective,psychological,andsomaticsymptoms ofdepression. Thereare10positively wordeditemsand10 negatively wordeditems assessedon a scale of 1(little of thetime)to4(mostofthetime).34TheZunghasbeen
vali-datedinColombiawithgoodreliability(alpha=0.85).35Inthe
presentstudy,thetotalscoreontheZungwasusedto repre-sentdepressivesymptomsonacontinuum.
SymptomChecklist-90-Revised(SCL-90R)
The Symptom Checklist-90-R (SCL-90R) evaluates a broad rangeofpsychologicalproblemsandpsychopathology.36The
scaleconsistsof90symptomsassessedonafive-point Lik-ert scale from 0 (not present or bothersome) to 4 (very presentorbothersome).Theitemsaregroupedintothe fol-lowingninedimensions:somatization,obsessive–compulsive, interpersonalsensitivity,depression,anxiety,hostility, pho-bicanxiety,paranoid ideation,and psychoticism.Thescale includesa Global Severity Index (GSI) to indicate the gen-eral level of distress caused by the symptoms, a Positive Symptom Distress Index (PSDI) to measure the intensity of symptoms experienced, and a Positive Symptom Total (PST)toreporttheself-reportedtotalnumberof90possible symptoms assessed.36 Higher scores indicate more
symp-tomsand/ormoredistress.TheSCL-90Rhasbeenvalidated in Colombia with good reliability across various samples (alpha’s=0.77–0.90).37
Statisticalanalyses
Thedatawereanalyzedusing IBMSPSS Statisticsfor Win-dows,Version20.0(IBMCorporation,2011).Frequenciesand descriptivestatisticswere calculatedforsocio-demographic and medical characteristics. Pearson correlations and t -testswereconductedtoexaminethebivariaterelationships between socio-demographics, medical characteristics, and psychosocialfactorsandQOL-RA.Amultivariatelinear regres-sion analysiswas conductedon QOL-RA using the factors foundtobesignificantinbivariateanalysesaspredictors.
Results
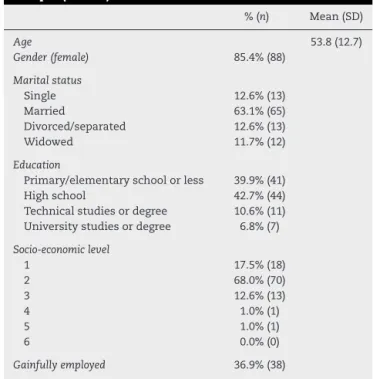
Table1describesthesocio-demographiccharacteristicsofthe sample(n=103),whichprimarilyconsistedofmarried(63.1%, n=65)women(85.4%,n=88)withanaverageageof54years. Eighty-fivepercent ofthe sample represented the bottom-mostsocio-economiclevelsinthecountry(levels1–2),with 36.9%gainfullyemployed.Table2describesthemedical char-acteristicsofthesample.Approximately85%ofthesample had moderate to high disease activity28 and had been
liv-ingwiththediseaseforanaverageof13years.Theaverage RApatient took three medications, with the majority tak-ingnon-steroidal anti-inflammatorydrugs(NSAIDS)(91.3%, n=94), disease modifying anti-rheumatic drugs (DMARDS) (77.7%,n=80),andsteroids(76.7%,n=79).Onepersonwason anti-depressantmedication,andanotheronanticonvulsant
Table1–Socio-demographiccharacteristicsofthe sample(n=103).
%(n) Mean(SD)
Age 53.8(12.7)
Gender(female) 85.4%(88)
Maritalstatus
Single 12.6%(13)
Married 63.1%(65)
Divorced/separated 12.6%(13)
Widowed 11.7%(12)
Education
Primary/elementaryschoolorless 39.9%(41)
Highschool 42.7%(44)
Technicalstudiesordegree 10.6%(11) Universitystudiesordegree 6.8%(7)
Socio-economiclevel
1 17.5%(18)
2 68.0%(70)
3 12.6%(13)
4 1.0%(1)
5 1.0%(1)
6 0.0%(0)
Gainfullyemployed 36.9%(38)
medication.Approximately half (n=52) hada co-morbidity, mostcommonlyhypertension(28.2%,n=29).
Participants reported average levels of disease-specific QOL [mean QOL-RA=50.50(12.10) with a maximum of 80 points total]. They alsoreported average depressive symp-tom and anxietyscores [meanZung=44.14(7.40)out of80,
Table2–Medicalcharacteristicsofthesample.
%(n) Mean(SD)
DiseaseActivityScale28(DAS28) 4.87(1.46) Severe(>5.1) 45.6%(47)
Moderate(3.2–5.1) 38.8%(40)
Low(2.6–3.2) 8.7%(9)
Remission(<2.6) 6.8%(7)
VisualAnalogScale(VAS)forDAS28 6.29(2.68)
Numberofyearswithdisease 12.97(11.63) EarlyRheumatoidArthritis(≤3
years)
20.4%(21)
Totalmedications,mean(SD) 3.03(0.88) Non-Steroidal
Anti-InflammatoryDrugs
91.3%(94)
DiseaseModifying Anti-RheumaticDrugs
77.7%(80)
Steroids 76.7%(79)
None 49.5%(51)
BiologicTherapy 44.7%(46)
Other 5.8%(6)
Opioids 4.9%(5)
Totalcomorbidities,mean(SD) 0.84(1.02)
Hypertension 28.2%(29)
Other 21.4%(22)
Cardiacdisease 14.6%(15)
Diabetes 8.7%(9)
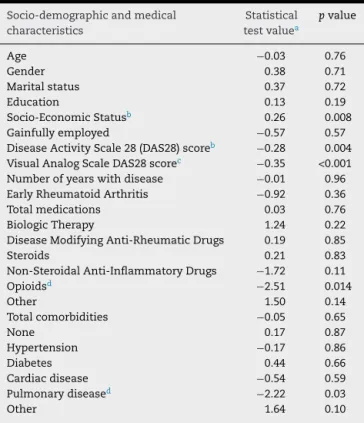
Table3–Bivariaterelationshipsbetween
socio-demographicandmedicalcharacteristicsand QOL-RA.
Socio-demographicandmedical characteristics
Statistical testvaluea
pvalue
Age −0.03 0.76
Gender 0.38 0.71
Maritalstatus 0.37 0.72
Education 0.13 0.19
Socio-EconomicStatusb 0.26 0.008
Gainfullyemployed −0.57 0.57
DiseaseActivityScale28(DAS28)scoreb −0.28 0.004
VisualAnalogScaleDAS28scorec −0.35 <0.001
Numberofyearswithdisease −0.01 0.96 EarlyRheumatoidArthritis −0.92 0.36
Totalmedications 0.03 0.76
BiologicTherapy 1.24 0.22
DiseaseModifyingAnti-RheumaticDrugs 0.19 0.85
Steroids 0.21 0.83
Non-SteroidalAnti-InflammatoryDrugs −1.72 0.11
Opioidsd −2.51 0.014
Other 1.50 0.14
Totalcomorbidities −0.05 0.65
None 0.17 0.87
Hypertension −0.17 0.86
Diabetes 0.44 0.66
Cardiacdisease −0.54 0.59
Pulmonarydiseased −2.22 0.03
Other 1.64 0.10
a Iftheindependentvariablewascontinuous,rvalueofa
Pear-soncorrelationwasprovided.Iftheindependentvariablewas categorical,tvalueoftheindependentttestwasprovided. b p<0.01.
c p<0.001.
dp<0.05.
STAI-State=35.26(10.21)outof80,andSTAI-Trait=38.39(9.72) out of 80]. Social support was high, with ISEL totals of 41.66(6.08) out of 48. Patients endorsed an average of 23.13(14.75)ofthe 90symptomson theSCL-90R(PST) with average severities [1.51(0.44), range 0–4; PSDI], and overall severitiesforthe90itemsof0.42(0.35)ona0–4scale(GSI).
Table3showsthebivariaterelationshipsbetween socio-demographic and medical characteristics and QOL-RA. Althoughage,gender,maritalstatusandeducationwerenot significantlyassociatedwithQOL-RA,socio-economicstatus (SES)waspositively correlatedwithQOL-RAscores(r=0.26, p<0.01).DASandVASscoreswerenegativelyassociatedwith QOL-RA(r=−0.28,p<0.01andr=−0.35,p<0.001).Opioiduse andpresenceofpulmonarydiseasewere negatively associ-ated withQOL-RA (t=−2.51, p<0.05 and t=−2.22,p<0.05), but number of years with disease,total medications,total comorbidities,otherspecificmedicationuse,andother spe-cificcomorbiditieswerenotrelatedtoQOL-RAinthissample. Table 4 shows the bivariate relationships between psy-chosocialfactors and QOL-RA.AlthoughSCL-90R PSDIwas not correlated with QOL-RA, all other psychosocial meas-ures were significant. Zung Depression total, STAI-State, andSTAI-Traitweresignificantlynegativelyassociatedwith QOL-RA(r=−0.72,p<0.001; r=−0.66,p<0.001and r=−0.70,
p<0.001,respectively).TheISELtotalandeachthreesubscales ofappraisal, belonging, and tangible, were all significantly
Table4–Bivariaterelationshipsbetweenpsychosocial factorsandQOL-RA.
Psychosocialfactor Statistical testvaluea
pvalue
ZungDepressionb −0.72 <0.001
State-TraitAnxiety Inventory-Stateb
−0.66 <0.001
State-TraitAnxiety Inventory-Traitb
−0.70 <0.001
InterpersonalSupportEvaluation List(ISEL)totalb
0.42 <0.001
ISELAppraisalb 0.31 <0.001
ISELBelongingb 0.41 <0.001
ISELTangibleb 0.38 <0.001
SymptomChecklist-90-Revised (SCL-90R)GlobalSeverityIndexb
−0.50 <0.001
SCL-90RPositiveSymptomTotalb −0.57 <0.001
SCL-90RPositiveSymptom DistressIndex
−0.10 0.33
SCL-90RSomatizationb −0.45 <0.001
SCL-90RObsessive–Compulsiveb −0.36 <0.001
SCL-90RInterpersonalSensitivityb −0.33 <0.001
SCL-90RDepressionb −0.51 <0.001
SCL-90RAnxietyb −0.54 <0.001
SCL-90RHostilityb −0.37 <0.001
SCL-90RPhobicAnxietyb −0.42 <0.001
SCL-90RParanoidIdeationc −0.21 0.03
SCL-90RPsychoticismd −0.30 0.002
a Iftheindependentvariablewascontinuous,rvalueofa
Pear-soncorrelationwasprovided.Iftheindependentvariablewas categorical,tvalueoftheindependentttestwasprovided. b p<0.001.
c p<0.05.
d p<0.01.
positively correlated with an increase in QOL-RA (r=0.42, p<0.001;r=0.31,p<0.001;andr=0.41,p<0.001,respectively). SCL-90R GSI and PST were significantly negatively corre-latedwithQOL-RA(r=−0.50,p<0.001andr=−0.57,p<0.001, respectively).AllsubscalesoftheSCL-90Rweresignificantly negativelycorrelatedwithQOL-RA.
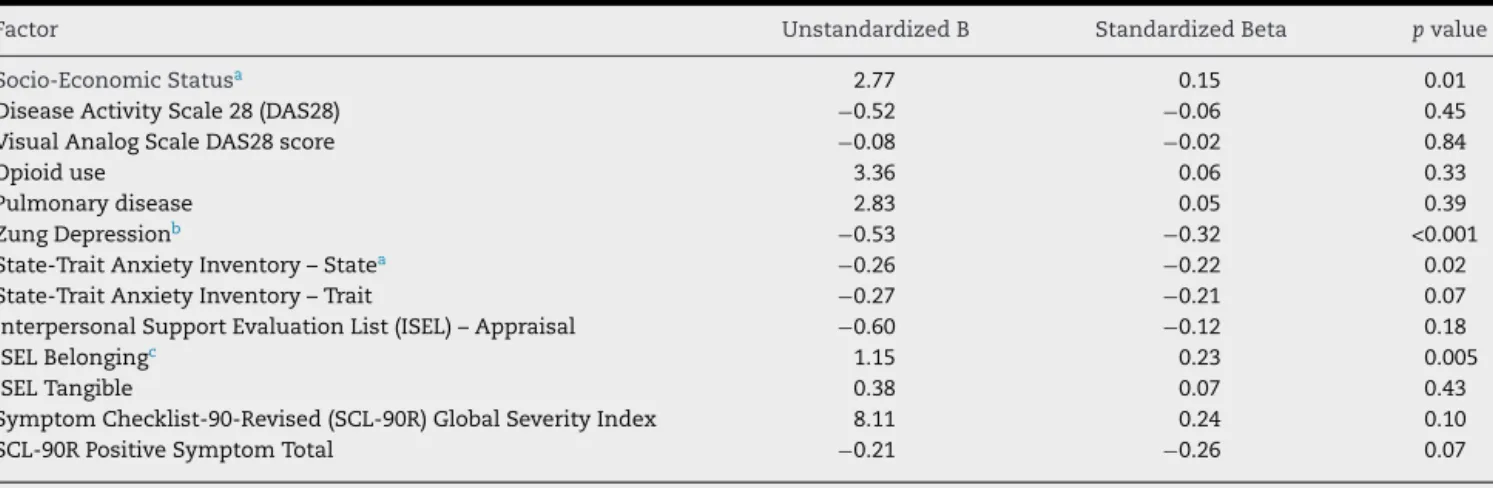
Theresultsofthemultivariatelinearregressionmodelare shown in Table 5. SES, Zung Depression, STAI-State Anxi-ety,andISELBelongingscoreswereindependentlyassociated with QOL-RA scores, controlling for DAS, VAS,opioid use, pulmonarydisease,STAI-TraitAnxiety, ISELAppraisal,ISEL Tangible,SCL-90RGSI,andSCL-90RPSTscores.HigherSESand ISELBelongingsub-scalescoreswereassociatedwithhigher QOL-RAscores(B=2.77,p<0.05andB=1.15,p<0.01, respec-tively),whilehigherZungDepressionandSTAI-StateAnxiety scoreswereassociatedwithlowerQOL-RAscores(B=−0.53,
p<0.001andB=−0.26,p<0.05,respectively).TheZung Depres-sion Scalescorewas thefactor mosthighly independently associatedwithQOL-RA(StandardizedBeta=−0.32).
Discussion
Table5–FactorsindependentlyassociatedwithQOL-RA.
Factor UnstandardizedB StandardizedBeta pvalue
Socio-EconomicStatusa 2.77 0.15 0.01
DiseaseActivityScale28(DAS28) −0.52 −0.06 0.45
VisualAnalogScaleDAS28score −0.08 −0.02 0.84
Opioiduse 3.36 0.06 0.33
Pulmonarydisease 2.83 0.05 0.39
ZungDepressionb −0.53 −0.32 <0.001
State-TraitAnxietyInventory–Statea −0.26 −0.22 0.02
State-TraitAnxietyInventory–Trait −0.27 −0.21 0.07
InterpersonalSupportEvaluationList(ISEL)–Appraisal −0.60 −0.12 0.18
ISELBelongingc 1.15 0.23 0.005
ISELTangible 0.38 0.07 0.43
SymptomChecklist-90-Revised(SCL-90R)GlobalSeverityIndex 8.11 0.24 0.10
SCL-90RPositiveSymptomTotal −0.21 −0.26 0.07
a p<0.05.
b p<0.001.
c p<0.01.
statuswere independentlyassociated withhigher disease-specificQOL.Depressivesymptoms,inparticular,weremost stronglyrelatedtoQOLinthisgroupofColombianRApatients. PsychosocialfactorsofRApatientsaffectwell-beingaboveand beyondtheinfluenceofdiseaseactivity.
These results are similar to prior research indicating anindependentrelationshipbetweendepressivesymptoms and decreased general physical or mental health QOL in individuals withRA.13–15 Thefindings ofthe present study
replicate those ofNas and colleagues, who found depres-siveandanxietysymptomsassociatedwithpoorerRA-specific QOL.12 Finally, Rupp and colleagues identified that
depres-sivesymptomspredictedmentalhealthQOLaftertakinginto accountdiseaseactivity,16 whilethepresent study extends
thisresearchtoindicatethatdepressiveandanxiety symp-toms are associated with disease-specific QOL (including physical,mental,andsocialimpacts)independentofdisease activity.Theclinicalimplicationssuggestpotentialvaluein screeningRA patientsfor emotionaldistress. For instance, theHamiltonAnxietyandDepressionScale(HADS)isa 14-iteminstrumentthatisconsideredtobethegoldstandardin rheumatoidpracticeandhasbeentranslatedandnormedfor useinColombia.38However,futureresearchshouldvalidate
theuseofthisscaleinColombianRApatients.
Socialsupport,and specifically the perceptionthat oth-ersareavailabletodothingswith(ISELbelongingsub-scale), wasfoundtoenhancedisease-specificQOLinRAaboveand beyondothersocio-demographic,medical,andpsychological factors.Priorresearchsuggeststhatsupportiverelationships are beneficial to individuals with RA,19 and that the
per-ception of adequate and positive social support enhances adherencetotreatmentregimens,rehabilitation,andoverall healthoutcomes,39whichmayexplainhigherQOL.Onestudy
foundthesocialdimensionofQOL-RAinColombiatobemuch highercomparedtotheUS.40 Itispossiblethat‘belonging’
socialsupport–havingsomeonetoparticipateinactivities likelunchoradaytrip–ismoreavailableand/orhighly val-uedinColombianculture,whichtendstobemorecollectivist thanindividualist.25Thefairlyconstantavailabilityof
com-panionshipinLatinoculturesmaymeanthattheimpactofa
lackofsocialsupportonQOLisfeltmuchmorethaninAnglo cultures.Inotherwords,themeasureof‘belonging’social sup-portmaybemoresensitiveinLatinAmerica.Futureresearch ontheroleofsocialsupportinthissocio-culturalcontextmay helptoelucidatethepositiveandnegativeimpactof compan-ionship,interaction,andassistanceinpatientsdealingwith RA,theresultingimpactonQOLandotherhealthoutcomes, andpossiblemechanismsofaction.
Thefindingsofthepresentstudyshouldbeinterpretedin lightofthefollowingcaveats.Thesamplewasfromarural towninColombiaandthefindingscanonlybegeneralizedto thisspecificgroup.However,thefactthatthesamplewasof lowSESmakesitrepresentativeofmuchofthegeneral popu-lationinLatinAmericaandisastrengthofthecurrentstudy. Becauseofthecross-sectionalnatureofthestudydesign,one cannotinferacause–effectrelationshipandfuture longitu-dinalstudiesare needed.Psychosocialfactorslikelyimpact QOL,butpoorQOLcanalsoincreasedepressivesymptomsand anxiety.TheZungDepressionScalewasselectedasa mea-sureofdepressionforthisstudybecauseithasbeenvalidated inColombia;however,itispossiblethattheirRAsymptoms mayhaveresultedinartificiallyhighdepressionscores.Itis ofnotethatanalyseswithasecond measureofdepression administeredinthisstudy[thePatientHealth Questionnaire-9(PHQ-9),arapidscreeningtoolevaluatingthefrequencyof nine keydepressive symptomsoverthe priortwoweeks]41
producedthe samemultivariatemodel,suggestingthatthe observedrelationshipisnotsimplyduetotheitemsaskedon theZungself-reportscale.
GiventheimportanceofpsychosocialfactorsonQOLinRA patientsacrossnumerousstudies(includingthisone), poten-tialinterventionstoimprovedepressivesymptoms,anxiety, andsocialsupportcouldbeconsidered.Cognitivebehavioral therapy(CBT),forinstance,hasbeenshowntosignificantly reducedepressivesymptomsandanxietycomparedtoroutine medicalmanagement inRA.42 Additionalresearchinto the
professionalsmaynotneedtoplayalargerolein psychoso-cialtreatmentstrategies.Forinstance,futureresearchcould examinetheimpactofprovidingopportunitiesforsocial inter-actionwithpeerswhosharesimilarsymptomsandconcerns, workingwithfamilymemberstoprovideadditionalsupport totheRApatient,and/orschedulinggroupactivitiesforthe socialnetwork.
Conclusion
This study is one of few examining associations between psychosocial factors and QOL among RApatients in Latin America. Depressive symptoms, anxiety, companionship / belongingsocialsupport,andSESwereallindependently asso-ciatedwithdisease-specificQOL,withdepressivesymptoms havingthe largest association.A Pan American Consensus Statementrecentlyconcludedthatthepsychosocial function-ingofRApatientsinLatinAmericanmustbeaddressed.2This
studyshowsthatemotionaldistressandsocialsupport influ-enceQOLaboveandbeyonddiseaseactivity.Itappearsthat RApatientscouldbenefitfromafocusonalleviatingthe emo-tionaldistressassociatedwiththeirchronicdisease,aswell asthemedicaldiseasemanagementprovidedbyhealth pro-fessionals,throughmorecomprehensiveRApatientcare.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. ScottDL,WolfeF,HuizingaTW.TheLancetseminar: rheumatoidarthritis.Lancet.2010;376:1094–108.
2. CardielMH.Latin-AmericanRheumatologyAssociationsof thePan-AmericanLeagueofAssociationsforRheumatology (Panlar),GrupoLatinoamericanodeEstudiodeArtritis Reumatoide(Gladar),FirstLatin-Americanpositionpaperon thepharmacologicaltreatmentofrheumatoidarthritis. Rheumatology(Oxford).2006;45Suppl.2:ii7–22. 3. AnayaJM,CorreaPA,MantillaRD,JimenezF,KuffnerT,
McNichollJM.RheumatoidarthritisinAfricanColombians fromQuibdo.SeminArthritisRheum.2001;31:191–8. 4. CaballeroUribeCV.Artritisreumatoidecomoenfermedadde
altocosto.RevColombReumatol.2004;11:225–31. 5. MaskaL,AndersonJ,MichaudK.Measuresoffunctional
statusandqualityoflifeinrheumatoidarthritis:health assessmentquestionnairedisabilityindex(HAQ),modified healthassessmentquestionnaire(MHAQ),multidimensional healthassessmentquestionnaire(MDHAQ),health
assessmentquestionnaireII(HAQ-II),improvedhealth assessmentquestionnaire(improvedHAQ),andrheumatoid arthritisqualityoflife(RAQoL).ArthritisCareRes.
2011;63(S11):S4–13.
6. DominickKL,AhernFM,GoldCH,HellerDA.Health-related qualityoflifeamongolderadultswitharthritis.HealthQual LifeOutcomes.2004;2:5.
7. KolahiS,KhbaziA,HajalilooM,NamvarL,FarzinH.The evaluationofqualityoflifeinwomenwithrheumatoid arthritis,osteoarthritisandfibromyalgiaascomparedwith qualityoflifeinnormalwomen.InternetJRheumatol. 2011;7:1.
8.KaneckiK,TyszkoP,WisłowskaM,Łyczkowska-PiotrowskaJ. Preliminaryreportonastudyofhealth-relatedqualityoflife inpatientswithrheumatoidarthritis.RheumatolInt. 2013;33:429–34.
9.SalaffiF,CarottiM,GaspariniS,IntorciaM,GrassiW.The health-relatedqualityoflifeinrheumatoidarthritis, ankylosingspondylitis,andpsoriaticarthritis:acomparison withaselectedsampleofhealthypeople.HealthQualLife Outcomes.2009;7:25–9.
10.LemppH,IbrahimF,ShawT,HofmannD,GravesH, ThornicroftG,etal.Comparativequalityoflifeinpatients withdepressionandrheumatoidarthritis.IntRevPsychiatry. 2011;23:118–24.
11.KvienT,UhligT.Qualityoflifeinrheumatoidarthritis.Scand JRheumatol.2005;34:333–41.
12.NasK,SaracAJ,GurA,CevikR,AltayZ,ErdalA,etal. Psychologicalstatusisassociatedwithhealthrelatedquality oflifeinpatientswithrheumatoidarthritis.JBack
MusculoskelRehabil.2011;24:95–100.
13.AlishiriGH,BayatN,AshtianiAF,TavallaiiSA,AssariS, MoharamzadY.Logisticregressionmodelsforpredicting physicalandmentalhealth-relatedqualityoflifein
rheumatoidarthritispatients.ModRheumatol.2008;18:601–8. 14.HyphantisT,KotsisK,TsifetakiN,CreedF,DrososA,Carvalho
AF,etal.Therelationshipbetweendepressivesymptoms, illnessperceptions,andqualityoflifeinankylosing spondylitisincomparisontorheumatoidarthritis.Clin Rheumatol.2013;32:635–44.
15.UhmDC,NamES,LeeHY,LeeEB,YoonYI,ChaiGJ. Health-relatedqualityoflifeinKoreanpatientswith rheumatoidarthritis:associationwithpain,diseaseactivity, disabilityinactivitiesofdailylivinganddepression.JKorean AcadNurs.2012;42:434–42.
16.RuppI,BoshuizenHC,JacobiCE,DinantHJ,VandenBosG. Comorbidityinpatientswithrheumatoidarthritis:effecton health-relatedqualityoflife.JRheumatol.2004;31:58–65. 17.KarimiS,YarmohammadianMH,ShokriA,MottaghiP,
QolipourK,KordiA,etal.Predictorsandeffectivefactorson qualityoflifeamongIranianpatientswithrheumatoid arthritis.MaterSociomed.2013;25:158–62.
18.MokC,LokE,CheungE.Concurrentpsychiatricdisordersare associatedwithsignificantlypoorerqualityoflifeinpatients withrheumatoidarthritis.ScandJRheumatol.2012;41: 253–9.
19.MinnockP,FitzgeraldO,BresnihanB.Qualityoflife,social support,andknowledgeofdiseaseinwomenwith rheumatoidarthritis.ArthritisCareRes.2003;49:221–7. 20.RiemsmaRP,TaalE,RaskerJJ.Perceptionsaboutperceived
functionaldisabilitiesandpainofpeoplewithrheumatoid arthritis:differencesbetweenpatientsandtheirspousesand correlateswithwell-being.ArthritisCareRes.2000;13:255–61. 21.StantonAL,RevensonTA,TennenH.Healthpsychology:
psychologicaladjustmenttochronicdisease.AnnuRev Psychol.2007;58:565–92.
22.DemangeV,GuilleminF,BaumannM,SuurmeijerP,MoumT, DoeglasD,etal.Aretheremorethancross-sectional relationshipsofsocialsupportandsupportnetworkswith functionallimitationsandpsychologicaldistressinearly rheumatoidarthritis?TheEuropeanresearchon
incapacitatingdiseasesandsocialsupportlongitudinalstudy. ArthritisCareRes.2004;51:782–91.
23.StratingMM,SuurmeijerTP,VanSchuurWH.Disability,social support,anddistressinrheumatoidarthritis:resultsfroma thirteen-yearprospectivestudy.ArthritisCareRes. 2006;55:736–44.
25.LeiningerMM,McFarlandMR.Culturecarediversityand universality:aworldwidenursingtheory.Burlington:Jones& BartlettLearning;2006.
26.AletahaD,NeogiT,SilmanAJ,FunovitsJ,FelsonDT,Bingham CO,etal.Rheumatoidarthritisclassificationcriteria:an AmericanCollegeofRheumatology/EuropeanLeagueAgainst Rheumatismcollaborativeinitiative.ArthritisRheum. 2010;62:2569–81.
27.PrevooML,Van‘tHofMA,KuperHH,VanLeeuwenMA,Van DePutteLB,VanRielPL.Modifieddiseaseactivityscoresthat includetwenty-eight-jointcounts.Developmentand validationinaprospectivelongitudinalstudyofpatientswith rheumatoidarthritis.ArthritisRheum.1995;38:44–8.
28.FransenJ,StuckiG,VanRielPL.Rheumatoidarthritis measures:DiseaseActivityScore(DAS),DiseaseActivity Score-28(DAS28),RapidAssessmentofDiseaseActivityin Rheumatology(Radar),andRheumatoidArthritisDisease ActivityIndex(Radai).ArthritisCareRes.2003;49(S5):S214–24. 29.DanaoLL,PadillaGV,JohnsonDA.AnEnglishandSpanish
qualityoflifemeasureforrheumatoidarthritis.ArthritisCare Res.2001;45:167–73.
30.SpielbergerCD.State-traitanxietyinventory.PaloAlto: ConsultingPsychologistsPress;1983.
31.VirellaB,ArbonaC,NovyDM.Psychometricpropertiesand factorstructureoftheSpanishversionoftheState-Trait AnxietyInventory.JPersAssess.1994;63:401–12.
32.CohenS,KamarckMermelsteinR,HobermanR.Measuring thefunctionalcomponentsofsocialsupport.In:SarsonIG, SarasonBR,editors.Socialsupport:theory,research,and applications.TheHague:MartinusNijhoff;1985.p.73–94. 33.MerzEL,RoeschSC,MalcarneVL,PenedoFJ,LlabreMM,
WeitzmanOB,etal.ValidationofInterpersonalSupport EvaluationList-12(Isel-12)scoresamongEnglishandSpanish speaking,Hispanics/latinosfromtheHCHS/SOL
(SocioculturalAncillaryStudy).PsycholAssess.2013.Epub. 34.ZungWW,RichardsCB,ShortMJ.Self-ratingdepressionscale
inanoutpatientclinic:furthervalidationoftheSDS.Arch GenPsychiatry.1965;13:508–15.
35.Campo-AriasA,RuedaG,JulianaS,HerreraS,MarcelaZ, RodriguezDC,etal.Percepciónderendimientoacadémicoy síntomasdepresivosenestudiantesdemediavocacionalde Bucaramanga,Colombia.ArchPediatrUrug.2005;76:21–6. 36.DerogatisL.SCL-90.Administration,scoring,andprocedures
manual-IfortheR(revised)versionandotherinstrumentsof thePsychopathologyRatingScalesSeries.Chicago:Johns HopkinsUniversitySchoolofMedicine;1977.
37.CanavalGE,GonzálezMC,HumphreysJ,DeLeónN,González S.Partnerviolenceandwomen’shealthreportedtothefamily commissariesinCali,Colombia.InvestEducEnferm. 2009;27:209–17.
38.HinzA,FinckC,GómezY,DaigI,GlaesmerH,SingerS. Anxietyanddepressioninthegeneralpopulationin Colombia:referencevaluesoftheHospitalAnxietyand DepressionScale(Hads).SocPsychiatryPsychiatrEpidemiol. 2014;49:41–9.
39.Abraído-LanzaAF,RevensonTA.Copingandsocialsupport resourcesamongLatinswitharthritis.ArthritisRheum. 1996;9:501–8.
40.VinacciaS,TobónS,CadenaJ,AnayaJM,SanpedroEM. Evaluacióndelacalidaddevidaenpacientescondiagnóstico deartritisreumatoide.RevIntPsicolTerPsicol.2005;5: 45–59.
41.SmarrKL,KeeferAL.Measuresofdepressionanddepressive symptoms:BeckDepressionInventory-II(BDI-II),Centerfor EpidemiologicStudiesDepressionScale(CES-D),Geriatric DepressionScale(GDS),HospitalAnxietyandDepression Scale(HADS),andPatientHealthQuestionnaire-9(PHQ-9). ArthritisCareRes.2011;63(S11):S454–66.
42.SharpeL,SenskyT,TimberlakeN,RyanB,AllardS.Long-term efficacyofacognitivebehaviouraltreatmentfroma