w w w . r b o . o r g . b r
Original
Article
Effects
of
long-term
administration
of
omeprazole
on
bone
mineral
density
and
the
mechanical
properties
of
the
bone
夽
Gabriela
Rezende
Yanagihara
a,∗,
Aline
Goulart
de
Paiva
a,
Maurílio
Pacheco
Neto
a,b,
Larissa
Helena
Torres
c,
Antônio
Carlos
Shimano
d,
Mário
Jefferson
Quirino
Louzada
e,
Raquel
Annoni
a,
Álvaro
César
de
Oliveira
Penoni
aaPousoAlegreSchoolofMedicalSciences,UniversidadedoValedoSapucaí,PousoAlegre,MG,Brazil bDepartmentofClinicalPathology,SchoolofMedicine,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
cDepartmentofClinicalandToxicologicalAnalyses,SchoolofPharmaceuticalSciences,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil dRibeirãoPretoSchoolofMedicine,UniversidadedeSãoPaulo,RibeirãoPreto,SãoPaulo,SP,Brazil
eArac¸atubaSchoolofVeterinaryMedicine,UniversidadeEstadualPaulistaJúlioMesquitaFilho,Arac¸atuba,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6April2014 Accepted19May2014 Availableonline14March2015
Keywords:
Bone Bonedensity Omeprazole Rats
a
b
s
t
r
a
c
t
Objectives:Epidemiologicalstudieshaveshownarelationship betweenlong-termuseof protonpumpinhibitorsandbonemetabolism.However,thisrelationshiphasnotyetbecome established.Theaimofthepresentstudywastoanalyzethemechanicalpropertiesandbone mineraldensity(BMD)ofratsthatweresubjectedtolong-termomeprazoleuse.
Methods:Fifty Wistar rats weighing between 200 and 240g were divided equally into five groups: OMP300 (omeprazole intake at a dose of 300moL/kg/day); OMP200 (200moL/kg/day); OMP40(40moL/kg/day);OMP10(10moL/kg/day);andCont(control group;intakeofdilutionvehicle).Thesolutionswereadministeredfor90consecutivedays. Aftertheratshadbeensacrificed,theirBMD,themechanicalpropertiesofthedissected femursandtheirserumCa++levelswereanalyzed.
Results:TheBMDoftheOMP300groupwaslowerthanthatofthecontrols(p=0.006).There wasnodifferenceoncomparingtheOMP200,OMP40andOMP10groupswiththecontrols. Themaximumstrengthandrigidityofthefemurdidnotdifferintheexperimentalgroups incomparisonwiththecontrols.TheOMP300grouphadastatisticallylowerserumCa++ concentrationthanthatofthecontrols(p=0.049),buttheothergroupsdidnotshowany differenceinrelationtothecontrols.
Conclusion:Dailyintakeof300moL/kg/dayofomeprazoledecreasedtheBMDofthefemur, butwithoutchangestotherigidityandstrengthofthefemurinadultrats.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedatthePousoAlegreSchoolofMedicalSciences,UniversidadedoValedoSapucaí,PousoAlegre,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](G.R.Yanagihara).
http://dx.doi.org/10.1016/j.rboe.2015.03.002
Efeitos
da
administrac¸ão
em
longo
prazo
do
omeprazol
sobre
a
densidade
mineral
óssea
e
as
propriedades
mecânicas
do
osso
Palavras-chave:
Osso
Densidadeóssea Omeprazol Ratos
r
e
s
u
m
o
Objetivos: Estudosepidemiológicosmostramumarelac¸ãoentreousoemlongoprazode inibidoresdebombadeprótonseometabolismoósseo,porémessarelac¸ãoaindanãoestá estabelecida.Oobjetivodesteestudofoianalisaraspropriedademecânicaseadensidade mineralóssea(DMO)deratossubmetidosaousodeomeprazolemlongoprazo.
Métodos: Cinquenta ratos Wistar, entre 200 e 240g, foram divididos igualmente em cincogrupos:OMP300(ingestãodeomeprazolnadosede300moL/Kg/dia),OMP200(200
moL/Kg/dia),OMP40(40moL/Kg/dia),OMP10(10moL/Kg/dia)eCont(grupocontrole;
ingestãodoveículodediluic¸ão).Aadministrac¸ãodassoluc¸õesocorreudurante90dias segui-dos.Apósaeutanásia,foramanalisadasaDMO,aspropriedadesmecânicasdosfêmures dissecadoseadosagemdeCa++sérico.
Resultados: ADMOdogrupoOMP300foimenordoqueadoCont(p=0,006).Nãohouve diferenc¸anacomparac¸ãoentreosgruposOMP200,OMP40eOMP10emrelac¸ãoaoCont.A forc¸amáximaerigidezdofêmurnãoforamdiferentesnosgruposexperimentaisquando comparadosaoCont.OgrupoOMP300teveconcentrac¸õesséricasdeCa++estatisticamente menoresdoqueogrupoCont(p=0,049)semdiferenc¸aentreosdemaisgruposemrelac¸ão aoCont.
Conclusão: Aingestãodiáriade300moL/Kg/diadeomeprazoldiminuiuaDMOdofêmur, porémsemalterac¸õesnarigidezenaforc¸adofêmurderatosadultos.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Proton pump inhibitors (PPIs) are the main drugs used for treating diseases such as duodenal ulcers and reflux esophagitis.1,2 Because these drugs present few adverse effectswhen administeredcorrectly,they havecometo be usednot onlyforacute symptoms inclinical practice, but alsoforlong-termpurposes,eventhoughsuchindicationsare highlydebatable.3–5
PPIsactmainlytowardsuppressinggastricacidsecretion bythe parietalcells ofthe stomach,sincethey inhibitthe enzymeH+K+ATPase,andthisacidsuppressionmaylastfor upto48h.6
Epidemiological studies have indicated that there is a relationship between prolonged use of PPIs and bone metabolism,7–9 althoughthisrelationshipisstillnottotally established. Yang et al.4 reported that administration of omeprazole (20mg/day), which is one of the most impor-tantPPIs,iscapableofsignificantlydiminishingbonemineral density(BMD).Itisbelieved that themechanism responsi-bleforthisconsistsofelevationofgastricpH,whichwould interferewithcalciumabsorption.4,10,11Thisoccursbecause somesalts,suchascalcium,are insolubleinbasicpHand wouldthereforebeabsorbedlessreadily.8 However,astudy by Hyun et al.3 suggested that using omeprazole would tendtodiminishbonereabsorptionandimpedethe progres-siontowardosteoporosis.Therefore,therelationshipbetween usingPPIsand bonedemineralizationand the riskof frac-turesassociatedwithprolongeduseofomeprazoleremains unclear.9
GiventhatthereisevidencethatprolongeduseofPPIsmay changethebehaviorofbonecells,ourobjectiveherewasto analyzethebonemineraldensityandmechanicalproperties ofratfemursthatweresubjectedtolong-termuseof omepra-zole.
Materials
and
methods
Typeofstudy
Thiswasanexperimentalstudyusingananimalmodel.
Animals
The procedures used in this study followed the standards describedbytheBrazilianCollegeforAnimalExperimentation (COBEA)in1991andtheInternationalGuidingPrinciplesfor BiomedicalResearchInvolvingAnimals12andwereapproved bytheEthicsCommitteeforAnimalResearchoftheUniversity ofValedoSapucaí.
FiftymaleadultratsofWistarlineage,weighing200–240g, wereusedinthisstudy.Theanimalswerekeptundernormal environmentalandtemperatureconditions(21±2◦C; humid-ity of55–60%; and light/darkcycles of12h).They received wateradlibitumandfeedsuitableforrats.Fastingof6hwas maintainedduringthedaytimeperiod,beforethedaily proto-colwasstarted.
Administration of omeprazole or dilution vehicle
Start of protocol
Day 1 Day 66 Day 90
Weighing Sacrifice
Fig.1–Experimentaldesignduringtheexposureperiod.
–200mol/kg;(3)OMP40–40mol/kg;(4)OMP10–10mol/kg; and(5)control(Cont)–intakeonlyofthedilutionvehicle.
Solutions
All theexperiments were performedusing gradeI purified water from the Milli-Q system and using analytical grade reagents.Thedrugsolutionswerepreparedasdescribedby Larssonetal.13Theomeprazolegranules(8.5%;Pharma Nos-tra,Lavras, Minas Gerais, Brazil) were ground up with the aidofamortarand weredispersedinavehiclecontaining 0.25%hydroxyethyl cellulose4400(GalenaQuímica,Lavras, MinasGerais,Brazil)ina0.1Msolutionofsodiumbicarbonate (pH≈7.4).Thesuspensionswerepreparedatconcentrations of10,40,200and300mol/kg.
Experimentalprotocol
Overa90-dayperiod,theanimalsoftheexperimentalgroups receivedtheirrespectivedosesofomeprazoleandtheanimals ofthecontrolgroupreceivedthedilutionvehicle.Thedoses wereadministered orallybymeans ofgavage.Fig.1shows theexperimentaldesignoverthecourseofthe90daysofthe experiment.
Attheendofthe90daysofreceivingthecompounds,the animalswereagainweighed.Theywerethenanesthetizedby meansofintramuscularinjectionofxylazine hydrochloride (95mg/kg)andketaminehydrochloride(12mg/kg)and sacri-ficedbymeansofexsanguination,usingcardiacpuncture.14,15 Therightandleftfemursofeachanimalwereextractedfrom theirbodysegmentsandthemuscleandconnectivetissues weretotallyremoved.Theanimalsandthespecimenswere weighedsimultaneously.Afterweighingandmeasurement, thestructureswerekeptinchilled salinesolutionuntilthe dayofthedensitometricanalysisandmechanicaltests(not morethan48hafterthedissection).
Densitometricanalysis
Therightfemursweresubjectedtoanalysisinadual-emission X-raydensitometerfor small animals (Lunar® DPX Alpha).
Theimageswere allacquiredwiththefemursinthesame position, immersed in water at a depth of 2cm. The fol-lowingimagingoptions were selected:appendicular;typeI bone; high-resolution mode; 76kVp; 150A; collimation at the fine adjustment; and areas of standardized size com-prising40mminwidthand20mminlength.Inaccordance
with the manufacturer’s recommendations, the apparatus was calibrated using a phantom that the manufacturer supplied.
Theanalysesontheimagingexaminationswereperformed withtheaidofthesamecomputersoftwareashadbeenused forimageacquisition.Usingaselectiontool,theboneswere fullydemarcatedandinformationontheirmassandarea,and consequentlytheirmineraldensity,wasgathered.
Mechanicalanalysis
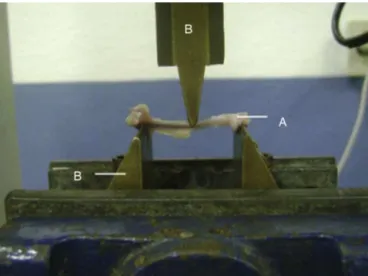
The animals’ left femurs were analyzed mechanically by meansofathree-pointmechanicalflexiontest(Fig.2).To per-formthesemechanicaltests, auniversaltest machinewas used (EMIC®, model DL 10000), with a load cell of
capac-ity 500N (certified by EMIC®), both of which belonged to
theBioengineeringLaboratoryoftheRibeirãoPretoSchoolof Medicine,UniversityofSãoPaulo,alongwithaccessories spe-ciallydevelopedforthree-pointflexiontestsonthebonesof smallanimals.16–18
The mechanical properties analyzed in the three-point flexiontestswerethemaximumstrength(Fmax)andrigidity (Rig).Thevelocityatwhichtheforcewasappliedinthe three-pointflexiontestswas1mm/min.Thespanbetweenthetest pointswas30mmand anaccommodationtimeof30swas used.
Fig.2–Three-pointmechanicalflexiontest:(A)bone
structure;(B)apparatusforapplyingforce.RibeirãoPreto
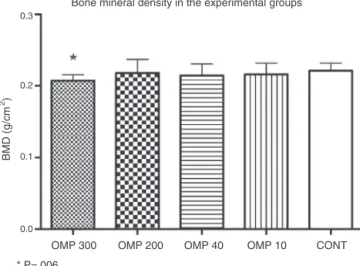
Bone mineral density in the experimental groups
OMP 300
BMD (g/cm
2)
OMP 200
* P=.006
OMP300 group compared with control group (Cont)
OMP 40 OMP 10 CONT 0.3
0.2
0.1
0.0
Fig.3–Graphshowingthebonemineraldensityresults
fromeachexperimentalgroup.Valuesareexpressedas
mean±standarddeviation.OMP300(omeprazole,
300mol/kg),OMP200(omeprazole200mol/kg),OMP40
(omeprazole40mol/kg),OMP10(omeprazole10mol/kg),
Cont(control);BMD,bonemineraldensity.
SerumCa++assay
Thebloodthathadbeencollectedthroughcardiacpuncture wasusedtoperformaserumcalciumassay,bymeansofa diagnostickitsuppliedbythecompanyDoles(Goiânia,Brazil). Aftercentrifugation(at1000g,for5min)oftheblood col-lectedbymeansofcardiacpuncture,theserumwascollected andtheserumcalciumassayswereperformedbymeansofa diagnostickitsuppliedbythecompanyDoles(Goiânia,Brazil). Themethodwasbasedon formationofa stainedcomplex betweencalciumandcresolphthaleininanalkalinemedium. Fortheanalyses,aFemto650®spectrophotometerwasused
(FemtoInd.eCom.deInstrumentosLtda.,SãoPaulo,Brazil), adjustedtoawavelengthof570nm.
Statisticalanalysis
Thestatisticalanalysisonthedatawasperformedusingthe SPSSsoftware(SPSS,Chicago,USA),version15.0.Totestthe normalityofthesample,theKolmogorov–Smirnovtestwas used.Becausethedatadistributionwasfoundtobenormal, comparisonsofparametersbetweenthecontrolgroupandthe otherexperimentalgroupsweremadeusingStudent’st-test. Tocomparetheanimals’weightsduringtheexperimentand theweightsofthefemurs,theone-wayANOVAtestwasused. Thesignificancelevelof5%(p≤0.05)wasusedandtheresults wereexpressedasmeans±standarddeviations.
Results
Duringtheexperiment,oneanimalbelongingtotheOMP300 groupwaslost.
Serum calcium concentration in the experimental groups
OMP 300
Ca
++
(mmol/L)
OMP 200
* P=.049.
OMP300 group compared with control group (Cont)
OMP 40 OMP 10 CONT
0 1 2 3 4 5 6
Fig.4–Serumcalciumconcentration(Ca++).Valuesare
expressedasmean±standarddeviation.OMP300
(omeprazole,300mol/kg),OMP200(omeprazole
200mol/kg),OMP40(omeprazole40mol/kg),OMP10
(omeprazole10mol/kg),Cont(control).
The animals’ mean weight did not differ between the groupsonday1(p=0.52),day66(p=0.74)orday90(p=0.45)of theexperiment(Table1).
ThebonedensityintheOMP300group(0.20±0.008g/cm2)
was lower than that ofthe Cont group (0.22±0.107g/cm2;
p=0.006). The other groups did not show any differ-ences in comparison with the control group: OMP200 (0.21±0.019g/cm2; p=0.644), OMP40 (0.21±0.015g/cm2;
p=0.305)andOMP10(0.21±0.016g/cm2;p=0.410)(Fig.3).
Therewerenodifferencesintheresultsrelatingtothe max-imumstrengthofthefemurs,incomparingtheContgroup with the other groups: OMP300 (p=0.09); OMP200 (p=0.55); OMP40(p=0.11)andOMP10(p=0.62).Likewise,therewereno differencesrelating tothe rigidityvalues,incomparingthe Contgroupwiththeothergroups:OMP300(p=0.98);OMP200 (p=0.84);OMP40(p=0.08)andOMP10(p=0.72).Thestrength andrigidityvaluesarelaidoutinTable1.
The serum concentration of Ca++ in the OMP300 group
(5.03±0.39mmol/L) was lower than that of the Cont group (5.39±0.35mmol/L; p=0.049). The other groups did not show any differences in comparison with the con-trol group: OMP200 (5.37±0.26mmol/L; p=0.860), OMP40 (5.40±0.25mmol/L;p=0.970)andOMP10(5.41±0.26mmol/L;
p=0.910)(Fig.4).
Discussion
Table1–Initial,meanandfinalweightsoftheanimals,maximumforce(Fmax)andrigidity(Rig).
Group Initialweight(g) Meanweight(g) Finalweight(g) Fmax(N) Rig(N/mm)
OMP300 196.88±14.90 357.55±39.61 379.44±43.94 92.35±11.61 154.92±33.52
OMP200 213.80±36.06 365.90±44.71 391.70±49.79 97.19±12.09 152.34±26.73
OMP40 223.40±39.90 355.10±57.83 382.10±59.283 91.22±14.93 130.30±18.50
OMP10 221.90±40.39 378.80±35.04 413.60±33.59 97.01±15.93 149.52±34.91
CONT 215.70±39.20 362.30±22.63 383.50±35.83 99.76±6.10 155.23±37.24
OMP300(omeprazole,300mol/kg),OMP200(omeprazole200mol/kg),OMP40(omeprazole40mol/kg),OMP10(omeprazole10mol/kg),Cont
(control).Resultsarepresentedasmean±standarddeviation.
inserum Ca++concentrationinthisgroup.However,useof omeprazolewasnotseentoinfluencethemechanical proper-tiesofthebonetissue.
Osteoporoticfracturesare considered tobeaworldwide
publichealthproblem.Themortalityrateduringthefirstyear afterhipfracturesisaround30%.19Ithasbeenestimatedthat intheUSA,1.5millionpeopleeveryyearareaffectedby frac-turesrelatingtoosteoporosis.Thisisaneventthatmayreduce qualityoflifeandincreasetheriskofdeath.5 However,the relationshipbetweentherisksofhipfractureandprolonged useofPPIsremainsunclear.
Inastudyconductedin1993,Mizunashietal.20evaluated theeffectofPPItherapyontheserumlevelsofparathormone (PTH)inasmallgroupofpatientswithgastriculcers(seven menand12women,withameanageof67±13years).The studyshowedthataftereightweeksoftherapywith omepra-zole,thePTH levelhad increasedby28% inrelationtothe baselineamongthesepatients,accompaniedbyincreasesin osteocalcin,alkalinephosphataseandtartrate-resistantacid phosphatase,whicharemarkersforboneformation.Thus,it wassuggestedthatinthatsmallgroup,therewasanincrease inboneformation,contrarytotheresultsfromthepresent study.
However,theurinaryexcretionofhydroxyprolineand cal-ciumamongthepatientsinthestudybyMizunashietal.20 decreased, whichmay suggest thatthere wasless calcium absorption.Thepossibilityforcomparisonwiththepresent studyislimited,giventhatthiswasanexperimentalstudy, whilethestudy byMizunashiet al.was conductedamong humans.Moreover,PTHwasonlymeasuredatonetimepoint, whichmaynotreflectthedynamiceffectofPTHovera24-h period;andalso,theomeprazoledoseand calcium supple-mentationamongthosepatientswasquestionable.
Ontheotherhand,severalpreviousstudieshave demon-stratedassociationsbetweenPPIuseandavarietyoffractures. Yang etal.4 stated that usingPPIs could cause deleterious effectsinbonetissueandcould increasetheriskof osteo-poroticfractures,especiallyafterfouryearsofcontinualuse. Vestergaardetal.21corroboratedthepreviousstudyand con-firmed the relationship between PPI use and osteoporotic fractures.Furthermore,Grayetal.22conductedaprospective analysisthatincluded161,806women,withtheaimof corre-latingPPIusewiththeriskofclinicalfractures.Theauthors concludedthattherewereassociationsbetweenPPIuseand occurrencesofclinicalfractures ofthe wrist,vertebraeand forearm. Thepresentstudy corroboratesthe previous find-ings,giventhatarelationshipbetweenomeprazoleuseand decreasedbonemineraldensitywasdemonstrated.Thiscan
betakentobeapredictivesignindicatingthatfracturesmay occurasaresultoflong-termPPIuse.
KayeandJick23conductedaretrospectivestudyinwhich PPIuseandtheriskofhipfractureswere evaluatedamong patientswithoutsignificantriskfactors.Theseauthors con-cludedthatpatientsintheagegroupof50–79yearswhomade useofPPIsdidnothaveriskfactorsandsowouldnothave higherfrequencyofhipfractures.Inthatstudy,the epidemi-ologicaldatausedcamefromthesamedatasourcethatYang etal.4usedin2006.However,Yangetal.4observedthatthe risksofhipfracturesincreasedwithPPIuse,especiallywhen usedforfouryearsormore.KayeandJicktooktheviewthat theresultsofYangetal.4referredonlytopatientswithsome formofriskfactorforhipfractures,giventhattheydidnot excludepatientswithsignificantriskfactors.
Targowniketal.9conductedacross-sectionalretrospective studyfollowedbyalongitudinalphase.Inthecross-sectional study,casesofhiporlumbarvertebralosteoporosiswere com-paredwithcontrolspresentingnormalbonemineraldensity. Inthelongitudinalanalysis,bonemineraldensityalterations amongpatientswhoeitherwereorwerenotusingPPIswere successivelyevaluated.Theresultsfromtheirstudyindicated thatchronicuseofPPIwasnotassociatedwithanincreased likelihoodofoccurrencesoffractures.Inaddition,theauthors concludedthathigherintensityofexposurewasnot associ-atedwithincreasedriskofpresentingosteoporosis.Inother words,theybelievedthattheriskoffractureswasrelatedto othervariablesthatwereindependentofthosecorrelatedwith osteoporosis.
Our study cannot be fully compared with that of Tar-gowniket al.,9 since ours was experimental. Nonetheless, it isknown that in addition to the mineral characteristics thatcanbeassessedusingDXA,boneshaveimportant vis-coelasticpropertiesthatallowthistissuetofulfillitsspecific functions.24,25 These properties are best evaluated through experimentalstudies,sincetheseenableexvivoanalyses.To ourknowledge,ourstudywasthefirsttoanalyzetheeffects ofPPIs onthe viscoelasticproperties ofthe bonetissueof animalssubjectedtodifferentdosesofomeprazolefora pro-longedtime.
especiallyamongovariectomizedfemalerats.Itcantherefore beconcludedthatthebonesofosteopenicfemaleratspresent alteredmechanicalproperties.
Despite the high dosages of medications and the long periodoverwhichtheanimalsremainedexposedto omepra-zole intake, the mechanism of action of the PPIs did not influenceanyofthemechanicalproperties ofthe bonesin ourstudy.Webelievethatthehighestdosestipulatedorthe lengthofusewasinsufficienttoalterthemechanical proper-tiesofthebones,eventhoughthesefactorsdiminishedthe bonemineralization.
WedidnotdeterminethedoseofPPIsintheseanimals thatcouldbestipulatedforsimulatingtheiruseinhumans. Thedoseofthismedicationthatisgenerallyadministeredto humansis20mgperday,althoughitmayreachupto90mg. However,itisnotknownwhattheequivalentdoseinanimals wouldbe.Itisknownthatomeprazolebindstoaround95%of theplasmainhumans28and,accordingtoRegårdhetal.,29the proportionofbindingwouldbelowerindogsandrats(90%and 87%,respectively).Thissuggeststhatasimplecalculationof doseperkilogramwouldnotreflectthedoseusedinhumans. Moreover,it hasbeen seenthatwhilethemean half-lifeof thisdrugis1hinhumansanddogs,half-livesintherangeof 5–15minhavebeenrecordedinrats.29
Somedose–responsestudiesonPPIsinanimalshavebeen conducted,butwithobjectivesthatdifferedfromthoseofour study.Londongetal.30conductedadose–responsestudyusing thedosesof30,60and90mg/kgandasecondstudyuseda doseof1–10mg/kg.31Adhikayetal.32usedadoseof3mg/kg inrats witha view to curing gastric ulcers that had been induced.In2003,Meloetal.33subjectedWistarratstointake 0.2mg/kg,withtheaimofevaluatingtheeffectofthisintake onpartialhepatectomy.Eventhoughmanydosageshavebeen observed,thereisnoconsensusintheliteratureonanimal experimentsregarding the PPI dose that would be equiva-lenttothoseusedinhumans,forthepurposeoflong-term testing.
ThepresentstudywasbasedontheworkbyCuietal.,1 inwhichtheobjectivesweresimilartoours,i.e.tostudythe long-termeffectsofPPIs.Cuietal.1treatedtheiranimalsfor 77days,atadoseof400mol.Thehighestdoseofthepresent study(300mol)wasstipulatedasslightlylowerthanthedose usedbythoseauthors,butwasusedfor90days,i.e.forslightly longerthaninthestudybyCuietal.1 Itcouldbeseenthat theeffectsweresimilar,sincethoseauthors alsoidentified decreasedbonemineraldensityamongtheiranimals.
Insummary,thepresent study demonstrated that long-termPPIusedidnotalterthemechanicalpropertiesofthe femursofadultrats.However,itwasobservedthatthefemurs ofthe ratssubjected todailyadministrationofomeprazole atadoseof300mol/kg/daydevelopedbone demineraliza-tion,whichmaysuggestthatthisgivesrisetopredisposition tobone fractures. Furtherexperimental studies using pro-tocolssimilartoourswouldbeusefulforconfirmingthese results.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
OursincerethankstoMessrs.LúcioIvandeMelo,JoséLopes and Marcos Martins for their assistance in caring for the animals,andtoMrs.NelsiNaraVieiraMarchetteforher con-tributionrelatingtothemedications.Alsotothepostgraduate studentBrunaRezende,forherhelpinthedensitometry anal-yses.
r
e
f
e
r
e
n
c
e
s
1.CuiGL,SyversenCM,ZhaoD,ChenHL.Long-term
omeprazoletreatmentsuppressesbodyweightgainandbone
mineralizationinyoungmalerats.ScandJGastroenterol.
2001;36(10):1011–5.
2.GuimarãesEV,MarguetC,CamargosPAM.Tratamentoda
doenc¸adorefluxogastroesofágico.JPediatr.2006;82(Suppl5):
133–45.
3.HyunJJ,ChunHJ,KeumB,SeoYS,KimYS,JeenYT,etal.Effect
ofomeprazoleontheexpressionoftranscriptionfactorsin
osteoclastsandosteoblasts.IntJMolMed.2010;26(6):877–83.
4.YangYX,LewisJD,EpsteinS,MetzDC.Long-termproton
pumpinhibitortherapyandriskofhipfracture.JAMA.
2006;296(24):2947–53.
5.YangY.Chronicprotonpumpinhibitortherapyandcalcium
metabolism.CurrGastroenterolRep.2012;14(6):473–9.
6.WagnerC.Eficáciadaassociac¸ãodeinibidoresdabombade
prótonscompastadehidróxidodecálciocomomedicac¸ão
intracanalemdentesderatoscomlesõesperiapicais
[dissertac¸ão].PortoAlegre:PontifíciaUniversidadeCatólica
doRioGrandedoSul.FaculdadedeOdontologia;2011.
7.KakehasiAM.Gastriteautoimuneegastriteassociadaà
infecc¸ãopelohelicobacterpylori–Estudohistológicoe
imuno-histoquímicodamucosagástricaoxínticaecorrelac¸ão
comadensidademineralóssea[tese].BeloHorizonte:
UniversidadeFederaldeMinasGerais:Faculdadede
Medicina;2008.
8.TargownikLE,LixLm,MetgeCJ,PriorHJP,LeungS,LeslieWD.
Useofprotonpumpinhibitorsandriskofosteoporosis
related.CMAJ.2008;179(4):319–26.
9.TargownikLE,LixLM,LeungS,LeslieWD.Proton-pump
inhibitorsuseisnotassociatedwithosteoporosisor
acceleratedbonemineraldensityloss.Gastroenterology.
2010;138(3):896–904.
10.WandallJH.Effectsofomeprazoleonneutrophilchemotaxis,
superoxideproduction,degranulation,andtranslocationof
cytochrome.GUT.1992;33(5):617–21.
11.ScaringiL,CornacchioneP,FettucciariK,RosatiE,RossiR,
MarcontiP,etal.Activityinhibitionofcytolyticlymphocytes
byomeprazole.ScandJImmunol.1996;44(3):204–14.
12.InternationalGuidingPrinciplesforBiomedicalResearch
InvolvingAnimals.CouncilforInternationalOrganizationsof
MedicalSciences(Cioms).Washington,DC:National
AcademyPress;1985.
13.LarssonH,CarlssonE,JungggrenU,OlbeL,SjöstrandSE,
SkanbergI,etal.Inhibitionofgastricacidsecretionby
omeprazoleinthedogandrat.Gastroenterology.
1983;85(4):900–7.
14.MelloJRB,MelloFB,EtgesRN,HollenbachC,RodriguesJM,
HirtzL.Toxicidadepré-clínicadefitoterápicocontendo
gossypiumherbaceum(algodoeiro)emratosWistar.LatAmJ
Pharm.2008;27(1):46–55.
15.SilvaAS,FernandesES,PintoRM,ReisJEP,GuerraMO,Peters
tratadascomextratodeginkgobiloba.RevInterdisciplEst
Experiment.2010;2(3):81–8.
16.MatheusJPC,MilaniJGPO,GomideLB,VolponJB,ShimanoAC.
Análisebiomecânicadosefeitosdacrioterapianotratamento
dalesãomuscularaguda.RevBrasMedEsporte.
2008;14(4):372–5.
17.FrateschiMEMJM.Efeitosdaimobilizac¸ãoeremobilizac¸ãoem
algumaspropriedadesmecânicasdoosso[dissertac¸ão].São
Carlos:UniversidadedeSãoPaulo,Bioengenharia;2002.
18.PugliesiHB,MoroCA,PaccolaCAJJ.Estudodaresistência
mecânicadoligamentocruzadoanterioremratosque
praticaramnatac¸ão.RevBrasOrtop.2005;40(5):260–9.
19.SzejnfeldVL,JenningsF,CastroCHM,PinheiroMM,LopesAC.
ConhecimentodosmédicosclínicosdoBrasilsobreas
estratégiasdeprevenc¸ãoetratamentodaosteoporose.Rev
BrasReumatol.2007;47(4):251–7.
20.MizunashiK,FurukawaY,KatanoK,AbeK.Effectof
omeprazole,aninhibitorofH+,K+-ATPase,onboneresorption
inhumans.CalcifTissueInt.1993;53(1):21–5.
21.VestergaardP,RejnmarkL,MosekildeL.Protonpump
inhibitors,histamineH2receptorantagonists,andother
antacidmedicationsandtheriskoffracture.CalcifTissueInt.
2006;79(2):76–83.
22.GraySL,LaCroixAZ,LarsonJ,RobbinsJ,CauleyJA,MansonJA,
etal.Protonpumpinhibitoruse,hipfracture,andchangein
bonemineraldensityinpostmenopausalwomen–results
fromthewomen’shealthinitiative.ArchInternMed.
2010;170(9):765–71.
23.KayeJA,JickH.Protonpumpinhibitoruseandriskofhip
fracturesinpatientswithoutmajorriskfactors.
Pharmacotherapy.2008;28(8):951–9.
24.NordinM,FrankelVH.Biomecânicabásicadosistema
musculoesquelético.3a.ed.RiodeJaneiro:Guanabara
Koogan;2003.
25.ShimanoAC,ShimanoMM.Ensaiostecnológicosdematérias
biológicos.In:VIICongressoBrasileirodeEngenharia
Biomédica.Florianópolis:SantaCatarina.AnaisdoVIIICebeb;
2000.
26.KodamaAC.Efeitosdoultrassompulsadodebaixa
intensidadeemummodeloósseoderatasovarectomizadas
analisadaspormeiodoensaiodeflexocompressão
[dissertac¸ão].SãoCarlos:UniversidadedeSãoPaulo,
Bioengenharia;2003.
27.PengZ,TuukkanenJ,ZhangH,JämsäT,VäänänenHK.The
mechanicalstrengthofboneindifferentratmodelsof
experimentalosteoporosis.Bone.1994;15(5):
523–32.
28.BRASIL.MinistériodaSaúde.Formulárioterapêuticonacional 2008:Rename2006.Brasília:MinistériodaSaúde;2008. Availablefrom:http://bvsms.saude.gov.br/bvs/publicacoes/
formularioterapeuticonacional2008.pdf
29.RegårdhCG,GabrielssonM,HoffmanKJ,LöfbergI,SkånbergI.
Pharmacokineticsandmetabolismofomeprazoleinanimals
andman–anoverview.ScandJGastroenterol.
1985;108(Suppl):79–94.
30.LondongW,LondongV,CederbergC,SteffenH.
Dose–responsestudyofomeprazoleonmeal-stimulated
gastricacidsecretionandgastrinrelease.Gastroenterology.
1983;85(6):1373–8.
31.TakeuchiK,KonakaA,NishijimaM,KatoS,YasuhiroT.
Effectsofpantoprazole,anovelH+/K+-ATPaseinhibitor,on
duodenalulcerogenicandhealingresponsesinrats:a
comparativestudywithomeprazoleandlansoprazole.J
GastroenterolHepatol.1999;14(3):251–7.
32.AdhikaryB,YadavSK,BandyopadhyaySK,ChattopadhyayS.
Epigallocatechingallateaccelerateshealingof
indomethacin-inducedstomachulcersinmice.Pharmacol
Rep.2011;63(2):527–36.
33.MeloGB,SilvaRL,FakhouriR,MeloVA,LimaSO.Efeitodo
omeprazoledopantoprazolsobrearegenerac¸ãohepática
apóshepatectomiaparcialemratos.ActaCirBras.