www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Antioxidant
therapy
in
the
elderly
with
tinnitus
夽
,
夽夽
José
Fernando
Polanski
a,b,∗,
Alexandra
Dezani
Soares
a,
Oswaldo
Laércio
de
Mendonc
¸a
Cruz
a,caFederalUniversityofSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
bHospitaldeClínicas,FederalUniversityofParaná(UFPR),Curitiba,PR,Brazil
cDepartmentofOtorhinolaryngologyandHeadandNeckSurgery,UniversidadeFederaldeSãoPaulo(UNIFESP),
SãoPaulo,SP,Brazil
Received16December2014;accepted27April2015 Availableonline17October2015
KEYWORDS Tinnitus; Antioxidants; Aged
Abstract
Introduction:Severalapproacheshavebeentriedforthetreatmentoftinnitus,from cognitive-behavioraltherapiesandsoundenrichmenttomedication.Inthiscontext,antioxidants,widely usedinnumerousareasofmedicine,appeartorepresentapromisingapproachforthecontrol ofthissymptom,whichoftenispoorlycontrolled.
Objective: Toevaluatethe effectsofantioxidant therapyfor tinnitus inagroup ofelderly patients.
Methods:Prospective,randomized,double-blinded,placebo-controlledclinicaltrial.The sam-pleconsistedof58subjectsaged60yearsorolder,withacomplaintoftinnitusassociatedwith sensorineuralhearingloss.TheseindividualscompletedtheTinnitusHandicapInventory(THI) questionnairebeforeandaftersixmonthsoftherapy.Thetreatmentregimenswere:Ginkgo bilobadryextract(120mg/day),␣-lipoicacid(60mg/day)+vitaminC(600mg/day),papaverine
hydrochloride(100mg/day)+vitaminE(400mg/day),andplacebo.
Results:TherewasnostatisticallysignificantdifferencebetweenTHIbydegree(p=0.441)and byscore(p=0.848)beforeandaftertreatment.
Conclusion: Therewasnobenefitfromtheuseofantioxidantagentsfortinnitusinthissample. © 2015Associac¸˜aoBrasileira de Otorrinolaringologiae CirurgiaC´ervico-Facial.Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Please citethisarticleas:Polanski JF, Soares AD,de Mendonc¸a CruzOL. Antioxidanttherapy in theelderly withtinnitus. BrazJ
Otorhinolaryngol.2016;82:269---74.
夽夽Institution:DepartmentofOtorhinolaryngologyandHeadandNeckSurgery,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,
SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](J.F.Polanski).
http://dx.doi.org/10.1016/j.bjorl.2015.04.016
PALAVRA-CHAVE Zumbido;
Antioxidantes; Idoso
Efeitodaterapiacomantioxidantessobreozumbidoemidosos
Resumo
Introduc¸ão:Uma série de abordagens terapêuticas tem sido empregada no tratamento do zumbido,desdeterapiascognitivo-comportamentaisedeenriquecimentosonoroatéterapias medicamentosas.Nessecontexto,osagentesantioxidantes,amplamenteutilizadosem diver-sasáreasdamedicina,parecemrepresentarumaperspectivapromissoraparaocontroledesse sintoma,quemuitasvezestemumcontroleclínicoinsatisfatório.
Objetivo:Avaliarosefeitosdaterapiacomagentesantioxidantessobreozumbidoemumgrupo depacientesidosos.
Método: Ensaio clínico prospectivo, randomizado, duplo-cego e controlado por placebo.A amostracompostade58indivíduoscom60anosoumais,comqueixaclínicadezumbido asso-ciado à perdaauditiva, dotipo neurossensorial, em graus variados.Esses indivíduos foram submetidos ao questionárioTHI(Tinnitus Handicap Inventory)anteseapós6 mesesdeuso damedicac¸ão.Osesquemas terapêuticos foramosseguintes:extratoseco deGinkgobiloba (120mg/dia),ácido␣-lipóico(60mg/dia)+vitaminaC(600mg/dia),cloridratodepapaverina
(100mg/dia)+vitaminaE(400mg/dia)eplacebo.
Resultados: OTHIapósotratamentofoiestatisticamenteigualao THIantesdotratamento, tantoemgraus(p=0,441)quantoemescores(p=0,848).
Conclusão:Não se verificou benefício estatisticamente significativo com o uso de agentes antioxidantesparaozumbidodosindivíduosavaliados.
©2015Associac¸˜aoBrasileira deOtorrinolaringologiaeCirurgiaC´ervico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Tinnitus,whose prevalence is estimated at approximately 10%oftheadultpopulation,hasrepercussionsandanimpact onquality of life of the affected individuals, that varies fromaslightperceptionwithoutdiscomforttoanextreme compromiseinqualityoflife.1
Forthosewhosetinnitushassignificant clinicalimpact, anumber oftherapeutic approaches have been described and employed, from cognitive-behavioral therapies and soundenrichment,todrugapproaches. Somestudieshave shown favorable results, while others did not result in benefits.2Varioussubstanceshavebeenusedandtestedas
drugtreatments.Amongthem,antioxidantshaveappeared promising.2 Antioxidants encompass a wide range of
sub-stances whose primary function is the neutralization and clearance of free radicals, that is, because of their molecular configuration, result in being toxic and harm-ful to cells and tissues. With respect to the auditory system, the action of free radicals in cochlear physi-ology has been demonstrated experimentally.3---6 In the
case of auditory disorders, antioxidants have been used in sudden deafness, to try to prevent ototoxicity, and for acute acoustic trauma,7,8 as well as in the approach
to presbycusis, sometimes with conflicting results.9,10 In
cases of tinnitus, probably the substance most widely used and studied currently is Ginkgo biloba, an herbal antioxidant. Associations of antioxidants, vitamins, and phospholipidsadministeredtopatientsdiagnosedwith idio-pathic tinnitus demonstrated relief of this condition and decreased serum levels of free radicals in a case series study.11
Thus,itwasdecidedtotesttheeffectsofantioxidantson tinnitusinagroupofelderlypatientsinacontrolledclinical study.
Methods
TheresearchprojectwassubmittedtotheEthics Commit-teeonInstitutionalResearchandapprovedunderNo.CEP 0723/10.
The research was registered with the International ClinicalTrialsplatformoftheWorldHealthOrganizationat:
http://apps.who.int/trialsearch/trial.aspx?trialid=ACTRN 12610000667011.
Thesample wascomposedof 58maleandfemale sub-jects aged 60 years or older with clinical complaints of tinnitus associated with a variable degree of sensorineu-ralhearinglossconfirmedbypreviousaudiometric testing. These subjects were administered the Tinnitus Handicap Inventory (THI) questionnaire12 before and after
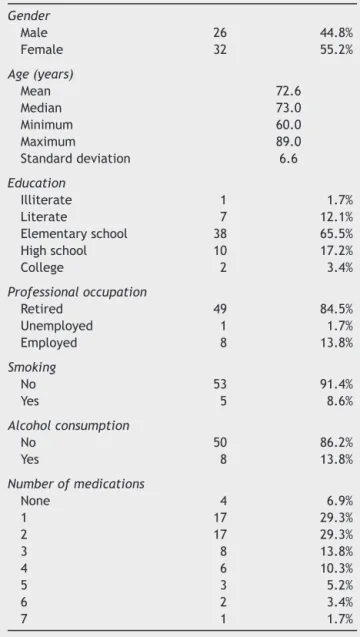
Table1 Profileofindividualswithcomplaintsoftinnitus. Gender
Male 26 44.8%
Female 32 55.2%
Age(years)
Mean 72.6
Median 73.0
Minimum 60.0
Maximum 89.0
Standarddeviation 6.6
Education
Illiterate 1 1.7%
Literate 7 12.1%
Elementaryschool 38 65.5%
Highschool 10 17.2%
College 2 3.4%
Professionaloccupation
Retired 49 84.5%
Unemployed 1 1.7%
Employed 8 13.8%
Smoking
No 53 91.4%
Yes 5 8.6%
Alcoholconsumption
No 50 86.2%
Yes 8 13.8%
Numberofmedications
None 4 6.9%
1 17 29.3%
2 17 29.3%
3 8 13.8%
4 6 10.3%
5 3 5.2%
6 2 3.4%
7 1 1.7%
The entire group wasinterviewedindetail about their medical history, and the data were recorded. Then, par-ticipants were asked to give information about hearing loss duration, use (or not) of hearing aids, hyperten-sion, dyslipidemia, heart disease, thyroid disease, and osteoarthropathy,andalsoinmen,benignprostatic hyper-plasia.Thesubjectswerealsoaskedaboutpossibleexposure to ototoxic substances or noisy environments, i.e., an exogenous auditory risk. In addition,a clinical exam was performed,focusedonotoscopy.
Patients were treated for a period of six months. They were allocated into four groups and treated with one of the following regimens: dry extract of G. biloba
(120mg/day), ␣-lipoic acid (60mg/day) plus vitamin C (600mg/day), papaverinehydrochloride(100mg/day)plus vitamin E (400mg/day), and placebo (starch capsules). The substances were not identified by name in the con-tainers into which they were packed, but rather through symbols definedbya professionalwhodidnotparticipate in the research, as a way of blinding investigators and patients.Fordistributionandrandomizationofparticipants,
Table 2 Distribution of the presence of comorbidities reportedbypatientswithcomplaintsoftinnitus.
Hearingaiduse
No 55 94.8%
Yes 3 5.2%
Systemicbloodhypertension
No 20 34.5%
Yes 38 65.5%
Dyslipidemia
No 49 84.5%
Yes 9 15.5%
Heartdisease
No 58 100.0%
Yes ---
---Hypothyroidism
No 49 84.5%
Yes 9 15.5%
Osteoporosis
No 49 84.5%
Yes 9 15.5%
Arthropathy
No 52 89.7%
Yes 6 10.3%
Benignprostatichyperplasia(amongmen)
No 22 84.6%
Yes 4 15.4%
Othercomorbidities
No 38 65.5%
Yes 20 34.5%
Hearinglosstime(years)
Mean 6.7
Median 5.0
Minimum 1.0
Maximum 25.0
Standarddeviation 4.9
Hearingrisk(exposuretooccupationalnoiseandto ototoxics)
No 52 89.7%
Yes 6 10.3%
Otoscopy
Nodistinctivefactors 57 98.3% Bilateraltympanosclerosis 1 1.7%
theresourcesavailableat http://www.randomization.com
wereused.
The statisticaltestsusedintheanalysisincluded Pear-son’schi-squaredtest,Fisher’sexacttest(oritsextension), andanalysisofvariancewithparametricandnon-parametric repeatedmeasures.Inallconclusions reachedthroughthe inferentialanalysis,thesignificancelevel˛=5%wasused.
Results
Thegeneralepidemiologicaldataofthesamplearelistedin
Table3 DistributionofTinnitusHandicapInventory(THI)bydegreeofsubjectswithcomplaintoftinnitus,forplacebo(P), Ginkgobiloba120mg/day(GB),␣-lipoicacid60mg/dayplusvitaminC600mg/day(AA+VC), andpapaverinehydrochloride
100mg/dayplusvitaminE400mg/day(PP+VE)groups,beforeandaftertreatmenttimepoints.
P GB AA+VC PP+VE
THIdegree---before
1 7 53.8% 3 25.0% 3 23.1% 4 26.7%
2 2 15.4% 5 41.7% 5 38.5% 8 53.3%
3 1 7.7% 3 25.0% 1 7.7% 1 6.7%
4 3 23.1% --- --- 4 30.8% 1 6.7%
5 --- --- 1 8.3% --- --- 1 6.7%
Total 13 100.0% 12 100.0% 13 100.0% 15 100.0%
THIdegree---after
1 7 53.8% 3 25.0% 4 30.8% 4 26.7%
2 3 23.1% 5 41.7% 5 38.5% 6 40.0%
3 1 7.7% 1 8.3% --- --- 3 20.0%
4 2 15.4% 2 16.7% 4 30.8% 1 6.7%
5 --- --- 1 8.3% --- --- 1 6.7%
Total 13 100.0% 12 100.0% 13 100.0% 15 100.0%
Themostsignificantgeneralclinicaldataofthesample arelistedinTable2.
Table3liststhedistributionofTHIbydegreeforsubjects withcomplaintsoftinnitus,inthedifferentgroups andin thetimepointsbeforeandaftertreatment.
Table4liststhedistributionofTHIinscoresforsubjects withcomplaintsoftinnitus,inthedifferentgroups andin thetimepointsbeforeandaftertreatment.
After statistical analysis, it was concluded that THI beforetreatment wasstatisticallyequivalenttoTHI after treatment, both by degree (p=0.441) and by score (p=0.848). Additionally, the inferential results revealed thatthefourtreatmentgroupswerestatisticallyequivalent, both in THI expressed by degree (p=0.663) and by score (p=0.715).
Discussion
Anumberofantioxidantshavebeenstudied,showing posi-tiveeffectsinseveralclinicalconditions.13---15Inthisstudy,
thechoiceoftheselectedsubstanceswasbasedonthe evi-dence and descriptions in the literature, both in clinical andexperimentalresearch,andalsoontheiravailabilityin this community. Briefly,G. biloba canbe described asan herbal medicine whose activepharmacologicalgroups are flavonoidswithantioxidantandvasodilatoraction,and ter-penelactones,whichactasantiplateletagents.16Originally,
␣-lipoicacidwasconsideredaspartofthevitaminB com-plex,butnowisnolongerconsideredasavitamin,because thereisevidencethatthissubstancecanbesynthesizedby thehumanbody.␣-Lipoicacidhasanantioxidanteffectand
Table4 DistributionofTinnitusHandicapInventory(THI)by scoreofsubjects withcomplaintoftinnitus,for placebo(P), Ginkgobiloba120mg/day(GB),␣-lipoicacid60mg/dayplusvitaminC600mg/day(AA+VC), andpapaverinehydrochloride
100mg/dayplusvitaminE400mg/day(PP+VE)groups,beforeandaftertreatmenttimepoints.
P GB AA+VC PP+VE
THIscore---before
n 13 12 13 15
Mean 28.2 32.8 38.8 28.0
Median 14.0 29.0 32.0 24.0
Minimum---maximum 2---72 12---80 4---76 2---96
Standarddeviation 25.1 19.9 24.7 23.8
THIscore---after
n 13 12 13 15
Mean 24.2 34.8 32.5 30.4
Median 14.0 24.0 24.0 24.0
Minimum---maximum 0---64 6---80 0---72 2---96
Standarddeviation 23.1 24.7 25.5 25.0
alsoanoxidativereductioneffectonother antioxidants.14
Vitamin E is an essential fat-soluble vitamin whose main functionisrelatedtothelipidstabilityofcellmembranes againstoxygenfreeradicals.Thisvitaminalsohasa modu-latingeffectoncellgrowth,inresponsetooxidativestress, hence its positive effect on atherosclerosis and certain neoplasms.17 VitaminCor ascorbicacidis awater-soluble
vitamin, criticalfor collagen andl-carnitine biosynthesis,
for theconversion of dopaminetonorepinephrine;it also improves iron absorption. Under physiological conditions, this vitamin also acts asa potent antioxidant.18
Papaver-inehydrochlorideisasyntheticalkaloidthatexertsatissue protective effectcorrelated toantioxidants, because this substancepromotesnon-specificsmoothmusclerelaxation, leading to vasodilation.19 Antioxidants act synergistically
withother agents or in isolation, functioning in different ways,protectingcellmembranesandalsoeliminating oxy-genfreeradicals.4,6
The afflictions of the auditory apparatus are complex conditions thatinvolve a number of physical phenomena, varioustissues,anddifferenttopographiesoftheauditory pathway. Tinnitusappearstobecaused by abnormal neu-ralactivityincochlea---auditorycortexpathway.20Thereisa
consensusintheliteraturethatatleastsomeofthechanges found alongthe auditorypathwayand relatedtoauditory symptoms appear to be related to biochemical changes, inflammation,andinjuriesinducedbyfreeradicals.8
The main cause of tinnitus is damage to hearing sen-sorycellsofthecochlea,withorwithoutassociationtoan injuryofcentralauditorysystemstructures,throughseveral etiopathogenicmechanisms.21Subjectswithnormalhearing
mayalsohavetinnitus;however,patientswithhearingloss maynothavetinnitus.Thesampleofthisstudywasentirely composedofsubjectswithtinnitusandsensorineural hear-ingloss.
With regard to the sample, anticoagulant users were excludeddue tothe chanceof bleedingwhenthesedrugs arecombinedwithG.biloba,whichhaveanantithrombotic effect.Anothergroup excluded wasdiabetics, due tothe chanceofglycemicimbalancewhenincombinationwith␣ -lipoic acid.14 Given the authors’ intention totest several
substancesin averydefinedpopulation group,thegroups hadarelativelylimitednumberofsubjects,buttheywere methodologicallysoundforthisstudyanditsstatistical eval-uation.
Thesubstanceschosenwereprocessedinacompounding pharmacy,sincethecombinationsusedarenotcommercially available.This wasalsoimportantintheblindingprocess, since the substanceswere packaged in identical capsules andidenticalbottles,butwereidentifiedbydifferent sym-bols, so they could not be identified by the subjects or researchers.The person responsible for handling the sub-stanceswasawareofthiscondition.Thedosesofsubstances used were based on what the literature recommends as an effective and clinically safe dose. In this study, there werenoadverse effects withthesesubstancesduring the study period and at the doses used. Moreover, according tothe literatureand pharmacologicalresearch,thereare no reports on the associations of substances proposed in this study, nor information to indicate that, once associ-ated,theycouldshowdecreasedinteractionorsummation oftheireffects.Thiswascorroboratedbyourresults,since
nomodificationoftheresearchedsymptomoccurredafter treatment.
The effects of antioxidant therapy for tinnitus were evaluatedthroughTHI,12avalidatedandwidelyused
ques-tionnaireto evaluate the influence of tinnitus on quality of life of the subjects tested. As described earlier, there wasnoobservableeffectoftheantioxidantsontinnitusin thesamplegroupsforaperiodofsixmonths.Somereports indicatethattheuseofB-complexvitaminscouldbe bene-ficialincontrollingtinnitus.However,nocontrolledclinical trialhasproventhishypothesis.22RegardingG.bilobainthe
treatmentoftinnitus,asystematicreviewevaluating stud-iesontheuseofthissubstance(initsEGb761presentation) has demonstrated efficacy when compared to placebo.23
AnotherCochranegroupreview conductedin2013 didnot demonstrateefficacyofG.bilobainthetreatmentof tinni-tus,irrespectiveoftheforminwhichtheplantextractwas obtained.24Thepresentstudyusedcompoundeddryextract
ofG.biloba.
These findings also corroborate a recent international recommendation, against prescribing vitamin and dietary supplementsfor thetreatment ofpatientswithpersistent andclinicallyrelevanttinnitus.25
Conclusion
Inthetimeintervalandsampleevaluated,weobservedno statisticallysignificantbenefitfromtheuseofantioxidants fortinnitus.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.DavisA,ElRafaieA.Epidemiologyoftinnitus.In:TylerRS, edi-tor.Tinnitushandbook.SanDiego:ThomsonLearning;2000.p. 1---23.
2.Baguley D, McFerran D, Hall D. Tinnitus. Lancet. 2013;382: 1600---7.
3.ClericiWJ,YangL.Directeffectsofintraperilymphatic reac-tiveoxygenspeciesgenerationoncochlearfunction.HearRes. 1996;101:14---22.
4.SeidmanMD.Effectsofdietaryrestrictionandantioxidantson presbycusis.Laryngoscope.2000;110:727---38.
5.JaconoAA, HuB,KopkeRD,HendersonD,VanDeWaterTR, SteinmanHM.Changesincochlearantioxidantenzymeactivity aftersoundconditioningandnoiseexposureinthechinchilla. HearRes.1998;117:31---8.
6.Heman-AckahSE,JuhnSK,HuangTC,WiedmannTS.A combi-nationantioxidanttherapypreventsage-relatedhearinglossin C57BL/6mice.OtolaryngolHeadNeckSurg.2010;143:429---34. 7.JoachimsHZ,SegalJ,GolzA,NetzerA,GoldenbergD. Antiox-idants in treatment of idiopathic sudden hearing loss. Otol Neurotol.2003;24:572---5.
8.HaaseGM, Prasad KN,ColeWC, Baggett-StrehlauJM, Wyatt SE. Antioxidant micronutrient impact on hearing disorders: concept,rationale,andevidence.AmJOtolaryngol.2011;32: 55---61.
10.Polanski JF, Cruz OL. Evaluation of antioxidant treat-ment in presbycusis: prospective, placebo-controlled, double-blind, randomised trial. J Laryngol Otol. 2013;127: 134---41.
11.Savastano M, Brescia G, Marioni G. Antioxidant therapy in idiopathic tinnitus: preliminary outcomes. Arch Med Res. 2007;38:456---9.
12.Newman CW, Jacobson GP, Spitzer JB. Development of the tinnitushandicapinventory.ArchOtolaryngolHeadNeckSurg. 1996;122:143---8.
13.ByersT,BowmanB.VitaminEsupplementsandcoronaryheart disease.NutrRev.1993;51:333---6.
14.BilskaA,WlodekL.Lipoicacid---thedrugofthefuture? Pharma-colRep.2005;57:570---7.
15.Mahadevan S, Park Y. Multifaceted therapeutic benefits of GinkgobilobaL.:chemistry,efficacy,safety,anduses.JFood Sci.2008;73:14---9.
16.Smith JV, Luo Y. Studies on molecular mechanisms of Ginkgo biloba extract. Appl Microbiol Biotechnol. 2004;64: 465---72.
17.MeydaniM.VitaminE.Lancet.1995;345:170---5.
18.LiY,SchellhornHE.Newdevelopmentsandnoveltherapeutic perspectivesforvitaminC.JNutr.2007;137:171---84.
19.Mathis JM, JensenME, Dion JE. Technical considerations on intra-arterialpapaverinehydrochlorideforcerebralvasospasm. Neuroradiology.1997;39:90---8.
20.Eggermont J. Pathophysiology of tinnitus. Prog Brain Res. 2007;166:19---35.
21.NondahlDM,CruickshanksKJ,HuangGH,KleinBE,KleinR,Nieto FJ,etal.TinnitusanditsriskfactorsintheBeaverDamoffspring study.IntJAudiol.2011;50:313---20.
22.Seidman MD, Standring RT, Dornhoffer JL. Tinnitus: cur-rentunderstandingandcontemporarymanagement.CurrOpin OtolaryngolHeadNeckSurg.2010;18:363---8.
23.Von Boetticher A. Ginkgo biloba extract in the treatment of tinnitus: a systematic review. Neuropsychiatr Dis Treat. 2011;7:441---7.
24.HiltonMP,ZimmermannEF,HuntWT.Ginkgobilobafortinnitus. CochraneDatabaseSystRev.2013;3:CD003852.