jcoloproctol(rioj).2016;36(4):216–219
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Incidence
of
fistula
after
management
of
perianal
abscess
Riyadh
Mohamad
Hasan
UniversityofBaghdad,Al-KindyCollegeofMedicine,DepartmentofSurgery,Baghdad,Iraq
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2May2016 Accepted15May2016 Availableonline5July2016
Keywords:
Fistula Perianal Abscess
a
b
s
t
r
a
c
t
Background:Perianalfistulaisamongthemostcommonanorectaldiseasesencountered inadults,menaremorepronetobeaffectedthanwomen.Thereisacloserelationship ofabscessandfistulainetiology,anatomy,pathophysiology,therapy,complicationsand morbidity,itisappropriatetoconsiderthemasoneentity.
Aimofstudy:Todeterminetheincidenceoffistulaformationandrecurrentabscessina sampleofIraqipatientsinBaghdadanddecidewhetherprimaryfistulotomyshouldbe performedatthetimeofincisionanddrainageofperianalabscesses.
Patientsandmethods:Aretrospectivestudyof68patientswithperianalabscessoperations conductedinBaghdad.Theyunderwentincisionanddrainageundereitherlocalorgeneral anesthesiaatAl-KindyTeachingHospitalsandprivatehospitalsovera15-yearperiodfrom January2000toDecember2015.Theiragesrangedfrom20to68years(40.21±1.34)males (63/68)(92.64%)weremorethanfemales(5/68)(7.35%).Patientsweretreatedwithincision overtheabscessunderanesthesiaanddrainageoftheabscesswasdone.Thepatientswere followedupforanaverage18months(range12–24months)afterabscessdrainageoruntil afistulaappearedandabscessrecurrence.
Results:Thestudygroupcomprisedof68(92.64%)patientswithperianalabscesswitha medianage39years(range20–68years).Themeanfollow-upperiodwasidentifiedtobe18 months(range12–24months).Males(63/68)(92.64%)weremorethanfemales(5/68)(7.35%). Theincidenceoffistulaformationafterfollowup,thepatientswithperianalabscessafter incisionanddrainagewas31/68(45.58%)andmales(30/31)(44.11%)weremorethanfemales (1/31)(1.47%).Themostcommonsitewasposteriorthenleftlateralposition.The percent-ageofpatientswithrecurrentabscessn=6(8.82%)werelowerthanfistulaformationn=31 (45.58%).Thepercentageofmalesn=4/6(5.88%)weremorethanfemales2/6(2.94%).
Conclusions:TheincidenceofanalfistulainasampleofIraqipatientswithperianalabscess was45.58%andpercentageofrecurrenceofperianalabscesswas8.82%.Toavoiddivisionof
E-mail:[email protected] http://dx.doi.org/10.1016/j.jcol.2016.05.002
jcoloproctol(rioj).2 0 1 6;36(4):216–219
217
analsphinctermuscle,secondaryfistulotomyisadvisedtobedonelaterwhenanalfistula willbeformed.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Incidência
de
fistulas
em
seguida
ao
tratamento
de
abscesso
perianal
Palavras-chave:
Fístula Perianal Abscesso
r
e
s
u
m
o
Experiência: Afistulaperianalestáentreasmaiscomunsdoenc¸asanorretaisobservadasem adultos;oshomensdemonstrammaiortendênciaparaseremafetados,emcomparac¸ão comasmulheres.Existeíntimarelac¸ãoentreabscessosefistulasemtermoseetiologia, anatomia,fisiopatologia,tratamento,complicac¸õesemorbidade;assim,écabível considerá-loscomoumamesmaentidade.
Objetivodoestudo:Determinaraincidênciadeformac¸ãodefístulasedeabscessorecorrente emumaamostradepacientesiraquianosemBagdá,edecidirseafistulotomiaprimáriadeve serrealizadaporocasiãodaincisãoedrenagemdeabscessosperianais.Pacientese méto-dos:Estudoretrospectivode68pacientescomoperac¸õesparaabscessoperianalrealizadas emBagdá.FoirealizadaincisãoedrenagemsobanestesialocalougeralnoHospital-Escola Al-Kindyeemhospitaisprivadosaolongodeumperíodode15anos,dejaneirode2000até dezembrode2015.Asidadesvariavamde20a68(40,21±1,34)anos.Haviamaiornúmerode homens(63/68)(92,64%)doquedemulheres(5/68)(7,35%).Ospacientestiveramoabscesso tratadosobanestesia,efoirealizadaadrenagemdoabscesso.Ospacientesforam moni-torados,emmédia,durante18meses(variac¸ão,12-24meses)apósadrenagemdoabscesso, ouatéosurgimentodeumafístulaerecorrênciadoabscesso.
Resultados: Ogrupodeestudocompreendeu68(92,64%)pacientescomabscessoperianal, comidademedianade39anos(variac¸ão,20-68anos).Operíodomédiodeseguimentofoide 18meses(variac¸ão,12-24meses).Haviamaiornúmerodehomens(63/68)(92,64%)versus mulheres(5/68)(7,35%).Noseguimento,aincidênciadeformac¸ãodefístulanospacientes comabscessoperianalapósaincisãoedrenagemfoide31/68(45,58%),eoshomensforam maisafetados(30/31)(44,11%)versusmulheres(1/31)(1,47%).Olocalmaiscomumfoia posic¸ãoposteriore,emseguida,alateralesquerda.Opercentualdepacientescomabscesso recorrente(6,8,82%)foimaisbaixodoqueopercentualparapacientescomformac¸ãode fístula(31,45,58%).Opercentualdehomens(4/6,5,88%)foimaiorversusmulheres(2/6, 2,94%).
Conclusões: A incidênciadefístulaanalemumaamostra depacientesiraquianoscom abscessoperianalfoide45,58%eopercentualderecorrênciadeabscessoperianalfoide 8,82%.Paraevitaradivisãodomúsculoesfinctéricoanal,éaconselhávelfazeruma fistulo-tomiasecundáriamaistarde,quandoafístulaanaljáestiverformada.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Fistula is among the most common anorectal diseases encounteredin adults,Men are moreprone to beaffected than women.1 Thereis acloserelationshipofabscessand
fistulainetiology,anatomy,pathophysiology, therapy, com-plicationsandmorbidity,itisappropriatetoconsiderthemas oneentity.2Aprevioushistoryofperianalabscesscanusually
bementionedanddrainedeitherspontaneouslyorsurgically underlocalorgeneralanesthesia,thusafistula-in-ano rep-resentsthechronicphaseofongoingperianalabscess.3Itisa
commondiseasewithanincidenceofabout2casesper10,000 populationperyearandlikelytooccurbetweentheagesof 30 and50 years.4 Fistula inanoare either associatedwith
perianalabscessfromoutsetorasalatersignin26–37%ofthe time.5–7 Afterdrainagetheabscess,probethecorresponding
analcryptgently,lookingforafistulainano.Primary fistulo-tomymaybeattemptedwhenitisidentifiedandsuperficial.8
About1000primaryfistulotomiesweredoneduringdrainage ofanabscesswithnoadverseresults.9Onecansuspect
devel-opmentoffistulalateronwhenthereisaprolongeddrainage fromanincisionsitebeyond2–3monthsandabscessheals andrecursatthesamefirstlocation.10Abscessrecurrenceand
lateronfistulaformationisduetoinsufficientdrainageand lateonsetdrainage.11–13Theincidenceoffistulafollowingan
abscessincisionanddrainagewas26%andincidenceof recur-rentabscesswas37%.14,15Theanalcanalshouldbesearched
218
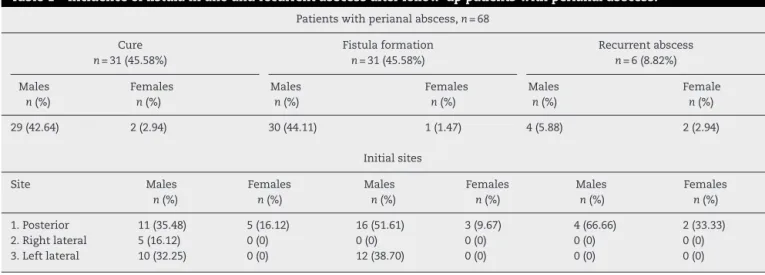
jcoloproctol(rioj).2 0 1 6;36(4):216–219Table1–Incidenceoffistulainanoandrecurrentabscessafterfollow-uppatientswithperianalabscess.
Patientswithperianalabscess,n=68 Cure
n=31(45.58%)
Fistulaformation
n=31(45.58%)
Recurrentabscess
n=6(8.82%) Males
n(%)
Females
n(%)
Males
n(%)
Females
n(%)
Males
n(%)
Female
n(%) 29(42.64) 2(2.94) 30(44.11) 1(1.47) 4(5.88) 2(2.94)
Initialsites Site Males
n(%)
Females
n(%)
Males
n(%)
Females
n(%)
Males
n(%)
Females
n(%) 1.Posterior 11(35.48) 5(16.12) 16(51.61) 3(9.67) 4(66.66) 2(33.33) 2.Rightlateral 5(16.12) 0(0) 0(0) 0(0) 0(0) 0(0) 3.Leftlateral 10(32.25) 0(0) 12(38.70) 0(0) 0(0) 0(0)
superficial, primary fistulotomy may be attempted using a loosesetonofbraided,nonabsorbablesuturethatinsertedinto thefistulatract,tiedlooselytoactasadrain.Thisistermeda “primary”or“synchronous”fistulotomywhichiscurativeand avoidtheneedforsubsequentfistulasurgery.8,10Ontheother
hand,abouttwothirdsofperianalabscessesneverprogress tofistulasandthat aprimaryfistulotomy withits possible complicationsisusuallyunnecessaryand thepatientswho areidealcandidatesforprimaryfistulotomyarealsothe eas-iesttotreat withdelayedfistulotomy withsubsequentlow morbidity.3Thus,theprudentrulewouldbetodefer
fistulo-tomyuntilthefistulabecomesobvious.
Theaimofthisstudywastoassesstheincidenceofanal fistulaand recurrentabscessafterincisionand drainageof perianalabscessinasampleofIraqipatientsinBaghdadand decidewhetherprimaryfistulotomyshouldbeperformedat thetimeofincisionanddrainageofanorectalabscesses.
Patients
and
methods
Aretrospectivestudyof68patientsoperateduponfor peri-analabscessconductedinBaghdad.Theyunderwentincision anddrainageundereitherlocalorgeneralanesthesiaat Al-KindyTeachingHospitalsandprivateHospitalsovera15-year periodfromJanuary2000toDecember2015.Theiragesranged from20to68years(40.21±1.34)males(63/68)(92.64%)were morethanfemales(5/68)(7.35%).Theinclusioncriteriawere adultsaged18yearsandabovewhopresentedwithperianal abscess,whiletheexclusioncriteriawerepatientsunder eigh-teenyears,abscesswithknownfistula,complicatedabscesses (multipleorbilateralabscess),Crohn’sdisease, immunosup-pression,malignancy,necrotizingfasciitisanddisseminated tuberculosis.TheScientificandEthicalCommitteeofAl-Kindy MedicalCollegeandHospitalshadapprovedthestudy. Writ-teninformedconsentswereobtainedfromthepatientswith perianalabscesses.
Patientsweretreatedwithincisionovertheabscessunder anesthesia(localorgeneral)thatallowsthorough examina-tionanddrainageoftheabscessandopeningallloculiwas done.Thepatientswerefollowedupforanaverage18months (range,12–24months)afterabscessdrainageoruntilafistula appearedandabscessrecurrence.
StatisticalanalysiswasdoneusingMINITABstatistical soft-ware13.20.
Results
Thestudygroupcomprisedof68(92.64%)patientswith peri-analabscesswithamedianageof39years(range20–68years). Themeanfollow-up periodwas identifiedtobe18months (range12–24months).Males(63/68)(92.64%)weremorethan females (5/68) (7.35%). All of them had a perianal abscess managed byincision and drainageunder anesthesia.Their durationofhospitalstaywas1–2days.
Theincidenceoffistulaformationafterfollowingupthe patientsoperatedforperianalabscesswas31/68(45.58%)and males(30/31)(44.11%)weremorethanfemales(1/31)(1.47%). Themostcommonsitewasposteriorthenleftlateralposition asshowninTable1.Thepercentageofpatientswithrecurrent abscessn=6(8.82%)werelowerthan fistulaformationn=31 (45.58%).Thepercentageofmalesn=4/6(5.88%)weremore thanfemales2/6(2.94%).Themostcommonsitewasalso pos-teriortoanus.Thepercentageofcuredpatients,31/68(45.58%) wassimilartopercentageofpatientswhodevelopedfistula, 31/68(45.58%).Maleswererepresentingthehigherpercentage 42.64%thanfemales2.94%.posteriorabscessrepresentsthe commonsite35.48%followedbyleftlateral32.25%andlastly therightlateral16.12%.
Discussion
Abscess and fistula in ano are common cryptoglandular disease16 which ismost common in people aged between
20 and 50 yearswithfour-fold male predominanceand an annualincidenceof1in10,000.17Thatisinagreementwith
our results, males were (63/68) (92.64%) that is more than females(5/68)(7.35%).Theirmedianagewas39years.Abscess after incision and drainage may manifests later on as fis-tulainanoandrecurrentabscessthatrequirerepeatsurgical drainage.Thus,treatingfistulaatthesametimemayreduce thelatesquealbutthiscouldaffectthefunctionoftheanal sphincter insomepatients who may nothave later devel-opedafistula-in-ano.18 Ourstudyshowedthatincidenceof
jcoloproctol(rioj).2 0 1 6;36(4):216–219
219
wasposteriorthen leftlateralposition.Regarding recurrent abscess,thepercentageofpatientswas6/68(8.82%)thatwas lowerthanfistulaformation31/68(45.58%).Thepercentage ofmales4/6(5.88%)wasmorethanfemales2/6(2.94%)and themostcommonsitewasalsoposteriortoanus.Ourresults inaccordancewithotherresults,thatrecurrentabscessand fistulaformationoccurredin11%and37%respectively.This supportstheruleofsecondaryfistulotomytoavoiddivision of sphincter muscle in patients who would not need it.15
Otherreportshowedthatrecurrenceofabscesswas3.7%and fistulaformation was 34.7%, so early aggressivetreatment ofabscessreducesthepossibilityofrecurrenceandfurther surgery.8Lohsiriwat etal.(2010)19 foundthatthe incidence
offistula-in-anofollowingincisionanddrainageofperianal abscesswas31%.Riskfactorslikesex,smoking,alcohol,fever; leukocytosis,andlocationofabscesswerenotprognosticand predictiveoffistulaformation.Patientsagedlessthan40years andnon-diabetic appearedtohaveahigher riskforfistula formation (43%). Regarding administration of perioperative antibioticssignificantlyreducedtherateofsubsequentfistula formationto(17%). Meta-analysisstudy demonstrated that fistulasurgerywithabscessdrainagesignificantlyreduced fis-tula/abscessrecurrenceandneedforfurthersurgery.20Sainio
(1984)1reportedtheincidenceofanalfistuladuringtenyears
periodper100,000populationwas8.6fornonspecificand fis-tula,12.3formalesand5.6forfemales.Healsoreportedthat nonspecificfistulaeaccountedabout90.4%,thetuberculous fistulaeabout0.2%,thepostoperativeandtraumaticfistulae about3.3%andfistulaeoriginatinginanalfissureabout3.3% andtheoccurrenceofanalfistulaaftertreatmentofperianal abscesswas35%whileinourstudywas(45.58%).Otherstudy showedthat the incidence offistula-in-anofollowing peri-analabscesseswas26%diagnosedeitherduringfollow-upor within6months.21Thedifferencesofourstudywithother
studiesmay bedue tosamplesize,criteria ofthepatients selectedinthestudy,durationoffollowup,useofantibiotics, sizeanddepthoftheabscessandsiteoftheabscess.Inour studythemostcommonlocationoftheabscesswasposterior, thisisduetomorefrequentanalglandslocatedposteriorly22,23
and morecommonlyfoundinmales than females.24 Thus
diseaseismorecommoninmalesthanfemales.
Conclusions
TheincidenceofanalfistulainasampleofIraqipatientswith perianalabscesswas45.58%andpercentageofrecurrenceof perianalabscesswas8.82%.Toavoiddivisionofanal sphinc-termuscle,secondaryfistulotomyisadvisedtobedonelater whenanalfistulawillbeformed.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SainioP.Fistula-in-anoinadefinedpopulation.Incidenceand epidemiologicalaspects.AnnChirGynaecol.1984;73:219–24.
2.AbcarianH.Anorectalinfection:abscess–fistula.ClinColon RectalSurg.2011;24:14–21.
3.WhitefordMH.Perianalabscess/fistuladisease.ClinColon RectalSurg.2007;20:102–9.
4.ZanottiC,Martinez-PuenteC,PascualI,PascualM,Herreros D,García-OlmoD.Anassessmentoftheincidenceof fistula-in-anoinfourcountriesoftheEuropeanUnion.IntJ ColorectalDis.2007;22:1459–62.
5.ReadDR,AbcarianH.Aprospectivesurveyof474patients withanorectalabscess.DisColonRectum.1979;22:566–8.
6.HenrichsenS,ChristiansenJ.Incidenceof
fistula-in-anocomplicatinganorectalsepsis:aprospective study.BrJSurg.1986;73:371–2.
7.NelsonR.Anorectalabscessfistula:whatdoweknow?Surg ClinNAm.2002;82:1139–51.
8.RamanujamPS,PrasadML,AbcarianH,TanAB.Perianal abscessesandfistulas.Astudyof1023patients.DisColon Rectum.1984;27:593–7.
9.McElwainJR,MacLeanMD,AlexanderRM,HoexterB,Guthrie JF.Anorectalproblems:experiencewithprimaryfistulectomy ofanorectalabscess:areportof1000cases.DisColon Rectum.1975;18:646–9.
10.RamanujamPS,PrasadML,AbcarianH.TheroleofSetonin fistulotomyoftheanus.SurgGynecolObstet.1983;157:419–22.
11.OnacaN,HirshbergA,AdarR.Earlyreoperationforperirectal abscess:apreventablecomplication.DisColonRectum. 2001;44:1469–73.
12.ChrabotCM,PrasadML,AbcarianH.Recurrentanorectal abscesses.DisColonRectum.1983;26:105–8.
13.YanoT,AsanoM,MatsudaY,KawakamiK,NakaiK,Nonaka M.Prognosticfactorsforrecurrencefollowingtheinitial drainageofananorectalabscess.IntJColorectalDis. 2010;25:1495–8.
14.ScomaJA,SalvatiEP,RubinRJ.Incidenceoffistulas subsequenttoanalabscesses.DisColonRectum. 1974;17:357–9.
15.VasilevskyCA,GordonPH.Theincidenceofrecurrent abscessesorfistula-in-anofollowinganorectalsuppuration. DisColonRectum.1984;27:126–30.
16.ParksAG.Pathogenesisandtreatmentoffistula-in-ano.Br MedJ.1961;1:463–9.
17.MaloufAJ,CadoganMD,BartoloDCC.Analcanal.In:Corson JD,WilliamsonRCN,editors.Surgery.London:Mosby;2001, 3.21.1-26.
18.GraceRH.Managementofacuteanorectalsepsis.In:Carter DCSir,RussellRCG,PittHA,editors.Atlasofgeneralsurgery. 3rded.London:ChapmanandHallMedical;1996.p.826–33.
19.LohsiriwatV,YodyingH,LohsiriwatD.Incidenceandfactors influencingthedevelopmentoffistula-in-anoafterincision anddrainageofperianalabscesses.JMedAssocThai. 2010;93:61–5.
20.MalikAI,NelsonRL,TouS.Incisionanddrainageofperianal abscesswithorwithouttreatmentofanalfistula.Cochrane DatabaseSystRev.2010;7:CD006827.
21.HenrichsenS,ChristiansenJ.Incidenceoffistula-in-ano complicatinganorectalsepsis:aprospectivestudy.BrJSurg. 1986;73:371–2.
22.AbeysuriyaV,SalgadoLS,SamarasekeraDN.Thedistribution oftheanalglandsandthevariableregionaloccurrenceof fistula-in-ano:istherearelationship.TechColoproctol. 2010;14:317–21.
23.Seow-ChoenF,HoJM.Histoanatomyofanalglands.DisColon Rectum.1994;37:1215–8.