Arq Neu ro p siq u iat r 2003;61(4):902-905
INFLUENCE OF INTRACRANIAL HEM ORRHAGE
AND NEONATAL SEIZURES ON THE NEUROLOGICAL
AND PSYCHOM OTOR DEVELOPM ENT OF PREM ATURE
INFANTS AT HOSPITAL DE CLÍNICAS DE PORTO
ALEGRE, BRAZIL
Lygia Ohlw eiler
1, Alexandre Rodrigues da Silva
2,
Sonja Vergínia Barros
2, Rudimar Riesgo
1, New ra Tellechea Rot t a
3ABSTRACT - This stud y com p ared the results of neurod evelop m ental exam ination at 6 m onths’ corrected ag e of p rem ature infants w ith neonatal seizures and /or intracranial hem orrhag e and norm al p rem ature infants. There w as a statistically sig nificant correlation (p = 0.000007) b etw een intracranial hem orrhag e and seizures in the group of 68 p rem ature infants seen in the neurod evelop m ental outp atient service at Hosp ital d e Clínicas d e Porto Aleg re, Brazil. Intracranial hem orrhag e w as sig nificantly associated w ith m ultip arity (p = 0.02). The neurod evelop m ental exam ination at 6 m onths’ corrected ag e revealed that p atients w ho suffered neonatal intracranial hem orrhag e and /or seizures had inap p rop riate m uscle tone, streng th and reflexes, as w ell as d elay in head control. Conclusion: w e com p ared the results of neurod evelop m ental exam inations of tw o g roup s of p rem ature infants at 6 m onths’ corrected ag e. The d ifference in neurolog ical d evelop m ent at 6 m onths’ corrected ag e w as statistically sig nificant w hen com p arison w as corrected for p rem ature infants w ho had neonatal seizures and p eriventricular hem orrhag e.
KEY WORDS: neurological and psychom otor developm ent, neonates, intracranial hem orrhage, neonatal seizures.
Influência da hemorragia intracraniana e crises neonatais sobre o desenvolvimento neurológico e psicomotor de recém-nascidos prematuros no Hospital de Clínicas de Porto Alegre, Brasil
RESUMO - Este estud o com p arou os resultad os d o exam e d o d esenvolvim ento neurop sicom otor aos seis m eses d e id ad e corrig id a d e lactentes p rem aturos com crises neonatais e/ou hem orrag ia intracraniana com la ct e n t e s p re m a t u ro s se m e st a s in t e rco rrê n cia s. Ho u ve u m a co rre la çã o e st a t ist ica m e n t e sig n ifica t iva (p = 0.000007) entre hem orrag ia intracraniana e crises neonatais no g rup o d e 68 lactentes p rem aturos vistos n o a m b u la t ó rio d e n eu ro d esen vo lvim en t o d o Ho sp it a l d e Clín ica s d e Po rt o Aleg re, Bra sil. Hem o rra g ia intracraniana foi sig nificativam ente associad a com m ultip arid ad e (p = 0.02). O exam e d o d esenvolvim ento neuropsicom otor aos 6 m eses de idade corrigida m ostrou que pacientes que sofreram hem orragia intracraniana neonatal e/ou crises neonatais tiveram tônus, forças e reflexos inap rop riad os, b em com o atraso no controle do sustento cefálico. Conclusões: Com param os os resultados dos exam es de desenvolvim ento neuropsicom otor d os d ois g rup os d e lactentes p rem aturos aos 6 m eses d e id ad e corrig id a. A d iferença no d esenvolvim ento neurológico aos 6 m eses d e id ad e corrigid a foi estatisticam ente significativa q uand o com p arad o com lactentes p rem aturos q ue tiveram crises neonatais e/ou hem orrag ia p eriventricular.
PALAVRAS-CHAVE: d esenvolvim ento neurológ ico e p sicom otor, recém -nascid os, hem orrag ia intracraniana, crises neonatais.
Un id ad e d e Neu ro lo g ia Ped iát rica d o Ho sp it al d e Clín icas d e Po rt o Aleg re (HCPA), Serviço d e Ped iat ria d o HCPA, Facu ld ad e d e Med icin a d a Un iversid ad e Fed eral d o Rio Gran d e d o Su l (FAMED - UFRGS), Po rt o Aleg re RS, Brasil: 1Ped iat ric Neu ro lo g ist ; 2Resid en t in Clild Neu ro lo g y; 3Head o f t h e Ped iat ric Neu ro lo g y Un it .
Received 14 Ju n e 2002, received in fin al fo rm 29 May 2003. Accep t ed 30 Ju n e 2003.
Dra. Lygia Ohlw eiler - Avenida Pirapó 71/702 - 90470-450 Port o Alegre RS - Brasil. E-mail: f p54@t erra.com.br
Prem aturity is a b iolog ical event with very d istinct an d so m etim es exclu sive ch aracteristics1. Th is even t,
w h ich m ay o r m ay n o t affect t h e fu t u re life o f p re-m a t u re in fa n t s, h a s b een in vest ig a t ed fo r a lo n g tim e2,3. Prem ature infants are neurologically d ifferent
from term infants b ecause they d o not com p lete cer-t ain in cer-t rau cer-t erin e n eu ro d evelo p m en cer-t al scer-t ag es3,4. Few
a-Arq Neu ro p siq u iat r 2003;61(4) 903
ture infants who had neonatal seizures or intracranial hemorrhage are even harder to obtain. Moreover, com-paring the neurological status of prem ature infants with that of term infants would be a serious error5,6.
The neurodevelopm ental exam ination is a useful tool in the assessm ent of these patients, who m ay have a b e t t e r p ro g n o sis a n d e a sie r re h a b ilit a t io n w h e n developm ental abnorm alities are identified early on.
The purpose of this study was to com pare the re-sults of neurodevelopm ental exam ination at 6 m on-ths’ corrected ag e for p rem ature infants that had neonatal seizures and intracranial hem orrhage with the results for neurologically normal premature infants.
M ETHOD
Sixt yeig h t p rem at u re p at ien t s in t h e Neu ro d evelo p -m en t a l Service a t Ho sp it a l d e Clín ica s d e Po rt o Aleg re (HCPA), Brazil, w ere selected an d d ivid ed in to tw o g ro u p s: p atients who had had intracranial hem orrhage and /or neon at al seizu res, aneon d p rem at u re ineon faneon t s w h o h ad neon o neon eu -rological p rob lem s. Patients with cereb ral hem orrhage that p rog ressed to hyd rocep halus and those w ith neonatal sei-zu res seco n d a ry t o in fect io n s o r g en et ic ca u ses w ere ex-clu d ed fro m t h e st u d y.
Th e g ro u p s w ere co m p ared w it h resp ect t o sex, race, m aternal ag e, m od e of d elivery, p arity, infant’s g estational ag e, w eig h t fo r g estatio n al ag e, b irth w eig h t, Ap g ar sco re at 5 m in u t es, u se o f m ech an ical ven t ilat io n , an d sep sis d uring gestation. Brain ultrasound stud ies were p erform ed fo r a ll p a t ien t s.
An experienced exam iner, blinded to patient’s group, exam ined the neurodevelopm ental status of infants at 6 months’ corrected age with respect to muscle tone, strength, deep tendon reflexes, Moro reflex, head control, sitting with support, and grasping objects. Results were analyzed with the software Epi-Info 6.04; level of significance was α = 0.05, β = 0.80, with 95% confidence intervals.
Th is st u d y w as ap p ro ved b y t h e Co m m it t ee fo r Et h ics in Resea rch , HCPA, a n d co n d u ct ed a ft er p a ren t s sig n ed an in fo rm ed co n sen t t erm .
RESULTS
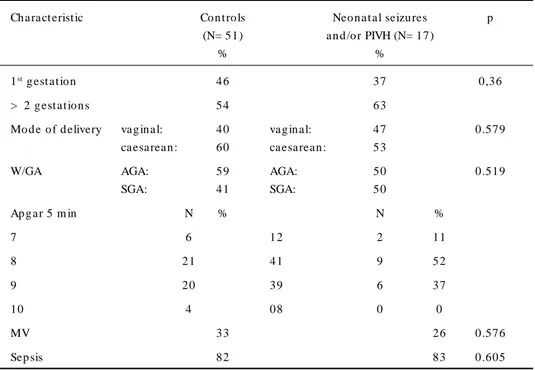
There were no significant differences between the g ro u p s w it h an d w it h o u t n eo n at al seizu res an d /o r in t racran ial h em o rrh ag e w it h resp ect t o sex, race, p arit y, g est at io n al ag e, w eig h t fo r g est at io n al ag e, Ap g ar sco re, m ech an ical ven t ilat io n , an d sep sis d u -ring hosp italization (Tab les 1 and 2). Six p atients had g rad e I h em o rrh ag e, an d five o f t h em h ad n eo n at al seizu res; t h ree h ad g rad e II h em o rrh ag e, an d all o f t h em h ad n eo n at al seizu res; o n e h ad g rad e II h e-m o rrh ag e an d n o seizu res; tw o h ad g rad e IV h ee-m o r-rh ag e, an d o n e o f t h em h ad n eo n at al seizu res. Th e fact o rs u n d er st u d y w ere o b served in 17 (25%) o f t h e 68 p a t ien t s, a n d t h ere w a s a st a t ist ica lly sig -nificant correlation between having neonatal seizures an d /o r h em o rrh ag e (p = 0.000007) (Tab le 3).
Th ere w ere n o d ifferen ces b etw een p atien ts w ith in t racran ial h em o rrh ag e an d co n t ro ls w it h resp ect t o sex, race, m at ern al ag e, m o d e o f d elivery, Ap g ar
Table 1. Pre- and perinat al charact erist ics.
Ch aract erist ic Co n t ro ls Neo n at al seizu res p
(N= 51) an d /o r PIVH (N= 17)
% %
1st g est at io n 46 37 0,36
> 2 g est at io n s 54 63
Mo d e o f d elivery vag in al: 40 vag in al: 47 0.579
caesarean : 60 caesarean : 53
W/GA AGA: 59 AGA: 50 0.519
SGA: 41 SGA: 50
Ap g ar 5 m in N % N %
7 6 12 2 11
8 21 41 9 52
9 20 39 6 37
10 4 08 0 0
MV 33 26 0.576
Sep sis 82 83 0.605
904 Arq Neu ro p siq u iat r 2003;61(4)
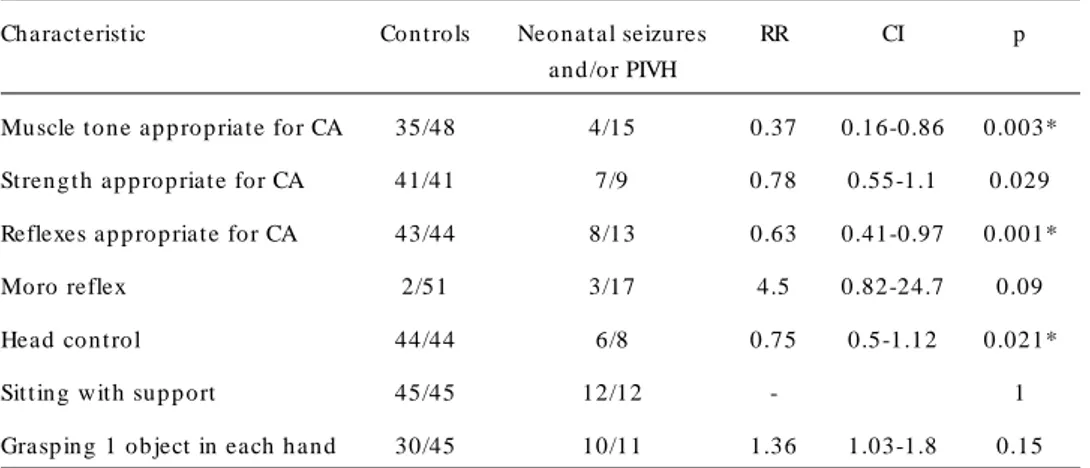
sco re, g est at io n al ag e, w eig h t fo r g est at io n al ag e, b irt h w eig h t , m ech an ical ven t ilat io n an d sep sis d u -rin g h o sp it alizat io n . Th ere w as a st at ist ically g reat er frequency of m ultiparity in the group of patients with in t racran ial h em o rrh ag e (p = 0.02). Th e n eu ro d eve-lo p m en t al exam in at io n p erfo rm ed at 6 m o n t h s’ is sh o w ed in t h e Tab le 4.
Th ere w ere n o d ifferen ces b etw een p atien ts w ith seizu res an d co n t ro l p at ien t s w it h resp ect t o sex, ra-ce, m aternal age, m ode of delivery, m ultiparity, Apgar sco re, g est at io n al ag e, w eig h t fo r g est at io n al ag e, b irt h w e ig h t , m e ch a n ica l ve n t ila t io n a n d se p sis d u rin g h o sp it alizat io n .
Again, no differences were found between patients with intracranial hem orrhage and seizures and con-trol patients with respect to sex, race, m aternal age, m ode of delivery, m ultiparity, Apgar score, gestational age, weight for gestational age, birth weight, m e-chanical ventilation, and sepsis during hospitalization.
DISCUSSION
Stud ies ab out the neurolog ical and p sychom otor d evelo p m en t o f p rem at u re in fan t s are q u it e recen t b ecau se t h e m o rt alit y rat es fo r t h ese p at ien t s u sed t o b e very h ig h so m e years ag o7,8. Th e creat io n an d
lat er d evelo p m en t o f n eo n at al in t en sive care u n it s
p ro m o t ed a sig n ifican t d ecrease in m o rt alit y an d in t h e o ccu rren ce o f b ro n ch o p u lm o n ary d ysp lasia an d interstitial em p hysem a9,10. The incid ence rate of
neu-rological sequelae in surviving infants is inversely pro-p o rt io n al t o g est at io n al ag e11. So m e im p o rt an t p h
ysio p at h o lo g ical fact o r m ay b e asso ciat ed t o t h e im -m at u rit y o f t h e cen t ral n ervo u s syst e-m (CNS), w h ich resu lt s in p o o r co n t ro l o ver t h e au t o n o m ic n ervo u s syst em (ANS) an d , co n seq u en t ly, o ver sp o n t an eo u s ven t ilat io n in p rem at u re in fan t s12.
Neo n at al seizu res are so m e o f t h e m o st freq u en t sig n s o f n eu ro lo g ical in vo lvem en t , an d m ay in t erfe-re w it h vit al fu n ct io n s, su ch as feed in g an d ven t ila-t io n13. Mo rt a lit y ra t es fo r n eo n a t a l seizu res h a ve
Table 2. M ot her-inf ant charact erist ics.
Co n t ro ls (N= 51) Neo n at al seizu res an d /o r PIVH (N= 17) p
m ean m ean
Mat ern al ag e (years) 28 26 0.816
Gest at io n al ag e (w eeks) 31.6 32 0.83
Birt h w eig h t (g ram s) 1254 1259 0.957
Table 3. Correlat ion bet w een neonat al seizures and PIVH.
Ch aract erist ic n (%)
Neo n at al seizu res an d PIVH 9 (13)
Neo n at al seizu res b u t n o PIVH 5 (7)
PIVH b u t n o seizu res 3 (5)
No n e 51 (75)
To t al 68 (100)*
*p , 7X10-6; PIVH, p eri- an d in t raven t ricu lar h em o rrh ag e.
Table 4. Neurodevelopment al examinat ion and neonat al seizures and/or PIVH.
Ch aract erist ic Co n t ro ls Neo n at al seizu res RR CI p
an d /o r PIVH
Mu scle t o n e ap p ro p riat e fo r CA 35/48 4/15 0.37 0.16-0.86 0.003* St ren g t h ap p ro p riat e fo r CA 41/41 7/9 0.78 0.55-1.1 0.029
Reflexes ap p ro p riat e fo r CA 43/44 8/13 0.63 0.41-0.97 0.001*
Mo ro reflex 2/51 3/17 4.5 0.82-24.7 0.09
Head co n t ro l 44/44 6/8 0.75 0.5-1.12 0.021*
Sit t in g w it h su p p o rt 45/45 12/12 - 1
Grasp in g 1 o b ject in each h an d 30/45 10/11 1.36 1.03-1.8 0.15
Arq Neu ro p siq u iat r 2003;61(4) 905
d ecreased o ver t h e last d ecad es, b u t t h ere h as n o t been great im provem ent in relation to sequelae, such as m en t al ret ard at io n an d m o t o r d eficit . Seizu res o ccu r in ab o u t 10% o f all p at ien t s w it h in t racran ial h em o rrh ag e, b u t t h is rat e is h ig h er fo r p rem at u re in fan t s. Ou r st u d y revealed a 75% freq u en cy rat e in cases of intracranial hem orrhag e, and d em onstrated that p rem ature p atients are m ore suscep tib le to the-se even t s. Periven t ricu lar an d ven t ricu lar h em o rrh a-ges are associated with prem aturity, and their severity is in versely p ro p o rt io n al t o g est at io n al ag e14-17.
Hyp ert o n ia is exp ect ed t o d ecrease at 6 m o n t h s’ o f ag e b ecau se o f t h e b eg in n in g o f co rt ical co n t ro l o ver reflex act ivit y. Ap p en d icu lar h yp ert o n ia an d h y-p erreflexia m ay b e strong evid ence that cortical con-t ro l is n o con-t efficien con-t yecon-t13. At t h e sam e ag e an d fo llo
-w in g t h e cra n io ca u d a l seq u en ce o f n eu ro lo g ica l developm ent - the infant is expected to hold the head up , sit w ithout sup p ort, and g rasp ob jects w ith b oth hand s. Prim itive reflexes of the new b orn infant, such as t h e Mo ro reflex, sh o u ld also d isap p ear. Ou r st u d y analyzed these key elem ents to m easure the d am ag e cau sed b y n eo n at al seizu res an d in t racran ial h em o r-rh ag e. Ab o u t 30 t o 60% o f all p rem at u re in fan t s w it h severe in t racran ial h em o rrh ag e an d ven t ricu lo -m eg aly h ad d evelo p -m en t al seq u elae, su ch as cere-b ral p alsy18-19. Even w h en n o t acco m p an ied b y h
e-m o rrh a g e, ven t ricu lo e-m eg a ly is a sso cia t ed w it h a h ig h er risk fo r d elay in n eu ro lo g ical d evelo p m en t20.
Rep o rt s in lit erat u re h ave am p ly d em o n st rat ed t h at t h ere is a cau se an d effect relat io n sh ip b et w een in -t racran ial h em o rrh ag e an d seizu res in -t h e n eo n a-t al p erio d . Th erefo re, t h e n eu ro lo g ical p ro g n o sis m ay be better when these two events are not associated21.
Abnorm al results in the neonatal neurological exa-m in at io n are asso ciat ed w it h iexa-m p aired n eu ro lo g ical d evelo p m en t in p rem at u re in fan t s21-23. An ab n o rm al
resu lt d o es n o t alw ays p red ict d evelo p m en t al p ro -b lem s, -b u t t h is exam in at io n is a g o o d t o o l t o screen this hig h-risk g roup of p atients w ho have to b e care-fu lly o b served an d , if n ecessary, t reat ed . Persist en t tone and reflex ab norm alities in infancy m ay sug g est cereb ral p alsy, m o t o r d ysfu n ct io n , learn in g o r b eh a-vioral p rob lem s24. Our p atients’ neurod evelop m ental
exam in at io n at 6 m o n t h s’ co rrect ed ag e revealed in ap p ro p riat e m u scle t o n e, st ren g t h an d reflexes, as w ell as d elay in h ead co n t ro l, fo r t h o se p at ien t s t h at h ad n eo n at al in t racran ial h em o rrh ag e an d /o r seizu -res. Early neurological assessm ent is extrem ely im por-t an por-t b ecau se ipor-t s resu lpor-t s h elp m akin g d ecisio n s ab o u por-t reh ab ilit at io n an d p reven t io n o f d iso rd ers t h at t yp i-cally affect t h ese p at ien t s.
The association between m ultiparity and intracra-nial hem orrhage m ay be explained by the shorter ex-pulsion stage of babies born to m ultiparous m others.
Conclusions - We co m p a re d t h e re su lt s o f neurod evelop m ental exam ination for tw o g roup s of p re m a t u re in fa n t s a t 6 m o n t h s’ co rre ct e d a g e . Fu rt h er st u d ies w it h t h ese sam e p rem at u re in fan t s are u n d er w ay, an d t h ese p at ien t s w ill b e fo llo w ed u p u n t il t h ey reach sch o o l ag e.
REFERENCES
1. Ehrenkranz RA , Yo unes N, Lemo ns JA . Lo ngitudinal gro w th o f hospitalized very low birth weight infants. Pediatrics 1999;104:280-289. 2. Fletcher JM, Landry SH, Bohan TP, et al. Effects of intraventricular hemorrhage and hydrocephalus on the long term neurobehavioral development of preterm very low birthweight infant. Dev Med Child Neurol 1997;39:5966-6016.
3. Rotta NT, Winckler MIB, Ohlweiler L, et al. Seguimento neurológico
de 90 recém-nascido de alto risco. Revista HCPA 1988;8:162-167. 4. Gherpelli JLD. Avaliação neurológica do recém-nascido prematuro. In
Diament A, Cypel, S (eds). Neurologia infantil, 3.Ed. Ateneu: São Pau-lo, 1996:22-23.
5. Pedroso FS, Rotta NT. From the foot-mouth reflex to the hand- mouth reflex: a continuum of responses to appendicular compression. Arq Neuropsiquiatr 1997;55:186-192.
6. Riesgo RS, Rotta AT, Rotta NT. Shock of birth. Arq Neuropsiquiartr 1996;54:361-368.
7. Sell EJ. Outcome of very very low birthweight infants. The tiny baby. Clin Perinatol 1986;13:451-460.
8. Washington Report: Neonatal intensive care for low birthweight infants: Costs and effectiveness. Health Technology Case Study 38. Washing-ton, DC: Office of Technology Assessment 1987:7-15.
9. Co llabo rativ e Euro p ean M ulticenter Stud y Gro up . Surfactant replacement therapy for severe neonatal respiratory distress syndrome: An international randomized clinical trial. Pediatrics 1988;82:683-691. 10. Lang MJ, Hall RT, Reddy NS. A controlled trial of human surfactant replacement therapy for severe respiratory distress syndrome in very low birth weight infants. J Pediatr 1990;116:295-300.
11. Whitfield MF, Johannsen DE. Major disabilities in surviving children of birthweight 800 grams or less in British Columbia: 1974 - 1988 births. Pediatr Res 1991;29:1609-1612.
12. Bellig LL. A w indo w o n the neo nate’ s brain. Neo natal Netw o rk 1989;7:13-20.
13. Vo lpe, JJ. Neo natal Seizures. In Neuro lo gy o f the New bo rn. 3th.
Philadelphia, W. B. Saunders 1995;172-207.
14. Hill A, Volpe JJ Intracraneal hemorrhage. In Avery GB, Fletcher MA, Macdonald (EDS). Neonatology-pathofisiology and management of the newborn. 4.Ed. Philadelphia: J.B. Lippincott. 1994:1127-1135. 15. Hack M, Wilson-Costello D, Friedman H, Taylor GH, Schluchter M,
Fanaro ff A A . Neuro develo pment and predicto rs o f o utco mes o f children with birth weights of less than 1000g: 1992-1995. Arch Pediatr Adolesc Med 2000;154:725-731.
16. Volpe JJ. Intracranial hemorrhage: germinal matrix-intraventricular haemorrhage of the premature infant. In Neurology of the newborn. 4th. Philadelphia, Saunders 2001;428-493.
17. Vohr BR, Wright LL, Dusik A M, et al. Neurodevelopmental and functional outcomes of extremely low birth weight infants the National Institute o f Child Health and Human Develo pment. Ped iatrics 2000;105:1216-1226.
18. Papile LA , Munsick-Bruno G, Schaefer A . Relationship of cerebral intraventricular hemorrhage and early chidhood neurologic handicaps. J Pediatr 1983;103:273-277.
19. Shankaran S, Koepke T, Woldt E, et al. Outcome after posthemorragic ventriculo megaly in co mpariso n w ith mild hemo rrhage w itho ut ventriculomegaly. J Pediatr 1989;114:109-114.
20. Stewart AL, Thorburn RJ, Hope PL, et al. Ultrasound appearance of the brain in very preterm infants and neuro-developmental outcome at 18 months of age. Arch Dis Child 1983;58:598-604.
21. Allen MC, Capute AJ. Neonatal neurodevelopmental examination as a predictor of neuromotor outcome in premature infants. Pediatrics 1989;83:498-506.
22. Brown JK, Purvis RJ, Forfar JO, et al. Neurological aspects of perinatal asphyxia. Dev Med Child Neurol 1974;16:567-580.
23. Ishikaw a T, Ogaw a Y, Kanayama M, et al. Long-term prognosis of asphyxiated full-term neonates with CNS complications. Brain Dev 1987;9:48-53.