w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Factors
associated
with
abdominal
pain
in
patients
submitted
to
colonoscopy
夽
Amanda
Colpani
Bellei
∗,
Daniela
Ghizoni
Dacoregio,
Flávio
Bianchini,
Jaime
César
Gelosa
Souza,
João
Martiniano
Lamim
Bello,
Kaiser
de
Souza
Kock
UniversidadedoSuldeSantaCatarina(UNISUL),DepartamentodeMedicina,Tubarão,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received5July2017 Accepted26August2017
Availableonline23September2017
Keywords: Colonoscopy Conscioussedation Abdominalpain Sedation
a
b
s
t
r
a
c
t
Objective:Thestudyevaluatedfactorsassociatedwithabdominalpainduringcolonoscopy. Methods:Thiswasacross-sectionalobservationalstudythatevaluatedpatientswho under-wentcolonoscopy between February 2014 and February 2015. Physical characteristics, surgicalhistoryandpreviouscolonoscopies,indicationandcurrentexaminationconditions, fentanylandmidazolamdose,andpainlevelwereanalyzed.Significanceleveladopted: p<0.05.Chi-squaredtestwasusedforassociationofcategoricalvariables,Student’st-test wasappliedforcomparisonofmeans,andSpearman’scoefficientwasusedforcorrelation. Results:Atotalof566womenand391menwithmeanageof54.81yearsandmeanBMIof 27,064wereevaluated.Ofthetotal,29(3.0%)hadmildpain,42(4.4%)hadmoderatepain, and18(1.9%)hadseverepain.Womenwerelesstolerant(p=0.011)andhadlongercecal intubationtimes(p=0.001).Meandurationofcolonoscopyandmeandoseofmidazolam werehigherinpatientswithpain(p=0.001),(p<0.001*).Amongthe39 patientswithan incompleteexamination,8reportedpain(p=0.049).
Conclusion:Femalegenderandprolongedintubationtimeweresignificantlyassociatedwith abdominalpainduringcolonoscopy.Patientswithdiscomforthadahigherfailurerateon theexam.Additionaldosesofmidazolamgiventopatientswithpainwerenoteffective.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileirade Coloproctologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Fatores
associados
à
dor
abdominal
em
pacientes
submetidos
à
colonoscopia
Palavras-chave: Colonoscopia Sedac¸ãoconsciente
r
e
s
u
m
o
Objetivo:Oestudoavalioufatoresassociadosàdorabdominalduranteacolonoscopia. Métodos:Estudoobservacionaltransversal,queavalioupacientesquerealizaram colono-scopia entreFevereiro de 2014 e Fevereiro de 2015. Analisou-se características físicas,
夽
StudyconductedattheClínicaPró-Vida,Servic¸odeEndoscopiaeColonoscopia,Tubarão,SC,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](A.C.Bellei).
https://doi.org/10.1016/j.jcol.2017.08.003
Dorabdominal Sedac¸ão
históricocirúrgicoecolonoscopiasprévias,indicac¸ãoecondic¸õesdoexameatual,dosede fentanilemidazolameníveldedor.Níveldesignificânciaadotado:p<0,05.Utilizou-seteste Qui-quadradoparaassociac¸ãodevariáveiscategóricas,testetdeStudentparacomparac¸ão demédiasecoeficientedeSpearmanparacorrelac¸ão.
Resultados: Avaliou-se566mulherese391homens,commédiadeidadede54,81anose IMCmédiode 27,064.Dototal,29 (3,0%)tiveramdorleve,42 (4,4%)dor moderadae18 (1,9%)dorintensa.Asmulheresforammenostolerantes(p=0,011)etiverammaiortempo deintubac¸ãocecal(p=0,001).Adurac¸ãomédiadacolonoscopiaedosemédiade midazo-lamadministradaforammaioresnospacientescomdor(p=0,001),(p<0,001*).Entreos39 pacientescomexameincompleto,8relataramdor(p=0,049).
Conclusão: Gênerofemininoetempodeintubac¸ãoprolongadotiveramassociac¸ão signi-ficativacomdorabdominalduranteacolonoscopia.Pacientescomdesconfortotiveram umataxamaiordeinsucessonoexame.Dosesadicionaisdemidazolamadministradasnos pacientescomdornãoforamefetivas.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade Coloproctologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Colonoscopyisthemostaccurateexaminationforthe diagno-sisandfollow-upofcolorectaldiseasessincethisprocedure allowsacompleteevaluationofmucosaeofthewholelarge intestineand distal terminalileum.1 Inorder toobtain an
effective,goodqualityexamination,whatisneededistocount onanexperiencedendoscopist,anadequatepreparationof thecolon,andpatientcooperationundereffectiveanalgesia andsedation.2–4
Inordertoperformtheendoscopicprocedure,thepatient issubmittedtoamoderatesedationofthe“conscious”type, inwhich the condition ofa responseto verbal and tactile stimulipersists,andthecardiovascularandrespiratory sys-temsremainwiththeirspontaneousfunctions.5,6Amongthe
characteristics of sedation during colonoscopy, those with animmediateeffectstandout;sedationshouldlastjustthe time of examination and the procedure should provide a rapidrecoveryofthepatient,causinglittleornosideeffect.6
In view of these premises, benzodiazepine agents (which reduce anxiety and sedate the patient) are routinely used in association with opioids (responsible for analgesia dur-ingtheexamination).7Inaddition,conscioussedation with
benzodiazepinesandopioidsisalower-costalternativewhen comparedtointravenoussedationperformedwithpropofol, ahypnoticagentwidelyusedtoperformendoscopic proce-dures.Thisdrugpromotesdeepsedationandbringsagreater riskofsideeffects,forexample,respiratorydepression.8
Several factors are related to the greater probability of occurrenceofpainduringcolonoscopy;suchfactorsmaybe intrinsictothepatientormaybeofanexternalorder.Some ofthesefactorsare:veryyoungoradvancedage,female gen-der,lowbodymassindex(BMI),previousabdominalorpelvic surgery,poorcolonic preparation,insufficientsedation,the formationofloops,and highpressure ofthe airinflated to promotecolonicdistension.9
Theaimofthisstudywastoidentifyfactorsrelatedtothe patientandtotheexaminationthatcouldbeassociatedwith theoccurrenceofabdominalpainduringcolonoscopy,aswell
asanevaluationofthelevelofpainpresentedbythepatients andtheefficacyofconscioussedation.
Methods
The present study,of the observationaltype witha cross-sectional design, was approved by the Research Ethics CommitteeoftheUniversidadedoSuldeSantaCatarinaunder opinion875.131,CAAE36089414.5.0000.5369,accordingtothe normsoftheConselhoNacionaldeSaúdeforresearch involv-inghumanbeings,resolution466/2012.
Patients who underwent elective colonoscopy between February 2014 and February 2015 by the Endoscopy and ColonoscopyServiceofaprivatepolyclinicfromacityinthe SouthofBrazil,whichattendsprivatehealthplansand con-sultations,wereevaluated.ThestudystartedinFebruary2015 andendedinNovember2015.
All patients who were attended on an outpatientbasis andwhounderwentcolonoscopywereincludedinthisstudy. Patients who needed an emergency examination or who underwentdeepsedationwereexcludedfromthestudy.
Allpatientsreceivedano-residuedietthedaybeforethe test,followedbya12-hourfast.Onthedayofcolonoscopy, colonicpreparationwasperformedwithabalancedsolution ofpolyethyleneglycol,1000mLPO,4hbeforethetest,in com-binationwiththeantiemeticagentondansetron,8mgPO.
MILD MODERATE SEVERE
VISUAL ANALOG SCALE (VAS)
0 1 2 3 4 5 6 7 8 9 10
Fig.1–VisualAnalogScale(VAS)forpain.
ofexperience.EndoscopesPentax® EPK1000serieswereused forthecolonoscopicprocedures.
Thefollowingdatawerecollectedbycompletinga Medi-calRecordsCard:age,gender,weight,height,BMI,indication ofcolonoscopy(diagnosticortherapeutic)andclinical indi-cation (which was the disease to be investigated and/or treated),theoccurrenceofapreviouspelvicsurgeryand/or prior colonoscopy, duration of examination (timed by the colonoscopydevice itself),anappropriate(withoutstool,or withaminimum ofsolidstoolsand presentingonlysmall amountsofclearliquidrequiringsuction)orinadequate (pres-enceofsolidorsemi-solidintestinalcontentsnoteffectively eliminated) preparation of the colon,10 a complete or an
incompleteexamination,theadministereddoseoffentanyl andmidazolam,andthedegreeofabdominalpaininformed (0:nopain,1–2:mildpain[welltolerated],3–7:moderatepain [bearable],or8–10:severepain[theworstpainpossible]),11as
measuredbytheVisualAnalogScale(VAS)forpain12(Fig.1).
VASwasappliedaftertheprocedurewasperformed,butonly whenthepatientshowedacompleterecoveryof conscious-ness.Thepatientwasthendischarged.
Forthisstudy,theFreeandInformedConsentTermwasnot obtained;onlyoneJustificationfornotusingthisdocument incasesofresearchcarriedoutbasedontheuseofclinical recordswasperformed.
ThedatawererecordedinaspreadsheetoftheEpiInfo® Program version 3.5.4and analyzedin the programSPSS® version20.0.Weadoptedasignificancelevellowerthan5% (p<0.05).Thevariablesweredescribedusingmean/standard deviationfornumericalvariables,andusingrelativefrequency forcategoricalvariables.Fortheassociationofcategorical vari-ablestheChi-squaredtestwasused;forthecomparisonof meanstheStudent’st-testwasused;andforthecorrelation ofvariablestheSpearmanCorrelationCoefficientwasapplied, withRho()between−1and+1.
Results
Ofthetotalof957patientsevaluated,566werewomen(59.1%) and391(40.9%)weremen,withameanageof54.81(20–87) years.ThemeanBMIforthesepatientswas27,064(14.5–45.4).
Table1liststhecharacteristicsofpatientsintermsof
gen-der, age, BMI, number (%) ofpatients who had previously undergoneacolonoscopy,numberofthosewhohadan appro-priatecolonpreparation,andthenumberofpatientswhohad acompleteexamination.
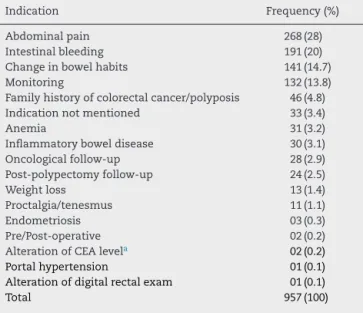
Table2liststhe indicationspresentedbythosepatients
seenforthecolonoscopy.
Table1–Generalaspectsofpatientsundergoing colonoscopyunderconscioussedation.
Characteristics Number(%)
Gender
Female 566(59.1)
Male 391(40.9)
Age(mean)
<54.81years 409(42.7)
≥54.81years 548(57.3)
BMI
<18.5 12(1.3)
≥18.5<25.0 319(33.3)
≥25.0<30.0 395(41.3)
≥30.0 231(24.1)
Previouscolonoscopy
Yes 216(22.6)
No 741(77.4)
Preparationofcolon
Suitable 941(98.3)
Inapporpriate 16(1.7)
Completeexamination
Yes 918(95.9)
No 39(4.1)
Table2–Indicationsforperformingcolonoscopyunder conscioussedation.
Indication Frequency(%)
Abdominalpain 268(28)
Intestinalbleeding 191(20) Changeinbowelhabits 141(14.7)
Monitoring 132(13.8)
Familyhistoryofcolorectalcancer/polyposis 46(4.8) Indicationnotmentioned 33(3.4)
Anemia 31(3.2)
Inflammatoryboweldisease 30(3.1) Oncologicalfollow-up 28(2.9) Post-polypectomyfollow-up 24(2.5)
Weightloss 13(1.4)
Proctalgia/tenesmus 11(1.1)
Endometriosis 03(0.3)
Pre/Post-operative 02(0.2) AlterationofCEAlevela 02(0.2)
Portalhypertension 01(0.1) Alterationofdigitalrectalexam 01(0.1) Total 957(100)
Table3–Abdominalpainlevelaccordingtothegender ofthepatientundergoingcolonoscopyunderconscious sedation.
Mildpain Moderatepain Intensepain p-Value
Gender
Female 21(3.7%) 31(5.5%) 15(2.6%) 0.011 Male 08(2%) 11(2.8%) 03(0.8%)
Amongthe957patients,868(90.7%)didnotpresent abdom-inalpain,while89(9.3%)reportedsomelevelofpainduringthe examination:29(3.0%)classifiedtheirpainasmild,42(4.4%) asmoderate,and18(1.9%)assevere.Themeanageofpatients withoutabdominalcomplaintswas54.99years,andthemean numberofpatientswithdiscomfortwas53.06years(p=0.216).
ThemeanBMIofpatientswithoutandwithpainwas27,025
and27,450,respectively(p=0.380).
Regarding gender, men presented greater tolerance to
colonoscopyversuswomen.Ofthe391malepatients,22(5.6%)
had some abdominal complaints regarding the procedure.
Amongthe566womensubmittedtocolonoscopy,painwas
recordedby67(11.8%)patients(p=0.011).Table3presentsthe abdominalpainlevels,accordingtogender.
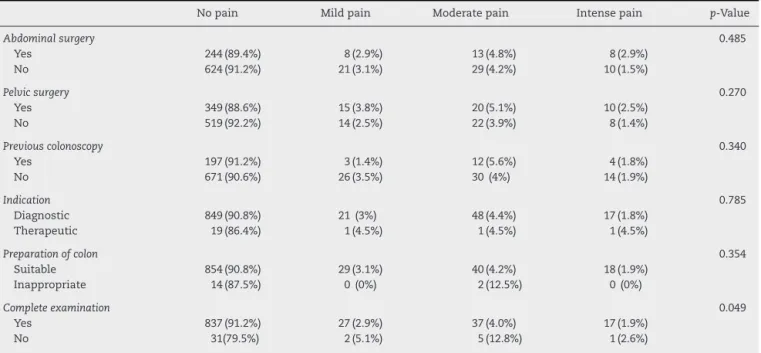
Among the 273 patients with some type of abdominal surgery,29(10.6%)reportedpainand60(8.8%)ofthe684 indi-vidualswhohadneverundergoneabdominalsurgerysuffered discomfortduringtheexamination(p=0.485).Amongthe394 individualswithapreviouspelvicsurgery,45(11.4%)showed intolerancetocolonoscopy.Ofthe563patientswithoutprior pelvicsurgery,44(7.8%)showedabdominalpain(p=0.270).
Regarding a previous colonoscopy, of the total of 216 patientswhohadpreviouslyperformedanexamination,19 (8.8%)showedsomeintoleranceduringtheirlastcolonoscopy.
Amongpatientswhounderwentcolonoscopyforthefirsttime, 70(9.4%)complainedofpain(p=0.340).
Ofthetotalof935patientsdiagnosedforcolonoscopy,86 (9.2%)reportedsomelevelofpain.Amongthe22patientswith atherapeuticindication,3(13.5%)reportedpain.
Ofthe 941individualswithan appropriatecolon prepa-ration, 87 (9.2%) reported some complaint during the examination.Ontheotherhand,amongthe16patientswho didnothaveagoodpreparationofthegastrointestinaltract, only2(12.5%)reportedpain(p=0.354).
Ofthetotalnumberofpatientsanalyzed,918underwenta completeexamination,81(8.8%)ofwhomwereintolerantto colonoscopy.Amongthe39patientswhocouldnotcomplete theexamination,8reporteddiscomfort(p=0.049).
Table4describesthepainlevelsfound,accordingtothe
variablesevaluatedbythestudy.
The mean duration ofcolonoscopy in patients without abdominalcomplaintswas10.57minandthemeannumber ofpatientswithabdominalpainwas12.26min(p=0.001).We observedthatthelongertheinsertiontimeofthecolonoscopy device (which corresponds to the time elapsed from the introduction of the device toits arrival inthe cecum), the higherthepatients’painlevel(p=0.036).Inwomenthe intu-bation time was longer, with a mean time of 11.18min, while in men the mean intubation time was 10.38min (p=0.001).
Regardingmedications,170patientsreceivedextradoses of midazolam, in accordance with the abdominal com-plaintsreportedduringtheexamination.Themeandoseof midazolam administered to patients with discomfort was 5.67mg,alevelhigherthanthemeandoseadministeredto patientswithoutcomplaints,whichwas5.16mg(p<0.001*). The mean dose of fentanyl given both in patients who reportednopainandinthosewhoreportedpainwas0.05mg (p=0.716).
Table4–Abdominalpainlevelofpatientsundergoingcolonoscopyunderconscioussedationaccordingtothestudy variablesevaluated.
Nopain Mildpain Moderatepain Intensepain p-Value
Abdominalsurgery 0.485
Yes 244(89.4%) 8(2.9%) 13(4.8%) 8(2.9%)
No 624(91.2%) 21(3.1%) 29(4.2%) 10(1.5%)
Pelvicsurgery 0.270
Yes 349(88.6%) 15(3.8%) 20(5.1%) 10(2.5%)
No 519(92.2%) 14(2.5%) 22(3.9%) 8(1.4%)
Previouscolonoscopy 0.340
Yes 197(91.2%) 3(1.4%) 12(5.6%) 4(1.8%)
No 671(90.6%) 26(3.5%) 30(4%) 14(1.9%)
Indication 0.785
Diagnostic 849(90.8%) 21(3%) 48(4.4%) 17(1.8%)
Therapeutic 19(86.4%) 1(4.5%) 1(4.5%) 1(4.5%)
Preparationofcolon 0.354
Suitable 854(90.8%) 29(3.1%) 40(4.2%) 18(1.9%)
Inappropriate 14(87.5%) 0(0%) 2(12.5%) 0(0%)
Completeexamination 0.049
Yes 837(91.2%) 27(2.9%) 37(4.0%) 17(1.9%)
Discussion
Colonoscopyisthemostaccuratediagnostictoolforcolorectal diseases;however,inaconsiderablenumberofsituationsit canbeanuncomfortableprocedureforthepatient,andthisis oneofthemaincausesofresistancetothisprocedure.
Manyofthefactorsthatcontributetoabdominal discom-fortduringcolonoscopyhavealreadybeenidentifiedandcan bemanagedinordertoincreasethepatient’stolerancetothe examination.Appropriateguidelinesontheprocedure,a cor-rectpreparationofthecolon,andagoodsedation/analgesia forthereductionofanxiety,aswellastheadoptionof estab-lishedtechniquesduringtheexamination(suchaschanging thepatient’spositionandtheuseofmanualabdominal com-pression)arekeymeasuresforobtainingalessuncomfortable colonoscopy.However,somefactorswidelydescribedinthe literatureareinherenttothepatientandcannotbemodified, suchasanatomy,gender,age,BMI,andpreviousclinicaland surgicalhistory.9
There iscurrently no standardizedmethod for evaluat-ingabdominalpainduringcolonoscopy.Inthepresentstudy, wechose touse VAS12 because this isa procedure that is
easytoapplyandunderstand,especiallyafterrecoveryfrom sedation.VASrangesfromzeroto10,wherezeromeansno pain,1–2equalsmildpain,3–7suggestsmoderatepain,and valuesbetween8and10correspondtoseverepain.This eval-uationisalsoaccompaniedbyvisualresources, withfacial expressionsthatillustratepainintensity.However,VASisa one-dimensional method, whichevaluates the intensity of painonlyatagivenmoment,withouttakingintoaccountany otheraspect.12
The present study showed that, despite all the factors thatmaycontributetoabdominalpainduringcolonoscopy, 868(90.7%)ofthose957patientstreatedtoleratedverywell the examination, without presenting any abdominal com-plaints.Regardingthosepatientswhoreporteddiscomfort,it wasobservedthatwomenshowedhigherlevelsofabdominal pain,withalongertimeofintubationofthecolon.Regarding the technique, prolonged intubationtimes are also associ-atedwithhigherlevelsofpainduringcolonoscopy.Itwasalso observedthatinpatientswhoreportedabdominalcomplaints, thetotaldoseofmidazolamadministeredwasgreaterthan thedoseadministeredinpatientswhodidnotcomplain.The percentageofincompleteexamswasalsohigherinpatients whoreportedpain.
Inthisstudy,theassociationbetweenfemalegenderand abdominalpainwaspositively significant.Ofthe 67(11.8%) womenwhoreportedpain,21describedtheepisodeasmild, 31asmoderate,and15assevere.Inanumberofpublished studies,13–15 female gender has already been identified as
anindependentriskfactorassociatedwithabdominalpain duringa colonoscopyprocedure. In addition tohigher lev-elsofdiscomfort,generallyinwomentheintubationtimes arelonger and thepercentageofincompleteexams isalso higher. This is because the female colon, especially the transversecolon, ismoreelongated;besides,its abdominal musculatureisweaker.Thissituationisapredisposingfactor for the formation of loops in the endoscope, which ham-perstheexamination.16,17Althoughthisrelationshipwasnot
detected in the present study, the female patients’ surgi-calhistory showedastrong relationshipwiththepresence of abdominal pain in previous studies.18,19 The procedure
ofcolonoscopyisalsohamperedbytheformationofbands and adhesions,whicharerelativelycommoncomplications ofabdominopelvic surgeries.In addition,the perceptionof paindiffersbetweengenders.Onestudy20demonstratedthat
womenhaveadifferentvisceralpainmemoryversusthatof men.Afterthepatientswerestimulatedbyarectaldistension toactivatevisceralpain,womendemonstratedamoreintense neuralresponsetopain,whichwouldexplainthemoresevere abdominalpaininfemalesubjects.
Theinsertiontimeofthecolonoscopewasautomatically timedbythedeviceused.Theevaluatedservicehasadopted this practicefor morethan 10years,and this variable has been routinely recorded in the patient’ medical record, in ordertoobtainabettercontroloftheintubationtime,since the prolongedinsertiontime ofthe devicealsocontributes toabdominaldiscomfort.17Thecompleteexaminationbegins
with theinsertion ofthedevice throughthe anus,passing through the rectum, sigmoid,descending colon, transverse colon,andascendingcolonuntilitreachesthececum.2Inthe
presentstudy,themeantimeofintubationofpatientswho reportedpainwas12.26min,i.e.1.29minlongerthanthemean intubationtimeforpatientswithoutabdominalcomplaints. Thepainlevelofthepatientsanalyzedwasdirectly propor-tionaltothetimeofintubationofthecolon:thelongerthe intubationtime,themoreseverethepainreported.Inthose womenwhoparticipatedinthepresentstudy,intubationtime waslonger(mean:11.18min),whileinmenthemean intuba-tiontimewas10.38min.Thisresultissimilartothatofastudy conductedinXijing,China,21inwhichtechnicaldifficulty,
pro-longedintubationtime,andconsequentlythepainlevelwere higherinfemalepatients.
A colonoscopycould be performed without any typeof analgesia;but becausethis isaninvasiveexaminationand alsobecauseoftheanxietyandfearofpainshownbymany patients,mostEndoscopyServicesusesomekindofconscious sedationthroughtheassociationofbenzodiazepinesand opi-oids. Midazolam isa benzodiazepine agentthat decreases anxietyandcausessedationofthepatient;ontheotherhand, fentanylisashort-actingopioidagent,responsiblefor anal-gesiaduringtheexamination.Theactionofthesetwodrugs beginsabout2minaftertheirintravenousadministrationand thepatient’srecoveryisrapid,7withduerespecttothe
pre-ceptsofconscioussedation.Weobservedthat170patients received extra doses of midazolam in addition to the ini-tial doseand thatthe mean doseadministered inpatients who experienced pain was significantly higher versus the doseadministeredinpatientswithoutcomplaints.Whilethe groupwhoreportedabdominalpainreceivedameandoseof midazolamof5.67mg,patientswithoutcomplaintsreceived ameandoseof5.16mg.Inmostofthesepatients,thetypeof paindescribedwasofthemoderatetype,whichshowsthat, evenwiththerecommendedsedationandanalgesia,the med-icationisoftenineffective.Astudy14alsodemonstratedthe
psychologicalprofileofthepatientshouldbepreviously inves-tigated.Inpatientswithariskfactorfordiscomfortduring colonoscopy,forexample,femalegender, anxiouspatients, and patients with low BMI, the sedation could be more intense.
Aslimitationsofthepresentstudy,wecanhighlightthe absenceofevaluationofthepatient’s socialconditionsand theiranxiouscomponentandcomorbidities,besidesthe med-ications used bythe study participants – factors that may influencetheperceptionofpain,increasingordecreasingits threshold.Themethodchosenfortheevaluationofabdominal painmeasuresonlyitsintensity,withouttakingintoaccount othercharacteristics.Anotherlimitationofthestudyislinked tothefactthatcolonoscopieswereperformedbymorethan oneprofessional;therefore,differencesintheprocedureand inthedescriptionofdatainthepatients’medicalrecordmay havebeengenerated.ThetimeofapplicationofVAS,12even
afterthefullrecoveryofconsciousnessbythepatient,may havecausedamemorybiasinsomeparticipants,considering thatoneofthepossiblesideeffectsofmidazolamisamnesia.7
Becausethisisacross-sectionalstudy,it isnotpossibleto determinethecausalityoftheresults.
Conclusion
Colonoscopywasawell-toleratedprocedurewhenperformed underconscious sedation,because despitethe several fac-torsthatcontributetotheappearanceofabdominalpain,in the current study the number of patients with discomfort was low: only 9.3% of the total of 957 individuals evalu-ated reported pain. Of the total number of patients with abdominalpainduringtheexamination,3.0%reportedmild pain,4.4%hadmoderatepain,andonly1.9%reportedsevere pain – data confirming that, despite being uncomfortable, colonoscopy is a well-tolerated examination. A significant associationbetweenfemalegenderandprolongedintubation timeversusabdominalpainduringcolonoscopywasfound, alsowithsignificancebetweenthesetwovariables.In rela-tiontosedationandanalgesiaofthepatients,itwaspossible toperceivethatthe associationoffentanylandmidazolam promoted an adequate effect; however, the administration ofsafe extradosesofmidazolaminpatients whoreported painduringtheexaminationwasnoteffectiveinimproving pain.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. RexDK,JohnsonDA,AndersonJC,SchoenfeldPS,BurkeCA,
InadomiJM.Americancollegeofgastroenterologyguidelines
forcolorectalcancerscreening2008.AmJGastroenterol.
2009;104:739–50.
2. MatosD,SaadSS,FernandesLC.Guiasdemedicina
ambulatorialehospitalarUNIFESP/escolapaulistade
medicinacoloproctologia.1aedic¸ãoBarueri(SP):Manole;
2004.
3.PolettiPB,GuardadoSM,BastosDA,MantelmacherM.
Endoscopicexamsinspecialpatients.In:ParadaAA,
CapellanesCA,VargasC,VencoFE,MansurGR,PaesIB,etal.,
editors.Therapeuticgastrointestinalendoscopy.Digestive
EndoscopyBrazilianSociety(SOBED).SãoPaulo(SC):
Tecmedd;2006.p.69–79.
4.FroehlichF,ThorensJ,SchwizerW,PreisigM,KohlerM,Hays
R,etal.Sedationandanalgesiaforcolonoscopy:patient
tolerance,pain,andcardiorespiratoryparameters.
GastrointestEndosc.1997;45:1–9.
5.AmericanSocietyofAnesthesiologistsTaskForceonSedation
andAnalgesiabyNon-Anesthesiologists.Practiceguidelines
forsedationandanalgesiabynon-anesthesiologists.
Anesthesiology.2002;96:1004–17.
6.TrainingCommittee.Americansocietyforgastrointestinal
endoscopy.Trainingguidelineforuseofpropofolin
gastrointestinalendoscopy.GastrointestEndosc.
2004;60:167–72.
7.AverbachM.Endoscopiadigestiva:diagnósticoetratamento.
2aedic¸ãoRiodeJaneiro(RJ):Revinter;2013.
8.dasNevesJF,AraújoMM,AraújoFP,FerreiraCM,DuarteFB,
PaceFH,etal.Sedac¸ãoparacolonoscopia:ensaioclínico
comparandopropofolefentanilassociadoounãoao
midazolam.RevBrasAnestesiol.2016;66:231–6.
9.ChurchJM.Completecolonoscopy:howoften?Andifnot,
whynot?AmJGastroenterol.1994;89:556–60.
10.RexDK,PetriniJL,BaronTH,ChakA,CohenJ,DealSE,etal.
Qualityindicatorsforcolonoscopy.AmJGastroenterol.
2006;101:873–85.
11.CalilAM,PimentaCAM.Intensidadedadoreadequac¸ãode
analgesia.RevLatino-amEnfermagem.2005;13:692–9.
12.MartinezJE,GrassiDC,MarquesLG.Análisedaaplicabilidade
detrêsinstrumentosdeavaliac¸ãodedoremdistintas
unidadesdeatendimento:ambulatório,enfermariae
urgência.RevBrasReumatol.2011;51:304–8.
13.RistikankareL,HartikainenJ,HeikkinenM,JanatuinenE,
JulkunenR.Theeffectsofgenderandageonthecolonoscopic
examination.JClinGastroenterol.2001;32:69–75.
14.ElphickDA,DonnellyMT,SmithKS,RileySA.Factors
associatedwithabdominaldiscomfortduringcolonoscopy:a
prospectiveanalysis.EurJGastroenterolHepatol.
2009;21:1076–82.
15.ParkDI,KimHJ,ParkJH,ChoYK,SohnCI,JeonWK,etal.
Factorsaffectingabdominalpainduringcolonoscopy.EurJ
GastroenterolHepatol.2007;19:695–9.
16.SaundersBP,FukomotoM,HaliganS,JoblingC,MoussaME,
BartramCI,etal.Whyiscolonoscopymoredifficultin
women?GastrointestEndosc.1996;43:124–6.
17.SadahiroS,OhmuraT,YamadaY,SaitoT,TakiY.Analysisof
lengthandsurfaceareaofeachsegmentofthelargeintestine
accordingtoage,sexandphysique.SurgRadiolAnat.
1992;14:251–7.
18.HullT,ChurchJM.Colonoscopy?Howdifficult,howpainful?
SurgEndosc.1994;8:784–7.
19.DysonJ,MasonJ,RutterM.Priorhysterectomyand
discomfortduringcolonoscopy:aretrospectivecohort
analysis.Endoscopy.2014;46:493–8.
20.BensonS,KattoorJ,KullmannJS,HofmannS,EnglerH,
ForstingM,etal.Towardsunderstandingsexdifferencesin
visceralpain:enhancedreactivationof
classically-conditionedfearinhealthywomen.Neurobiol
LearnMem.2014;109:113–21.
21.JiaH,WangL,LuoH,YaoS,WangX,ZhangL,etal.Difficult
colonoscopyscoreidentifiesthedifficultpatientsundergoing