www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Peritumoral
infiltrate
in
the
prognosis
of
epidermoid
carcinoma
of
the
oral
cavity
夽
,
夽夽
Vivian
Regina
Affonso
a,b,
José
Raphael
de
Moura
Campos
Montoro
a,
Luiz
Carlos
Conti
de
Freitas
b,
Fabiano
Pinto
Saggioro
c,d,
Luiz
de
Souza
e,
Rui
Celso
Martins
Mamede
b,∗aFaculdadedeMedicinadeMarília,Marília,SP,Brazil
bDepartmentofOphthalmology,Otorhinolaryngology,andHeadandNeckSurgery,HospitaldasClínicas,FaculdadedeMedicina
deRibeirãoPreto,UniversidadedeSãoPaulo(HCFMRP-USP),RibeirãoPreto,SP,Brazil
cDepartmentofPathology,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(FMRP-USP),RibeirãoPreto,SP,
Brazil
dPathologyService,HospitaldasClínicas,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(HCFMRP-USP),
RibeirãoPreto,SP,Brazil
eDepartmentofChildCareandPediatrics,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(FMRP-USP),
RibeirãoPreto,SP,Brazil
Received13June2014;accepted21September2014 Availableonline10June2015
KEYWORDS
Squamouscell carcinoma;
Mouthneoplasms;
Survival; Prognosis
Abstract
Introduction:Patientswithsquamouscellcarcinomaoftheoralcavitypresentdeficitsintheir cellularimmunitythatcontributetoneoplasticgrowth.Thus,theinflammatoryactivity,such astheimmunologicalresponsetothetumor,canbeusedasaprognosticfactor.
Objectives:Toevaluatethecorrelationbetweenperitumoralinflammationandclinical char-acteristicsofthepatients,survival,andthedisease-freeinterval.
Methods:The study sample consisted of a retrospective hospital-based cohort of patients undergoingsurgeryforresectionoforalcavitytumor.Theinflammatoryinfiltrateontheslides wasevaluatedsemi-quantitatively,andweredividedintominorandmajorinflammatory pro-cesses.
Results:Thisstudyincluded57tumorsamples,withinfiltrationoflymphocytes,plasmacells, andhistiocytes.Thelog-ranktestshowednosignificanceforthesurvivalcurvesandrecurrence ofthe‘‘minorinflammatory’’and‘‘majorinflammatory’’processes,withp=0.14andp=0.24,
夽
Pleasecitethisarticleas:AffonsoVR,MontoroJRMC,deFreitasLCC,SaggioroFP,deSouzaL,MamedeRCM.Peritumoralinfiltratein theprognosisofepidermoidcarcinomaoftheoralcavity.BrazJOtorhinolaryngol.2015;81:416---21.
夽夽
Institution:FaculdadedeMedicinadeRibeirãoPretodaUniversidadedeSãoPaulo(FMRB-USP),RibeirãoPreto,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](R.C.M.Mamede).
http://dx.doi.org/10.1016/j.bjorl.2014.09.010
1808-8694/©2015Associac¸ãoBrasileiradeOtorrinolaringologia eCirurgiaCérvico-Facial. PublishedbyElsevierEditoraLtda.All rights
respectively. Adirectassociationbetweenageandinflammation(p=0.04)was observed,as wellasanindirectassociationbetweenthedegreeoftumordifferentiationandinflammation (p=0.01).
Conclusion: Althoughassociatedwithhistologicaldifferentiation,theperitumoralinflammatory processcannotbeconsideredaprognosticfactorinsquamouscellcarcinomaoftheoralcavity, asitisnotrelatedtosurvivalanddisease-freeinterval.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Carcinomadecélulas escamosas;
Neoplasiasbucais; Sobrevida; Prognóstico
Infiltradoperitumoralnoprognósticodocarcinomaepidermoidedecavidadeoral
Resumo
Introduc¸ão: Pacientescomcarcinomaepidermoidedecavidadeoralmostramdéficitsemsua imunidade celular,que contribuempara ocrescimento neoplásico.Assim,aatividade infla-matória,comorespostaimunológicaaotumor,podeservircomofatorprognóstico.
Objetivos: Avaliaracorrelac¸ãoentreoprocessoinflamatórioperitumoralcomascaracterísticas clínicasdospacientes,comasobrevidaecomotempolivrededoenc¸a.
Método: Aamostradesteestudofoicompostaporumacoorteretrospectivadebasehospitalar com pacientessubmetidos àcirurgia para remoc¸ão de carcinomaepidermoidede cavidade oral.Oinfiltradoinflamatóriopresentenaslâminasfoiavaliadosemiquantitativamente,sendo divididoemprocessoinflamatório:menoremaior.
Resultados: Analisaram-se57 amostrastumorais, cominfiltradode linfócitos,plasmócitose histiócitos.Otestelog-ranknãomostrousignificânciaparaascurvasdesobrevidaederecidiva dosprocessos‘‘inflamatóriomenor’’e‘‘inflamatóriomaior’’,p=0,14ep=0,24, respectiva-mente.Observou-seassociac¸ãodiretadaidadecomoprocessoinflamatório(p=0,04),erelac¸ão indiretaentreograudediferenciac¸ãotumoraleoprocessoinflamatório(p=0,01).
Conclusão:Oprocessoinflamatórioperitumoral,emborarelacionadocomadiferenciac¸ão his-tológica,nãopodeserconsideradofatorprognósticodecarcinomaepidermoidedecavidade oral,poisnãoserelacionacomsobrevidaetempolivredadoenc¸a.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Despite treatment advances over the last20 years, squa-mouscellcarcinomaoftheoralcavity(SCCOC)continuesto have survivalrates at fiveyearsof 45---50%,1---3 mainlydue
toitsheterogeneousbehavior.4Thisfacthasledtoseveral
studies aimingto detect biologicaland molecular charac-teristicsthatmayindicateprognosisandtreatmentofthese tumors; most of them relate to histopathological staging ofthesurgicalspecimenanddonothavedirectimpacton clinicalpractice.5Currently,itisalsoknownthatthe
pres-enceofneckmetastasisandsurgicalmargininvolvementare prognosticfactorsforSCCOC.6,7
Innate immunity is the first reaction of the host to an offending agent.Adaptive immunity is a delayed type of immunitythat leaves immunologicalmemory, with the participation of B lymphocytes (humoral immunity) and cytotoxic T lymphocyte (cellular immunity). According to Abbas et al.8 the main anti-tumor defense mechanism is
the death of neoplastic cells by CD8+ T or cytotoxic T lymphocytes. However, individuals with SCCOC have cel-lularimmunity deficits, includingalterations in monocyte chemotaxis and defects in the interaction between the monocytes that have antigens and lymphocytes. These
defects contribute to neoplastic growth. According to Whiteside9 the same mechanisms used for immunological
escape in human malignancies may explain discrepancies betweenfailuresandsuccessesinimmunotherapy.
Inflammatory activity, such as immunological response tothe tumor, could be usedas a prognosticfactor, since the lower the inflammatory infiltrate, the greater the riskof regionalor distantmetastasis.10---12 However,Vieira
etal.7 observedacorrelation betweenahigherdegree of
malignancyandhigherinflammatoryintensity,suggestinga positive association between the intensity of the inflam-matoryresponseandthe degreeof tumor differentiation, withoutnecessarilyinfluencingpatientprognosis.
Therefore,thisstudyaimedtoevaluatethecorrelation betweentheperitumoralinflammatoryprocessandclinical characteristicsofpatients withSCCOC,aswellassurvival anddisease-freeinterval.
Methods
surgicalspecimenswerepart.Datarelatedtothe indepen-dent variablesthat couldbe associatedto thesurvival of cancerpatients, suchassociodemographic variables (gen-der,age,smokingstatus,andalcoholconsumption),clinical variables (primarysubsite), clinical staging(TNM, clinical stage),andhistologicalstaging(differentiation, angiolym-phatic invasion, and perineural invasion) were obtained throughmedicalfilereview.
Excluded werepatients whodidnot have tumor tissue samplesstored,aswellasthosewithasurgicalmargin com-promisedbythetumor atthehistopathologicalanalysisof surgicalspecimens,patientslosttopost-surgicalfollow-up, andthosewhodiedfromcausesunrelated tothedisease. Allstudiedsubjects,atthetimeofthesurgery,signedthe informed consent form approved by the Research Ethics Committee(RECNo.9371/2003).
Histologicalanalysis
Histopathologicalassessmentofthecaseswasconductedat theDepartmentofPathology,aftertheparaffinblockswere removedfromtheHeadandNeckSurgerySurgicalSpecimen Bank(CEPNo.9371/2003).Theseblockswereprocessedto obtainfour-micrometersectionsandroutinelystainedwith hematoxylinandeosin(HE)forhistologicalanalysis.
The peritumoral inflammatory infiltratewas character-ized by the influx of mononuclear cells from the chronic inflammatoryprocess(lymphocytes, plasmocytes,and his-tiocytes) into the connective tissue that permeates the invadingneoplasticcells thathave brokenthebasal mem-braneofthesquamousepithelialoralmucosa.Thisinfiltrate wasstainedwithhematoxylin-eosinandthe4micron-thick tumor histological sections were assessed by two experi-encedexaminersusingthesemiquantitativemethodbylight microscopywithobjectivelens,witha40×magnification. Theinflammatoryinfiltratewasquantifiedas:
--- Grade 0:when no or only rare mononuclear inflamma-torycells(lymphocytes,plasmocytes,and/orhistiocytes) were identified in the interface between the invasive tumorandchorion;
--- Grade 1 (mild): when less than 50% of the interface between theinvasivetumor andchorionwasinfiltrated bymononuclearinflammatorycells;
--- Grade2(moderate):whentheinflammatoryinfiltratewas ≥50%and≤75%inthetumor-chorioninterface;
--- Grade3(intense):whentheinflammatoryresponsewas presentin>75%ofthetumor-chorioninterface.
Statisticalanalysis
Forthestatisticalanalysis,patientswithinflammatory pro-cessgradezeroand one(0and1)were groupedasminor inflammatoryprocessandthoseclassifiedasgrades2and3, asmajorinflammatoryprocess.Tworesponsevariableswere consideredseparately:deathandrecurrence.Foreachone, theassociationwiththeinflammatoryprocess(explanatory variable)wasassessed.
Survivalcurvesforeachvariablewereestimatedbythe Kaplan---Meiermethod,whichwerecomparedusingthe log-ranktest.Coxregression(proportionalhazardsmodel)was
1.00
0.75
0.50
0.25
0.00
0 20 40 60 80 100
Time (months)
Minor inflammatory process Major inflammatory process Kaplan-Meier survival curves
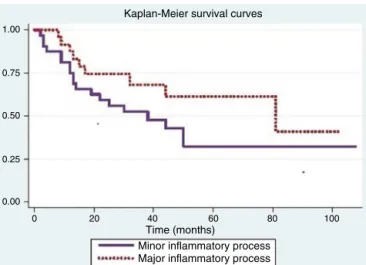
Figure1 Kaplan---Meiersurvivalestimates,perinflammatory process.
usedtoevaluatetheeffectoftheinflammatoryprocesson response(deathorrecurrence),consideringtheadjustment foreachoftheothervariables.13
The association of the inflammatory process with the other sociodemographic aspects, clinical aspects, clinical staging, and histological stagingvariables wereevaluated byFisher’sexacttest.
Results
Atotalof57tumorsampleswereanalyzed,inwhichthe per-itumoralinflammatory infiltrateconsistedof lymphocytes, plasmocytes,and/orhistiocytes.
Fig.1shows that theprobabilityof survivalin over 12 months was 0.75 (95% CI: 0.56---0.87) for individuals with minorinflammatoryprocess(Grades0and1)and0.88(95% CI>0.66---0.96)forsubjectswithmajorinflammatoryprocess (Grades2and3).Thelog-ranktestusedtocomparesurvival curvesofbothprocessesshowednosignificance(p=0.14).
TheCoxproportionalhazardsmodelwasusedtoassess differencesbetweeninflammatoryprocesseswhenadjusted forvariablesthatweresignificantinthelog-ranktest.When adjustedfor smoking,therewasadifferencein inflamma-toryresponse(p=0.05);fortheothervariables,theresults werenotsignificant.
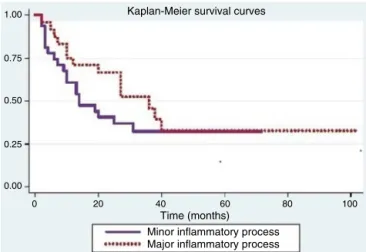
Tumorrecurrenceis shown in Fig.2.The log-ranktest usedtocomparetherecurrencecurvesfor bothprocesses wasnotsignificant(p=0.24).
Positivesignificance forrecurrencewasobserved when considering age (p=0.04), smoking (p<0.01), alcoholism (p<0.01), and degree of tumor differentiation (p=0.02). Theothervariableswerenotsignificant.
TheCoxproportionalhazardsmodelwasusedtoassess the differences between inflammatory processes when adjustedforvariablesthatweresignificantinthelog-rank test.Whenadjustingforsmoking,adifferencewasobserved betweentheinflammatoryprocesses(p=0.05).
Table1 FrequencydistributionoftheinflammatoryprocessinrelationtosociodemographicvariablesandFisher’sexacttest p-value.
Variable p Inflammatoryprocess Total
n Major(%) n Minor(%)
Age 0.04
>50years 7 38.9 11 61.1 18
51---59years 10 52.6 9 47.4 19
>60years 15 79 4 21 14
Gender 0.18
Male 28 62.2 17 37.8 45
Female 4 36.4 7 63.6 11
Smoker 0.74
Yes 26 59.1 18 40.9 44
No 6 50 6 50 12
Alcoholconsumption 0.57
Yes 22 61.1 14 38.9 36
No 10 50 10 50 20
associated with older ages and minor inflammatory pro-cesseswithyoungerages(Table1).
Discussion
AccordingtoRoithmaieretal.14 theimmunesystemhasan
important rolein the developmentof malignancies,since
patients undergoing immunosuppression to receive organ transplantswere21timesmorelikelytohaveheadandneck neoplasms than the overall population. Moreover, Galon etal.15verifiedthattheimmunesystemalsoinfluences
can-cerrecurrence,asincolon cancer, andthepresence ofT cellsintheresectedtumorpredictstumorevolutionmore accuratelythanstaging. However,the roleof theimmune
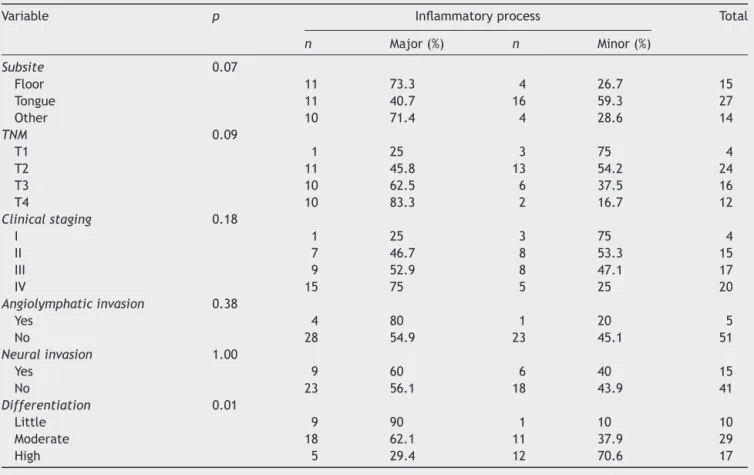
Table2 Frequency distributionofthe inflammatoryprocess inrelationto ageanddifferentiationand Fisher’sexact test p-value.
Variable p Inflammatoryprocess Total
n Major(%) n Minor(%)
Subsite 0.07
Floor 11 73.3 4 26.7 15
Tongue 11 40.7 16 59.3 27
Other 10 71.4 4 28.6 14
TNM 0.09
T1 1 25 3 75 4
T2 11 45.8 13 54.2 24
T3 10 62.5 6 37.5 16
T4 10 83.3 2 16.7 12
Clinicalstaging 0.18
I 1 25 3 75 4
II 7 46.7 8 53.3 15
III 9 52.9 8 47.1 17
IV 15 75 5 25 20
Angiolymphaticinvasion 0.38
Yes 4 80 1 20 5
No 28 54.9 23 45.1 51
Neuralinvasion 1.00
Yes 9 60 6 40 15
No 23 56.1 18 43.9 41
Differentiation 0.01
Little 9 90 1 10 10
Moderate 18 62.1 11 37.9 29
1.00
0.75
0.50
0.25
0.00
0 20 40 60 80 100
Time (months) Minor inflammatory process Major inflammatory process Kaplan-Meier survival curves
Figure2 Kaplan---Meierestimatesofrecurrenceper inflam-matoryprocess.
system in cancer progression is not clear. The immune
surveillanceconceptstatesthatthesystemshouldrecognize anddestroythetransformedcellclonesbeforethey gener-atetumors.However,the importanceofsuchsurveillance hasbeen metwith reservation,since theydo not appear toreact tomany neoplasms.8 Conti-Freitas et al.16 when
analyzingcellculturesin17patientswithlaryngealcancer, concludedthattherewasadeficiencyoftheimmunological system (decreased induced lymphoproliferation in stimu-lated culturesand deficiencies in theproduction of IFN-y andTNF-␣ inunstimulatedcultures)thattendstonormalize
aftertumorresection(laryngectomy)orBCGuse.
AccordingtoWhiteside9thereareseveralpossible
mech-anisms for tumors to escape immunologic suppression including:theexpression ofpoorlyimmunogenicantigens, defectsinantigenprocessing pathways,inadequate inter-actions, and production of immunosuppressive factors by inflammatory cells adjacent to theneoplasm. We believe thatis waswhathappened inour study,sinceno statisti-cally significant differenceswere observed comparingthe prognosticfactors survivaland disease-freeinterval, with the presence of minor and the major inflammatory pro-cesses.Thisresultmaybeduetosamplesize(57tumors),as Manzanoetal.11 withasampleof46patientswithSCCOC,
alsofoundnosignificantdifferencebetweentheintensities ofperitumoralinflammatoryinfiltrate andsurvivalcurves, althoughtheyobservedthatthemorefrequentthepresence ofneckmetastasis,thelowertheintensityoftheinfiltrate. Inthisstudy,weobserveda statisticallysignificant dif-ference betweenthe degree of tumor differentiation and peritumoral inflammatory infiltrate; the lower the tumor differentiation (more aggressive), the greater the inflam-matoryprocess.
Inasimilarstudy,Vieiraetal.7concludedthatthe
cellu-larimmuneresponseisamajordefensemechanismofthe oralmucosa,astheyobservedtheexpression ofagreater numberofTlymphocytesinundifferentiatedsquamouscell carcinoma.Moreover,Manzanoetal.11showedastrong
ten-dencytowardaworseprognosisamongtumorswithpoorly differentiatedcellsandlessinflammatoryinfiltrate.
The results of the present study show that, as tumor stage increases, such as in growth (TNM classification), thereisatrendtowardincreasedperitumoralinflammatory
infiltrate,butwithoutstatisticaldifferences,whichmeans thattheinflammatoryinfiltratetendstoincreasealongwith thetumormassgrowth.Thisobservationleadstothe conclu-sion,asChavesetal.17 thattheimbalancein theimmune
system does notnecessarily correlate withthenumber of defensecellsthatarepresent,butoftenresultsfrom fail-ureinthefunction,regulation,ormigration,ofapopulation ofimmunecellstothetumorsite.Similarly,Abreuetal.18
observedan inverseassociationbetweenadvancedtumors and degree of differentiation, and Costa et al.19
demon-strated worse prognosis in advanced tumors, considering metastasisasthemainprognosticindicator.
Ithasbeenmentioned thattheintensityofthe inflam-matory infiltrate ranges from mild to severe in tumors; thehighestdensityofinflammatorycellsisassociatedwith lower rates of recurrence and, when lymphocytes pene-tratethetumor,prognosisismorefavorable.15However,this
studyonlyshowedthatolderpatientshadahigherincidence ofinflammatoryprocess,whichwasstatisticallysignificant; however, thisincreasedcelldensity didnot translateinto increased survival.It is believed thatall tested cell lines arepresent,butonlyThelperlymphocytesareassociated withthedegreeoftumormalignancyandnottotheamount of inflammatory cells. Conversely, Chaves et al.17 when
studying30casesofSCCOC,foundnostatisticalcorrelation betweeninflammatoryinfiltrateandage.
Itwasalsopossibletoverifythatsurvivalandrecurrence showed anassociation withsmoking, alcohol consumption anddegreeoftumordifferentiation,similartothatobtained by Montoro etal.6 whoobserved a statistical significance
betweensurvivalandthefollowingvariables:age,gender, smoking and alcohol consumption, while Almeida et al.20
showed an association between smoking andalcohol con-sumptionwithprognosis,incontrasttoOliveiraetal.21who
found noinfluence of smokingonrecurrences and metas-tases.
Furtherstudiesmustbeconductedwithalargersample sizetoverifytherealinfluenceoftheinflammatoryprocess asaprognosticfactorandotherpossibleinteractionswith oralcancer.
Conclusion
Theperitumoralinflammatoryprocess,althoughassociated withthe degree of histologicaldifferentiation, cannot be consideredaprognosticfactorforSCCOC,asitisnot associ-ated with survival and disease-free interval.Additionally, there was a direct association between the peritumoral inflammatoryprocessandfactorssuchasage,smoking,and alcoholconsumption.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ParkinDM,BrayF,FerlayJ,PisaniP.Globalcancerstatistics, 2002.CACancerJClin.2005;55:74---108.
3.BungetA,FronieA,AfremE,CorlanPuscuD,ManoleaH,DanAR, etal.Microscopicaspectsofangiogenesisand lymphangiogen-esisinoralsquamouscellcarcinoma.RomJMorpholEmbryol. 2013;54:623---7.
4.SeverinoP,AlvaresAM,MichaluartPJr,OkamotoOK,NunesFD, Moreira-FilhoCA,theHeadandNeckGenomeProjectGENCAPO. Global gene expression profiling of oral cavity cancers sug-gestsmolecular heterogeneitywithinanatomicsubsites.BMC ResNotes.2008;1:113.
5.MassanoJ, Regateiro FS, JanuárioG, FerreiraA. Oral squa-mous cell carcinoma: review of prognostic and predictive factors.Oral Surg OralMed Oral Pathol Oral Radiol Endod. 2006;102:67---76.
6.Montoro JRMC, Hicz HA, Souza L, Livingstone D, Melo DH, Tiveron RC, et al. Prognostic factors in squamous cell car-cinoma oftheoral cavity.Braz J Otorhinolaryngol.2008;74: 861---6.
7.VieiraLDF,VieiraBJ,GuimaraesMAM,AarestrupFM.Cellular profileoftheperitumoralinflammatoryinfiltrateinsquamous cellscarcinoma oforalmucosa:correlationwiththe expres-sionofKi67and histologicgrading.BMC OralHealth.2008;8: 1---8.
8.AbbasAK,BenoistC,BluestoneJA,CampbellDJ,GhoshS,Hori S,etal.RegulatoryTcells:recommendationstosimplifythe nomenclature.NatImmunol.2013;14:307---8.
9.WhitesideA.Poverty and HIV/AIDSinAfrica.Third WorldQ. 2002;23:313---32.
10.JingJ,LiL,WeiE,SunG.Prognosticpredictorsofsquamouscell carcinomaofthebuccalmucosawithnegativesurgicalmargins. JOralMaxillofacSurg.2006;64:896---901.
11.Manzano AC, Altemani A, Martins AS, Del Negro A, Tincani AJ.Caracterizac¸ãoimuno-histoquímicadoinfiltradolinfocitário embiópsiadecarcinomaespinocelulardalínguaesoalhooral esuaimplicac¸ão prognostica. Rev BrasCir Cabec¸a Pescoc¸o. 2010;39:270---6.
12.WadiaP,RaoD,PradhanT, PathakA,Chiplunkar S.Impaired lymphocyte responses and their restoration in oral cancer patientsexpressingdistinctTCRvariableregion.Cancer Inves-tig.2008;26:471---80.
13.HosmerDW,LemeshowS.Appliedsurvivalanalysis.NewYork: Wiley;1999.
14.RoithmaierS,HaydonAM,LoiS,EsmoreD,GriffithsA,Bergin P,etal.Incidenceofmalignanciesinheartand/orlung trans-plantrecipients:asingle-institutionexperience.JHeartLung Transplant.2007;26:845---9.
15.Galon J, Costes A, Sanchez-Cabo F, KirilovskyA, Mlecnik B, Lagorce-PagèsC,etal.Type,density,andlocationofimmune cellswithinhumancolorectaltumorspredictclinicaloutcome. Science.2006;313:1960---4.
16.Conti-FreitasLC,Foss-FreitasMC,MamedeRCM,FossNT.Effect ofsurgicaltreatmentonlymphoproliferationinadvanced supra-glotticlaryngealcancer.Laryngoscope.2007;117:268---71.
17.ChavesACM,RamalhoL,Sant’AnaMF.Avaliac¸ãodascélulasdo infiltradoinflamatórioperitumoraldoscarcinomas espinocelu-laresdeboca.RevFacOdontol.2002;43:60---4.
18.AbreuMAMM,PimentelDRN,SilvaOMP,BlachmanIT,Michany NS, Hirata CH, et al. Carcinoma espinocelular do lábio: avaliac¸ão de fatores prognósticos. Braz J Otorhinolaryngol. 2004;70:765---70.
19.Costa AL, Araujo Júnior RF, Ramos CC. Correlac¸ão entre a classificac¸ãoTNMemalignidade---característicahistológicade carcinomadecélulasescamosasoral.BrazJOtorhinolaryngol. 2005;71:181---7.
20.AlmeidaFCS,CazalC,NunesFD,AraújoME,DiasRB,SilvaDP. Fatoresprognósticosnocâncerdeboca.RevBrasCiêncSaúde. 2011;15:471---8.