www.jped.com.br
ORIGINAL
ARTICLE
The
effect
of
NaCl
0.9%
and
NaCl
0.45%
on
sodium,
chloride,
and
acid---base
balance
in
a
PICU
population
夽
,
夽夽
Helena
Isabel
Almeida
a,∗,
Maria
Inês
Mascarenhas
a,
Helena
Cristina
Loureiro
a,
Clara
S.
Abadesso
a,
Pedro
S.
Nunes
a,
Marta
S.
Moniz
a,
Maria
Céu
Machado
baPediatricIntensiveCareUnit,PediatricDepartment,HospitalProf.DoutorFernandoFonsecaEPE,Amadora,Portugal bFacultyofMedicine,UniversidadedeLisboa,Lisbon,Portugal
Received22August2014;accepted17December2014
Availableonline10June2015
KEYWORDS
Acid---base equilibrium; Chloride; Hyponatremia; Maintenancefluids; Pediatrics;
Sodium
Abstract
Objectives: Tostudytheeffectoftwointravenousmaintenancefluidsonplasmasodium(Na), andacid---basebalanceinpediatricintensivecarepatientsduringthefirst24hofhospitalization. Methods: A prospective randomized controlled study was performed, which allocated 233 patients togroups: (A)NaCl0.9%or(B)NaCl0.45%. Patientswereaged 1dayto18 years, hadnormalelectrolyteconcentrations,andsufferedanacuteinsult(medical/surgical).Main outcomemeasured:changeinplasmasodium.Parametrictests:t-tests,ANOVA,X2statistical significancelevelwassetat˛=0.05.
Results: Group A(n=130):serum Naincreasedby 2.91(±3.9)mmol/Lat24h(p<0.01);2% patientshadNahigherthan150mmol/L.MeanurinaryNa:106.6(±56.8)mmol/L.Nochange inpHat0and24h.GroupB(n=103):serumNadidnotdisplaystatisticallysignificantchanges. FifteenpercentofthepatientshadNa<135mmol/Lat24h.Thetwofluidshaddifferenteffects onrespiratoryandpost-operativesituations.
Conclusions: Theuseofsaline0.9%wasassociatedwithalowerincidenceofelectrolyte dis-turbances.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:AlmeidaHI,MascarenhasMI,LoureiroHC,AbadessoCS,NunesPS,MonizMS,etal.TheeffectofNaCl0.9%
andNaCl0.45%onsodium,chloride,andacid---basebalanceinaPICUpopulation.JPediatr(RioJ).2015;91:499---505.
夽夽
StudyconductedatPediatricIntensiveCareUnit,DepartmentofPediatrics,HospitalProf.DoutorFernandoFonsecaEPE,Amadora, Portugal.
∗Correspondingauthor.
E-mail:[email protected](H.I.Almeida).
http://dx.doi.org/10.1016/j.jped.2014.12.003
PALAVRAS-CHAVE
EquilíbrioÁcido-Base; Cloreto;
Hiponatremia; Fluidosde manutenc¸ão; Pediatria; Sódio
EfeitodoNaCla0,9%edoNaCla0,45%sobreosódio,cloretoeequilíbrioácido-base emumapopulac¸ãodeUTIP
Resumo
Objetivo: Estudar o efeito de dois fluidos de manutenc¸ão intravenosos sobre o sódio (Na) plasmáticoeoequilíbrioácido-baseempacientesdeterapiaintensivapediátricaduranteas primeiras24horasdeinternac¸ão.
Métodos: Foirealizado um estudocontroladorandomizadoprospectivo.Alocamos aleatoria-mente233pacientesparaosgrupos:(A)NaCla0,9%ou(B)NaCla0,45%.Ospacientescom 1dia a18 anosde idade apresentavam concentrac¸ões normais de eletrólitose sofriam de insulto agudo (médico/cirúrgico). Principal resultado: variac¸ão no sódio plasmático. Testes paramétricos:testet,ANOVA,qui-quadrado.Onívelderelevânciaestatísticafoiestabelecido em˛=0,05.
Resultados: GrupoA(n=130):oNaséricoaumentou2,91(±3,9)mmolL−1em24h(p<0,01); 2% dos pacientes apresentaram Na acima de 150mmolL−1. Concentrac¸ão média de Na na urina: 106,6 (±56,8)mmolL−1.Sem alterac¸ão nopH em 0 e 24h. Grupo B (n=103): o Na sériconãoapresentoualterac¸ões estatisticamentesignificativas.15%dospacientes apresen-taramNa<135mmolL−1em24h.Osdoisfluidostiveramefeitosdiferentessobreassituac¸ões respiratóriaepós-operatória.
Conclusão: Ousodesoluc¸ãofisiológicaa0,9%foiassociadoàmenorincidênciadedistúrbios eletrolíticos.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
The choice of maintenance fluids in hospitalized patients is an issue thatphysicians frequently have toconsider.In the last decade, the recognition of severe complications associatedwithexcessvolumeadministrationandiatrogenic hyponatremiahasraisedincreasedinterestinthe prescrip-tionoffluidsandonitsconsequences,especiallyincritical careconditions.1---4
Hyponatremia is defined as a concentration of plasma Nalowerthan135mmol/L.5Nearlyallhospitalizedpatients
have the risk of developing hyponatremia as a result of the potential presence of known stimuli for producing anti-diuretic-hormone (ADH).6---9 In children admitted toa
PICU,10---12 many such stimuli may be present: (1) those
relatedto hemodynamic status --- hypovolemiaor hyperv-olemiaand(2)thoserelatedtoinappropriate antidiuretic hormone release syndrome (IADHRS), present in central nervoussystem disturbances,pulmonarydiseases, tumors, andpostoperativeconditions.2,3,6,10---12Untilrecently,
hypo-tonic fluids (0.2---0.3% saline) were used as maintenance fluidsforhospitalizedchildren,basedontheHolliday---Segar equation,13,14butrecentstudiesshowedthathyponatremia
maybeexacerbatedbyhypotonicintravenousfluids.15---19
Hypernatremia,whichmaybedefinedasserumNahigher than145mmol/L(althoughvaluesunder150mmol/Larenot considereddeleterious),hasalsobeenextensivelydescribed inpatientsin intensive careunits.10,11 At admission,2---6%
of patients are hypernatremic, and during the course of treatment in the ICU, 4---26% of patients become hyper-natremic. Many factors may contribute to hypernatremia
in thesepatients,suchaspatientinability tocontrolfree water intake(sedated, intubated, mental statusaltered), fluidrestriction,excessivefluidlosses,andtreatmentwith Nacontainingfluids.AsPICUpatientsareatincreasedrisk of developingelectrolyte imbalance,it wouldbe relevant to identify a maintenancefluid not associated with elec-trolyticdisturbances,suitabletoadministertoawiderange ofpatients.
ThisstudycomparestheeffectsonNahomeostasisand acid---basebalance,inpatientsadmittedtothePICU,oftwo intravenousmaintenancefluids:NaCl0.9%,with154mEqNa andCl/L(FluidA),andNaCl0.45%,with75mEqNaandCl/L (FluidB),bothin5%dextrose.FluidAishypernatremicand hyperosmotic, while FluidB is hyponatremicand closeto plasma osmolarity. These are the two maintenance fluids mostusedinthis department,wherelowerNa concentra-tionintravenousfluids(includingsaline0.18%)havenotbeen usedsince2000.
Theprimaryobjectiveofthestudywastodetermineand compare theeffects at 24h onplasma Naof thetwo flu-idsstudied.Otheroutcomesconsideredweretheincidence of hypernatremia and hyponatremia, urinary excretion of electrolytes,andacid---basebalance(pH,bicarbonate,base excess,totalCO2,chloride)after24hundertreatmentwith thetwomaintenancefluids.
Methods
Studydesign
A prospective, randomized, open, label-controlled study wasused,witha simplerandomizationlist.Patientswere distributedbetweentwogroups,AandB.InGroupApatients weretreatedwithsaline0.9%in5%dextroseasmaintenance fluid,whileinGroupBpatientsreceivedsaline0.45%in5% dextroseasmaintenancefluid.Datawerecollectedat24h. Thestudywasterminatedwhenenteralfluidswere admin-isteredataratehigherthanmL/kg/hinchildrenlessthan 10kgor10mL/hinolderchildren.
Participants
ThisstudywasconductedinasecondaryPICUwith11beds thatadmits450patientsannually.Patientsaged1dayto18 yearsoldwereincluded,withanacuteinsult(medicalor sur-gical),whoneededexclusiveadministrationofintravenous fluidsfor morethan24h.Patientswithsevereelectrolyte andacid---basedisturbances,metabolicdisease,plasmaNa lowerthan135mEq/Lorhigherthan150mEq/L,renal insuf-ficiency,orwhorefusedtosign aninformedconsentwere excludedfromthestudy.Duringthestudy,patientsinwhom themaintenancefluidwasswitched orinterrupted before 24hwereexcluded.
Interventionsandtherapeuticprotocol
Inbotharmsofthestudy,fluidvolumeprotocolswerethe same.Inpatientswithrespiratorydisease,fluidrestriction withadministrationof50---90% of thevolumeproposedby theHolliday---Segarequationwasused.Inabdominalsurgery, 100---120% of the dailyproposed intake wasadministered. Duringthisstudy,everyfluidressuscitationwasdonewith NaCl0.9%,20mL/kgfor20---30min,whenshockorpre-shock were detected. A daily waterbalance of zero was aimed in this set of patients, and diuretic (furosemide), when needed,wasadministeredtoachievethisgoal.
Datacollection,variables,andoutcomes
This study used a questionnaire designed to collect epi-demiologic,clinical,andlaboratorydata.Variablesincluded were:date,gender,age,weight,neonate(y/n),diagnosis, diagnosticgroup, previous existence ofa chronic disease, PIM2(PediatricIndexofMortality),needforfluidexpansion, diuretics, volume of fluids administered, urinary output, water balance,Na, Cl, potassium, pH andbicarbonate at T0h (prior to fluid administration) and 24h, and urinary ionogramatT24h.
Primary outcomewasthedifferencebetweenNaat T0 andT24hinmmol/L(Na24h/Na0h) withmaintenance Fluids A and B. Secondary outcomes were: incidence of hyper or hyponatremia, pH, bicarbonate, base excess, tCO2andchlorideatT24h,andurinaryexcretionofNaand Cl.
Samplesize
Inapriorpilotstudy,20 thepresentauthorsdetecteda
dif-ference in serumNa of 2mmol/L after 24h using normal salineor0.45%salineinPICUpatients.For˛=0.05,apower
of0.9,andanexpecteddifferenceof2mmol/LinserumNa at24h betweenthetwogroups,it wasconcludedthat66 patientswereneededin eacharm ofthestudy.Fora dif-ferencebetweenthetwovaluesof1.5mmol/L,eachgroup wouldneed117patients.
Randomization
Patientswererandomizedusingasinglesequenceofrandom assignments,withasimplerandomizationtablebetweenthe twoarms of the study (Fluids Aand B). The physician in chargeofthepatientconsultedthisrandomizationtableand assignedthechildtoGroupAorB.
Statisticalmethods
Descriptivestatisticswerecalculatedforthewholesample andforGroupsAandB.Thedataweretestedfornormality, asrequired by subsequentparametric statistical tests. To analyzedifferencesinNabetweenT0andT24h(main out-come)anddifferencesinClandacid---basebalancebetween T0and T24 and between electrolytesin Groups A and B, independentandpairedt-testsandANOVAwereused.The univariateanalysisalso utilizedX2.Statistical significance levelwassetat 0.05.Datawereanalyzed usingSPSS ver-sion19(SPSS,Inc.,SPSSforWindows,Version19.0,Chicago, USA).
Ethics
Informedconsentwasobtainedfromtheparents/guardians ofpatientsunder16yearsold,andfromadolescentsaged16 orolder.ThestudywasapprovedbytheEthicsCommittee ofHospitalFernandoFonseca.
Results
Flowchart
During2011, 268 episodeswere included and randomized toarm A---FluidA(n=135)orB---FluidB(n=133)ofthe study.InGroupsA andB,5 and30episodes,respectively, wereexcludedbecauseofmissingdataconsideredrelevant forthestudy.Attheend,therewere130patientsinGroup Aand103inGroupB,foratotalof233patientsanalyzed (Fig.1).
Results
Assessed for eligibility (n = 268)
Excluded (n = 15)
♦ Did not meet inclusion criteria (n = 15)
Analysed (n = 135)
♦Excluded from analysis (missing data) (n = 5) Lost to follow-up (give reasons) (n = 0)
Discontinued intervention (give reasons) (n = 0) Allocated to intervention A (n = 135)
♦ Received allocated intervention (n = 135)
Lost to follow-up (give reasons) (n = 0)
Discontinued intervention (change of maintenance fluid before 24h) (n = 15) Allocated to intervention B (n = 133)
♦ Received allocated intervention (n = 133) ♦ Did not receive allocated intervention (n = 0)
Analysed (n = 118)
♦ Excluded from analysis (missing data) (n = 15)
Allocation
Analysis Follow-up Randomized (n = 253) Enrollment
Figure1 Studyflowchart.CONSORT2010flowchart.
onewereadmittedforarespiratoryproblem,65aftermajor surgery,24forshock,and23hadmiscellaneousconditions. Fifty-threepatientsweremechanicallyventilated.
Fluid volume aimed for a daily balance of 0 and var-iedbetween 24% (respiratory patient)and 193% (surgical patient)ofbasalfluidrequirements,withameanof91.0%.
Dailywaterbalancehadameanof+2.4mL,withastandard deviation of388mL.The median was+125mL, with mini-mumof−688andmaximumof2066mL.Meanandmedian urine output were,respectively, 2.15mL/kg/h (±1.6) and 1.7mL/kg/h (min 0.25, max 10.5). Fifty-one had hemo-dynamic instability. Volume expansion was needed in 43
Table1 EmographicandclinicalcharacterizationofGroupsAandB.
GroupA(n=130) GroupB(n=103) p
Gender
Male(%) 80(62%) 53(57%) 0.28
Female(%) 48(38%) 44(43%)
Meanage(months)(SD) 49.9(SD±62.5) 41.1(SD±64.4) 0.22
Chronicdisease(%) 38(29.7%) 39(40.2%) 0.1
Mechanicalventilation(%) 31(23.8%) 22(21.4%) 0.79 Waterbalanceat24h(mL) 252.2(SD±330.7) 244.7(SD±440.6) 0.73 Na+atT0h 138.1(SD±4.30) 137.7(SD±3.09) 0.72 Cl−atT0h 103.7(SD±4.50) 102.4(SD±4.14) 0.59 pHatT0h 7.34(SD±0.093) 7.34(SD±0.097) 0.78 HCO3atT0h 24.8(SD±3.99) 24.9(SD±4.47) 0.43 Dailyfluid(%basicneeds) 90.8%(SD±18.9) 91.5%(SD±28.6) 0.12
Diuretics 63/128(49%) 40/94(42.5%) 0.15
Fluidresuscitation 22/128(17.2%) 11/91(12.1%) 0.16 NaCl0.9%(20---30mL/kg)
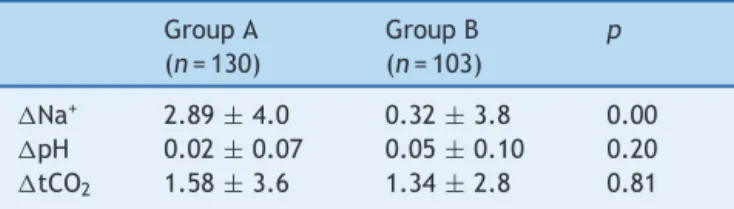
Table2 Sodium,pH,andtCO2variationbetweenGroups AandB.
GroupA (n=130)
GroupB (n=103)
p
Na+ 2.89±4.0 0.32±3.8 0.00 pH 0.02±0.07 0.05±0.10 0.20 tCO2 1.58±3.6 1.34±2.8 0.81
patients,diureticsin105,bloodproductsin35,and inotrop-icsin30.PlasmaNa,Cl,pH,andurinaryNaandClatT0and T24areshowninTable1.
The 35patientsexcluded fromthestudyhadamedian age of 13 months,19 were male, and theirmean sodium was137.9mmol/L.
ComparisonofeffectsofFluidsAandB
Descriptive statistics show that both groups were similar regarding age, gender, chronic disease, PIM2, diagnostic groups,mechanicalventilation,Na,Cl,pHatthebeginning ofthestudy,waterbalance,volumeadministered,andurine output.Useofdiureticsandvolumeexpansionwere statis-tically similarin bothgroups (Table1). Basedonthis, the effectsofbothfluids(AandB)onNaandpHbalancewere compared(Table2).
EffectsonNa
GroupA---NaCl0.9%(n=130)
Using Fluid A, serum Na increased from 138.1mmol/L (±4.3)attimeT0to140.9mmol/L(±4.9)atT24h,witha meanincreaseof2.9mmol/L(±3.9)(p<0.01).Tenpatients (5%) had Na higher than 145mmol/L and three of them hadsodiumhigherthan150mmol/L (151.4;152.6;155.0). This corresponds to an attributable risk of 2%. Seven patients in this group had hyponatremia, with Na higher than 130mmol/L. Urinary Na in this group had a mean of 106.6mmol/L (±56.8).Clinical symptomatologydue to hypernatremiaorhyponatremiawasnotregistered.
GroupB---NaCl0.45%(n=103)
WithFluidB,atT0,serumNawas137.86mmol/L(±3.1),and at T24,137.81mmol/L (±3.0),witha meandifferenceof −0.2mmol/L,whichwasnotstatisticallysignificant. Four-teenpatients hadNavaluesunder135mmol/L(130---134). Inthese14patients,thedifferencesinNabetweenT0and T24variedfrom0.5to−10mmol/Landcorrespondedtoan attributablerisk of15%. None ofthesepatients had clini-calsignsofhyponatremia.Twopatientshadhypernatremia (Naof146.5and147mmol/L).UrinaryNainthisgrouphad a meanof 81.8mmol/L (±5.0),and thisvalue was statis-ticallysignificantlydifferentfromtheNaurinaryexcretion withFluidA(p=0.04).
Effectofbothfluidsonacid---basebalance
HCO3 pH, totalcontent inCO2 andbase excess increased inbothgroups fromT0toT24.Therewerenostatistically
significant differences using these maintenance fluids. Saline0.9%andsaline0.45%increasedthetotalCO2at24h (Table2).
Fluid A increased serum Cl levels from 104.0mmol/L (±4.7)to106.7mmol/L (±6.7)(p<0.01).FluidBchanged the initial Cl from 102.7mmol/L (±4.2) to 102.3mmol/L (±6.1);thiswasnotasignificantdifference(Table2).
Neonates(n=42)
Based on different physiologic knowledge, neonates are expectedtobehavedifferentlyfromolderchildrenin rela-tion to electrolyte balance. This study observed those aspectsandconcludedthatneonatesinGroupAhadgreater increasesinNaserumconcentration(5.0±4.6mmol/L ver-sus 2.5±3.8mmol/L in older children) at 24h, and one neonatehadaplasmaNalevelof152.6mmol/L.InGroupB, nodifferencesweredetectedintheseparametersbetween neonates and older children. No differences were seen betweenneonatesandchildreninrelationtourinary elec-trolyteexcretionandurinaryoutput.
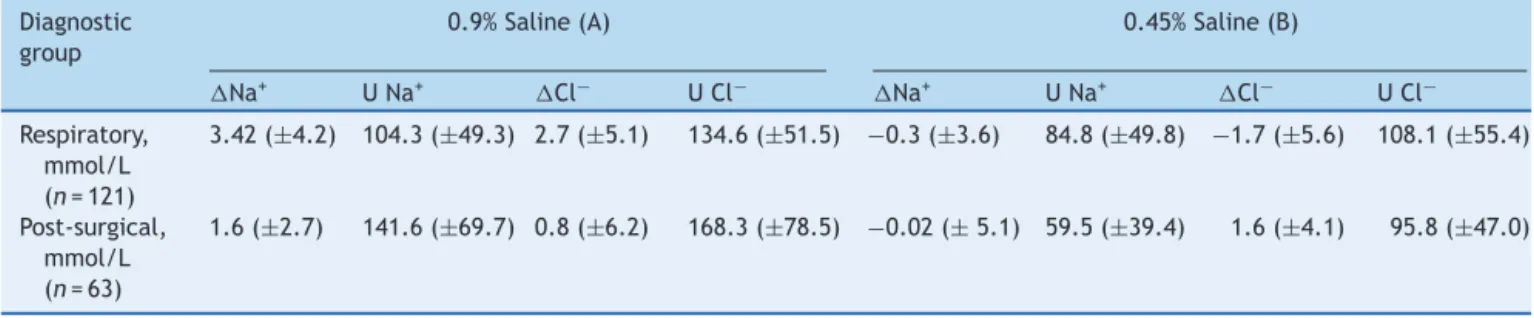
Respiratoryandpost-operatorypatients
Differences were detected between major diagnostic groups,assubsequentlyexplained(Table3).
Respiratorygroup(n=121)
When using Fluid A (n=63), the Na plasma concentra-tion increased by 3.42mmol/L (±4.2), and decreased by 0.3mmol/L (±3.6) when using FluidB (n=58) (p<0.001). Urinary excretion withFluid A was104.3mmol/L (±49.3) and84.8mmol/L(±49.8)withFluidB,withnostatistically differencebetweenthesevalues.
Post-operativegroup(n=65)
In post-operative patients, urinary excretion of Na was 141.6mmol/L(±69.7)withFluidA(n=33)and59.5mmol/L (±39.4) with Fluid B (n=20), p<0.001. The differences in serum Na when using Fluids A or B were not statis-tically significant. In this group of patients, electrolyte urinary excretion was significantly different between the twogroups, andthe differencein serumelectrolytes was notstatisticallysignificant.
Discussion
Saline 0.9% was compared to saline 0.45%. The risk of hypernatremiausingsaline0.9%wassignificantlylower(2%) thantheriskofhyponatremiausingsaline0.45%(15%),and hyponatremiais arelevant issue inintensive care units.21
BothfluidsinducedmarkedurinaryexcretionofNa. Sabaetal.,22intheirclinicaltrialwith36children,
Table3 Differencesinelectrolytesvariationbetweendiagnosticgroups:respiratoryandpost-surgical.
Diagnostic group
0.9%Saline(A) 0.45%Saline(B)
Na+ UNa+ Cl− UCl− Na+ UNa+ Cl− UCl−
Respiratory, mmol/L (n=121)
3.42(±4.2) 104.3(±49.3) 2.7(±5.1) 134.6(±51.5) −0.3(±3.6) 84.8(±49.8) −1.7(±5.6) 108.1(±55.4)
Post-surgical, mmol/L (n=63)
1.6(±2.7) 141.6(±69.7) 0.8(±6.2) 168.3(±78.5) −0.02(±5.1) 59.5(±39.4) 1.6(±4.1) 95.8(±47.0)
Reyetal.,12inaprospectiverandomizedstudy,compared
theutilizationoffluidswith30---50mmol/LNatofluidswith 136mmol/L Na in a group of 134 ICU patients. They also concludedthathypotonicfluidsincreasedtheriskof hypona-tremia. They described only one case of hypernatremia with normal saline. In the present study hypernatremia wasdetected in three patients, which corresponds to an attributableriskof2%.Thisdiscrepancymaybedueto dif-ferentclinicaland therapeutic situationsbetween studies (differenthemodynamic status), although theywere both conductedinPICUs.
Yung and Keeley23 compared normal saline with 0.18%
salinein aPICU population, concludingthatboth mainte-nancefluidswererelatedwithhyponatremia.Theirsample wassmallerandinsomeaspectsdifferentfromthe popula-tionstudiedinthisstudy:mostofthepatientsweresurgical, mildlyill,andnotventilated.TheyalsostudiedtheNa uri-nary output, which wassimilar in both groups and lower thanthatofthepresentsample.Inthepresent study,the hypotonicfluidstudiedalsoinducedhyponatremia.
There are studies including only post-operative patients24---26: Choong et al.24 conducted a randomized
controlledtrialincluding258patients(someofthem admit-ted to the PICU) comparing 0.45% saline to 0.9% saline. The 0.9% fluid proved to be less deleterious. Coulthard etal.26comparedtheeffectsonplasmasodiumat16---18h
ofHartmann’ssolutionand5%dextroseor0.45%salineand 5% dextrose in 82 patients following major surgery; they concludedthatthepostoperativefallinNawassmallerin childrenwhoreceivedHartmann’ssolutionand5%dextrose. Thepresentresultsagreewiththeseconclusions.
Effectsonacid---basebalancewerealsoregarded.Saline 0.9%,whenusedinlargevolumes,isknowntocause hyper-chloremicmetabolicacidosis27;basedontheseresultsitis
possibletoconcludethatwhenusedasmaintenancefluid, saline0.9%orsaline0.45%didnothavethateffect,although bothfluidsincreasedthetotalCO2.
In this sample of 233 acutely ill medical and surgical patients,0.45%normalsalineinducedhyponatremiain15% ofthepatients, andnone ofthe fluidsinduced significant changesinacid---basebalance.Theseresultsstrengthenthe choiceofanisonatremicmaintenancefluidinthisgroupof patients.
This study has several strengths beyond the size of the sample. To the authors’ knowledge, no other stud-iesfocused onthe effectof maintenance fluidson serum Cl concentrations or acid---base balance. In this study, no effects on acid---base balance were seen with the use of the two different fluids. Individualizing twodiagnostic
groups (respiratory and postoperative) showed different effectsonNaandClconcentrations.Thisraisesthe possibil-ityof interferenceof differenthormonalor multifactorial mechanisms. Postoperative patients excreted higher con-centrations of Na and Cl, which may be related to ADH secretion.McCluskeyetal.28 showedthatinadult
noncar-diac surgery, hyperchloremia is associated with mortality andlongerhospitalization.
Certainlimitationsinherenttothisstudymustbe recog-nized: 35patients wereexcluded(5 fromGroupA and30 from Group B)due tomissing data or interruption of the study;demonstratingthatthetwogroupsstudiedwere sim-ilaratthebeginningofthestudy,andthatthe35patients excludedhadthesameepidemiologiccharacteristicsasthe 233patientsincludedattenuatesthislimitation.
Withthisprospectivecontrolledrandomizedstudy,ithas been observed that although both saline 0.9% and saline 0.45% may be usedin a PICU during 24h asmaintenance fluids,normalsalineshouldbepreferred,asitwasableto increaseplasmaNa,incontrastto0.45%saline,whichwas associated witharelevant risk ofhyponatremia. No clini-calsignsofhypernatremiaorhyponatremiaweredetected. Noneofthefluidsinducedhyperchloremicmetabolic acido-sis.The studyshows thattheprescription ofmaintenance fluids must take into account age, diagnosis, fluid bal-ance, andtheuseofdiuretics orexpansionfluids. Studies addressingthesedifferentvariablesneedtobeperformed. TheuseofbalancedfluidslikeRinger’slactateorother poly-electrolytesolutionsneedstobestudied,astheymayhave substantialclinicaladvantagesinrelationtoNaClfluids.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.HalberthalM,HalperinML,BohnD.Lessonoftheweek:acute hyponatraemiainchildrenadmittedtohospital:retrospective analysisoffactorscontributingtoitsdevelopmentand resolu-tion.BMJ.2001;322:780---2.
2.DearloveOR,RamAD,NatsagdoyS,HumphreyG,CunliffeM, PotterF.Hyponatraemiaafterpostoperativefluidmanagement inchildren.BrJAnaesth.2006;97:897---8.
4.Shafiee MA, Bohn D, Hoorn EJ, Halperin ML. How to select optimal maintenance intravenous fluid therapy. QJM. 2003;96:601---10.
5.Adrogué HJ, Madias NE. Hyponatremia. N Engl J Med. 2000;342:1581---9.
6.PautO,BissonnetteB.Syndromeofinappropriateantidiuretic hormonesecretionafterspinalsurgery inchildren.CritCare Med.2000;28:3126---7.
7.NevilleKA,VergeCF,O’MearaMW,WalkerJL.Highantidiuretic hormonelevelsandhyponatremiainchildrenwith gastroenteri-tis.Pediatrics.2005;116:1401---7.
8.CarlottiAP,BohnD,MallieJP, HalperinML.Tonicitybalance, andnotelectrolyte-free watercalculations, moreaccurately guidestherapyfor acutechangesinnatremia.IntensiveCare Med.2001;27:921---4.
9.AroraSK.Hypernatremicdisordersintheintensivecareunit.J IntensiveCareMed.2013;28:37---45.
10.LindnerG,FunkGC.Hypernatremiaincriticallyillpatients.J CritCare.2013;28(216):e11---20.
11.GehanEA. Clinical trials in cancerresearch. EnvironHealth Perspect.1979;32:31---48.
12.ReyC,Los-ArcosM,HernándezA,SánchezA,DíazJJ, López-Herce J. Hypotonic versus isotonic maintenance fluids in critically ill children: a multicenter prospective randomized study.ActaPaediatr.2011;100:1138---43.
13.Kannan L, Lodha R, Vivekanandhan S, Bagga A, Kabra SK, KabraM.Intravenousfluidregimenandhyponatraemiaamong children: a randomized controlled trial. Pediatr Nephrol. 2010;25:2303---9.
14.ChoongK,KhoME,MenonK,BohnD.Hypotonicversusisotonic salineinhospitalisedchildren: asystematicreview. ArchDis Child.2006;91:828---35.
15.AuAK, RayPE, McBrydeKD,NewmanKD,WeinsteinSL,Bell MJ.Incidenceofpostoperativehyponatremiaandcomplications incritically-illchildrentreatedwithhypotonicandnormotonic solutions.JPediatr.2008;152:33---8.
16.HollidayMA,Segar WE. The maintenance need for water in parenteralfluidtherapy.Pediatrics.1957;19:823---32.
17.DukeT,MolyneuxEM.Intravenousfluidsforseriouslyillchildren: timetoreconsider.Lancet.2003;362:1320---3.
18.LoboDN,DubeMG,NealKR,SimpsonJ,RowlandsBJ,AllisonSP. Problemswithsolutions:drowninginthebrineofaninadequate knowledgebase.ClinNutr.2001;20:125---30.
19.Moritz ML, Ayus JC. Prevention of hospital-acquired hyponatremia: a case for using isotonic saline. Pediatrics. 2003;111:227---30.
20.Almeida H. Normal saline as manutention fluid in respira-torypatients in aPICU. Pediatr CritCareMed. 2011;12:A52 [abstract].
21.KellumJA,ElbersPW,editors.Stewart’stextbookofacid---base. 2nded.Amsterdam:AcidBase.org;2009.
22.Saba TG, Fairbairn J, Houghton F, Laforte D, Foster BJ. A randomizedcontrolledtrialofisotonicversushypotonic main-tenanceintravenousfluidsinhospitalizedchildren.BMCPediatr. 2011;11:82.
23.YungM,KeeleyS.Randomisedcontrolledtrialofintravenous maintenancefluids.JPaediatrChildHealth.2009;45:9---14.
24.ChoongK,AroraS,ChengJ,FarrokhyarF,ReddyD,Thabane L, et al. Hypotonic versusisotonic maintenance fluids after surgeryforchildren:arandomizedcontrolledtrial.Pediatrics. 2011;128:857---66.
25.EulmesekianPG,PérezA,MincesPG,BohnD.Hospital-acquired hyponatremiainpostoperativepediatricpatients:prospective observationalstudy.PediatrCritCareMed.2010;11:479---83.
26.CoulthardMG,LongDA,UllmanAJ,WareRS.Arandomised con-trolledtrialofHartmann’ssolutionversushalfnormalsalinein postoperativepaediatricspinalinstrumentationandcraniotomy patients.ArchDisChild.2012;97:491---6.
27.ChuaHR,VenkateshB,StachowskiE,SchneiderAG,PerkinsK, LadanyiS,etal.Plasma-Lyte148vs0.9%salineforfluid resus-citationindiabeticketoacidosis.JCritCare.2012;27:138---45.