REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Publicação Oficial da Sociedade Brasileira de Anestesiologiawww.sba.com.br
CLINICAL
INFORMATION
Ultrasound-guided
peripheral
nerve
blocks
in
anticoagulated
patients
---
case
series
Luis
Eduardo
Silveira
Martins
a,
Leonardo
Henrique
Cunha
Ferraro
a,b,∗,
Alexandre
Takeda
a,b,
Masashi
Munechika
a,b,
Maria
Angela
Tardelli
a,baUniversidadeFederaldeSãoPaulo(Unifesp),EscolaPaulistadeMedicina,DisciplinadeAnestesiologia,DoreTerapiaIntensiva,
SãoPaulo,SP,Brazil
bSociedadeBrasileiradeAnestesiologia,SãoPaulo,SP,Brazil
Received20May2015;accepted15June2015
Availableonline26October2016
KEYWORDS Peripheralnerve block;
Ultrasound; Coagulation
Abstract
Backgroundandobjectives: The adventof ultrasound hasbrought many benefits to periph-eralnerveblocks.Itincludesbothsafetyandeffectiveness,giventhepossibilityofvisualizing the neurovascular structures andthe needleduring the procedure.Despitethese benefits, thereisnoconsensusintheliteratureontheuseofthistechniqueinanticoagulatedpatients orwithothercoagulationdisorders.Moreover,peripheralblocksvaryindepth,spreadability, andpossibilityoflocalcompression.However,fewsocietiestakeitintoaccountwhen draw-ingupitsrecommendations,establishingasinglerecommendationforperformingperipheral blocks,regardlessoftherouteused.Theobjectiveofthisseriesistoexpandthediscussionon peripheralnerveblockinanticoagulatedpatients.
Casereports: This series reports 9 cases of superficial peripheral nerve blocks guided by ultrasound inpatients withprimary or secondary dyscrasias.All blocks were performed by experiencedanesthesiologistsinthemanagementofultrasound,andtherewasnobruisingor neurologicalinjuriesinthecases.
Conclusions:This caseseriessupport thediscussiononconducting surfaceperipheralnerve blocksandeasylocalknowledgeastheaxillary,interscalene,femoral,saphenousorpopliteal inanticoagulatedpatients,ondualantiaggregationtherapyand/orwithothercoagulation dis-orders,providedthatguidedbyultrasoundandperformedbyananesthesiologistwithextensive experienceinguidednerveblocks.However,largerseriesshouldbeperformedtoprovethe safetyofthetechniqueforthesepatients.
©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](L.H.Ferraro).
http://dx.doi.org/10.1016/j.bjane.2015.06.005
PALAVRAS-CHAVE Bloqueionervo periférico; Ultrassom; Coagulac¸ão
Bloqueiosdenervosperiféricosguiadosporultrassomempacientesanticoagulados ---sériedecasos
Resumo
Justificativaeobjetivos: Oadventodaultrassonografiatrouxeinúmerosbenefíciosparaos blo-queiosdenervosperiféricos.Agregoutantoseguranc¸aquantoeficácia,dadaapossibilidadede visualizac¸ãodeestruturasneurovascularesedaagulhaduranteoprocedimento.Apesardesses benefícios,nãoháconsensonaliteraturasobreousodatécnicaempacientesanticoaguladosou comoutrosdistúrbiosdacoagulac¸ão.Alémdisso,osbloqueiosperiféricosvariamcomrelac¸ãoà profundidade,expansibilidadeepossibilidadedecompressãolocal.Porém,poucassociedades levamissoemconsiderac¸ãoparaelaborarsuasrecomendac¸ões,estabelecemumrecomendac¸ão única parabloqueiosperiféricos,independentementedaviausada. Oobjetivodestasérieé ampliaradiscussãosobrebloqueiodenervosperiféricosempacientesanticoagulados. Relatodecasos: Estasérierelata9casosdebloqueiosdenervosperiféricossuperficiaisguiados porultrassonografiaempacientescomdiscrasiasprimáriasousecundárias.Todososbloqueios foramfeitosporanestesiologistasexperientesnomanejodoultrassom,quenãoforam obser-vadoshematomasoulesõesneurológicasnoscasos.
Conclusões: Asériedecasosemquestãoajudaadiscussãosobrebloqueiosperiféricos superfici-aisedefácilcompressãolocal,comooaxilar,interescalênico,femoral,safenooupoplíteo,em pacientesanticoagulados,duplamenteantiagregadose/oucomoutrosdistúrbiosdacoagulac¸ão desdequeguiadosporultrassomefeitosporanestesiologistacomvastaexperiênciaem blo-queiosguiados.Entretanto,maioressériesdevemserfeitasparacomprovar aseguranc¸a da técnicaparaessespacientes.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theuseofultrasoundisincreasinglypresentintheeveryday lifeofanesthesiologists.Itisusedfordeepveinpuncture, peripheral block or even for neuraxial nerve blocks. The introduction of ultrasoundhas come toadd safety, effec-tiveness,andsuccesstosurgicalprocedures.1
Some benefits of this technique over neurostimulation havebeendemonstratedintheliterature.Amongthese,we highlight lowerincidenceoffailure,lesstimetoperform, shorterlatency,prolongedblockade,andlowerriskof acci-dentalvascularpuncture.2---10Lesslikelytopromotevascular lesions,ultrasound is an interesting tool toguide periph-eralnerveblocks,particularlyinpatientsonanticoagulants or withcoagulation disorders,which impose certain chal-lenges for regionalanesthesia dueto therisk of bleeding complicationsincaseofvascularinjury,especiallyatsites thathindervesselcompression.11
Despite the benefits mentioned, thereis no consensus in the literature regarding the indication of ultrasound-guided peripheral nerve blocks in patients with bleeding disorders. Despite the popularization and development of this technique, there are few cases described in the literature with the use of ultrasound in this type of patient.12
Below, we present a series of cases in which sciatic, femoral,andbrachialplexusnerveblocksguidedby ultra-sound wereperformed in anticoagulated patients, double
aggregatedor withother coagulation disorderswere per-formed.
Case
reports
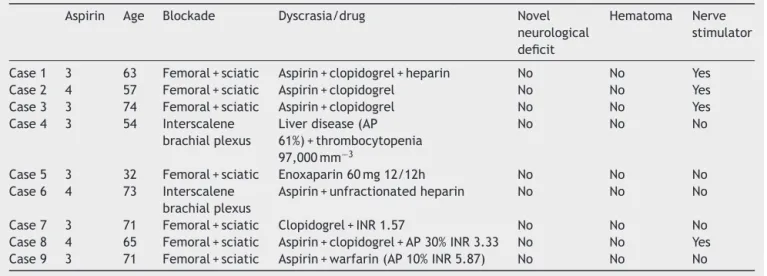
SeeTable1.
Case1
SRR, female, 63 years old, ASA 3, history of systemic hypertension, chronic renal failure in conservative treat-ment, and type 2 diabetes mellitus. The patient was taken piperacillin---tazobactam due to severe focal sepsis on right lower limb, scheduled for transtibial amputa-tion.She wasalsotakenaspirin 100mgday−1, clopidogrel 75mgday−1,unfractionated heparin5000U8/8h, simvas-tatin 20mgday−1, enalapril 20mg 12/12h, glibenclamide 5mg2×day,andmetformin850mg2×day.
Surgicalschedule
Righttranstibialamputation.
Proposedanesthesia
Table1 Summaryofultrasound-guidedperipheralnerveblocksinanticoagulatedpatients.
Aspirin Age Blockade Dyscrasia/drug Novel
neurological deficit
Hematoma Nerve
stimulator
Case1 3 63 Femoral+sciatic Aspirin+clopidogrel+heparin No No Yes
Case2 4 57 Femoral+sciatic Aspirin+clopidogrel No No Yes
Case3 3 74 Femoral+sciatic Aspirin+clopidogrel No No Yes
Case4 3 54 Interscalene
brachialplexus
Liverdisease(AP 61%)+thrombocytopenia 97,000mm−3
No No No
Case5 3 32 Femoral+sciatic Enoxaparin60mg12/12h No No No
Case6 4 73 Interscalene
brachialplexus
Aspirin+unfractionatedheparin No No No
Case7 3 71 Femoral+sciatic Clopidogrel+INR1.57 No No No
Case8 4 65 Femoral+sciatic Aspirin+clopidogrel+AP30%INR3.33 No No Yes
Case9 3 71 Femoral+sciatic Aspirin+warfarin(AP10%INR5.87) No No No
Femoralnerveblockwasperformed,inguinallevelwith 0.375% bupivacaine (10mL), with vasoconstrictor in 1.5% lidocaine (10mL), vasoconstrictor associated with sciatic nerve block, popliteal approach with 0.375% bupivacaine (15mL)andvasoconstrictor,and1.5%lidocaine(15mL)with vasoconstrictor.
The procedure was uneventful. In the postoperative period,thepatientprogressedwithadequate paincontrol andnochangesinsensitivityormotorfunctioninthe terri-toryoftheblockednerves.
Case2
ACR, 57 years old, ASA 4, history of dialysis for chronic renalfailure,chronicatrialfibrillation,hypertension,type 2 diabetes mellitus, and smoker (40packyears−1). The patientwas taking losartan, clonidine, enalapril, nifedip-ine, hydralazine, NPH insulin, in addition to clopidogrel 75mgday−1,andaspirin100mgday−1duetorecentballoon angioplastyinrightposteriortibialartery.
Surgicalschedule
Righttransmetatarsalamputation.
Proposedanesthesia
Ultrasound-guided femoral and sciatic nerve blocks and peripheralnervestimulator.
Femoralnerveblockwasperformed,inguinallevelwith 0.5% ropivacaine (10mL) and 1.5% lidocaine (10mL) with vasoconstrictor associated with sciatic nerve blockade, poplitealapproachwith0.5%ropivacaine(15mL)and1.5% lidocaine(10mL)withvasoconstrictor.
Surgicalprocedurewasuneventful,withdurationof1h and25min under lightsedation. Takentopost-anesthesia careunit (PACU),thepatient evolvedwithadequate pain control and no neurological deficits was seen in the first postoperativeperiod.
Case3
RCB, male, 74 years old, ASA 3, history of systemic hypertensionandperipheral arterialdisease,takenaspirin 100mgday−1 and clopidogrel 75mgday−1 due toleftiliac
arterystent1monthearly.
Surgicalschedule
Lefttranstibialamputation.
Proposedanesthesia
Ultrasound-guided femoral and sciatic nerve blocks and peripheralnervestimulator.
Femoral nerve block was performed, popliteal level, with0.5% ropivacaine(10mL) and1.5%lidocaine (10mL), withvasoconstrictorassociatedwithsciaticnerveblockade, posterior suprapopliteal approach with 0.5% ropivacaine (10mL)and1.5%lidocaine(10mL)withvasoconstrictor.
Surgicalprocedurewasuneventful,withdurationof3h under light sedation. Taken toPACU, the patientevolved withadequatepaincontrolandnoneurologicaldeficitswas seeninthefirstpostoperativeperiod.
Case4
VLBNQ, female, 54 years old, ASA 3 due to liver disease secondarytohepatitisCvirus(HCV)infection,altered coag-ulation (61% prothrombin activity, INR 1.59). Additional testsevidencedplateletcount97,000L−1.Thepatientwas broughttotheoperatingroomforfixationofaleftforearm complexfracture.
Surgicalschedule
Proposedanesthetictechnique
General anesthesia associated with ultrasound-guided brachialplexusblock.
Ultrasound-guidedbrachialplexusblockwasperformed, interscalene approach, with 0.375% bupivacaine with vasoconstrictor(10mL)associatedwith0.25%lidocainewith vasoconstrictor(20mL).
Surgicalprocedurewasuneventful,withdurationof4h and50min.TakentoPACUundersensoryandmotorblock, thepatientevolvedwithadequatepaincontrolandno neu-rological deficitsseen in thefirst postoperative periodat hospitaldischarge.
Case5
FAS,male,32yearsold,ASA3duetothromboangiitis oblit-erans, taking enoxaparin 60mg 12/12h. The patient was broughttotheoperatingroomfordebridementofleft fore-footulcer.
Surgicalschedule
Surgicaldebridementofleftforefootulcer.
Proposedanesthetictechnique
Ultrasound-guidedfemoralandsciaticnerveblocks. Ultrasound-guided sciatic nerve block was performed, poplitealapproach, with0.375%bupivacaine(20mL) with-outvasoconstrictor,associatedwith1.5%lidocaine(20mL) withoutvasoconstrictor.
Surgicalprocedurewasuneventful,withdurationof1h under light sedation. Takento PACU,the patient evolved withadequatepaincontrolandnoneurologicaldeficitsseen inthefirstpostoperativeperiod.
Case6
LHO, female, 73 years old, ASA 4 due to chronic renal failureonhemodialysis,coronaryarterydisease,heart fail-ure, diabetes mellitus, and hypertension.It evolvedwith arteriovenous fistula thrombosis in the left upper limb. BroughttotheoperatingroomforFogarty thromboembolec-tomy.Takingunfractionatedheparinincontinuousinfusion pump,aspirin100mgday−1,isosorbide20mg8/8h,atenolol 50mgday−1,hydralazine50mg12/12h,andregularinsulin.
Surgicalschedule
Fogartythromboembolectomyofleftbrachiocephalic arte-riovenousfistula.
Proposedanesthetictechnique
Ultrasound-guidedbrachialplexusblock
Ultrasound-guidedbrachialplexusblockwasperformed, axillary approach, with0.5% ropivacaine (15mL).Surgical procedurewasuneventful,withdurationof2hand10min
underlight sedation. Taken toPACU, the patient evolved withadequatepaincontrolwithoutneurologicaldeficitsor bruisingseeninthefirstpostoperativeperiodandwas dis-chargedonthethirdpostoperativeperiod.
Case7
Malepatient,71yearsold,ASA3duetosystemic hyperten-sion,type2diabetes mellitus, congestiveheart failureof ischemicetiology(three previousacutemyocardial infarc-tion,underwentcoronaryarterybypasssurgeryin2010;at theproceduretime,withoutangina,dyspnea,orthopnea), dyslipidemia,andsmoker(180pack-years).Taking clopido-grel 75mgday−1 with INR 1.57; chest radiograph showed bilateralcongestionwithcostophrenicsinusopacificationon theright,andmarkedcardiomegaly.
Surgicalschedule
Righttranstibialamputation.
Proposedanesthetictechnique
Ultrasound-guidedfemoralandsciaticnerveblocks. Femoralnerveblockwasperformed,inguinallevel,with 0.5%ropivacaine(10mL) and1.5% lidocaine(10mL) with-outvasoconstrictorassociatedwithsciaticnerveblockwith poplitealapproach,with0.5%ropivacaine(10mL)and1.5% lidocaine(10mL)withoutvasoconstrictor.
Surgicalprocedurewasuneventfulunderlightsedation, withdurationof 1h and15min. At theend of the proce-dure,the patientwastakentothe recoveryroom. Inthe first24haftersurgery,therewerenobleeding,bruising,or novel neurologicaldeficits.Patient showed improvedpain controlinthefirst10haftertheprocedure.
Case8
Male patient, 65 years old, ASA 4 due to exacerbated chronic obstructivepulmonary disease, chronic renal fail-ureonhemodialysis,peripheralarterialdiseaseinthelower limbs,dyslipidemia,hypertension,tobacco(50pack-years) and alcohol consumption. Taking aspirin 100mgday−1, clopidogrel 75mgday−1, captopril 75mgday−1, propra-nolol 80mgday−1, omeprazole 20mgday−1. Preoperative tests:hemoglobina=7.9gdL−1;hematocrits=22.6%; leuko-cytes=13.100L−1; platelets=263.000L−1; prothrombin activity=30%; international normalized ratio=3.39; acti-vatedthromboplastintime=172.4swithnormalizedratioof 6.63;creatinine=6.30mgdL−1;urea=71mgdL−1.Admitted totheinfirmaryforexacerbatedCOPDtreatment; evolved withpaininthelegandleftfoot.Vascularsurgeryfor left footevaluation revealed the presence of necrosis in 1st, 2nd,3rd,and4thtoes andwoundwithinfectious signsin theanteriorregion;emergencyamputationwasindicated.
Surgicalschedule
Proposedanesthesia
Ultrasound-guided femoral and sciatic nerve blocks and peripheralnervestimulator.
Femoralnerveblockwasperformed,inguinallevel,with 0.375%bupivacaine(20mL)withvasoconstrictorassociated with sciatic nerve blockade with subsequent infragluteal approachwithlidocaine1.5%(20mL)without vasoconstric-tor.
Surgicalprocedurewasuneventful,withdurationof1h and45min.The patientwastakentoPACU.Postoperative limbperfusionassessmentwasperformedusingDopplerand neurologicexaminationwasperformedtocheckthemotor responseintheterritoryofthefemoralandsciaticnerves, both within the normal range. On physical examination, therewas nodevelopment of hematoma at the puncture site.Thepatientremainedwithoutpaininthefirst10hafter theblockade.
Case9
Male patient, 71 years old, ASA 3 due to congestive heartfailureofischemicetiology(acutemyocardial infarc-tion, septal and inferior wall, two years ago), atrial fibrillation, chronic arterial disease of the lower limbs, hypertension, former smoker, ex-alcoholic; taking aspirin 100mgday−1,warfarin5mgday−1, captopril150mgday−1,
carvedilol50mgday−1,furosemide80mgday−1,simvastatin 20mgday−1. Preoperative tests: hemoglobina=9.4gdL−1; hematocrit=27.8%; platelet=335,000L−1; prothrombin activity=10%; international normalized ratio=5.84; acti-vatedthromboplastin time=84s; urea=120mgdL−1; crea-tinine=2.17mgdL−1.Patientistakentotheoperatingroom forurgentsurgicalcleaningofrightkneepioarthritis.
Surgicalschedule
Surgicalcleaningofrightknee.
Proposedanesthetictechnique
Ultrasound-guidedfemoralandsciaticnerveblocks. Femoral nerve block was performed, inguinal level, guidedbyultrasoundandperipheralnervestimulator,with 0.375%bupivacaine(20mL)withoutvasoconstrictor associ-atedwithUS-guidedinfraglutealsciaticblockandperipheral nervestimulator,with1.5%lidocaine(20mL)without vaso-constrictor.
Surgicalprocedurewasuneventful,withdurationof1h and30min.Postoperatively,thepatientshowednobruising atthepuncturesiteandthetestshowednomotororsensory changesin theterritory ofthefemoralandsciaticnerves. Thepatientremainedwithoutpaininthefirst12hafterthe blockade.
Therewerenoneurovascularcomplications inthenine reportedcases.Patientswerefollowed-upinthefirst24h aftersurgery,andnonovelneurologicaldeficitorhematoma wasfoundatthepuncturesites.Allprocedureswereguided byultrasound,andnerve stimulatorwasalsousedinfour cases.
Discussion
Withadvancesinmedicine,introductionofnewdrugsand technologies,lifeexpectancyhasincreasedsignificantlyin recent decades. With this advance, it has been observed a higher prevalence of cardiovascular diseases. Thus, it is routine to come across patients taking anticoagulant drugs and/or antiplatelet agents admitted tothe operat-ing room for urgent/emergency surgery. It is known that thediscontinuationofantiplateletdrugs,suchasclopidogrel andaspirin,maybringcomplications.Studiessuggest that aspirin discontinuation increases the incidence of throm-boticeventsin3.4%.13
Althoughspinalhematomais themostseriousbleeding complicationofregionalanesthesiaduetothecatastrophic effect of medullary canal bleeding, not expandable and non-compressible, the risk associated with techniques of plexus and peripheral nerves blocks is not well defined. Thefrequencyandseverityofbleedingcomplicationsafter plexusandperipheralnerveblockshavebeenlittlestudied. However, some reports of serious complications following vascular catheterizationfor surgical, radiological or heart procedureshavebeen describedintheliteratureandmay helpestimatethe riskofsome oftheperipheral blocksin thispopulation.14
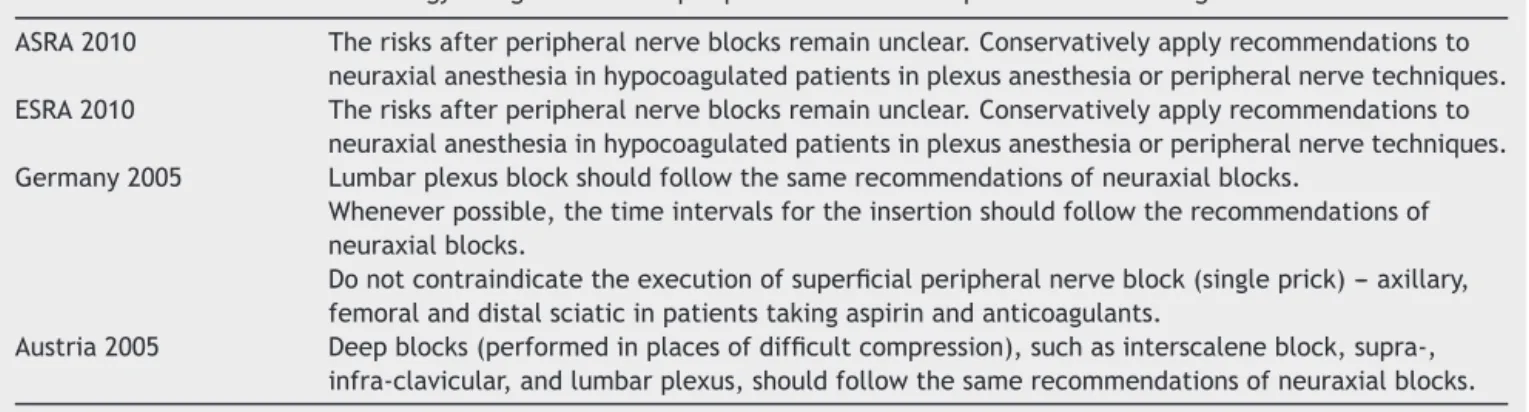
Table2 Societiesofanesthesiologyandguidelinesforperipheralblocksinthepresenceofanticoagulants.
ASRA2010 Therisksafterperipheralnerveblocksremainunclear.Conservativelyapplyrecommendationsto neuraxialanesthesiainhypocoagulatedpatientsinplexusanesthesiaorperipheralnervetechniques. ESRA2010 Therisksafterperipheralnerveblocksremainunclear.Conservativelyapplyrecommendationsto
neuraxialanesthesiainhypocoagulatedpatientsinplexusanesthesiaorperipheralnervetechniques. Germany2005 Lumbarplexusblockshouldfollowthesamerecommendationsofneuraxialblocks.
Wheneverpossible,thetimeintervalsfortheinsertionshouldfollowtherecommendationsof neuraxialblocks.
Donotcontraindicatetheexecutionofsuperficialperipheralnerveblock(singleprick)---axillary, femoralanddistalsciaticinpatientstakingaspirinandanticoagulants.
Austria2005 Deepblocks(performedinplacesofdifficultcompression),suchasinterscaleneblock,supra-, infra-clavicular,andlumbarplexus,shouldfollowthesamerecommendationsofneuraxialblocks.
Some societies, suchastheAustrianand German Soci-eties of Anesthesiology explicitly differentiate superficial nerve,deepperipheral, andneuraxialblocks.Ofthefirst, theaxillary,femoral,anddistalpoplitealmaybeperformed inthepresenceofanticoagulation(Table2).21
Furthermore,another factorthat shouldbeconsidered in peripheral nerve blocks in anticoagulated patients is theuseofultrasound.Meta-analysiscomparing ultrasound-guided peripheral nerveblock withthe classictechniques (paresthesia and neurostimulation) demonstrated a lower incidence of vascular puncture in cases with the aid of ultrasound.8
Thus, in our institution a protocol was established in which peripheral blocks are considered in anticoagulated patientsinthefollowingsituations:
Superficial blockage and of easy compression site; for example: axillary, interscalene, femoral, saphenous, popliteal.
Blockadesmustbeguidedbyultrasoundandmustbe per-formedbyananesthesiologistwithextensiveexperiencein guidednerveblocks.
Therefore,takingintoaccountthebenefitsof ultrasound-guided peripheral nerve puncture, as well as some characteristics of some routes for blockade, such as the depthandthepossibilityofcompression, someperipheral nerveblocksmaybecameasafeoptioninpatientswith pri-maryorsecondaryblooddyscrasias.However,largerseries shouldbeconductedtoprovethesafetyofthe technique forthesepatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.RandoK,Castelli J,PrattJP, etal. Ultrasound-guided inter-naljugularveincatheterization:arandomizedcontrolledtrial. HeartLungVessel.2014;6:13---23.
2.KapralS,GreherM,HuberG,etal.Ultrasonographicguidance improvesthesuccessrateofinterscalenebrachialplexus block-ade.RegAnesthPainMed.2008;33:253---8.
3.PerlasA,BrullR,ChanVWS,etal.Ultrasoundguidanceimproves thesuccess ofsciaticnerveblockatthepoplitealfossa. Reg AnesthPainMed.2008;33:259---65.
4.SauterAR,DodgsonMS,StubhaugA,etal.Electricalnerve stim-ulationorultrasoundguidanceforlateralsagittalinfraclavicular blocks:arandomized,controlled,observer-blinded, compara-tivestudy.AnesthAnalg.2008;106:1910---5.
5.ChanVW,PerlasA,McCartneyCJ,etal.Ultrasoundguidance improvessuccessrateofaxillarybrachialplexusblock.CanJ Anaesth.2007;54:176---82.
6.Domingo-Triado V, Selfa S, Martınez F, et al. Ultrasound guidanceforlateralmidfemoralsciaticnerveblock:a prospec-tive,comparative,randomizedstudy.AnesthAnalg.2007;104: 1270---4.
7.WilliamsSR,ChouinardP,ArcandG,etal.Ultrasoundguidance speedsexecutionand improvesthequalityofsupraclavicular block.AnesthAnalg.2003;97:1518---23.
8.AbrahamsMS,AzizMF,FuRF,etal.Ultrasoundguidance com-pared with electrical neurostimulation for peripheral nerve block: asystematic reviewand meta-analysis ofrandomized controlledtrials.BrJAnaesth.2009;102:408---17.
9.WarmanP,NichollsB.Ultrasound-guidednerveblocks:efficacy andsafety.BestPractResClinAnaesthesiol.2009;23:313---26.
10.Koscielniak-Nielsen ZJ. Ultrasound-guided peripheral nerve blocks: what are the benefits? Acta Anaesthesiol Scand. 2008;52:727---37.
11.Ferraro LHC, Tardelli MA, Yamashita AM, et al. Bloqueio dos nervos femoral e isquiático guiados por ultrassom em pacienteanticoagulado.Relatodecasos.RevBrasAnestesiol. 2010;60:422---8.
12.Bigeleisen PE. Ultrasound-guided infraclavicular block in an anticoagulated and anesthetized patient. Anesth Analg. 2007;104:1285---7;
KhelemskyY,RosenblattMA.Ultrasound-guidedsupraclavicular blockinapatientanticoagulatedwithargatroban.PainPract. 2008;8:152.
13.MaulazAB,BezerraD,MichelP,etal.Effectofdiscontinuing aspirintherapyontheriskofbrainisquemicstroke.ArchNeurol. 2005;62:1217---20.
14.HorlockerTT,WedelDJ,RowlingsonJC,etal.Regional anes-thesiainthepatientreceivingantithromboticorthrombolytic therapy: American Society of Regional Anesthesia and Pain MedicineEvidence-BasedGuidelines(ThirdEdition).RegAnesth PainMed.2010;35:64---101.
15.Fransson SG, Nylander E. Vascular injury following cardiac catheterization, coronary angiography, and coronary angio-plasty.EurHeartJ.1994;15:232---5.
16.ChellyJE,SzczodryDM,NeumannKJ.Internationalnormalized ratioandprothrombintimevaluesbeforetheremovalofa lum-barplexuscatheterinpatientsreceivingwarfarinaftertotal hipreplacement.BrJAnaesth.2008;101:250---4.
underwentlumbarplexusblockandwerelateranticoagulated. Anesthesiology.2003;98:581---5.
18.Bicker P, Brandes J, Lee M, et al. Bleeding complications from femoraland sciaticnerve cathetersin patients receiv-ing low molecular weight heparin. Anesth Analg. 2006;103: 1036---7.
19.KleinSM,D’ErcoleF,GreengrassRA,etal.Enoxaparin associ-atedwithpsoashematomaandlumbarplexopathyafterlumbar plexusblock.Anesthesiology.1997;87:1576---9.
20.WelleR, Gerancher JC, Crews J, et al. Extensive retroperi-tonealhematomawithoutneurologicdeficitintwopatientswho underwentlumbarplexusblockandwerelateranticoagulated. Anesthesiology.2003;98:581---5.