Case R eport
Use of a platysma myocutane ous flap for the re implantation
of a se ve re d e ar: e xpe rie nce with five case s
Department of Surgery, Orthopedics and Traumatology,
Faculdade de Medicina de Ribeirão Preto, University of São Paulo, São Paulo, Brazil
Francisco Veríssimo de Mello-Filho Rui Celso Martins Mamede Adilon Passinho KouryINTRODUCTION
The traumatic lo ss o f an ear g reatly affects the pa tient b ec a use o f the severe a esthetic defo rmity it entails. The characteristic fo rmat o f the ear, with a fine skin co vering a thin and elastic cartilag e, is no t fo und anywhere else in the human bo dy. Thus, to reco nstruct an ear, the surg eo n may try to imitate it by sculpting cartilag e and co vering it with skin. W ith a few ho no rable exceptio ns, the results are usually unsatisfacto ry. O n this basis, the mo st lo g ical pro cedure wo uld be to preserve the severed ear and reimplant it. Ho wever, the surg ical salvag e o f a severed ear is quite difficult, as co nfirmed by the frequent unsatisfacto ry results repo rted. The simple implantatio n o f the ear at its o rig inal site a s a c o mpo und g ra ft usua lly le a ds to ne c ro sis, w ith a to ta l lo ss o f the o rg a n. Furthermo re, lo ss o f skin o f the auricular reg io n co mmo nly o ccurs in these accidents, to g ether with lo cal co ntaminatio n, a fact that ends up d isc o ura g ing a ny a tte mp t a t imme d ia te reco nstructio n. The severed ear may also suffer severe skin lo sses and defo rming lesio ns o f the c a rtila g e , le a d ing the surg e o n to o p t fo r discarding the o rg an.
W e pro po se here the use o f a platysma
ABSTRACT
Contex t: The traumatic lo ss o f an ear greatly affects the patient because o f the severe aesthetic defo rmity it entails. The characteristic fo rmat o f the ear, with a fine skin co vering a thin and elastic cartilage, is no t fo und anywhere else in the human bo dy. Thus, to reco nstruct an ear, the surgeo n may try to imitate it by sculpting cartilage and co vering it with skin.
O bjective: To use a platysma myo cutaneo us flap fo r the reimplantatio n o f a severed ear in humans.
Design: Case repo rt.
Setting: Emergency unit o f the university ho spital, Faculty o f Medicine, Ribeirão Preto - USP.
Ca se Report: Five cases are repo rted, with who le ear reimplantatio n in 3 o f them and o nly segments in 2 cases. The surgical technique used was o riginal and was based o n the principle o f auricular cartilage revascularizatio n using the platysma muscle. W e implanted traumatically severed auricular cartilage into the platysma muscle. The prefabricated ear was later transferred to its o riginal site in the fo rm o f a myo cutaneo us-cartilagino us flap. O f the 5 cases treated using this technique, 4 were successful. In these 4 cases the reimplanted ears sho wed no sho rt- o r lo ng-term pro blems, with an aesthetic result quite clo se to natural appearance. In o ne case there was necro sis o f the entire flap, with to tal lo ss o f the ear. The surgical technique described is simple and utilizes the severed ear o f the patient. Its applicatio n is excellent fo r skin lo sses in the auricular regio n o r fo r the ear itself, thus o bviating the need fo r micro surgery o r the use o f pro theses o r grafts.
myo cutaneo us flap fo r the reimplantatio n o f a severed ear in two surgical steps.
CASES REPORT
Patients. Five patients who had suffered partial o r to tal traumatic avulsio n o f an ear were seen at the emerg ency unit o f the university ho spital o f the Faculty o f Medicine o f Ribeirão Preto , University o f Sao Paulo . The characteristics o f the patients are listed in Table 1 . After the initial care pro vided fo r all po lytraumatiz ed patients, specific treatment was started fo r the preservatio n o f auricular cartilage (AC).
Surg ic a l te c hniq ue . During the first o perative phase, the severed ear was washed with 0 .9 % so dium chlo ride and disinfected with 1 0 % po lyvinylpyrro lido ne io dine. The entire skin c o ver wa s then dissec ted a nd the ea r wa s remo ved, with skeleto niz atio n o f AC. W hen fractures or lesions of AC were present, they were co rrected using co lo rless mo no nylo n 5 -0 sutures, thus establishing the o riginal architecture o f the o rgan. Exhaustive irrigatio n o f the entire AC with 0 .9 % so dium chlo ride was then perfo rmed under pressure. After this preparatio n, the pro cedure o f AC implantatio n in the supraclavicular fo ssa was started o n the same side as the lesio n.
An incisio n o f appro ximately 8 cm was made in the supraclavicular fo ssa parallel to the clavicle and the platysma muscle was identified (Fig. 1 , incisio n A). The skin o f the regio n was detached fro m the muscle by blunt dissectio n until a po cket was created that co uld acco mmo date the AC, at a distance o f at least 3 cm abo ve the incisio n made in the skin. The AC was intro duced so tha t its la te ra l surfa c e fa c e d the skin, hemostasis was revised, the skin was sutured with
simple stitches, a slightly co mpressive dressing was applied, and the pro cedure was terminated (Fig. 1 ).
The seco nd surgical step was started after full patient reco very and full healing o f the auricular regio n. The patient was then prepared fo r ear reimplantatio n.
The skin and platysma were sectio ned alo ng the entire leng th o f the muscle by an incisio n o n the supraclavicular scar o f the first surg e ry (Fig . 1 , inc isio n A). Sub p la tysma l undermining was then perfo rmed alo ng the co vering fascia o f the muscle until the lo wer margin o f the mandible was reached. Ano ther incisio n, o nly in the cervical skin immediately abo ve the site o f AC implantatio n, was then perfo rmed to create a skin ellipse at the site (Fig. 2, incision B). Using blunt dissection, the platysma skin was detached fro m incisio n B to the lo wer margin o f the mandible. Incisio n A was then sutured to incisio n B with mo no nylo n 5 -0 sutures. Thus, the AC was envelo ped by the skin in a pedicled island in the platysma muscle, with the co nstructio n o f a co mpo und platysma cartilage-muscle-skin flap (PCMSF) (Fig. 2 ). Ano ther 8 cm incisio n (Fig. 3 , incisio n C) was then perfo rmed at the site where the ear wo uld be implanted, and the skin was detached fro m the auricular reg io n to the previo usly undermined cervical re g io n, fo rming a n a mp le c o mmunic a tio n between areas.
The PCMSF was ro tated 1 8 0o under the cervical skin and transpo rted to the regio n o f ear implantatio n (Fig. 3 ), where it was fixed with simple mo no nylo n 5 -0 sutures. The do no r area was primarily clo sed with simple mo no nylo n 5 -0 sutures and a drain with co ntinuo us aspiratio n was intro duced (Figure 4 A).
Ta ble 1 - Pa tient number, a ge, side of severed ea r, da te of a ccident, ca use of a vulsion a nd type of a vulsion
Patient Age Side Cause Type
1 9 years Right Automobile accident Total
2 1 1 years Right Dog bite Partial (upper half)
3 2 4 years Right Automobile accident Total
4 2 0 years Right Automobile accident Total
Figure 4 B sho w the results o btained after reimplantatio n o f a to tally severed and partially severed ear, respectively, using a PCMSF. The results are summarized in Table 2 .
DISCUSSION
Several treatment mo dalities fo r fully o r partially severed ears are currently being used. Ho wever, no ne o f them appears to have so lved the pro blem in a definitive manner. Successful simple repositioning of severed portions has been repo rted bo th in cases o f partial1 ,2 and to tal3 lo sses. Ho wever, in clinical practice, success is rarely o btained with this pro cedure unless the severed segment has a reaso nable skin pedicle. O f the five cases in which we used PCMSF, o nly o ne presented to tal necro sis after reimplantatio n (Table 2 ). This lack o f success was attributed to a possible lesion of the dominant vascular pedicle o f the platysma, co nsisting o f the submental artery, a branch o f the facial artery.4
Micro surgical ear reimplantatio n was first perfo rmed o n a human being in 1 9 8 0 .5 Despite the excellent results repo rted and the natural aspect o f a micro surgically reimplanted ear, the small caliber o f auricular vessels implies great technical difficulties, which limit the metho d to specialized centers and selected cases. In an attempt to o verco me the technical limitatio ns o f micro surgical anasto mo sis in the very fine vessels o f the ear, Sucur et al6 pro po sed the implantatio n o f deepithelializ ed AC into a subcutaneo us pocket on the forearm, which has vessels of larger caliber, in o rder to facilitate the pro cedure o f micro surgical transfer. W ith the use o f a PCMSF we eliminated all the technical difficulties o f
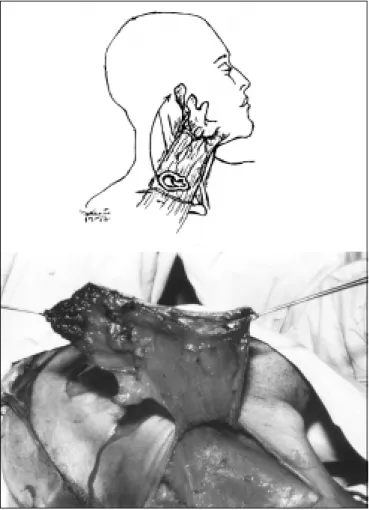
Fig. 1 - Preoperative stage of the second surgical
step. Note the absence of the upper half of the patient’s right ear, which is located in the supraclav-icular fossa. 1-A: Schematic illustration of the inci-sion used to introduce the auricular cartilage into the supraclavicular fossa. 1-B: Photograph of the auricular cartilage (arrow) under the cervical skin.
Fig. 2 - Intraoperative stage of the second surgical
step. 2-A: Schematic illustration of the incisions (a, b and c) performed for PCMSF transfer from the su-praclavicular region to the original site of the ear. 2-B: Close-up of the PCMSF before transfer.
Ta ble 2 - Pa tient number, time until
fla p tra nsfer a nd fina l result
Patient Time(months) Final result
1 14 Reimplanted ear without complications 2 2 Reimplanted ear without complications 3 4 Reimplanted ear without complications
4 4 Total loss due to flap necrosis
Fig. 3. Intraoperative stage of the second surgical step. 3-A: Schematic illustration of the 180o rotation performed with the PCMSF under the cervical skin. 3-B: Photograph of the PCMSF attached only to the mandible and ready for transfer.
Fig. 4. Postoperative stage. 4-A: Schematic illustration of the PCMSF transferred to the site of the ear, with the donor area closed. 4-B: Final aspect of the procedure.
micro surgery, thus permitting reimplantatio n o f fully o r partially severed ears in a pro cedure that c a n b e e xe c ute d in a ny e me rg e nc y unit. Furthermore, the skin of the supraclavicular region is practically identical to that o f the ear in terms o f co lo r, thickness and absence o f hair, thus pro viding the natural aspect o f the o riginal shape by clo sely adapting to the varying relief o f the AC.
The use o f an external pro sthesis sho uld be limite d to se le c te d c a se s b e c a use o f the inco nvenience o f fixatio n and exchange. Even bo ne-integrated pro stheses sho uld be limited to p o o rly c o o p e ra ting p a tie nts w ho ha ve no po ssibility o f using their o wn cartilage, since the greatest disadvantage o f the metho d is no t using the tissue o f the patient himself.7 W ith the PCMSF, o nly the patient’s o wn tissue is used and in a definitive manner, with minimal sequels in the do no r area, represented by a cervical scar.
The ide a o f sa ving a se ve re d e a r b y keeping the cartilage skeleton for later positioning go es back quite a lo ng time. The cartilage may be skeleto nized and implanted into a skin po cket in the auricular reg io n itself, o r the variatio n pro po sed b y Mla dic k et a l.8 ma y b e used, whereby the cartilage po rtio n is buried witho ut skeleto niz a tio n b ut a fter derma b ra sio n. The pro b le m with the se te c hniq ue s is tha t the ir executio n requires the presence o f intact skin in the ear regio n fo r implantatio n, o r that the ear itself be co vered with tegument. W ith the PCMSF, o nly the AC is used, being implanted into a pocket under the skin of the supraclavicular fossa. Thus, a skin lo ss in the e a r re g io n due to mechanical, thermal o r chemical trauma o r even due to severe lo cal co ntaminatio n do es no t pre ve nt the use o f this te c hniq ue . Ano the r disadvantage o f burying the severed ear in the auricular regio n is its later repo sitio ning. It is necessary to use skin grafts o r flaps to co ver the median surface o f the AC, a fact that may cause disto rtio ns o f the cartilag e itself o r scarring retractio ns that mo dify its po sitio ning. Since the PCMSF has a lo ng muscle pedicle, it can be easily implanted witho ut tensio n. The skin o f the supraclavicular regio n o ffers ample co verage o f
o r flaps.
The platysma muscle is fixed to the posterior surface o f the AC, g uaranteeing a vascular supply and a generous amount of skin that insures its implantatio n free fro m hairs.
Although in the presented study we waited a long time before reimplanting the ears (Table 2), we believe that this lo ng perio d o f time is no t necessary. The ability of a muscle to neovascularize cartilage has been well established. The study of neovascularization of the cartilage of the trachea with the sterno hyo id muscle sho wed that safe neovascularization of the cartilage occurred after 21 days, permitting reimplantation after this time.9
After the pio neering study o f Futrell et al1 0 using a myo cutaneo us platysma flap fo r intrao ral reco nstructio n, this type o f flap was successfully used fo r the reco nstructio n o f o ther regio ns such as the lip1 1 and trachea.1 2 Fo r ear reco nstructio n we fo und o nly o ne case published by Arian,1 3 in which the platysma myo cutaneo us flap was used as a “ sandwich” with an o uter muscle-cutaneo us pedicle and tubulated to co ver the auricular regio n that had lo st the skin. The no vel feature o f the technique described here is the use o f a platysma myo cutaneo us flap with a vascular pedicle in the facial artery and o nly a skin island at the end fo r receiving and neo vascularizing the AC, which was later transpo rted to the site o f o rigin.
The surgical reco nstructio n o f an ear is a difficult task and the results are po o r. The fact that the final result lo o ks like an ear o nly because o f its lo catio n is disco uraging.1 4 Thus, the AC o f the pa tie nt sho uld a lwa ys b e pre se rve d to guarantee appro priate reco nstructio n.
The advantages o f the use o f a PCMSF fo r ear reimplantatio n are: the simplicity o f surgical technique, which can be applied to to tally o r partially severed ears, dispensing with the need fo r micro surg ical techniques and g rafts; the po ssibility o f saving the ear cartilage regardless o f the co nditio ns o f the area o f the ear itself; the pro visio n o f skin tissue identical to that o f the ear; the achievement o f a stable and adequate aesthetic result with the absence o f hairs.
The disadvantages o f the RCMPC are: the
need fo r two surgical steps; the o ccurrence o f a scar in the supraclavicular do no r reg io n; the po ssibility o f flap necro sis with a to tal lo ss o f the implanted ear.
REFERENCES
1. Gilfo rd GH Jr. Replantatio n o f severed part o f an ear. Plast Reco nstr
Surg 1972; 49:202-2.
2. Lewis EC II, Fo wler JR. Two replantatio ns o f severed ear parts. Plast
Reco nstr Surg 1979; 64:703-5.
3. Salyapo ngse A, Maun LP, Suthunyarat, P. Successful replantatio n o f
a to tally severed ear. Plast Reco nstr Surg 1979; 64:706-8.
4. Hurwitz DJ, Ro bso n JA, Futrell JW. The anato mic basis fo r the platysma
skin flap. Plast Reco nstr Surg 1983; 72:302-14.
5. Penningto n DG, Pelly AD. Successful replantatio n o f a co mpletely
avulsed ear by micro vascular anasto mo sis. Plast Reco nstr Surg1980;
65:820-3.
6 Sucur S, Ninko vic M, Marko vic S, et al. Reco nstructio n o f an
avulsed ear by co nstructing a co mpo site free flap. Br J Plast Sur 1991; 44:153-4.
7. Wilke s GH, Wo lfaardt JE. Osse o inte grate d allo plastic ve rsus
auto geno us ear reco nstructio n: criteria fo r treatment selectio n. Plast
Reco nstr Surg1994; 93:967-79.
8. Mladick RA, Ho rto n CE, Adamso n JE, et al. The po cket principle? A
new technique fo r the reattachment o f a severed ear part. Plast Reco nstr Surg 1971; 48:219-23.
9. Me llo - Filho FV, Mam e d e RCM, Ve llud o MASL. Trac he al
neo vascularizatio n: a metho d invo lving mo bilizatio n o f a co mplete tracheal neo vascularizatio n segment using a sterno hyo id muscle
flap. Laryngo sco pe1996; 106:81-5.
10. Futrell JW, Jo hns ME, Edgerto n MT, et al. Platysma myo cutaneo us
flap fo r intrao ral reco nstructio n. Am J Surg 1978; 136:504-7.
11. Mello -Filho FV, Mamede RCM. Reco nstructio n o f the lo wer lip with
a platysma myo cutaneo us flap. Acta Onco l Bras1992; 12:119-22.
12. Mello -Filho FV, Mamede RCM, Sader AA, et al. Use o f the platysma
m yo c utane o us flap fo r c e rvic al trac he al re c o nstruc tio n: an
experimental study in do gs. Laryngo sco pe1993; 103:1161-7.
13. Arian S, Chicarelli ZN. Replantatio n o f a to tally amputated ear by
means o f a platysma musculo cutaneo us “sandwich” flap. Plast
Reco nstr Surg1986; 78:385-9.
14. Brent B, Byrd SS. Seco ndary ear reco nstructio n with cartilage grafts
co vered by axial, rando m and free flaps o f tempo parietal fascia. Plast
Reco nstr Surg1983; 72:41-51.
Ack now ledgm ents - W e are grateful to Dr. Ro dio Luis Brandão Camara, a po stgraduate student in the
Department o f Surgery, O rtho pedics and Traumato lo gy o f this Institutio n, fo r devising the illustratio ns used in the present paper.
Fra ncisco Veríssim o de M ello-Filho - MD, PhD. Department o f Surg ery, O rtho pedics and Traumato lo g y, Faculty o f Medicine o f Ribeirão Preto , University o f São Paulo .
Rui Celso M a rtins M a m ede - MD, PhD. Department o f Surgery, O rtho pedics and Traumato lo gy, Faculty o f Medicine o f Ribeirão Preto , University o f São Paulo .
Sources of funding: N o t declared
Conflict of interest: No t declared
La st received: 1 6 No vember 1 9 9 8
Accepted: 1 0 February 1 9 9 9
Address for correspondence:
Francisco Veríssimo de Mello -Filho
Departamento de Cirurgia, O rto pedia e Traumato lo gia da Faculdade de Medicina de Ribeirão Preto , USP
Ribeirão Preto / SP - Brasil - CEP 1 4 0 4 9 -9 0 0 E-mail: fdmfilho @ fmrp.usp.br
RESUMO
Contex to: A perda da orelha por trauma produz inconformismo no paciente pela grave deformidade estética que acarreta. O formato característico da orelha, com uma fina pele de revestimento sobre uma delgada e elástica cartilagem, não pode ser encontrado em outros locais de nosso corpo. Portanto, para reconstruir uma orelha, resta aos cirurgiões a tentativa de imitá-la, esculpindo cartilagens e revestindo-as com pele. Objetivos: Utilizar o retalho miocutâneo do platisma para reimplantação de orelha amputada em humanos. Tipo de estudo: Relato de casos. Local: Unidade de Emergência do Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo. Relato de casos: Cinco pacientes foram operados, sendo reimplantada a orelha toda em três e, em dois casos, apenas segmentos. A técnica cirúrgica empregada é original, baseado no princípio da
revascularização da cartilagem auricular pelo músculo platisma. Implantamos a cartilagem auricular amputada no músculo platisma, homolateral à amputação. Posteriormente, foi realizada a transferência da orelha pré-fabricada para seu local original sob a forma de retalho cartilágeno-músculo-cutâneo e descrita detalhadamente. Dos cinco casos tratados, obteve-se sucesse em quatro. A reimplantação da orelha não apresentou problemas com resultado estético muito próximo do natural. Em um caso ocorreu necrose de todo retalho com perda total da orelha. A técnica cirúrgica aplicada é simples e aproveita a própria orelha amputada do paciente. É excelente sua aplicação nas perdas de pele da região auricular ou da própria orelha, prescindindo-se da utilização de técnica microcirúrgica ou do uso de prótese ou enxerto.