www.revportcardiol.org
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
ORIGINAL
ARTICLE
Infective
endocarditis:
Surgical
management
and
prognostic
predictors
Rita
Ilhão
Moreira
a,∗,
Madalena
Coutinho
Cruz
a,
Luísa
Moura
Branco
a,
Ana
Galrinho
a,
Luís
Coutinho
Miranda
b,
José
Fragata
b,
Rui
Cruz
Ferreira
aaServic¸odeCardiologia,HospitaldeSantaMarta,CentroHospitalardeLisboaCentral,Lisboa,Portugal
bServic¸odeCirurgiaCardiotorácica,HospitaldeSantaMarta,CentroHospitalardeLisboaCentral,Lisboa,Portugal
Received16January2017;accepted5August2017 Availableonline3May2018
KEYWORDS Infective endocarditis; Surgery; Prognosis Abstract
IntroductionandAim:Infectiveendocarditis(IE)isassociatedwithhighmorbidityand mortal-ity.Itisimportanttodeterminewhichfactorsincrease theriskofpooroutcomeinorderto enableearlydetectionandaggressivetreatment,includingsurgery.Theaimofourstudywas toidentifyfactorspredictingcomplicationsandin-hospitalmortalityinpatientswithIEandto analyzeconditionspredisposingtosurgeryanditsoutcome.
Methods:WeperformedaretrospectivestudyincludingpatientswithIEwhounderwent trans-esophagealechocardiographyinatertiaryhospitalcenter(2006-2014).
Results:Atotalof233patientswereanalyzed(69.1%male;meanage63.4±15.2years;mean follow-up28.4±30.7months).Thecomplicationratewas56.6%andin-hospitalmortalitywas 16.3%.Independentpredictorsofmortalitywerechronicobstructivepulmonarydisease (OR 4.89;CI1.36-17.63;p=0.015),clinicalcoursecomplicatedbycerebralembolism(OR9.38;CI 3.26-26.96;p<0.001),andIEduetoStaphylococcusspp.(OR3.78;CI1.32-10.85;p=0.014)and non-HACEKGram-negativebacilli(OR12.85;CI2.61-63.23;p=0.002).Surgerywasperformed in36.9%.Thisgrouphadhigherpercentagesofmales,youngerpatients,aorticvalveIE,large vegetations,perivalvularextension,severevalvularregurgitationandheartfailure.Inpatients withsurgicalindication(n=133),thosewhounderwentsurgeryhadlowerin-hospitalmortality (15.5%vs.32.6%,p=0.028)andbetterlong-termsurvival(log-rankp=0.029).
Conclusion:TheresultsofthisstudymayhelptoidentifyIEpatientswhoareatincreasedrisk ofworseoutcome,offeringtheopportunitytochangethecourseofthediseaseandtoimprove prognosiswithearlierandmoreaggressiveintervention.
©2018SociedadePortuguesa deCardiologia.Publishedby ElsevierEspa˜na,S.L.U.All rights reserved.
∗Correspondingauthor.
E-mailaddress:[email protected](R.IlhãoMoreira).
https://doi.org/10.1016/j.repc.2017.08.007
0870-2551/©2018SociedadePortuguesadeCardiologia.PublishedbyElsevierEspa˜na,S.L.U.Allrightsreserved.
PALAVRAS-CHAVE
Endocardite infeciosa; Cirurgia; Prognóstico
Endocarditeinfeciosa:tratamentocirúrgicoepreditoresprognósticos Resumo
Introduc¸ãoeobjetivo: A endocardite infeciosa (EI) está a associada a elevada morbi-mortalidade. Torna-seimportantedefinir osfatores queaumentam orisco deum desfecho desfavoráveldemodoatratardeumaformaprecoceeagressiva,incluindotratamento cirúr-gico.Oobjetivodesteestudofoiidentificarfatorespreditivosdecomplicac¸õesemortalidade intra-hospitalaremdoentescomEIeanalisarascondic¸õespredisponentesparacirurgiaeoseu resultado.
Métodos: EstudoretrospetivoqueincluiudoentescomEI quefizeramecocardiograma trans-esofágiconumcentrohospitalarterciário(2006-2014).
Resultados: Foram avaliados 233 pacientes (69,1% homens; idade média 63,4±15,2 anos; follow-up médio 28,4±30,7 meses). A taxa de complicac¸ões foi 56,6% e mortalidade intra-hospitalar 16,3%. Preditores independentes de mortalidade foram doenc¸a pulmonar obstrutivacrónica(OR4,89;CI1,36-17,63;p=0,015),emboliacerebral(OR9,38;CI3,26-26,96; p<0,001) e EI por Staphylococcus spp. (OR 3,78; CI 1,32-10,85; p=0,014) e bacilos Gram-negativosnãoHACEK(OR12,85;CI2,61-63,23;p=0,002).Fez-secirurgiaem36,9%.Essegrupo apresentavamaiorpercentagemdehomens,jovens,EIdaválvulaaórtica,vegetac¸õesgrandes, extensão perivalvular,regurgitac¸ão valvular grave einsuficiência cardíaca.No subgrupo de doentescomindicac¸ãocirúrgica(133),aquelessubmetidosacirurgiativeramumamortalidade intra-hospitalarmenor(15,5%versus32,6%,p=0,028)emelhorsobrevidaemlongoprazo (log-rankp=0,029).
Conclusão:OsresultadosdesteestudopodemajudaraidentificardoentescomEIque apresen-tammaiorriscodeumdesfechodesfavorável,permitemalterarocursodadoenc¸aemelhorar oprognósticoatravésdeumaintervenc¸ãomaisprecoceeagressiva.
©2018SociedadePortuguesadeCardiologia.PublicadoporElsevierEspa˜na,S.L.U.Todosos direitosreservados.
Introduction
The challenges associated withinfective endocarditis (IE) aregreaterthanever.The patientsaffectedareolderand sickerthaninthepast,andoftenhavemanycomorbidities.1
The role of surgeryin active IEhas expanded progres-sively,andnowadaysalmosthalfofpatientswithIEundergo surgery.2 Therearethreemainindications: valve
dysfunc-tionleadingtoheartfailure,uncontrolledinfection,andfor preventionofembolism.
Despiteimprovementsinmanagement,IEisstill associ-atedwithhighmortalityandseverecomplications.Prognosis is influenced by many factors and early identification of high-riskpatientsmaychangethecourseofthediseaseand improveoutcome.
The aimofthisstudywastoidentifyfactorspredicting in-hospitalmortalityandcomplicationsandtoanalyze con-ditionspredisposingtosurgicaltherapyanditsoutcomein asingletertiaryhospitalwithfacilitiesforsurgicaltherapy.
Methods
Studypopulation
All patients who underwent transesophageal echocardio-graphy in a tertiary hospital center with cardiac surgery facilities due to suspicion of IE and diagnosed with IE
between 2006 and 2014 were recorded in a uniform database.
The study included casesfrom ourhospital,as well as fromcommunityandreferralhospitals.
Criteriaanddefinitions
Patientswere included iftheymetcriteriafor definite or possible IE(if considered and treated as endocarditis) by the modified Dukecriteria.3 Patientswithcardiac
device-relatedIEwereexcluded.
In-hospital mortality was defined as all in-hospital deaths, includingpatients transferredtoother acutecare facilities.
The complications analyzed were heart failure, perivalvular extension, and cerebral and peripheral embolism. Perivalvular extension was defined by the presenceofabscesses,pseudoaneurysmsorfistulae.
Regarding timing, prosthetic valve endocarditis was definedasearlyifitoccurredwithin12monthsofprevious surgery. Surgicaltherapywasdefinedasearlyifthe inter-ventionwasperformedwithinsevendaysofdiagnosis,and lateifperformedthereafter.
Indicationsforsurgerywereinaccordancewiththe cur-rentEuropeanSocietyofCardiologyguidelines.4Follow-up
datawereobtainedbyreviewofmedicalrecords,outpatient clinicalvisits,andtelephonecontact.
Ethicalandhospitalpermissionswereobtainedfromthe appropriatelocalauthorities.
Statisticalanalysis
Descriptiveresultsareexpressedasmeans±standard devi-ationormedians(interquartilerange).Categoricalvariables areexpressedasabsolutenumbersandproportions. Inferen-tialstatisticsusingparametricornonparametrictestswere used asappropriate for the type of data. The chi-square test or Fisher’sexact test were used toanalyze all cate-goricalvariables.The Student’sttestwasusedtoanalyze continuousvariableswithanormaldistribution.
Statistical significance was established at a two-tailed levelof<5%.Factorsassociatedwithmortalityonunivariate analysiswereenteredintoamultivariatestepwiselogistic regression model. The cumulative mortalityrate was cal-culated usingtheKaplan-Meiermethod.Allanalyses were performed withSPSSfor Windows,version22.0(IBMSPSS, Inc.,Chicago,IL,USA).
Results
Intotal,233patientswerediagnosedwithIEduringthestudy period,ofwhom108(46.4%)caseswereconsideredas defi-niteand125(53.6%)aspossibleIEaccordingtothemodified Dukecriteria. The meanagewas63.4±15.2years(range: 13-89)and161weremale.
Baseline characteristics, comorbidities, echocardio-graphic findingsandisolatedmicroorganismsareshown in
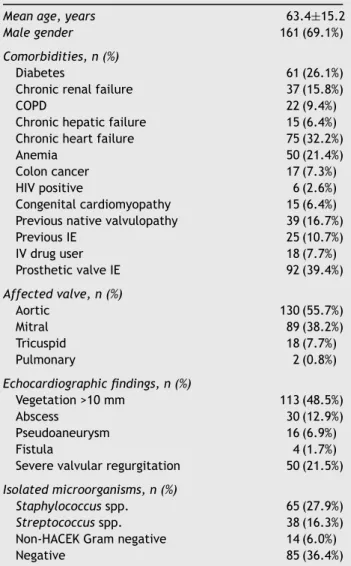
Table 1. A substantial proportion of the population were affectedbycomorbidities,themostfrequentbeingchronic heartfailureanddiabetes(32.2%and26.1%,respectively), whilethemostcommonpredisposingconditionwasthe pres-enceofaprostheticvalve,with22.7%beingconsideredearly prostheticvalveIE.
The aortic valve wasmost often affected, in 55.7% of cases,followed bythemitralvalve, with7.7%of patients having both aortic and mitral valve involvement. Though right-sidedIEwasmorefrequentinintravenousdrugusers (p=0.017),left-sidedIEwasstillmoreprevalentinthisgroup (77.8%vs.22.2%).Allpatientsunderwenttransthoracicand transesophageal echocardiographyandmorethan 90%had evidenceofvegetations,whichwerelargerthan10mmin 48.5%.Abscesswasthemostcommonparavalvular compli-cation,followedbypseudoaneurysmandfistula.Regarding isolatedmicroorganisms,Staphylococcusspp.wasthemost frequentetiologicalagent(27.9%),followedby Streptococ-cusspp.Bloodculture-negativeIEwaspresentinmorethan athirdofthepatients.
Mortalityandcomplications
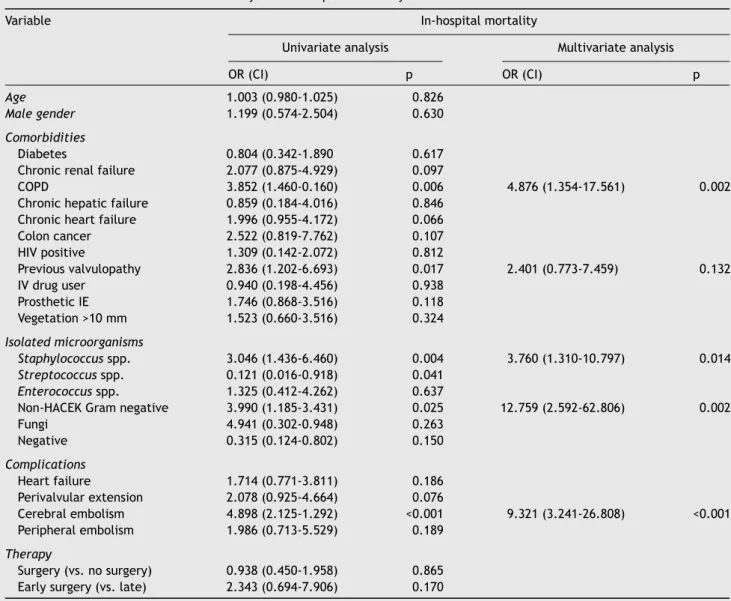
Thirty-eightpatientsdiedduring hospitalstay (16.3%)and 30-day mortalitywas22.7%. Theresults of univariateand multivariate analysis for in-hospital and 30-day mortal-ity are presented in Table 2 and Supplementary Table 1 (Appendix).Inmultivariateanalysis,independentpredictors ofin-hospitalmortalitywerechronicobstructivepulmonary disease (COPD), clinical course complicated by cerebral
Table1 Baseline clinical characteristicsof the patients (n=233).
Meanage,years 63.4±15.2
Malegender 161(69.1%)
Comorbidities,n(%)
Diabetes 61(26.1%)
Chronicrenalfailure 37(15.8%)
COPD 22(9.4%)
Chronichepaticfailure 15(6.4%)
Chronicheartfailure 75(32.2%)
Anemia 50(21.4%)
Coloncancer 17(7.3%)
HIVpositive 6(2.6%)
Congenitalcardiomyopathy 15(6.4%)
Previousnativevalvulopathy 39(16.7%)
PreviousIE 25(10.7%) IVdruguser 18(7.7%) ProstheticvalveIE 92(39.4%) Affectedvalve,n(%) Aortic 130(55.7%) Mitral 89(38.2%) Tricuspid 18(7.7%) Pulmonary 2(0.8%) Echocardiographicfindings,n(%) Vegetation>10mm 113(48.5%) Abscess 30(12.9%) Pseudoaneurysm 16(6.9%) Fistula 4(1.7%)
Severevalvularregurgitation 50(21.5%)
Isolatedmicroorganisms,n(%)
Staphylococcusspp. 65(27.9%)
Streptococcusspp. 38(16.3%)
Non-HACEKGramnegative 14(6.0%)
Negative 85(36.4%)
COPD: chronic obstructive pulmonary disease; HIV: human immunodeficiency virus; IE: infective endocarditis; IV: intra-venous.
embolismandIEduetoStaphylococcusspp.andnon-HACEK Gram-negativebacilli,thelatterbeingthestrongest predic-tor.
Overall,the complicationratewas56.6%andthemost frequent complications were (in descending order): heart failure (37.3%); perivalvular extension (25.8%); cerebral embolism(23.2%);andperipheralembolism(13.0%).In mul-tivariateanalysis,thevariablessignificantlyassociatedwith eachcomplicationwere:forheartfailure,previoushistory ofCOPD(oddsratio[OR]3.86;confidenceinterval[CI] 1.16-12.81;p=0.028)andpresenceofvalvularregurgitation(OR 2.74;CI1.26-5.96;p=0.011);forperivalvularextension,IE affectingtheaorticvalve(OR6.63;CI2.34-18.76;p<0.001) and prosthetic valve endocarditis (OR 2.83; IC 1.21-6.61; p=0.016); for cerebral embolism, IE affecting the mitral valve (OR 2.38; IC 1.12-5.04; p=0.024); and for periph-eralembolism,Staphylococcusspp.(OR3.22;CI1.21-8.59; p=0.019) and age under 65 years (OR 3.34; CI 1.25-8.94; p=0.017).
Table2 Univariateandmultivariateanalysisofin-hospitalmortality.
Variable In-hospitalmortality
Univariateanalysis Multivariateanalysis
OR(CI) p OR(CI) p
Age 1.003(0.980-1.025) 0.826
Malegender 1.199(0.574-2.504) 0.630
Comorbidities
Diabetes 0.804(0.342-1.890 0.617
Chronicrenalfailure 2.077(0.875-4.929) 0.097
COPD 3.852(1.460-0.160) 0.006 4.876(1.354-17.561) 0.002
Chronichepaticfailure 0.859(0.184-4.016) 0.846
Chronicheartfailure 1.996(0.955-4.172) 0.066
Coloncancer 2.522(0.819-7.762) 0.107 HIVpositive 1.309(0.142-2.072) 0.812 Previousvalvulopathy 2.836(1.202-6.693) 0.017 2.401(0.773-7.459) 0.132 IVdruguser 0.940(0.198-4.456) 0.938 ProstheticIE 1.746(0.868-3.516) 0.118 Vegetation>10mm 1.523(0.660-3.516) 0.324 Isolatedmicroorganisms Staphylococcusspp. 3.046(1.436-6.460) 0.004 3.760(1.310-10.797) 0.014 Streptococcusspp. 0.121(0.016-0.918) 0.041 Enterococcusspp. 1.325(0.412-4.262) 0.637
Non-HACEKGramnegative 3.990(1.185-3.431) 0.025 12.759(2.592-62.806) 0.002
Fungi 4.941(0.302-0.948) 0.263 Negative 0.315(0.124-0.802) 0.150 Complications Heartfailure 1.714(0.771-3.811) 0.186 Perivalvularextension 2.078(0.925-4.664) 0.076 Cerebralembolism 4.898(2.125-1.292) <0.001 9.321(3.241-26.808) <0.001 Peripheralembolism 1.986(0.713-5.529) 0.189 Therapy Surgery(vs.nosurgery) 0.938(0.450-1.958) 0.865
Earlysurgery(vs.late) 2.343(0.694-7.906) 0.170
CI:confidenceinterval;COPD:chronicobstructivepulmonarydisease;HIV:humanimmunodeficiencyvirus;IE:infectiveendocarditis; OR:oddsratio;IV:intravenous.
Surgicalmanagementofinfectiveendocarditis
Valvesurgerywasperformed in 86patients (36.9%),early in 44.2% of cases (Figure 1). The main indications for surgerywereheartfailure(50.0%)anduncontrolled infec-tion(46.8%),followedbypreventionofembolism(15.6%).
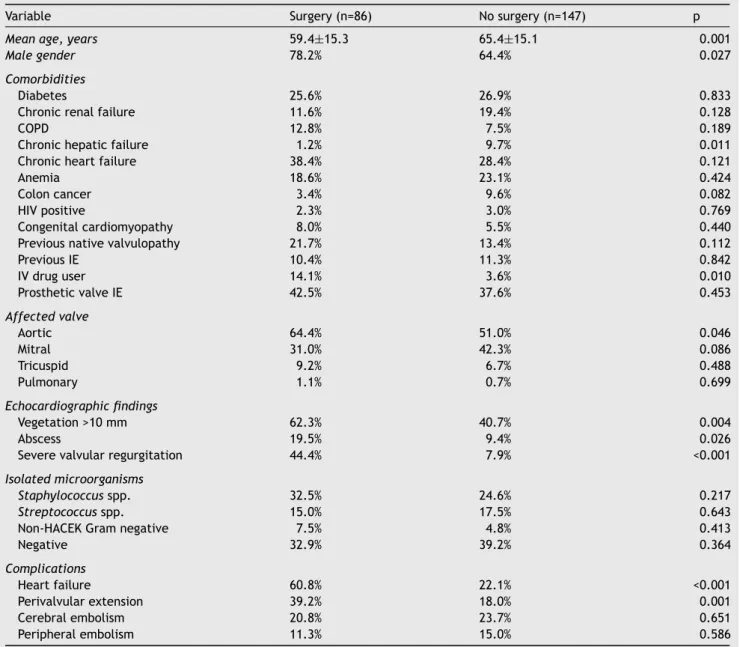
Comparing patients who underwent surgical treatment with those whoreceived only medical therapy (Table 3), theformerweremorelikelytobemale,youngerand intra-venousdrugusers.AorticvalveIEwasmorefrequentinthe surgicalgroup,buttherewerenodifferencesregarding pros-theticvalveendocarditis. Surgical therapy wasassociated with the presence of perivalvular abscesses, vegetations >10mmandseverevalvularregurgitation.Heartfailureand perivalvularextension weremore common in thesurgical group,withoutdifferenceinemboliccomplications.
When theoverallcohortwasanalyzed,surgerywasnot associated with decreased in-hospital mortality (15.5% in thesurgicalgroupvs.16.3%inthemedicalgroup,p=0.865).
Total 233 (100%) Surgical indication 133 (57%) Medical therapy 147 (63%) Surgical therapy 86 (37%)
(64% of patients with surgical indication)
Early surgery 38 (44%)
Late surgery 48 (56%)
Figure 1 Flowchart of the destination therapy of the patients.
However,consideringonlythesubgroupofpatientswith sur-gical indicationaccordingtotheguidelines(133patients),
Table3 Clinicalcharacteristicsofpatientstreatedwithsurgeryvs.nosurgery.
Variable Surgery(n=86) Nosurgery(n=147) p
Meanage,years 59.4±15.3 65.4±15.1 0.001
Malegender 78.2% 64.4% 0.027
Comorbidities
Diabetes 25.6% 26.9% 0.833
Chronicrenalfailure 11.6% 19.4% 0.128
COPD 12.8% 7.5% 0.189
Chronichepaticfailure 1.2% 9.7% 0.011
Chronicheartfailure 38.4% 28.4% 0.121
Anemia 18.6% 23.1% 0.424
Coloncancer 3.4% 9.6% 0.082
HIVpositive 2.3% 3.0% 0.769
Congenitalcardiomyopathy 8.0% 5.5% 0.440
Previousnativevalvulopathy 21.7% 13.4% 0.112
PreviousIE 10.4% 11.3% 0.842 IVdruguser 14.1% 3.6% 0.010 ProstheticvalveIE 42.5% 37.6% 0.453 Affectedvalve Aortic 64.4% 51.0% 0.046 Mitral 31.0% 42.3% 0.086 Tricuspid 9.2% 6.7% 0.488 Pulmonary 1.1% 0.7% 0.699 Echocardiographicfindings Vegetation>10mm 62.3% 40.7% 0.004 Abscess 19.5% 9.4% 0.026
Severevalvularregurgitation 44.4% 7.9% <0.001
Isolatedmicroorganisms
Staphylococcusspp. 32.5% 24.6% 0.217
Streptococcusspp. 15.0% 17.5% 0.643
Non-HACEKGramnegative 7.5% 4.8% 0.413
Negative 32.9% 39.2% 0.364 Complications Heartfailure 60.8% 22.1% <0.001 Perivalvularextension 39.2% 18.0% 0.001 Cerebralembolism 20.8% 23.7% 0.651 Peripheralembolism 11.3% 15.0% 0.586
COPD:chronicobstructivepulmonarydisease;HIV:humanimmunodeficiencyvirus;IE:infectiveendocarditis;IV:intravenous.
surgicaltreatmentwasassociatedwithasignificant reduc-tioninin-hospitalmortality(15.5%vs.32.6%,p=0.028).
The mean follow-up was 28.4±30.7 months and was achievedin95.3%ofthepopulation.Seventypatientsdied during the follow-up period, with one-year mortality of 33.0%andfive-yearmortalityof42.9%.
Therewerenodifferencesbetweenthegroupsregarding all-causemortalityintheoverallcohort(log-rankp=0.241) (Figure 2A). In patients with surgical indication, surgical treatmentcontinuedtohaveabeneficialeffect,withbetter long-termsurvival(log-rankp=0.029)(Figure2B).
Regardingtimingoftheprocedure,earlysurgerywasnot associated with increased mortality compared with later surgery(OR2.34,CI0.69-7.91,p=0.176).
Discussion
The findings of the present study can be summarized as follows: (i) in-hospital mortality from IE was >15% and morethan half ofthe patientshad acomplicated clinical course;(ii)COPD,cerebralembolismandIEdueto Staphy-lococcus spp. and non-HACEK Gram-negative bacilli were independentpredictorsofworsein-hospitaloutcomes;and (iii)surgerywasassociatedwithlowerin-hospitaland long-termmortalityinpatientswithsurgicalindication.
The characteristics of our population were similar to those described in other studies, including those in Por-tuguese cohorts.5 In our study the patients’ mean age
A
Overall population 1.0 p=0.241 p=0.029 Surgery No surgery Surgery No surgery 0.8 Cum ulativ e sur viv al Cum ulativ e sur viv al 0.6 0.4 0.2 0.0 1.0 0.8 0.6 0.4 0.2 0.0 0.0 Number at risk Surgery 86 147 119 64 44 99 24 79 59 15 7 39 86 47 30 64 44 15 9 24 15 5 2 7 No surgery Number at risk Surgery No surgery 20.0Follow-up (months) Follow-up (months)
40.0 60.0 80.0 100.0 120.0 0.0 20.0 40.0 60.0 80.0 100.0 120.0
Patients with surgical indication
B
Figure2 Kaplan-Meierestimateofall-causemortality.(A)Intheoverallcohort, theprobabilityofall-causemortalitydidnot differsignificantlybetween patientswho underwentsurgeryandthosetreatedwithmedicaltherapyonly; (B)inpatients with surgicalindication,surgicaltreatmentledtobetterlong-termsurvival.
descriptions,6 but inagreement withmorerecent series.1
Overall,themostcommonlyobservedcomorbiditiesinour cohortwerechronicheartfailureanddiabetes (32.2%and 26.1%,respectively).Inalargemultinationalobservational study,diabeteswasthemainunderlyingcondition(16.2%).1
The higher prevalence of comorbidities observed in our study,includingchronicheart failure,couldbeduetothe factthat somepatients hadbeen referred tooursurgical hospital,andsothepercentageof sickerpatients maybe overestimated.
In agreementwithrecentstudies,1,7,8therewasa
pre-dominanceofStaphylococcusspp.overStreptococcusspp., which used to be the most prevalent pathogen.6 The
higherincidenceofculture-negativeendocarditiscouldbe explainedbyfrequentpreviousantibioticadministrationdue tothe suspicionof other localized infections, although IE duetofastidiousandintracellularmicroorganismsmayalso havecontributedtothisfinding.9
The reported in-hospital mortality of patients with IE variesfrom12%to30%.1,10---12Inourstudy,in-hospital
mor-talityof16.3%wasobserved,suggestingthatourpopulation issimilartootherregistries.
PrognosisinIEisinfluencedbyfourmainfactors:patient characteristics, the presence or absence of cardiac and non-cardiaccomplications,theinfectingorganism andthe echocardiographic findings.4 Multivariate analysis in our
study identified COPD, Staphylococcus spp., non-HACEK Gram-negative bacilli and cerebral embolism as indepen-dent predictors of in-hospital mortality. Of these four factors,non-HACEK Gram-negativebacilli hadthe highest oddsratio.Otherstudieshaveconfirmedtheassociationof thesefactorswithworseprognosis.1,13,14 Apossible
expla-nationforthedismalprognosisassociatedwithnon-HACEK Gram-negativebacilliendocarditiscouldthatthese microor-ganismsarehealthcare-related agents.15 Increasingage,16
diabetes,17prostheticvalveinvolvement,18heartfailureand
paravalvularcomplications13 havebeen identifiedin other
studiesasriskfactorsforhighermortality.
In our study, clinical course was complicated in more thanhalfofthepatients.Heartfailureisthemostfrequent complicationof IE19,20 andisassociatedwithsevereacute
valvular regurgitation,19 which was also observed in our
study.Uncontrolled infection,the nextmostlikelyreason forsurgicalintervention,20---22isfrequentlydueto
perivalvu-lar extension,which is more commonin aortic valveand prostheticvalveendocarditis,22asalsodemonstratedinour
study.
Embolic events are a life-threatening complication. Predictorsofcerebralembolismhavebeenidentifiedin pre-vious studiesandincludesizeandmobilityof vegetations, causalmicroorganismandtheaffectedvalve.23---25Ourstudy
identified mitral valve IE as an independent predictor of embolism. Large vegetationsonthe mitralvalve are usu-allyassociatedwithahigherincidenceofembolism,25 and
thisisprobablythereasonforourfinding.Regarding periph-eralembolism,olderpatientsinthepresentstudyhadlower ratesofperipheralembolism,asreportedpreviously,16
pos-sibly simplydue tobeingunderdiagnosedbecauseof mild clinicalsignsandsymptoms.
Surgeryisperformedin23-53%ofpatientswithIEinmost series,2,10,26 including Portuguese cohorts,5 and our study
wasconsistent withthisprevalence(36.9%). Factors asso-ciatedwiththeneedforsurgeryweredemographics(male andyoungerpatientsmoreoftenunderwentsurgery)andthe affectedvalve(theaorticvalvewasmorecommonlytreated inthesurgicalgroup,probablyduetoahigherincidenceof perivalvularextensionoftheinfection,aswealso demon-strated). Although intravenous drug users usually have a predominance of right-sided IE caused by Staphylococcus
spp., onlyrarelyneeding surgerybecausetheyareusually responsivetomedicaltherapyalone,27inourstudy
ofsurgicaltherapy.Thisprobablyresultsfromthefactthat weareasurgicalcenterandmostcasesthatareindicated forsurgeryarereferredtous.Also,therehasrecentlybeen anincreaseinleft-sidedIEinintravenousdrugusers.28
Someechocardiographicfindingsandcomplicationssuch as acute severe valvular regurgitation and perivalvular extension were also associated with surgical treatment. However,embolismwasnotmoreprevalentinthesurgical group. Embolism is usuallymore frequent inthe firsttwo weeksoftherapyandlesssothereafter.29Althoughsurgeryis
notcontraindicatedinIEcomplicatedbyembolism, includ-ing ischemic stroke unless the neurological prognosis is judged too poor,29---31 the optimal timing remains
contro-versial becauseof therisk ofrecurrent embolismandthe hemorrhagicriskassociatedwithsurgery.29
Some studies appear to question the importance of surgery in IE patients, asthey found no survival benefit. However,intheInternationalCollaborationon Endocarditis-ProspectiveCohortStudyof1552patientswithnativevalve IE,32 surgery during the index hospitalization was
associ-ated with a significant reduction in in-hospital mortality (12.1%vs.20.7%,p<0.001).Afterpropensity matchingand adjustmentforsurvivalbias,thesurvivalbenefitofsurgery remained (absolute risk reduction of 5.9%), especially in patientswithcomplications.32Furthermore,ameta-analysis
byHeadetal.33demonstratedahighlysignificantbenefitof
surgery(p=0.0008).Inourcohortwefoundnosignificant dif-ferenceinmortalitybetweenpatientswhohadvalvesurgery and those who did not in the overall population, but in patientswithsurgicalindicationaccordingtotheguidelines, mortality wassignificantly lower in those whounderwent surgery(15.5%vs.32.6%,p=0.028).Thisshowsthatsurgery by itself is not associated withhigher mortality, and the fact thatoverall mortalitywasbetterappears toindicate aprognosticbenefitofsurgerywhenperformedinselected patients.
Regardingsurgicaltiming,we alsofound noincrease in mortalityinpatientswhounderwentearlyvs.latesurgery.In aprospectiverandomizedstudybyKangetal.onpatients withleft-sided IE, severe valvedisease andlarge vegeta-tions, there was no difference in survival at six months betweenthosewhounderwentearlysurgery(within48hours afterrandomization)orafter,butthoseoperatedearlyhad significantlylowerratesofthecompositeendpointofdeath fromanycause,embolicevents,orrecurrenceofIEatsix months(hazardratio0.08,CI0.01-0.65;p=0.02).34
Study
limitations
Ourstudyhassomelimitations.First,itwasaretrospective observational study, and therefore information was lim-itedtomedicalrecordsandimportantdatamayhavebeen incomplete.Thisstudyreportedfindingsofasingletertiary referral center, whichlimitsgeneralization ofthe results. Finally,sincesomecasescamefromotherhospitalcenters, thepercentageofcomplicatedcasesmaybeoverestimated, andsomepatients(4.7%)werelosttofollow-upbecauseof transfertotheirhospitalsoforigin.
However,thisstudyinvolves ananalysisofasignificant numberofpatientsandenablessomeinterestingconclusions tobedrawn.
Conclusion
TheresultsofthepresentstudyhelptoidentifyIEpatients whoareatincreasedriskofworseoutcome.Weidentified COPD,clinicalcoursecomplicatedbycerebralembolismand IEduetoStaphylococcusspp.andnon-HACEKGram-negative bacilli as independentpredictors of in-hospital mortality. More than half of the patients presented complicated IE, andpredictivefactorsforeachcomplicationwereanalyzed. Surgerywasperformed inmorethan onethirdofpatients and in patients with surgical indication it was associated withimprovedlong-termsurvival.
RapididentificationofpatientswithIEathigherriskof mortalitymayoffertheopportunitytochangethecourseof thediseaseandimproveprognosis.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
Appendix
A.
Supplementary
material
Supplementary material associated with this article can be found in the online version at
doi:10.1016/j.repc.2017.08.007.
References
1.Murdoch DR, Corey GR, Hoen B, et al. Clinical presenta-tion, etiology, and outcome ofinfective endocarditis in the 21stcentury:theInternationalCollaborationon Endocarditis-ProspectiveCohortStudy.ArchInternMed.2009;169:463---73.
2.Prendergast BD, Tornos P. Surgeryfor infective endocarditis: whoandwhen?Circulation.2010;121:1141---52.
3.LiJS,SextonDJ,MickN,etal.Proposedmodificationstothe Duke criteriafor thediagnosisofinfectiveendocarditis. Clin InfectDis.2000;30(4):633---8.
4.HabibG,LancellottiP,AntunesMJ,etal.2015ESCGuidelines for the management of infective endocarditis. EurHeart J. 2015;36:3075---123.
5.Ferreira JP,Gomes F,Rodrigues P,et al. Left-sidedinfective endocarditis:analysisofin-hospitalandmedium-termoutcome andpredictorsofmortality.RevPortCardiol.2013;32:777---84.
6.HoenB,AllaF,Selton-SutyC,etal.Changingprofileof infec-tiveendocarditis: resultsofa1-yearsurveyinFrance.JAMA. 2002;288:75---81.
7.Mu˜nozP,KestlerM,DeAlarconA,etal.Currentepidemiology andoutcomeofinfectiveendocarditis:amulticenter, prospec-tive,cohortstudy.Medicine(Baltimore).2015;94:e1816.
8.MoingVLe,Doco-lecompteT,ChirouzeC,etal.Preeminence of Staphylococcus aureus in infective endocarditis: a 1-year population-basedsurvey.ClinInfectDis.2012;54:1230---9.
9.FournierP-E,ThunyF,RichetH,etal.Comprehensivediagnostic strategyforbloodculture-negativeendocarditis:aprospective studyof819newcases.ClinInfectDis.2010;51:131---40.
10.Tornos P,IungB, Permanyer-MiraldaG, etal.Infective endo-carditisinEurope:lessonsfromtheEuroheartsurvey.Heart. 2005;91:571---5.
11.Delahaye F,Alla F,BéguinotI,et al. In-hospitalmortalityof infectiveendocarditis:prognosticfactorsandevolutionoveran 8-yearperiod.ScandJInfectDis.2007;39:849---57.
12.Lo J,OlmosC,VilacostaI,etal.Contemporaryepidemiology and prognosis of septic shock in infective endocarditis. Eur HeartJ.2013;34:1999---2006.
13.AlbertoJ,RománS,LópezJ,etal.Prognosticstratificationof patientswithleft-sidedendocarditisdeterminedatadmission. AmJMed.2007;120:369.
14.MisfeldM,GirrbachF,EtzCD,etal.Surgeryforinfective endo-carditiscomplicatedbycerebralembolism:aconsecutiveseries of375patients.JThoracCardiovascSurg.2014;147:1837---44.
15.Morpeth S, Murdoch D, Cabell CH, et al. Non-HACEK gram-negative bacillus endocarditis. Ann Intern Med. 2007;147:829---35.
16.Durante-MangoniE,BradleyS,Selton-SutyC,etal.Current fea-turesofinfectiveendocarditisinelderlypatients:resultsofthe InternationalCollaborationonEndocarditisProspectiveCohort Study.ArchInternMed.2008;168:2095---103.
17.Kourany WM, Miro JM, Moreno A, et al. Influence of dia-betesmellitusontheclinicalmanifestationsandprognosisof infectiveendocarditis:areportfromtheInternational Collab-oration onEndocarditis-MergedDatabase.ScandJInfect Dis. 2006;38:613---9.
18.LalaniT,KanafaniZA,ChuVH,etal.Prostheticvalve endocardi-tisduetocoagulase-negativestaphylococci:findingsfromthe International CollaborationonEndocarditisMergedDatabase. EurJClinMicrobiolInfectDis.2006;25:365---8.
19.Nadji G, Rusinaru D, Rámadi JP, et al. Heart failure in left-sidednativevalveinfectiveendocarditis:characteristics, prognosis,andresultsofsurgicaltreatment.EurJHeartFail. 2009;11:668---75.
20.RevillaA, López J,VilacostaI,et al.Clinicaland prognostic profileofpatientswithinfectiveendocarditiswhoneedurgent surgery.EurHeartJ.2007;28:65---71.
21.AgapitoA,BrancoL,PatrícioL,etal.Cirurgianaendocardite infecciosa.RevPortCardiol.1990;9:683---6.
22.Graupner C, Vilacosta I, SanRoman J, et al. Periannu-lar extension of infective endocarditis. J Am Coll Cardiol. 2002;39:1204---11.
23.VilacostaI,GraupnerC,SanRománJ,etal.Riskofembolization afterinstitutionofantibiotictherapyforinfectiveendocarditis. JAmCollCardiol.2002;39:1489---95.
24.Tischler MD, Vaitkus PT. The ability of vegetation size on echocardiography to predict clinical complications: a meta-analysis.JAmSocEchocardiogr.1997;10:562---8.
25.Mügge A, Daniel WG. Echocardiographic assessment of veg-etations in patients with infective endocarditis: prognostic implications.Echocardiography.1995;12:651---61.
26.Thuny F, Grisoli D, Collart F, et al. Management of infective endocarditis: challenges and perspectives. Lancet. 2012;379:965---75.
27.FronteraJ,GradonJD.Right-sideendocarditisininjectiondrug users:review of proposedmechanismsof pathogenesis.Clin InfectDis.2000;30:374---9.
28.CarozzaA,DeSantoLS,RomanoG,etal.Infective endocardi-tisinintravenousdrugabusers:patternsofpresentationand long-termoutcomesofsurgicaltreatment.JHeartValveDis. 2006;15:125---31.
29.RuttmannE,WilleitJ,Ulmer H,etal. Neurologicaloutcome of septic cardioembolic stroke after infective endocarditis. Stroke.2006;37:2094---9.
30.García-CabreraE,Fernández-HidalgoN,AlmiranteB,etal. Neu-rologicalcomplications ofinfective endocarditisriskfactors, outcome,andimpactofcardiacsurgery:amulticenter obser-vationalstudy.Circulation.2013;127:2272---84.
31.Novy E, Sonneville R, Mazighi M, et al. Neurological complicationsofinfectiveendocarditis:newbreakthroughsin diagnosisandmanagement.MedMalInfect.2013;43:443---50.
32.LalaniT,CabellCH,BenjaminDK,etal.Analysisoftheimpact ofearlysurgeryonin-hospitalmortalityofnativevalve endo-carditis: use of propensity score and instrumental variable methodsto adjust for treatment-selection bias.Circulation. 2010;121:1005---13.
33.Head S, Mokhles M,Osnabrugge R, et al.Surgery in current therapy for infective endocarditis. Vasc Health Risk Manag. 2011;7:255---63.
34.KangD-H,KimY-J,KimS-H, etal. Earlysurgeryversus con-ventionaltreatmentforinfectiveendocarditis.NEngl JMed. 2012;366:2466---73.