r e v b r a s r e u m a t o l . 2017;57(6):623–625
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Relapsing
polychondritis
and
lymphocytic
meningitis
with
varied
neurological
symptoms
Policondrite
recidivante
e
meningite
linfocitária
com
sintomas
neurológicos
variados
Renata
Dal-Prá
Ducci
a,
Francisco
Manoel
Branco
Germiniani
a,∗,
Letícia
Elizabeth
Augustin
Czecko
a,
Eduardo
S.
Paiva
b,
Hélio
Afonso
Ghizoni
Teive
aaUniversidadeFederaldoParaná,HospitaldasClínicas,DepartamentodeMedicinaInterna,Servic¸odeNeurologia,Curitiba,PR,Brazil bUniversidadeFederaldoParaná,HospitaldeClínicas,DepartamentodeMedicinaInterna,Servic¸odeReumatologia,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14March2015
Accepted25September2015
Availableonline17March2016
Introduction
Relapsingpolychondritisisarareautoimmunedisease,1,2with
afemale–maleratioof2:4,3withsymptom’sonsetbetween20
and60yearsofage(peakincidencearound40y/o),4
charac-terizedbybilateralauricularandnasalchondritis,vestibular
involvementand varied systemic symptoms due to
recur-rentandprogressiveinflammationofcartilaginoustissueand
proteoglycan-richstructuresinvarioussitesofthebody.1,2We
reportthecaseofapatientwithrelapsingpolychondritiswith
severalneurologicalmanifestations.
Case
report
A69year-oldmalewithdiabetes,hypothyroidismand
dysli-pidemiahadatwo-monthhistoryofswellingandpainofboth
earlobesandedemaandarthralgiaofmetacarpophalangeal
∗ Correspondingauthor.
E-mail:[email protected](F.M.Germiniani).
joints and ankles,aswell asgeneralized painwith a
wax-ingandwaningcourse.Twentydayspriortohisadmissionin
ourhospitalhestartedwithataxia,paraparesis,tinnitus,
ver-tigoandconfusion.Hehadbeenpreviouslyseenatanother
hospital,aroundthetimeofconfusiononset,wherehewas
treatedforherpeticencephalitisfollowingalumbarpuncture
which disclosed elevated leukocytes, witha predominance
oflymphocytes.Althoughatfirsthehadanimprovementof
confusion,hisparaparesisremainedunaffected.Onphysical
examinationhehadnystagmusinthedownwardgaze,rigidity
ofupperlimbs,paraparesis,absentreflexes,tactile
hypoesthe-sia,dysmetricmovements,grossposturalandactiontremor,
bradykinesia and truncal ataxia. He alsohad swelling and
a purplish erythemaofboth earlobes and arthritisin the
metacarpophalangealjointsofthesecondandthirdfingers
oftherighthand(Fig.1).BrainandcervicalMRIdiscloseda
mildthickeningofthedura(Fig.1).Anewlumbarpuncture
confirmed the presenceof elevatedleukocytes and
labora-toryexamsdisclosedaugmentedinflammatoryactivity and
http://dx.doi.org/10.1016/j.rbre.2016.02.005
2255-5021/©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
624
rev bras reumatol.2017;57(6):623–625Fig.1–Rheumatologicalclinicalfindings(upperimages):(A)edemaofmetacarpophalangealjoints;(B)earlobechondritis. BrainMRIfindings(lowerimages):(C)axialdiffusionwiththickeningoftheduraofbothfrontallobes;(D)sagittalT1FSE FATSATwithincreasedmeningealsignaladjacenttothecerebellum;(E)T2FSEshowingmildcerebellaratrophy.
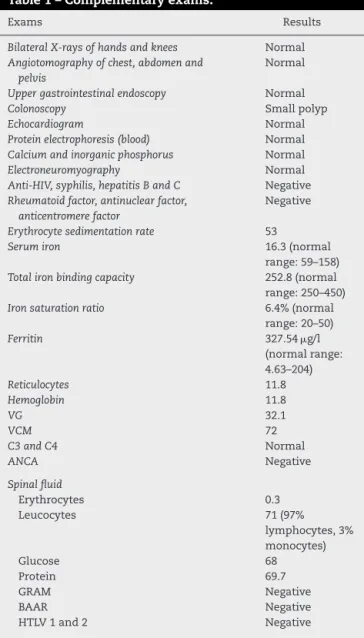
iron-deficientanemia(Table1).Adiagnosisofrelapsing
poly-chondritiswasmadebasedontheassociationofchondritis,
arthritisandvestibularataxiawithpredominant
neurologi-calsymptoms.FollowingacourseofPrednisone1mg/kgqd
therewasmajorimprovementofchondritis,arthritis,ataxia
and paraparesis, but the tremor remained unchanged. On
a one-year follow-up visit he had developed several
com-plicationsofchroniccorticosteroiduse,suchasosteopenia,
hypertension,Cushing’ssyndrome,worseningofobstructive
apneasyndromeandoneepisodeofbilateralcutaneous
Her-pes Zoster of the trunk. These complications warranted a
changeofimmunosuppressivetreatmentfromPrednisoneto
Methotrexate.In spiteofthis,hehad no newneurological
symptomsandremainedwithmoderateataxia.
Discussion
Relapsingpolychondritisisararemultisystemicautoimmune
disease that affects cartilaginous tissue, especially hyaline
cartilages at multiple sites, most often compromising the
antihelixofbothearlobes,withsparingofthelobule.2,5
Sero-negative polyarthritis and systemic compromise of other
organsmayalsooccur(includingocularinflammation,
audio-vestibularimpairment,vasculitis,skininvolvement,valvular
insufficiency and neurological symptoms) due to
compro-miseofproteoglycan-richtissues.6,7Around30%ofthecases
are associated with concurrent autoimmune disease,
sys-temicvasculitisandmyelodysplasticsyndrome.5,8Diagnosis
ismadeonclinicalgrounds,occasionallywithpathology
dis-closing inflammatory compromiseof affected cartilaginous
tissue.5,7 Currently, the diagnosis is made on the basisof
demonstrationofeitherchondritisintwoofthreesites
(auric-ular, nasal,laryngotracheal); or oneofthese sitesand two
additional features, including ocular inflammation,
audio-vestibulardamage,orsero-negativeinflammatoryarthritis.1,9
There are no specific laboratory findings.5,7 Neurological
symptomsoccurinaminorityofcases(3%)andmayrange
from compromiseofcranialnervestoamoreovert
presen-tation with cerebellar compromise, seizures or other focal
findings suggestive ofcorticalcompromise. These are
vas-culitic in nature. Aseptic meningitis, with thickening of
themeninges,lymphocyticmeningoencephalitis,
rhomboen-cephalitisandcerebralaneurysmscanalsooccur.1,10–12Inour
casewemadethediagnosissolelyonclinicalgrounds,asthere
wasevidenceonphysicalexaminationofchondritisofboth
earlobes,sero-negativepolychondritisandneurological
com-promisewithasepticmeningitis.About25%ofpatientsdiein
uptofiveyearsfollowingdiagnosis;laryngotracheal
rev bras reumatol.2017;57(6):623–625
625
Table1–Complementaryexams.
Exams Results
BilateralX-raysofhandsandknees Normal
Angiotomographyofchest,abdomenand pelvis
Normal
Uppergastrointestinalendoscopy Normal
Colonoscopy Smallpolyp
Echocardiogram Normal
Proteinelectrophoresis(blood) Normal
Calciumandinorganicphosphorus Normal
Electroneuromyography Normal
Anti-HIV,syphilis,hepatitisBandC Negative
Rheumatoidfactor,antinuclearfactor, anticentromerefactor
Negative
Erythrocytesedimentationrate 53
Serumiron 16.3(normal
range:59–158)
Totalironbindingcapacity 252.8(normal range:250–450)
Ironsaturationratio 6.4%(normal
range:20–50)
Ferritin 327.54g/l
(normalrange: 4.63–204)
Reticulocytes 11.8
Hemoglobin 11.8
VG 32.1
VCM 72
C3andC4 Normal
ANCA Negative
Spinalfluid
Erythrocytes 0.3
Leucocytes 71(97%
lymphocytes,3% monocytes)
Glucose 68
Protein 69.7
GRAM Negative
BAAR Negative
HTLV1and2 Negative
ofdeath.1,4 Factorsthathaveanegativeimpactonsurvival
atthetimeofdiagnosisincludeoldage,anemiaand
laryn-gotracheal stricture.1,2 Oralnonsteroidal anti-inflammatory
drugs may be used to treat patients with arthralgias and
mildarthritis.Standardimmunosuppressivetreatmentstarts
with high doses of corticosteroids(Prednisone 1mg/kgqd),
which islater tapered off to a smaller dosage in patients
withmoderatetoseverecompromise.Methotrexatemaybe
used asasecond-line drugtoavoidside effectsofchronic
corticosteroid treatment. Azathioprine, cyclophosphamide,
cyclosporine,mycophenolatemofetilandTNF-antagonistsare
otheroptions.5,11
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.KentPD,MichetCJJr,LuthraHS.Relapsingpolychondritis. CurrOpinRheumatol.2004;16:56–61.
2.SharmaA,GnanapandithanK,SharmaK,SharmaS. Relapsingpolychondritis:areview.ClinRheumatol. 2013;32:1575–83.
3.PintoP,BritoI,BritoJ,PintoJ,VenturaF.Policondrite
recidivante.Estudoretrospectivodeseiscasos.ActaMedPort. 2006;10:213–6.
4.RodriguesEM,SilveiraRCN,LeiteN,TepedinoMM.Relapsing polychondritis:acasereport.RevBrasOtorrinolaringol. 2003;69:128–30.
5.LahmerT,TreiberM,vonWerderA,FoergerF,KnopfA, HeemannU,etal.Relapsingpolychondritis:anautoimmune diseasewithmanyfaces.AutoimmunRev.2010;9:540–6.
6.ArnaudL,MathianA,HarocheJ,GorochovG,AmouraZ. Pathogenesisofrelapsingpolychondritis:a2013update. AutoimmunRev.2014;13:90–5.
7.WangZJ,PuCQ,WangZJ,ZhangJT,WangXQ,YuSY,etal. Meningoencephalitisormeningitisinrelapsing
polychondritis:fourcasereportsandaliteraturereview.JClin Neurosci.2011;18:1608–15.
8.YangS,ChouC.Relapsingpolychondritiswithencephalitis.J ClinRheumatol.2004;10:83–5.
9.EdreesA.Relapsingpolychondritis:adescriptionofacase andreviewarticle.JClinRheumatol.2011;31:707–13.
10.ChoiHJ,LeeHJ.Relapsingpolychondritiswithencephalitis.J ClinRheumatol.2011;17:329–31.
11.ChopraR,ChaudharyN,KayJ.Relapsingpolychondritis. RheumDisClinNorthAm.2013;39:263–76.