www.elsevier.es/ai
ORIGINAL
ARTICLE
Off-label
prescribing
for
allergic
diseases
in
pre-school
children
M.
Morais-Almeida
∗,
A.J.
Cabral
ImmunoallergyDepartment,CUFDescobertasHospital,Lisbon,Portugal
Received29December2012;accepted2February2013
KEYWORDS
Asthma; Atopiceczema; Infant;
Off-label prescription; Pre-schoolchildren; Rhinitis
Abstract
Background: Severalstudieshavedemonstratedthatmedicationiscommonlyusedoff-label inchildrenwithallergic diseases.Theaimofthisstudywas tocharacteriseoff-labeluseof prescriptionsforallergicdiseasesinpre-schoolchildrenfromanallergologyoutpatientunit.
Methods:Theclinicalfilesofchildrenaged≤6yearsseeninareferenceallergologyconsultation
withasthma,allergicrhinitis,and/oratopiceczemawerereviewed.Atotalof500patientswere consecutivelyobservedfromJanuarytoJune2012.Thedatacollectedincludedgender,age, diagnosis,andprescriptionswiththerespectivedailydosage.
Results:Atotalof1224prescriptionswereregistered.Themostprescribedmedicationswere oralantihistamines(34.6%),antileukotrienes(22.6%),topicalnasalcorticosteroids(20.3%),and inhaledcorticosteroids(17.7%).Fromallprescriptions,422(34.5%)wereconsideredoff-label forage(62.6%),dosage(31.7%),orclinicalindication(5.7%).Off-labelusewasmorefrequent inchildrenaged<2years,with73.5%prescribedforchildrenofthisage.
Conclusions: Off-labeluseofdrugs forthetreatmentofpaediatricallergicdiseasesishigh. However,theseprescriptionsarenotnecessarilywrong,andarerecommendedinmany guide-lines. Randomised controlledstudies arelimitedbymethodological difficulties creatingthe need formore observationalstudiesinordertofurther evaluate thesafetyandefficacy of drugsusedinchildren.
©2012SEICAP.PublishedbyElsevierEspaña,S.L.Allrightsreserved.
Introduction
Manydrugs usedin thetreatment of allergicdiseases are notappropriatelystudiedinthepaediatricpopulation, espe-cially in infants and younger children. Nonetheless, their
∗Correspondingauthor.
E-mailaddress:[email protected]
(M.Morais-Almeida).
off-labeluse,i.e.useoutsidetheformalindications autho-risedbytheregulatoryauthorities,inadifferentagegroup, dose,orindication1iscommoninmanypaediatricillnesses
likeallergicdisease.Thishappensbecauseofpracticaland ethicalconsiderations incarryingout clinicaltrials inthis population.2 In general,off-label prescription rates range
from 11% to 37% in children treated in the community setting, and in up to62% of children in paediatric hospi-tal wards.3 The major concern with this off-label use is
theincreasedriskofadversedrugreactions.4Additionally,
0301-0546/$–seefrontmatter©2012SEICAP.PublishedbyElsevierEspaña,S.L.Allrightsreserved.
Pleasecitethisarticleinpressas:Morais-AlmeidaM,CabralAJ.Off-labelprescribingforallergicdiseasesinpre-school Table1 Drugsusedfortreatmentofasthma,allergicrhinitis,andatopiceczema,andtheirauthorizationsforuseaccording toageanddose.
Category Drug Minimumage Maximumdose
IC Budesonide 2years 400g/day---2to7years
Fluticasone 12months 200g/day---1to4years;400g/day---4to16years
NC Budesonide 6years 400g/day Fluticasonefuroate 6years 55g/day Mometasone 6years 100g/day
LABAa Salmeterol 4years 100g/day
AH Cetirizine 2years 5mg/day---2to6years;10mg/day---6to18years Levocetirizine 2years 2.5mg/day---2to6years;5mg/day---olderthan6years Loratadine 2years 5mg/day---2to6years;10mg/day---6to18years Desloratadine 12months 1.25mg/day---1to5years;2.5mg/day---6to12years Ebastine 2years 2.5mg/day---2to5years;5mg/day---6to11years
Ketotifen 6months 0.1mg/kg/day-6monthsto3years;2mg/day---olderthan3years
AL Montelukast 6months 4mg/day---6monthsto5years;5mg/day---6to14years
TI Pimecrolimus 2years
Source:Infarmed,I.P.11
IC:inhaledcorticoids;NC:nasaltopiccorticoids;LABA:longacting2agonists;AH:oralantihistamines;AL:anti-leukotriene;TI:topic
immunomodulator.
aAlwaysusedincombinationwithfluticasone---authorisationsidenticaltoisolateduse.
youngerchildrenandinfantshaveaconsiderablyincreased riskofprescriptionerrors,especiallydosageerrors.5
However, off-label prescriptions are not necessarily incorrect,6 and may evenbe appropriate in certain
clini-calsituations provided thereis no alternative treatment, andwhenthelikelybenefitsoutweighthepotentialrisks,7
suchaswhenconventionaltreatmentsareunabletoachieve controlofthedisease.Thepotentialadvantagesofoff-label prescribing,apart from the probable benefit to the indi-vidual patient, are that new therapeutic uses may be described,anddataontheefficacyandsafetyofthedrug being used in new settings may be collected.8 With
off-labelprescriptions,thephysicianmustactasanenlightened intermediary. On the one hand, managing the regulatory dataaimedatensuringtheeffectivenessandsafetyofthe prescription,andontheotherhand, puttingallhisorher knowledgeintoservingtheinterestsofthepatient.
Several studies have consistently shown that off-label useinchildreniscommon.Apopulation-basedcohortstudy carriedout in primarycare units in Holland assessed the prescribingof respiratory drugs in 2502children, showing thatalmost37%wereoff-label,and39%inthisgroupwere prescriptionsforasthma.9TheTEDDYstudy,comparingthe
use of anti-asthmatic drugs in children in Holland, Italy, andtheUnited Kingdom,established thatoff-label useof 2-agonists andinhaled corticosteroids is frequent, inclu-ding upto80% ofthe inhaled budesonide prescriptionsin Italy.10
In Portugal, few studies exist concerning off-label use of drugs in paediatric populations, and none are speci-fically related to drugs for the treatment of aller-gic disease. This study aimed to characterise off-label prescribing of drugs used in the treatment and con-trol of asthma, allergic rhinitis, and atopic eczema in a significant sample of pre-school aged children followed
by allergy specialists at a referenceallergology consulta-tion.
Methods
Theclinicalfilesofchildrenaged≤6yearsfollowedinour allergology consultationwhowere diagnosedwithcurrent asthma,allergicrhinitis,and/oratopiceczemaphenotypes, withpredominantly moderate tosevere clinical presenta-tions, were systematicallyreviewed. Consecutive medical visitswereanalysedfromthebeginningofJanuary2012until theinclusionofatotalof500patients(June2012).
Thedatacollectedincludedgender,age,diagnosis,and drugs prescribed for the control of allergic diseases that were used for a minimum period of two weeks, as well astherespectivedosages.Drugsusedforacutetreatment werenotconsidered.Thedrugsincludedwereclassifiedas follows: (1) inhaled corticosteroids (IC); (2) nasal topical corticosteroids(NC);(3)longacting2agonists(LABA);(4) oralantihistamines(AH);(5)oralantileukotrienes(AL);(6) topicalimmunomodulators(TI).
Theformalindicationsforeachdrugwereavailablefrom Infarmed --- Autoridade Nacional do Medicamento e Pro-dutos, I.P. (Infarmed),11 the national authority on drug
controlandauthorisation,andwereconfirmedbythe phar-maceuticalcompaniesresponsiblefortheirproductionand distribution; these indications were systematically com-paredbytheauthors,whofoundnodiscrepancies(Table1). Theage groups wereclassified accordingtothe paedi-atric age definitions provided by the EuropeanMedicines Agency(EMA).12Assuch,thesamplewasdividedasfollows:
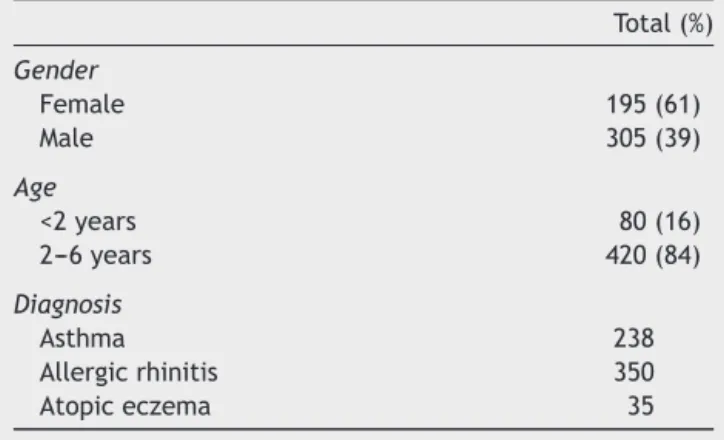
Table2 Characterisationofthestudypopulation.
Total(%)
Gender
Female 195(61)
Male 305(39)
Age
<2years 80(16)
2---6years 420(84)
Diagnosis
Asthma 238
Allergicrhinitis 350
Atopiceczema 35
Thestudywasapprovedbytheethicalcommitteeofthe institution.
Statisticalanalysis
Statistical comparisons(chi-square)were performed using the statistical program IBM SPSS Statistics version 19.0.0 (2010,Chicago, IL,USA), andp<0.05wasconsidered sta-tisticallysignificant.
Results
A total of 500 patient files were verified (Table 2), corresponding to 1224 prescriptions used to control the previously mentioned pathologies. The most pre-scribed drugs were oral antihistamines (34.6%), followed
by antileukotrienes (22.6%), nasal topical corticosteroids (20.3%), inhaled corticosteroids (17.7%), association of inhaledcorticosteroidsandLABA(4.6%),and,finally,topic immunomodulators(0.2%).Themostoftenuseddrugswere montelukast (22.6%), levocetirizine (17.1%), mometasone (17.1%),andfluticasone(17.0%)(Table3).
Ofalltheprescriptions,802(65.5%)wereauthorisedfor use in children and were used according to the formally approvedindication.Theremaining422(34.5%)drugswere usedoff-label,outsidetheapprovalsforage(62.6%),dosage (31.7%),or clinicalindication(5.7%).Mometasone, flutica-sone, and levocetirizine were the drugs most frequently prescribedinthis fashion(Table3).InPortugal,asin sev-eralother European countries, mometasoneis authorised solelyforchildrenaged>6yearsandisthereforefrequently usedoff-label.The sameoccurswithlevocetirizine,which isauthorisedonly for childrenaged>2 years.As for fluti-casone,its off-label use wasrelated to prescribingdoses greater than the approveddosage. Onlymontelukast was prescribedoutsideofitsclinicalindicationsince,in Portu-galasinothercountries,itcanonlybeusedasadjunctive therapyinthepreventivetreatmentof asthmainchildren age<2years,beingnotauthorisedasasingletherapy,11with
theexceptionifitisnotpossibletouseinhaledsteroidsas controllermedication.
Dividingthe prescriptions intocategories, we highlight theoff-labeluseofnasaltopicalcorticoidsinover75%ofthe totalprescription(Table4),whichwasalwaysduetotheage limitation.We alsonotetheoff-labeluseofpimecrolimus due toage in cases of severe atopiceczema, despite its reducedprescribing in three patients aged 8, 10, and 12 months,respectively.
Table3 Totalnumberofprescriptionsstudied.
Category Drug Prescriptions
Total Off-label
Total % Age Dose Indication
IC Budesonide 9 1 11.1 1 ---
---Fluticasone 208 94 45.2 --- 94
---NC Budesonide 11 9 81.8 9 ---
---Fluticasonefuroate 28 12 42.9 12 ---
---Mometasone 209 168 80.4 168 ---
---LABA Salmeterol 56 17 30.4 17 ---
---AH Cetirizine 115 16 13.9 6 10
---Levocetirizine 209 52 24.9 48 4
---Loratadine 3 0 0 --- ---
---Desloratadine 53 19 35.8 --- 19
---Ebastine 5 5 100.0 --- 5
---Ketotifen 38 1 2.6 --- 1
---AL Montelukast 277 25 9.0 --- 1 24
TI Pimecrolimus 3 3 100.0 3 ---
---Totals 1224 422 34.5 264(62.6%) 134(31.7%) 24(5.7%)
Pleasecitethisarticleinpressas:Morais-AlmeidaM,CabralAJ.Off-labelprescribingforallergicdiseasesinpre-school Table4 Prescriptionsaccordingtoageanddrugcategory.
Total Authorised Off-label
Total % Total % Age Dose Indication
Agegroup(years)
<2 181 48 26.5 133 73.5* 68 41 24
2---6 1043 754 72.5 289 27.5* 195 94
---Drugcategory
IC 217 122 56.2 95 43.8 1 94
---NC 248 59 23.8 189 76.2 189 ---
---IC+LABA 56 39 69.6 17 30.4 17 ---
---AH 423 330 78.0 93 22.0 54 39
---AL 277 252 91.0 25 9.0 --- 1 24
TI 3 --- --- 3 100 3 ---
---Results in n, except when pointedout. IC: inhaled corticoids; NC:nasal topic corticoids;LABA: long acting2 agonist;AH: oral
antihistamines;AL:anti-leukotriene;TI:topicimmunomodulator.
* p<0.001.
Although the overall prescribing for children aged <2 yearswaslower than in older children, off-label use was relativelymuchmorefrequent.Upto73.5%ofprescriptions in this age group were off-label compared with 27.7% in theoldestagegroup(Table4).Thisdifferencewas statisti-callysignificant(p<0.001).Notethat,withoneexception, allchildren aged<2 years receivedat least oneoff-label prescription.
Discussion
Thisstudyprovidesdetailedandoriginalinformationabout national off-label prescribing for the allergic diseases asthma,allergic rhinitis,and atopiceczemain the paedi-atricpopulation.
Wefound that,inpre-schoolchildren,theuseofdrugs fortheseconditionsinmoderatetosevereformsisfrequent (34.5%),particularlyin childrenaged<2years,withmore than73%ofprescriptionsmadeforthisgroup.Thisis proba-blyduetotheabsenceofdataonthesafetyandefficacyof drugsatthisagegroup,owingtothelackofclinicaltrials.1---4
The lack of clinical researchin the paediatric popula-tion,mainlyininfants,resultsfromacombinationoffactors that can contribute to this age group being the last to benefitfrom medicalprogress.2,13 Pharmaceutical
compa-nies,whichcanneverpromoteorrecommendoff-labeluse oftheirdrugs,apparentlyviewtheapprovalofdrugsin chil-drenasamarketthat wouldbringsmallfinancial benefit, withonlyafewdrugsrepresentingalargeenougheconomic interest.Assuch,itisnotsurprisingthatthedrugsthathave beenadequatelystudiedinchildrenareanti-infectious vac-cinesandsomeantibiotics.Specificmedicaltechniquesand appropriateequipmentarealsonecessaryforclinical inves-tigationinthepaediatricpopulation;technicalprocedures thatseemsimplein adults,suchasdrawingblood, among other minimallyinvasive interventions, canbe difficult to execute or even authorise in children. Lastly, the ethical implicationsin childrenaremore complex,withpotential risksassociatedwiththeintervention,andsignificantly hin-derclinicaltrialsinthispopulation.14
The clinical investigation of drugs in the paediatric populationisregulatedbyinternationalstandards(ICHE11), includingEuropean(ECno.1902/2006),whichsetout spe-cificrequirementsfortheprotectionofchildreninclinical trials.15,16However,thecurrentEMAregulationsencourage
researchanddevelopmentofdrugsinthepaediatric popu-lationtoimprovetheavailableinformationonthesedrugs, by assigning benefits to the pharmaceutical industry like extendingtheperiodofpatentexclusivity.17,18
Nonetheless,mostdrugsavailableonthemarketarenot specificallytestedinchildren,particularlyyoungerchildren. In Portugal,Infarmed has specialisedcommittees,namely the Committee for the Evaluation of Medicinal Products, which is responsible for issuing opinions on the quality, safety,andefficacyofdrugswithintheirmarketing authori-sations(AIM).Theyhavetheresponsibilityforreviewingand approvingtheSummariesofProductCharacteristics(RCM). However,theuse ofdrugsoutside theirauthorisedRCM is nottheconcernofauthoritiesandisthesoleresponsibility oftheprescriber.19
This study showed a great number of off-label prescriptions,althoughitcanbeoverestimatedrelatedwith the severityofthe clinicalmanifestationsof theincluded children; these values must be interpreted with caution, however,astheymaysuggestinadequateorinappropriate use.Off-labelprescribingisnotnecessarilyincorrect6andis
contemplatedinseveraltherapeuticguidelinesthatinclude paediatric populations,but remarkably withnoindication that some of the drugs are being recommended for unli-censedandoff-labeluse.20Infact,indicationsfordrugusein
therapeuticguidelinesdonotclinicallyorlegallyauthorise theiruse,eveniftheguidelinessupportit.
necessityforthedrug’suse,whichwasinvariablyauthorised after the requested clarifications, increasing the compli-ancetotheindicatedtreatments.Thistypeofinformation isveryimportantforpatientandcaregiveradherence,but it is often omitted. A survey conducted in the UK found thatmost paediatriciansdidnotobtaininformedconsent, or inform the children’s parents that the drug’s use was off-label,whichcouldindicatepoormedicalpractice.21
Fromtheprescriptionsstudies,wenotetheveryfrequent off-label use of a very safe topical nasal corticosteroid, mometasone.Thereasonforoff-labelusewasentirelydue to itsuse outside the authorised age group, as it is only approvedforchildrenaged≥6years.Thisimpositionismade by EMA, whereas the U.S. Food and Drug Administration (FDA)alreadyallowstheuseofthisdruginyoungerchildren, i.e.thoseaged>2years.22 Despitethediscrepancyin
per-missions,thefactthattheFDA,whichisresponsibleforthe regulationofdrugsintheUnitedStates,hasalready autho-risedbroaderuseofthisdrugoffersadditionalsecurityfor prescribingitoff-labelinEurope.Iftheauthorisationswere identical,off-labeluseofmometasonewouldbeonly4.3%. Thesamecanbesaidoftheuseofsomeantihistamines, in particular levocetirizine, whose off-label use was approximately 25%, and almost entirely due toits use in childrenagedundertheauthorisedage.Asof2009,theFDA approvedprescribingthisdrugforchildrenandinfantsfrom six months of age22 after publication of long-term trials
thatdemonstrateditssafetyandefficacyinthispaediatric population.23 Inourpharmaceuticalmarket,levocetirizine
isstillonlyapprovedforchildrenaged>2years.11Asinthe
above-mentioned case, if the indications were the same onbothcontinents,off-labelprescribingofthisdrugwould havebeenirrelevant.
Regardingtopicalimmunomodulators,pimecrolimuswas prescribedforonlythreecasesofatopiceczema,butalways off-label for age, despite its use being justified by clini-calseverity.Thispathologyappearsinover60%ofpatients before the age of 12 months;24 however, these drugs are
onlyapprovedfor childrenaged>2yearsby boththeFDA andEMA.11,22,25 Thislimitationwasimposedbecausethere
arenocurrentstudiesoflong-termsafetythataredeemed sufficientforapprovalinyoungerchildren.Theconcernsof theregulatoryauthoritiesarebasedonthetheoreticalrisk ofsystemicimmunosuppressionderivedfromtheuseoforal calcineurininhibitorssuchaspimecrolimusortacrolimusin transplantrecipients,andtheexistenceofrareinstancesof malignancyassociatedwiththeiruse.26 However,
pharma-cokineticdataobtainedfromclinicaltrialsinchildrenaged <2yearsdidnotsuggestconcentrationshighenoughtocause systemicimmunosuppression,unlikeoraladministration,or demonstrateacorrelationbetweensystemicconcentrations andpercentagebodysurfaceareatreatedorthedurationof treatment.27 Likewise, therewasnointerferencewiththe
developmentofnormalimmuneresponsestovaccinations.28
Besidesdemonstratingextremeefficacy,thesetrials demon-strate safetydata for ITuse in atopic eczema, but more extensive surveillance is needed to determine long-term safety.Nonetheless,sinceitsintroductiononthemarketin 2001,nodefinitecausalrelationshipbetweentheuseofIT andmalignancyhasbeenestablished.26
Inthisstudy,weconfirmedthattheoff-labeluseof anti-allergicdrugsinpre-school-agedchildrenforthetreatment
of moderate tosevere allergic diseases is high. With few studiesoflong-termsafety,theimplicationsinherentinthis typeofuse becomeevident.The PaediatricCommitteeof theEMA has issued a listof drugs currently administered to children for which information on pharmacokinetics, efficacy, and safety are urgently needed; fluticasone and montelukast,amongothers,wereincluded.29Thestandard
methodconsists of performingrandomised controlled tri-als,whicharelimitedbymethodologicaldifficulties,hence theneed to develop sufficientlyextensive post-marketing observationalstudies in ordertoobtain sufficient data to evaluatethesafetyandefficacyofdrugsusedinpaediatric populations.
Insome emergingdiseasesin ourareaof expertisethe majorityofdrugsavailablethatprovidethebestresultsare usedoff-labelregardlessofage.30
The presence of complete and updated records with detailed information on the drugs used, dosages, routes of administration, and adverse effects are important in obtainingreliabledataessentialforfurtherevaluationofthe safetyandefficacyofdrugsinwhichmorecomplexstudies in children are not feasible for practical and/or ethical reasons.Aswithother populationswithunique character-istics,suchaspregnantwomenandtheelderly,publication anddistributionof thisinformationby thescientific com-munityis critical for the acquisition of new safety data, allowingtheapprovalof newdosages,clinicalindications, and/orprescribingforyoungerchildren,reducingoff-label druguse that, although often appropriate,is not without risks.
Finally,thisstudy shouldincreaseclinicians’awareness ofprescribingdrugsoff-labelsuchthattheyareavailableat anytimetodiscussuseofthedrugswithpatientsandtheir families,aswell asprovide the motivesthat justify their use,valuingbenefitsversusrisks,increasingcomplianceand contributingtoachievebetteroutcomes.
Ethical
disclosures
Protection ofhuman subjects and animalsin research. The authorsdeclare thatnoexperimentswere performed onhumansoranimalsforthisinvestigation.
Patients’ data protection.Confidentiality of data. The authorsdeclarethatnopatientdataappearinthisarticle.
Right to privacy and informed consent.The authors declarethatnopatientdataappearinthisarticle.
Funding
Nonetodeclare.
Conflict
of
interest
Pleasecitethisarticleinpressas:Morais-AlmeidaM,CabralAJ.Off-labelprescribingforallergicdiseasesinpre-school
References
1.GazarianM,KellyM,McPheeJR,GraudinsLV,WardRL,Campbell TJ.Off-labeluseofmedicines:consensusrecommendationsfor evaluatingappropriateness.MedJAust.2006;185:544---8.
2.BurnsJP.Researchinchildren.CritCareMed.2003;31Suppl. 3:S131---6.
3.PandolfiniC,BonatiM.Aliteraturereviewonoff-labeldruguse inchildren.EurJPediatr.2005;164:552---8.
4.ChoonaraI,ConroyS.Unlicensedandoff-labeldrugusein chil-dren:implicationsforsafety.DrugSaf.2002;25:1---5.
5.GhalebMA,BarberN,FranklinBD,YeungVW,KhakiZF,WongIC. Systematicreviewofmedicationerrorsinpediatricpatients. AnnPharmacother.2006;40:1766---76.
6.Collier J. Paediatric prescribing: using unlicensed drugs and medicines outside their licensed indications. Br J Clin Pharmacol.1999;48:5---8.
7.Uses ofdrugs notdescribed inthe packageinsert (off-label uses).Pediatrics.2002;110:181---3.
8.Bennett WM. Off-label use of approved drugs: therapeutic opportunityandchallenges.JAmSocNephrol.2004;15:830---1.
9.tJongGW,ElandIA,SturkenboomMC,vandenAnkerJN, Strick-erf BH. Unlicensed and off-label prescription of respiratory drugstochildren.EurRespirJ.2004;23:310---3.
10.SenEF,VerhammeKM,NeubertA,HsiaY,MurrayM,FelisiM, etal.Assessmentofpediatricasthmadruguseinthree Euro-peancountries;aTEDDYstudy.EurJPediatr.2011;170:81---92.
11.Information aboutauthorized drugs use; 2012. Available at:
www.infarmed.pt/infomed/inicio.php[accessed20.06.12]. 12.Noteforguidanceonclinicalinvestigationofmedicinalproducts
in children. London: European Agency for theEvaluation of MedicinalProductsHMEU;1997.
13.Meadows M. Drug research and children. FDA Consum. 2003;37:12---7.
14.SteinbrookR. Testing medicationsin children.NEnglJMed. 2002;347:1462---70.
15.ICH Guidance E11: Note for guidance on clinical
investi-gation of medicinal products in the paediatric population
(CPMP/ICH/2711/99); 2012 (June). Available from:
http://www.ema.europa.eu/pdfs/human/ich/271199en.pdf
[on-line].
16.AmendingRegulationECNo.1902/2006onmedicinalproducts
for paediatric use; 2012 (June). Available from: http://ec.
europa.eu/health/files/eudralex/vol-1/reg20061902/reg 20061902en.pdf[online].
17.DunneJ.TheEuropeanRegulationonmedicinesforpaediatric use.PaediatrRespirRev.2007;8:177---83.
18.Sammons HM, Choonara I. What is happening to improve drug therapy in children. Paediatr Child Health. 2007;17: 108---10.
19.Infarmed. Utilizac¸ão de medicamentos off-label. Infarmed; 2010.
20.RiordanFA.Useofunlabelledandofflicencedrugsinchildren. Useofunlicenseddrugsmaybe recommendedinguidelines. BMJ.2000;320:1210.
21.McLayJS,TanakaM,Ekins-DaukesS,HelmsPJ.Aprospective questionnaireassessmentofattitudesand experiencesofoff labelprescribingamonghospitalbasedpaediatricians.ArchDis Child.2006;91:584---7.
22.Informations about authorized drugs use obtained on U.S.
Food and Drug Administration (FDA) site; 2012. FDA.
Available online at: http://www.accessdata.fda.gov/scripts/
cder/drugsatfda/index.cfm[accessed20.06.12].
23.Simons FE. Safety of levocetirizine treatment in young atopicchildren:an18-monthstudy.PediatrAllergyImmunol. 2007;18:535---42.
24.Wuthrich B, Schmid-Grendelmeier P. The atopic eczema/dermatitis syndrome. Epidemiology, natural course, and immunology of the IgE-associated (extrinsic) and the nonallergic(intrinsic)AEDS.JInvestigAllergol ClinImmunol. 2003;13:1---5.
25.InformationsaboutauthorizeddrugsuseobtainedonEuropean
Medicines Agency (EMA) site; 2012. EMA. Available online
at: http://www.ema.europa.eu/ema/index.jsp?curl=/pages/ medicines/landing/eparsearch.jsp&mid=WC0b01ac058001d124
[assessed26.06.12].
26.Munzenberger PJ, Montejo JM. Safety of topical cal-cineurin inhibitors for the treatment of atopic dermatitis. Pharmacotherapy.2007;27:1020---8.
27.PatelRR,VanderStratenMR,KormanNJ.Thesafetyand effi-cacyoftacrolimustherapyinpatientsyoungerthan2yearswith atopicdermatitis.ArchDermatol.2003;139:1184---6.
28.Papp KA, Breuer K, Meurer M, Ortonne JP, Potter PC, de ProstY,etal.Long-termtreatmentofatopicdermatitiswith pimecrolimuscream1%ininfantsdoesnotinterferewiththe developmentofprotectiveantibodiesaftervaccination.JAm AcadDermatol.2005;52:247---53.
29.List of paediatrics needs (as established by the
Pae-diatric Working Party); 2012 (June). Available from:
http://www.emea.europa.eu/docs/enGB/documentlibrary/ Other/2009/10/WC500004058.pdf