Survey of Reproductive Health in Young Adults,
Greater Santiago, 19881
M.
SOLANGEVALENZUELAG.,~JOAN
M.HEROLD,~
LEO
Moms,4aILSEL6PEZ
B.5444
This article reports the results of an interview survey with 1,665 residents of Metro- politan Santiago 15-24 years old. The survey, which dealt with various aspects of reproductive health, indicated that the sex education received by 75% of the subjects generally failed to convey an accurate knowledge of the basic concepts of sexuality; that use of contraceptive methods was very limited; that approximately 25% of the 865 women interviewed had been pregnant at some time; and that 40% of all the pregnancies were unplanned. These findings demonstrate a need to begin effective sex education programs and to provide adolescent services commensurate with the circumstances of modern life.
T
he past few decades have witnesseda growing world interest in adoles-
cent fertility, unwanted pregnancy, the
increasing numbers of single mothers,
and in general the reproductive health of both adolescents and young adults (Z-5). To satisfy the need for reliable informa-
tion, surveys on reproductive health
have been conducted on representative
The study reported here was funded by PAHO [Grant HPMIMPMIFP/013/67/3 (l)], the United Nations Population Fund (UNFPA), and the Cen- ter for Population Options (Washington, D.C.). This article will also be published in Spanish in the Boletz’n de la Oficina Sanitaria Panamericma, Vol. 112, No. 1,199Z.
2Department of Public Health, Division of Medical Sciences, West Campus, School of Medicine, Uni- versitv of Chile, Santiago, Chile. Mailine address: Depakamento de SaludYl%blica, Divisi& Ciencias Medicas Occidente, Facultad de Medicina, Univer- sidad de Chile, Casilla 33052, Correo 33, Santiago, Chile.
sEmory University School of Public Health and Di- vision of Reproductive Health, United States Cen- ters for Disease Control, Atlanta, Georgia, U.S.A. 4Division of Reproductive Health, United States
Centers for D&ease Control, Atlanta, Georgia, U.S.A.
sSchoo1 of Public Health, Faculty of Medicine, Uni- versity of Chile, Santiago, Chile.
samples of young people of both sexes in
various countries. Within the area of
Latin America and the Caribbean, spe-
cific reference may be made to studies
performed in Brazil, Ecuador, Gua-
temala, Jamaica, and Mexico (6-20). In Chile, scattered efforts have pro- vided information on some aspects of fer- tility. Among other things, a stable ado- lescent fertility rate has been found that contrasts sharply with a decreased fertil- ity rate found among women 25 to 34 years of age. Also, a marked increase has been found in births to single women,
particularly adolescents: In 1965, 29.6%
of all live births to young people under 20 were illegitimate; as of 1987 this figure had risen to 58.2%. Similarly, 18.8% of the births to mothers in all age groups were illegitimate in 1965, as compared to 32.8% in 1987 (11, 22).
Certain aspects of young people’s re-
productive health in our country have
not been considered for lack of data. In particular, no information has been avail- able regarding the frequency of premari- tal sexual activity and use of contracep- tives. Nor have evaluations been made of
the sex education provided to young peo- ple inside or outside the school system.
The above trends, along with other
considerations, point to a need for better
knowledge of the sexual behavior and
fertility patterns of adolescents and
young adults in Chile-in conjunction
with knowledge of their beliefs, atti-
tudes, sexual activities, and use of con- traceptive methods. Chile did not partici- pate in the last World Fertility Survey; and failure to do so, combined with the
great sociodemographic and political
changes that took place during the 1970s and 198Os, have made it essential for the country to have reliable and current in-
formation. Against this backdrop, the
study reported here sought to provide
needed data about the reproductive
knowledge, sexual activity patterns, and
contraceptive attitudes and practices
among young people between the ages of 15 and 24 in Greater Santiago.
The investigation was funded by the
Pan American Health Organization,
the United Nations Population Fund
(UNFPA), and the Center for Population
Options in Washington, D.C. Technical
assistance and long-term collaboration
were provided by the Reproductive
Health Division of the United States Cen- ters for Disease Control (CDC). The proj- ect was sponsored by the Chilean Minis- try of Health and the School of Medicine of the University of Chile.
MATERIALS AND METHODS
The study population or universe con-
sisted of young men and women be-
tween 15 and 24 years of age residing in
the urban area of the Metropolitan Re-
gion of Santiago (Greater Santiago).
According to the 1982 census (the XV Na-
tional Population and IV Housing
Census), this area then had a total popu- lation of 903,000 inhabitants.
A multiphased, self-weighted proba-
294 Bulletin of PAHO 25(4), 1991
bility sample, which did not substitute subjects already selected, was designed for the entire urban area of Santiago,
thereby ensuring due representation of
all socioeconomic sectors. The final phase
consisted of random selection of the
households from which the young peo-
ple were to be recruited for the survey.
This selection was carried out on the
basis of information provided by the
census (13).
The census divided the metropolitan
region into 34 communities (comunas),
each subdivided into census districts. In all there were 265 census districts, the
number of districts in a given ccmuna
varying from 2 to 28 depending on the
comuna’s size. Sixty-three of these dis- tricts were selected in the first phase of
the study, using a probability propor-
tional to each com~rzu’s size. These dis-
tricts constituted the primary sampling
units (PSU). Within each unit, the num- ber of households needed to obtain a rep-
resentative number of interviews with
subjects of each sex was assessed on the
basis of a hypothetical assumption that
each occupied home contained 0.54
women and 0.51 men.
Independent samples were selected by
sex. In each KU, groups or conglom-
erates of equal numbers of households were defined and numbered in a correla- tive fashion. Then, in each unit, one con-
glomerate was selected at random for
women and the next one was selected for men.
In designing the questionnaire to meet the aims of the study, those topics con-
sidered most important were selected,
and the variables to be investigated by the study were specified for each. Be- cause of the private nature of the subject matter under investigation, particular at- tention was given to preparing the ques- tionnaire so as to elicit a cooperative re-
sponse from those interviewed. Also,
questions), efforts were made to ensure that it would not be monotonous or bor-
ing. Some of the questions used were
taken from previous surveys on the re-
productive health of young people that
had been carried out in Guatemala and
Brazil (B-10), while others were new
questions devised in accordance with the specific aims of the Santiago study.
A pilot project was carried out during a one-week period in May 1988. The inter-
viewers, the great majority of whom
were health professionals with previous
survey experience, received 40 hours of training and submitted the questionnaire to 100 young people, 50 of each sex. This activity made it possible to examine each question’s relevance and clarity in terms
of the responses received, and also to
identify problem areas. Among other
things, the results provided a basis for
reformulating certain questions, insert-
ing new response categories into the
questionnaire, and confirming the
usefulness of the interviewer’s manual. Before work in the field began, another
training period of 40 additional hours
was provided to the field team members.
These were organized into two teams,
one of men and one of women, each con- sisting of five interviewers and one su- pervisor. There was also a field coordina-
tor who supervised the interviewers
jointly with the corresponding team su-
pervisor. The activities of both teams
were also regulated by the principal
investigator and by guidance provided
through a computer program: The sur-
vey proper was conducted during Sep-
tember, October, and the first two weeks of November 1988.
RESULTS
Interview Response
Following the described procedure,
2,898 households in the male sample and
an equal number in the female sample
were visited. In accordance with the
household questionnaire, the names of
all male or female household residents
between 15 and 24 years of age were re- quested, and these became the subjects eligible for individual interviews. This process located eligible young people in slightly over a quarter of the households visited. The household visits elicited no positive response at small percentages of the residences surveyed (5.7% and 5.3% of those in the female and male samples,
respectively), while in the remaining
households (67.9% and 69.3% respec-
tively) no eligible young person was
named.
As Table 1 indicates, individual inter- views were completed with 88.0% of the
Table 1. Results of household and individual surveys designed to locate and interview young men and women 15-24 years old in the Santiago Metropolitan Area in 1988, by sex.
Female Male sample % sample % Housing survey results:
No young person 15-24 in residence
Young person 15-24 in residence
No cooperation Residence vacant Tenants absent Other
Total
(No. of households) Individual survey results: Interview completed Interview refused Young person absent Informant inadequate Other
Total
(No. of possible interviews) (No. of interviews
completed) (Average length, in
minutes, of completed interview)
67.9
26.4 25.3 3.1 4.0 2.4 1.2 0.1 0.0 0.1 0.1 100.0 100.0 GW’8) C&898)
88.0 83.9 7.3 4.7 4.1 9.9 0.6 0.6 0.0 0.9 100.0 100.0
(9831
(865)
(21.2)
69.3
(954)
(800)
(23.8)
983 eligible female subjects and 83.9% of the 954 eligible male subjects. The lower response rate for men was mainly attrib- utable to the difficulty of finding young men at home, even after six or more visits. In addition, 7.3% of the women
and 4.7% of the men refused the inter- view; this group includes both those who refused to answer any of the questions
and those who stopped during the
course of the interview. In all, interviews were completed with 865 women and 800 men.
Comparison with Other Data
Because no other recent survey existed with which to compare the characteristics of our interview subjects, the 1982 census (23) was used for this purpose. Poten- tially, this comparison could provide as- sistance in assessing the reliability of
information regarding our interview sub-
jects’ age and civil status. (Since the
census provided data on the general
household population and our survey
also employed a representative house-
hold sample, it was expected that a simi-
lar percentage distribution would be
found in both cases.) In addition, it was
possible that the comparison might de-
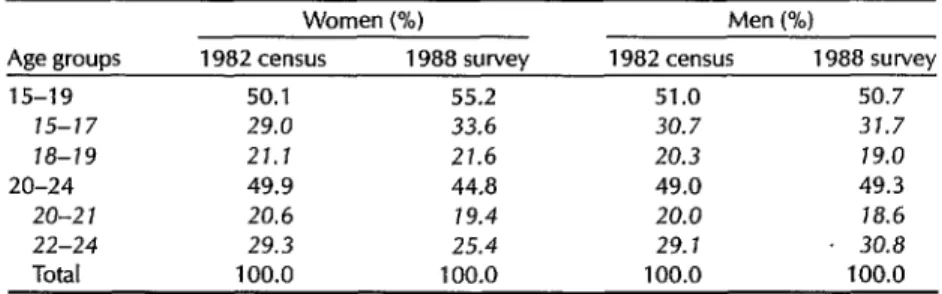
tect recent changes in these distributions. As Table 2 shows, our survey found a higher percentage of girls 15 to 19 years
old in the 15-24 age group than did the
census. This could have reflected in-
creased migration by adolescents in this age group to the capital city in recent years; or, alternatively, it could have re- flected a failure by our survey to include
a representative percentage of young wo-
men between the ages of 20 and 24 in the sample. More detailed study of the fig- ures showed that our survey obviously
undercounted young women from 22 to
24 years of age and overcounted those
between 15 and 17. The age distribution
of males indicated by our survey was
quite similar to that indicated by the
census.
Sex Education
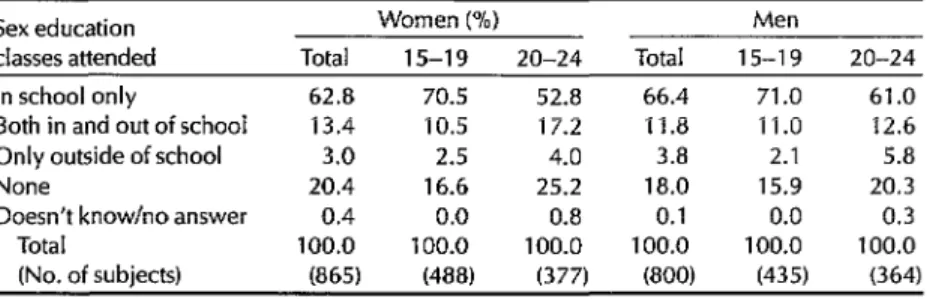
The proportion of our young survey
subjects who had received sex education
at school is noteworthy-more than 75%
in both sexes. Nevertheless, a group still remained that had not attended sex edu- cation classes either inside or outside the school system (Table 3).
It should also be mentioned that the first class of this kind, both for males and females, is received between the ages of 12 and 15, mostly in the eighth grade. Because a substantial percentage of chil- dren drop out of school in the eighth grade, it seems clear that starting sex ed- ucation there causes a significant number
Table 2. Distribution of the 1988 Santiago interview subjects by age group, as compared to the distribution within comparable age groups in the 1982 census, by sex.
Age groups
15-19 ts-17 18-19 20-24
20-Z 1 22-24 Total
Women (%) Men (%)
1982 census 1988 survey 1982 census 1988 survey 50.1 55.2 51.0 50.7 29.0 33.6 30.7 31.7
21.1 21.6 20.3 19.0
49.9 44.8 49.0 49.3
20.6 19.4 20.0 18.6
29.3 25.4 29. I 30.8 100.0 100.0 100.0 100.0
Table 3. Percentages of the 1988 Santiago survey subjects attending sex education classes in or outside the school svstem.
Sex education Women (%) Men
classes attended Total 15-19 20-24 Total 15-19 20-24 In school only
Both in and out of school Only outside of school None
Doesn’t know/no answer Total
(No. of subjects)
62.8 70.5 52.8 66.4 71 .o 61.0 13.4 10.5 17.2 11.8 11.0 12.6 3.0 2.5 4.0 3.8 2.1 5.8 20.4 16.6 25.2 18.0 15.9 20.3
0.4 0.0 0.8 0.1 0.0 0.3 100.0 100.0 100.0 100.0 100.0 100.0
(865) (488) (377) (800) (435) (364)
of students to be missed. In any case, for other reasons it is too late an age to un- dertake this kind of instruction.
The great majority of those who taught the first classes in sex education were regular schoolteachers. It is of course es- sential for such professionals to receive
proper training before undertaking this
task. Outside of school, the church was
the place providing most young people
with sex education.
The subjects most discussed in both the school and outside classes were sex-
ual development and the biology of re-
production, with stress on the menstrual cycle. Sexually transmitted diseases were
most often mentioned as being among
the subjects of greatest concern to young
people. It is noteworthy that a large per-
centage of the female survey subjects
(61.9%) indicated they had never at-
tended sex education classes or had at- tended them only after having had their first menstrual period (Table 4).
Outside of these systematic sex educa- tion classes, those who most frequently
provided advice on these matters were
mothers in the case of young women and male friends in the case of young men. An appreciable number of students said they had received no such advice at all.
In general, the survey only measured the quantity of education or information provided; and while it showed that a sig- nificant proportion of the young people
surveyed had attended sex education
Table 4. Percentages of female survey subjects who attended sex education classes and discussed menstruation with their mothers before and after menarche.
Sex education Total
Discussed Did not discuss menstruation menstruation
with mother with mother before menarche before menarche Did not attend classes 23.5 1 a.3 34.5 Had a course after menarche 38.4 38.5 37.7 Had a course the same year as menarche 16.4 19.0 10.7 Had a course before menarche 20.5 23.1 15.3 Doesn’t know/no answer 1.3 1.0 1.8
Total 100.0 100.0 100.0
(No. of subjects) (865)a (579) C-281) aThis total includes fwe subjects who did not remember the dates of their menarche or first sex education class. These subjects are not listed elsewhere in the table.
classes, it provided no
clear
knowledge regarding the qualityof
this information or instruction.Sexual Experience and Use of
Contraceptive Methods
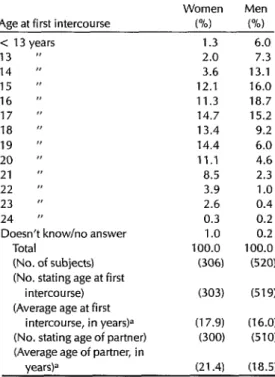
The survey indicated that 35.4% of the
women interviewed and 45% of the men
had premarital sexual relations. The aver- age age of their first premarital sexual ex-
perience was 17.9 years for the women
and 16.0 years for the men (Table 5).
Their partners, on the average, were
3.5 years older in the case of the women and 2.5 years older in the case of the
men. The young women’s partners in
this first sexual experience were mostly
steady boyfriends, and the young men’s
were mostly steady or other girlfriends. Only a small percentage of male sexual initiations took place with prostitutes.
Table 5. Age at first intercourse of those study subjects with premarital sexual experience.
Women Men Age at first intercourse w rw < 13 years
13 I’ 14 " 15 " 16 " 17 "
ia
11
19 ” 20 " 21 " 22 'I 23 " 24 "
Doesn’t know/no answer Total
(No. of subjects) (No. stating age at first
intercourse) (Average age at first
intercourse, in years)a (No. stating age of partner) (Average age of partner, in
1.3 6.0 2.0 7.3 3.6 13.1 12.1 16.0 11.3 is.7 14.7 15.2 13.4 9.2 14.4 6.0 11.1 4.6 a.5 2.3 3.9 1 .o 2.6 0.4 0.3 0.2 1.0 0.2 100.0 100.0
(306) 62’3
(303)
(17.9) (300)
619)
(16.0) (510)
yearsP (21.4) (la.51 aExcludingthose who said they did notknowordidn't answer.
Generally speaking, the most common
feelings following sexual initiation were love and fear among the women, plea- sure and elation among the men.
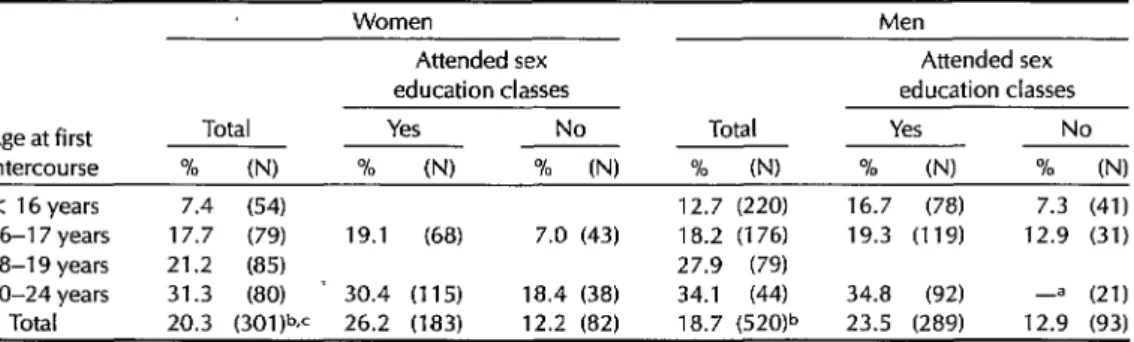
About a fifth of these subjects (20.3% of the women and 18.7% of the men)
used some contraceptive method during
their first premarital sexual relations. As Table 6 indicates, these percentages were higher among subjects who were older at
first intercourse and among those who
had received prior sex education. The
rhythm method was the method used
most commonly during initial premarital
intercourse by subjects of both sexes.
This was followed in second place by oral contraceptives, and in third place by ei- ther condoms (used by partners of the
women interviewed) or coitus inter-
ruptus (employed by the men inter-
viewed). According to the women inter-
viewed, the decision to use a birth
control method was mutual, whereas the
men more frequently said that it was
their partners who made this decision.
The reason most frequently given for
not using contraceptives was the unex-
pectedness of the sexual encounter (“I
didn’t
expect to have sexual relations atthat time”). The other reason given
(which was inversely correlated with the age of initiation) was ignorance of any method. Both reasons may be interpreted as deriving from a lack of preparation for sexual life.
As indicated in Table 7, about a third of the unmarried subjects with sexual expe- rience indicated they were sexually active at the time of the interview (reporting that they had had sexual relations within
the preceding four weeks). Of these,
100% of the women and 92% of the men declared themselves to be monogamous. It is also worth noting that by and large young people do not appear to have fre-
quent intercourse, a circumstance that
gives them special contraceptive needs.
Within this context, it should be
Table 6. Percentages of survey subjects with premarital sexual experience who used contraceptive methods in their first sexual relations, by age at first intercourse and whether or not sex education classes were attended before initiation of sexual relations. In each case the percentage using contraceptive methods is shown together with the number of subjects in the group.
Age at first intercourse
Total 70 (N)
Women Men
Attended sex Attended sex education classes education classes
Yes No Total Yes No
70 (I’4 ~ % (NJ % N % N ~ % N < 16 years 7.4 (54) 12.7 (220) 16.7 (78) 7.3 (41) 16-l 7 years 17.7 (79) 19.1 (68) 7.0 (43) 18.2 (176) 19.3 (119) 12.9 (31) 18-l 9 years 21.2 (85) 27.9 (79)
20-24 years 31.3 (80) ’ 30.4 (115) 18.4 (38) 34.1 (44) 34.8 (92) -= (21) Total 20.3 (301F 26.2 (183) 12.2 (82) 18.7 (520)” 23.5 (289) 12.9 (93) aThe percentage was not calculated when the basewas less than 25 subjects.
bThis total includes subjects who did not recall their age at first intercourse or at the time of their first sex education class, as well as subjects who had their first sex education class at the same age as their first intercourse. These subjects are not included elsewhere in the table.
cThis total excludes five women who reported their first intercourse as rape.
Table 7. Percentages of unmarried survey subjects who had sexual relations within the four weeks preceding the interview and the percentages using contraceptive methods, by age and sex.
Women Men
Total 15-19 20-24 Total 15-19 20-24 % INI % (N) % (N) % (NJ % (NI % (NJ Had sexual relations
within the last
four weeks 36.9 (179)= 43.3 (67)= 33.0 (1 12)a 29.3 (451P 21.6 (199)” 35.3 (252P Used a
contraceptive
methodb 65.2 (66)~ 48.3 (29)= 78.4 (37)= 59.5 (131jc 57.1 KY 60.7 (89)c aThe number of unmarried subjects with sexual experience.
bThese data do not include one male subject who reported the intercourse as rape.
<The number of unmarried subjects who had sexual relations within four weeks of the intervrew.
pointed out that although general data
on use of contraceptive methods in Chile are not available, it is known that at pres- ent some 54.8% of the married women in Santiago between the ages of 15 and 24 use contraceptives, most of which are ob- tamed from public hospitals and clinics;
national birth rate data suggest that a
similar contraceptive use pattern prevails in other parts of the country.
Reproduction
A total of 24.3% of the young women
interviewed had been pregnant at some
time in their lives, and among the sub-
sample that was sexually experienced
this percentage increased to 62.4%. The percentage was even higher among those who had their first sexual experience af- ter marriage, 85.0% of whom had been pregnant (Table 8).
Of the women with premarital sexual
experience who had become pregnant, 26.5% had had more than one pregnancy (Table 9). This figure is lower than that obtained by a Guatemalan survey, which found that 47.0% of those interviewed had had more than one pregnancy (8).
More than 60.0% of the first live births
Table 8. Percentage of women interviewed who reported having been pregnant, grouped according to age and whether they had sexual relations before marriage.
Women with prior sexual experience Postmarital Premarital Age group All women Total experience ’ experience
in years % (NJ % N % (N) % N
15-17 4.1 (295) 33.3 (33) -= (0) 33.3 (33) 18-19 21.8 (193) 67.7 (62) -= (3) 67.8 (59) 20-24 41.4 (377) 65.3 (239) 88.0 (25) 62.6 (214) Total 24.3 (865) 62.6 (334) 85.7 (28) 60.5 (306) AThe percentage was not calculated when the base was less than 25 subjects.
Table 9. Percentage distribution of the women interviewed who had been pregnant according to the number of pregnancies reported, the subjects’ ages, and sexual experience.
Premarital sexual Number of Age in years experience BreQnancies Total 15-19 20-24 No Yes
1 71.4 81.5 68.0 -a 73.5
2 25.7 18.5 28.2 -a 23.8
3 2.9 0.0 3.8 -a 2.7
Total 100.0 100.0 100.0 100.0 (No. of subjects) (210)” (54) (156) ii; (185) aThe percentage was not calculated when the base was less than 25 subjects.
bThis total includes one subject who did not recall the date of first intercourse and who is not included in the “premarital sexual experience” columns.
reported by our survey subjects resulted from premarital conception. This leads to the conjecture that a significant propor- tion of young women make hasty mar- riages or give birth to a child while still single. In the process, they and their chil-
dren suffer major hardships, since most
of these mothers are compelled to drop out of school, become underemployed,
and contend with a motherhood for
which they are commonly unprepared.
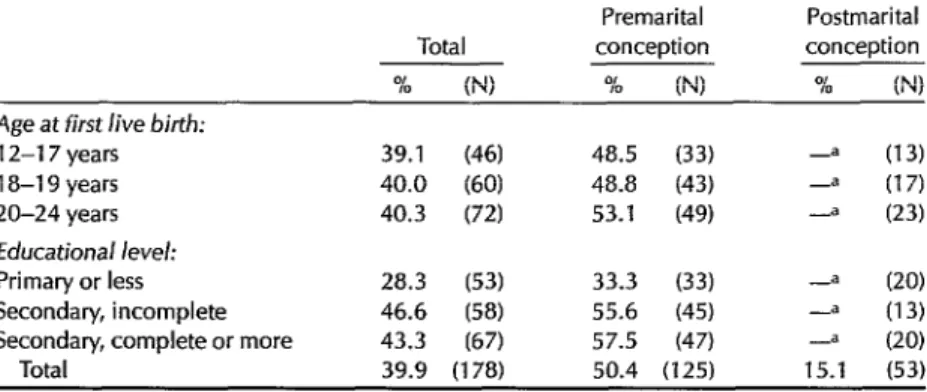
The high percentage of unplanned
pregnancies detected by the survey also
seems important. Overall, 39.9% of the
first live births reported in our survey
were unplanned, this figure rising to
50.4% among those resulting from pre-
marital conception (Table 10). In view of the fact that more than 90% of the
women involved received prenatal care
whether their pregnancies were planned
300 Bulletin of PAHO 25(4), 1991
or not, prenatal care should be better uti- lized for the purpose of preventing sub- sequent unwanted pregnancies.
Knowledge and Attitudes
The low percentage of young people who knew the time of a woman’s fertile period was surprising.6 Indeed, the per-
centage with this knowledge was low
among those who had received sex edu- cation (28.7% among the women, 25.2% among the men) as well as among those who had not. The percentages of young
Table 10. Percentages of women interviewed who said their first live births resulted from conceptions that were unplanned, by age group, educational level, and whether conception occurred before or after marriage.
Premarital Postmarital Total conception conception
% (NJ % N % U-4
Age at first live birth:
12-l 7 years 39.1 WI 48.5 (33) -= (13) 18-l 9 years 40.0 (60) 48.8 (43) -a (17) 20-24 years 40.3 (72) 53.1 (49) -= (23)
Educational level:
Primary or less 28.3 (53) 33.3 (33) -= (20)
Secondary, incomplete 46.6 (58) 55.6 (45) --a (13) Secondary, complete or more 43.3 (67) 57.5 (47) --a (20)
Total 39.9 (178) 50.4 (125) 15.1 (53) aThe percentage was not calculated when the base was less than 25 subjects.
Table 11. Percentages of interview subjects who answered correctly regarding a woman’s fertile period by age group, sex, educational level, and sex education.
Age group: 15-l 9 years 20-24 years Educational level: Primary or less Secondary, incomplete Secondary, complete or more Sex education:
Attended class No class
Women Men
% N % N
27.9 (488) 20.2 (435P 25.2 (377) 27.5 (364)"
11.7 (171) 11.5 (157) 22.4 (349) 19.8 (313) 38.6 (345) 33.0 (330)
28.7 (686P 25.2 (655)a 19.3 (1 76ja 16.7 (144P Total 26.7 (865) 23.5 18OOJ
aThe indicated figures do not include three women and one man who did not answer the question about sex education.
men and women with this knowledge were higher among those with higher ed- ucational levels (Table 11).
The contraceptive methods given most
use and widest circulation (oral contra-
ceptives, intrauterine devices, condoms,
etc.) were also the ones known best by both our male and female survey partici- pants. And conversely, the methods that were least used and circulated (vaginal methods, the Billings method, etc.) were also the least known by our subjects.
With regard to sexually transmitted
diseases, we found that the least known to members of both sexes was syphilis, while the best known was AIDS. More
than 80.0% correctly answered a ques-
tion7 regarding who transmits these dis- eases, but the percentage answering cor- rectly was found to vary in accordance with the subjects’ educational level and
The question, posed after one asking about knowl- edge of sexually transmitted diseases, was “Who transmits these diseases? (1) both sexes, (2) only men, (3) only women, (4) depends on the disease, (5) don’t know, (6) no answer.”
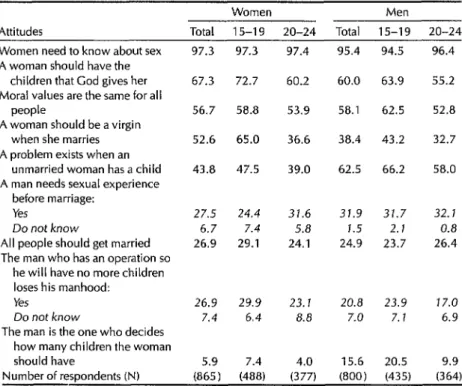
Table 12. Percentages of study subjects providing affirmative answers= to questions on attitudes toward sex roles, by age and sex.
Women Men
Attitudes Total 15-l 9 20-24 Total 15-l 9 20-24 Women need to know about sex
A woman should have the children that God gives her Moral values are the same for all
people
A woman should be a virgin when she marries A problem exists when an
unmarried woman has a child A man needs sexual experience
before marriage: Yes
Do not know
All people should get married The man who has an operation so
he will have no more children loses his manhood:
Yes Do not know
The man is the one who decides how many children the woman should have
97.3 97.3
67.3 72.7
56.7 58.8
52.6 65.0
43.8 47.5
27.5 24.4 31.6 6.7 7.4 5.8 26.9 29.1 24.1
26.9 29.9 23. I 20.8 23.9 77.0 7.4 6.4 8.8 7.0 7. I 6.9
5.9 7.4
97.4 96.4
60.2
95.4 94.5
60.0 63.9
58.1 62.5
38.4 43.2
62.5 66.2
31.9 31.7 1.5 2.1 24.9 23.7
55.2
53.9 52.8
36.6 32.7
39.0 58.0
32.1 0.8 26.4
4.0 15.6 20.5 9.9 Number of respondents (N) (865) (488) (377) (800) (435) (364)
aBesides the percentages answering affirmatively, those saying they “do not know” are listed when they equaled 5% or more of the total respondents of one or both sexes.
whether or not they had attended sex ed- ucation classes.
Regarding gender roles, over 95% of
the young people interviewed thought
that women needed to know about sex; however, only about 30% of those sur- veyed felt that sexual experience before marriage was necessary for men. Many
of the young women 15-19 years old
(65.0%) felt virginity to be an important condition for marriage, but this percent- age was lower among women in the 20- 24 year group and among the men in general (Table 12).
principally because the respondents saw
it as a way for a woman to realize herself, an opinion more prevalent among those
with higher educational levels. Accep-
tance of female employment for eco-
nomic reasons was more frequent among those with lower educational levels.
Many of the answers provided during
the interviews indicated that survey
subjects with higher educational levels
tended to adhere less strongly to con-
servative values.
Nearly half of the survey subjects re- ported that drugs posed the most com- mon problem for young people in San-
tiago. A considerable number of others
(around 18%) felt the most common diffi-
culties arose from family conflicts and
lack of communication with parents (Ta-
ble 13).
Acquired Immunodeficiency
Syndrome (AIDS)
A large percentage of those inter- More than 90% of the young people
viewed believed that women should interviewed knew the three principal
work once they were married. This was ways in which AIDS is contracted:
Table 13. Percentages of survey subjects who cited particular problems as being the most common among young people, by sex.
Most common problem
Women Men (W (%) Drugs
Smoking habit Alcoholism
Drugs and alcoholism, drugs and cigarettes, drugs and smoking habit
Lack of communication with parents and family problems
Adolescent pregnancy Unemployment Violence and political
problems
Lack of money, lack of opportunity
Insecurity about the future, disorientation
Othera
Doesn’t know/no answer Total
45.1 49.6 3.0 3.8 2.8 5.1
1.7 1.8
1 9.7 16.0 7.3 1.4 5.3 8.6
2.5 5.8
1.5 0.9
2.8 1.6 6.8 4.8 1.5 0.8 100.0 100.0 Number of subjects (N) (865) (800) aIncludes great sexual freedom. lack of information about sex, and others.
through sexual relations, blood transfu-
sions, and injections. However, a large
number also believed AIDS could be
transmitted by bathroom facilities or din- nerware used by infected persons.
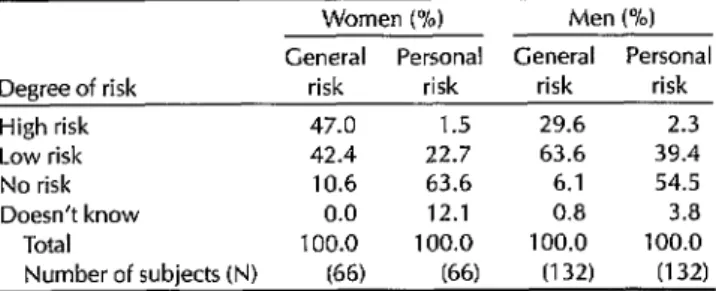
In assessing the AIDS risk faced by
various population groups, our survey
subjects generally assigned the greatest risk to those actually running the greatest risk. Roughly a third of the survey sub- jects (both men and women) also recog-
nized that they themselves faced some
risk. However, as Table 14 shows, most
believed themselves to be at low risk, less than 3.0% saying they considered them- selves to be at high risk. Moreover, as indicated in Table 15, young, sexually ac- tive interview subjects tended to assign
less risk to themselves than they as-
signed to members of the general popula- tion in similar circumstances. These find- ings suggest that young sexually active people view AIDS as a disease that may affect others but is unlikely to affect themselves.
DISCUSSION AND CONCLUSIONS
Of the sexually experienced interview As already noted, this survey obtained
subjects, only 21.3% of the women and its data from young people at all socio-
51.5% of the men were practicing some
form of prevention. The principal rea-
sons given for not taking preventive mea- sures were that they were involved in a stable relationship, they did not believe that contagion was possible, or that they
had relations only with people whom
they knew.
Table 14. Distribution of the interview subjects according to the degree of AIDS risk they attributed to themselves, by marital status and sexual experience. The figures do not include one man and one woman who did not provide answers regarding their sexual experience.
Women Men
Unmarried Unmarried With Without With Without sexual sexual sexual sexual Degree of risk Married experience experience Married experience experience High risk 1.9 2.2 1.9 2.8 2.2 0.4 Low risk 25.2 22.3 30.4 33.3 35.4 24.4 No risk 60.7 62.6 58.7 59.7 58.0 71.6 Doesn’t know 12.3 12.3 8.9 4.2 4.4 3.6 No answer 0.0 0.6 0.2 0.0 0.0 0.0 Total 100.0 100.0 100.0 100.0 100.0 100.0 Number of subjects (N) (155) (179) (530) (72) (452) (275)
Table 15. Degrees of AIDS risk that unmarried, sexually active interview subjects attributed to themselves and to other unmarried sexually active young people.
Women Y/O) Men (%) General Personal General Personal Degree of risk risk risk risk risk High risk 47.0 1.5 29.6 2.3 Low risk 42.4 22.7 63.6 39.4 No risk 10.6 63.6 6.1 54.5 Doesn’t know 0.0 12.1 0.8 3.8
Total 100.0 100.0 100.0 100.0 Number of subjects(N) (66) 66) (132) (132)
economic levels in Greater Santiago by means of a sampling procedure that en- sured all sectors were appropriately rep-
resented. It is therefore important to
make an in-depth analysis of some of the findings.
Among the conclusions derived from
the assessment presented here are the
following:
Although a sizable proportion of the
interview subjects had attended sex edu-
cation classes, an appreciable number
had not. It is therefore important to seek
ways of providing information and edu-
cation about sex to those who have not had access to systematic sex education. It
is also of fundamental importance to
train those responsible for imparting
knowledge of this nature, most of whom
are regular schoolteachers without spe-
cific expertise in this field.
Just as important as training educators is the need to change the concept of sex education, which at the present time con- sists almost entirely of education about
sexual development and the biology of
reproduction.
Finally, although the survey shows
that a large percentage of young people have engaged in premarital sexual activ- ity, it also shows that there has been little use of contraceptive methods. This real- ity has created an urgent need to facilitate
access to family planning services-ser-
304 Bulletin ofPAH0 2X4), 2991
vices that afford one way of diminishing,
and ideally preventing, the large and
daily growing numbers of illegitimate
and unwanted children being born in our country.
REFERENCES
1.
2.
3.
4.
5.
World Health Organization. Health prob- lems of adolescence: report
of
a WHO expertcommittee. Geneva: 1965. (WHO Technical
Report Series, no 308).
Chile, Servicio de Salud, Valparafso. Sim- posio de salud integral para la adolescente: temas diversos. Vii’ia de1 Mar, Chile: 1981. Population Information Program. Fecun- didad adolescenfe, riesgos y consecuencias: edad al casarse y fecundidad. Washington, DC: George Washington University; 1982.
Darabi K, Philliber GS, Rosenfield A. A perspective on adolescent fertility in de- veloping countries. Sfud Fam Plunn. 1979;10(10):300.
Morris L. Fecundidad adolescente en las Americas: datos y definiciones del prob- lema. In: Monroy de Velasco A, Martinez J (eds). Memoria de la Primera Reunio’n lnter- national sobre Salud Sexual y Reproductiva de 10s Adolescenfes y Jhenes. Mexico City: 1986.
cidn para Adolescentes (CORA) y Aca- demia Mexicana de Investigacidn en Demograffa Medica; 1987.
7. Jamaica, National Family Planning Board. Jamaica Young Adult Reproductive Sur- vey 1987: prehrninary report. Kingston: 1987.
8. Asociacidn Guatemaheca de Education Sexual (AGES). Encuesta sobre salud y educacidn sexual de jovenes: reporte fi- nal. Guatemala City: 1988.
9. Universidad Federal de Bahia. SaIud y ed- ucacion sexual de1 joven bahiano: reporte prehminar. Salvador, Brazil: 1988.
10. Proaiio B, Paez E lnforme preliminar de la
Encuesta de lnfortnacick y Experiencia Repro- ductiva de 10s Jbvenes Ecuatorianos en Quito y Guayaquil1989. Quito: 1989.
11. Chile, Instituto NacionaI de Estadfsticas (INE). Demografia. Santiago: 1984, 1985, 1986.
12. Barrfa EM, Wderrama RE, Eckardt S. Caracterfsticas de1 embarazo, parto y perf- odo neonatal precoz se&n legitimidad. Rev Chil Pediatr. 1982;53:589.
13. Chile, Instituto NacionaI de Estadfsticas (INE). XV Censo National de PobZaci6n y IV de Vivienda: Regio’n Metropolitana de San- tiago, AbriZ 1982 (vol 1). Santiago: Minis- terio de Economfa; 1986.
444
Building a Tobacco-#?ee
World
The 8th World Conference on Tobacco or Health will take place in Buenos Aires, Argentina, from 30 March to 3 April 1992. The meeting, sponsored
by the American Cancer Society, the Union Antitabaquica Argentina, and
the Latin American Coordinating Committee against Smoking, is the first of these conferences to be held in a developing country and the first to highlight the needs of developing countries in Latin America, Africa, and
Southeast Asia targeted by the multinational tobacco companies. The Pan
American Health Organization is among the official cosponsors.
The conference, subtitled “Building a Tobacco-free World,” will focus on four main themes: countering tobacco advertising, marketing, and pro- motior; preventing tobacco use by children; establishing clean indoor air policies; and building support for tobacco control. Plenary speeches and panel discussions related to the major topic areas will be augmented by skills-building workshops and scientific paper presentations. Each after- noon will feature regional planning sessions to assist in the development of country plans and regional support networks, particularly for develop- ing countries.
The Honorary Chairman of the conference, Surgeon General of the United States of America, Antonia Novello, M.D., will deliver the opening address and introduce the U.S. Surgeon General’s report on smoking in the Americas, the first to focus on the effects of tobacco outside the United
States. Former president Jimmy Carter will give the closing speech.
For further information, contact: Secretariat/Bth World Conference on
Tobacco or Health, c/o American Cancer Society, 1599 Clifton Road NE, Atlanta, GA 30329; telephone (404) 329-7575.