309
Revista da Sociedade Brasileira de Medicina Tropical 44(3):309-312, mai-jun, 2011
INTRODUCTION
1. Departamento de Estudos em Microbiologia, Universidade Gulbarga, Gulbarga, Karnataka, India. 2. Departamento de Microbiologia, Faculdade de Gestão Administrativa, Bangalore, India. 3. Departamento de Microbiologia, Faculdade de Medicina St. John’s, Bangalore, India. 4. Curso de Odontologia, Faculdade Seema, Ghaziabad, India. 5. Departamento de Biotecnologia e Tecnologia de Alimentos, Universidade de Tecnologia, Durban, Africa do Sul.
Address to: Dr. Rajendra Goud. Depto Microbiologia/Faculdade de Gestão Administrativa. 560083
Bangalore, India. Phone: 91 80 2782-8657 e-mail: [email protected] Received in 05/10/2010 Accepted in 19/01/2011
Community prevalence of methicillin and vancomycin resistant
Staphylococcus aureus
in and around Bangalore, southern India
Prevalência de
Staphylococcus aureus
resistente à meticilina e à vancomicina em comunidade
no entorno de Bangalore, Índia do Sul
Rajendra Goud
1,2, Soham Gupta
3, Ujjwal Neogi
2,3, Deepali Agarwal
4, Kesava Naidu
1, Raju Chalannavar
5and Gaddad Subhaschandra
1ABSTACT
Introduction: Staphylococcus aureus is a known colonizer in humans and has been implicated in community acquired sot tissue infections. However emergence of methicillin resistant S. aureus
(MRSA) has aroused great concern worldwide. his study aimed to determine the prevalence of MRSA in the community of Bangalore, southern India. Methods: Swabs were collected from anterior nares, forearm, dorsum and palm of the hands of 1,000 healthy individuals residing in and around Bangalore, belonging to diferent socioeconomic strata and age groups. Results:
Analysis veriied that 22.5% and 16.6% of the individuals presented Staphylococcus aureus and MRSA, respectively, at any of the three sites. Vancomycin resistance was observed in 1.4% of the S. aureus isolates, which was conirmed by detection of the vanA gene. It was interesting to note that 58.8% of the children in the age group 1-5 years-old presented MRSA, the highest percentage compared to other age groups of < 1 (44.4%) year-old, 5-20 (21.7%) years-old, > 40 (11%) years-old and 20-40 (9.9%) years-old. Among the population of various socioeconomic strata, maximum MRSA colonization was observed among doctors (22.2%), followed by upper economic class (18.8%), lower economic class (17.7%), apparently healthy hospital in-patients (16.5%), nurses (16%) and middle economic class (12.5%). Most of the MRSA isolates were capsular polysaccharide antigen type 8 (57.1%). Conclusions: here is a need for continuous surveillance and monitoring of the presence of MRSA in the community and a clearer understanding of the dynamics of the spread of MRSA will assist in controlling its dissemination.
Keywords:Staphylococcus aureus. Methicillin resistance. Vancomycin resistance. Healthy population. Colonization.
RESUMO
Introdução: O Staphylococcus aureus é conhecido por ser um colonizador em humanos sendo implicado em infecções comunitárias dos tecidos moles. Contudo, a resistência à meticilina e emergência de S. aureus meticilina resistentes (MRSA) têm despertado preocupação em todo o mundo. O presente estudo visa encontrar a prevalência de MRSA na comunidade de Bangalore, sul da Índia. Métodos:Suabes foram coletados de narinas anteriores, antebraço e dorso da palma de 1.000 indivíduos saudáveis, residentes em Bangalore e nas proximidades, pertencentes a diferentes estratos socioeconômicos e faixas etárias. Resultados: Observou-se que 22,5% e 16,6% dos indivíduos foram abrigar Staphylococcus aureus e MRSA, respectivamente, em qualquer um dos três locais. Dos S. aureus isolados, 1,4% também foram resistentes à vancomicina, o que foi conirmado pela detecção do gene vanA. Foi interessante notar que 58,8% das crianças na faixa etária de 1-5 anos foram abrigar MRSA, o mais elevado em comparação com outros grupos etários de < 1 (44,4%) ano, 50-20 (21,7%) anos, > 40 (11%) anos e 20-40 (9,9%) anos. Entre a população de diferentes estratos socioeconômicos, a colonização de MRSA máxima foi observada entre os médicos (22,2%), seguida pela classe econômica superior (18,8%), classe baixa (17,7%), pacientes aparentemente saudáveis (16,5%), enfermeiros (16%) e classe econômica média (12,5%). A maioria dos MRSA isolados eram do tipo polissacarídeo capsular antígeno 8 (57,1%). Conclusões: Há uma necessidade de vigilância e monitorização contínua da presença de MRSA na comunidade, bem como uma melhor compreensão da dinâmica de propagação de MRSA pode ajudar no controle da disseminação.
Palavras-chaves: Staphylococcus aureus. Resistência à meticilina. Resistência à vancomicina. População saudável. Colonização.
Staphylococcus aureus is ubiquitous in nature and a known colonizer in humans. Community acquired sot tissue infections due to S. aureus is quite common1. Recently, community acquired S. aureus
has raised concerns due to increasing methicillin resistance. Methicillin resistant Staphylococcus aureus
(MRSA) infections do not respond to beta-lactam antibiotics and vancomycin is the drug of choice2-4.
MRSA has been implicated in both community acquired and hospital acquired infections and many of the clinical infections arise from the spread from healthy carriers. he anterior nares are the most common site for colonization, due to moist squamous epithelium and ventilation, and are also responsible for dissemination in the community. Even healthy individuals carrying MRSA present a small risk of contracting an invasive infection.
hus, it is imperative to determine the prevalence of MRSA as colonizers in the community, as well as presence of vancomycin resistance among them.
METHODS
In between april 2003 to december 2007, 1000 individuals (M:F=3:2) of various Socio-economic status based on the monthly per capita income (MPCI) in Rs. namely upper economic class (MPCI > Rs. 20000) (n=324), middle economic class (MPCI Rs. 5,000-20,000) (n=233), lower economic class (MPCI< Rs. 5,000) (n=181), doctors (n = 27), nurses (n = 144), apparently healthy hospital in-patients (n = 91), belonging to the age groups (< 1 year-old [n = 9], 1-5 years-old [n=24], 5-20 years-old [n = 434]; 20-40 old [n = 424] and > 40 years-old [n = 109]), who were not on any antibiotic therapy and residing in the City of Bangalore and the adjacent Kolar district were recruited. Following free informed consent, swabs were collected from the anterior nares for resident lora and from the forearm, dorsum and palm of the hands for transient flora from 1,000 individuals. Transport swabs (Himedia, India) were used for sample collection and transportation to the
Article/Artigo
310
RESULTS
Goud R et al - Community prevalence of MRSA in southern India
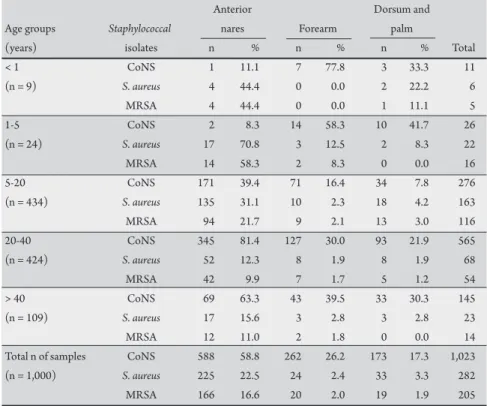
TABLE 1 - Distribution of Staphylococci colonization in healthy individuals according to age.
Anterior Dorsum and
Age groups Staphylococcal nares Forearm palm
(years) isolates n % n % n % Total
< 1 CoNS 1 11.1 7 77.8 3 33.3 11
(n = 9) S. aureus 4 44.4 0 0.0 2 22.2 6
MRSA 4 44.4 0 0.0 1 11.1 5
1-5 CoNS 2 8.3 14 58.3 10 41.7 26
(n = 24) S. aureus 17 70.8 3 12.5 2 8.3 22
MRSA 14 58.3 2 8.3 0 0.0 16
5-20 CoNS 171 39.4 71 16.4 34 7.8 276
(n = 434) S. aureus 135 31.1 10 2.3 18 4.2 163
MRSA 94 21.7 9 2.1 13 3.0 116
20-40 CoNS 345 81.4 127 30.0 93 21.9 565
(n = 424) S. aureus 52 12.3 8 1.9 8 1.9 68
MRSA 42 9.9 7 1.7 5 1.2 54
> 40 CoNS 69 63.3 43 39.5 33 30.3 145
(n = 109) S. aureus 17 15.6 3 2.8 3 2.8 23
MRSA 12 11.0 2 1.8 0 0.0 14
Total n of samples CoNS 588 58.8 262 26.2 173 17.3 1,023
(n = 1,000) S. aureus 225 22.5 24 2.4 33 3.3 282
MRSA 166 16.6 20 2.0 19 1.9 205
CoNS: coagulase negative Staphylococci, S. aureus: Staphylococcus aureus, MRSA: methicillin resistant Staphylococcus aureus.
laboratory. Culture and identiication was performed, according to standard procedures5. All the S. aureus isolates were screened for
methicillin and vancomycin resistance using the modiied Kirby Bauer disc difusion method, according to the NCCLS guidelines6.
All the vancomycin resistant strains were further confirmed by detecting the van A gene by polymerase chain reaction using the primers UNRG-Fp- 5’- CATGAATAGAATAAAAGTGCAATA-3’ and UNRG- Rp- 5’ CCCCTTTAACGCTAATACGATCAA described earlier by Tiwari et al7.
For all the strains of S. aureus that were isolated, including MRSAs, capsular antigen typing was performed against speciic antisera of type-5 and 8 capsular serotype strains, as previously described by Paul et al8.
Ethical considerations
he Ethical Review Board of Gulbarga University approved the study. Sampling was performed ater obtaining oral consent from the subjects.
From the three anatomical sites of the 1,000 individuals screened, 1,023 coagulase negative Staphylococci (CoNS) and 282 S. aureus were isolated, of which 205 were MRSA. Among the CoNS, 58.8% were isolated from the anterior nares (n = 588), 26.2% from the forearm (n = 262) and 17.3% were from the dorsum and palm of the hands (n = 173). For S. aureus, 22.5% were isolated from the anterior nares (n = 225), 2.4% from the forearm (n =24) and 3.3% from the dorsum and palm of the hands (n = 33). he distribution of MRSA was highest in the anterior nares (16.6%; n = 166), followed by the forearm (2%; n = 20) and the dorsum and palm of the hands (1.9%; n = 9). All the patients presenting S. aureus as transient lora on
their forearms and the dorsum and palm of the hands also presented
S. aureus in their anterior nares and thus the individual prevalence of
S. aureus determined was 22.5%. A similar value was determined for MRSA, with an individual MRSA prevalence of 16.6%.
he distribution of S. aureus and MRSA according to age is presented in Table 1. he greatest presence of MRSA was observed in the age group 1-5 (58.3%) years-old, followed by < 1 (44.4%) year-old, 5-20 (21.7%) years-year-old, > 40 (11%) years-old and 20-40 (9.9%) years-old. Although a high percentage of MRSA was determined for resident lora in the age groups < 1 year-old and 1-5 years-old, the percentage of MRSA as transient lora was very low.
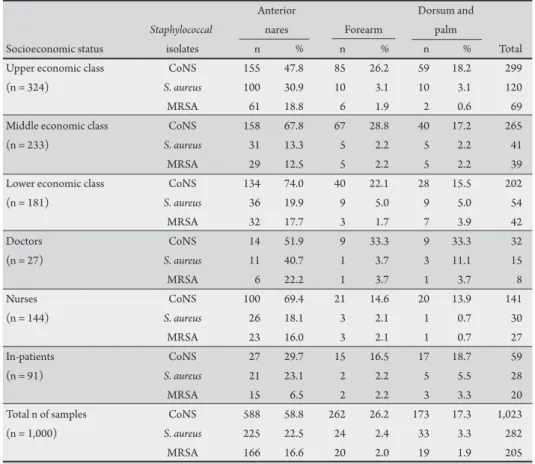
he prevalence of S. aureus and MRSA according to occupation and socioeconomic status is presented in the Table 2. Of some interest was the fact that 22.2% of the doctors presented MRSA as resident lora and 3.7% as transient lora, the highest values for any group. Doctors were followed by individuals from the higher economic class (18.8%), the lower economic class (17.7%), apparently healthy in-patients (16.5%) and nurses (16%), while the lowest values occurred in the middle economic class (12.5%).
Vancomycin resistance was observed in the 1.4% (n = 4) of the
S. aureus isolates. Vancomycin resistance was conirmed by PCR ampliication of the vanA gene. All the vancomycin resistant strains were resistant to methicillin, except one.
311
Rev Soc Bras Med Trop 44(3):309-312, mai-jun, 2011
DISCUSSION
TABLE 2 - Distribution of Staphylococci in healthy individuals according to socioeconomic strata.
Anterior Dorsum and
Staphylococcal nares Forearm palm
Socioeconomic status isolates n % n % n % Total
Upper economic class CoNS 155 47.8 85 26.2 59 18.2 299
(n = 324) S. aureus 100 30.9 10 3.1 10 3.1 120
MRSA 61 18.8 6 1.9 2 0.6 69
Middle economic class CoNS 158 67.8 67 28.8 40 17.2 265
(n = 233) S. aureus 31 13.3 5 2.2 5 2.2 41
MRSA 29 12.5 5 2.2 5 2.2 39
Lower economic class CoNS 134 74.0 40 22.1 28 15.5 202
(n = 181) S. aureus 36 19.9 9 5.0 9 5.0 54
MRSA 32 17.7 3 1.7 7 3.9 42
Doctors CoNS 14 51.9 9 33.3 9 33.3 32
(n = 27) S. aureus 11 40.7 1 3.7 3 11.1 15
MRSA 6 22.2 1 3.7 1 3.7 8
Nurses CoNS 100 69.4 21 14.6 20 13.9 141
(n = 144) S. aureus 26 18.1 3 2.1 1 0.7 30
MRSA 23 16.0 3 2.1 1 0.7 27
In-patients CoNS 27 29.7 15 16.5 17 18.7 59
(n = 91) S. aureus 21 23.1 2 2.2 5 5.5 28
MRSA 15 6.5 2 2.2 3 3.3 20
Total n of samples CoNS 588 58.8 262 26.2 173 17.3 1,023
(n = 1,000) S. aureus 225 22.5 24 2.4 33 3.3 282
MRSA 166 16.6 20 2.0 19 1.9 205
CoNS: coagulase negative Staphylococci, S. aureus: Staphylococcus aureus, MRSA: methicillin resistant Staphylococcus aureus.
TABLE 3 - Capsular polysaccharide antigen types in Staphylococcus aureus and MRSA isolates as colonizers from healthy individuals.
Capsular antigen types
Total n of T5 T8 Non T5/T8
Organisms isolates n % n % n %
Staphylococcus aureus 282 61 21.6 153 54.3 68 24.1
MRSA 205 43 21.0 117 57.1 45 21.9
T5: type 5, T8: type 8, MRSA: methicillin resistant Staphylococcus aureus.
Resistance to methicillin and the emergence of MRSA has aroused great concerns all over the world during the last few decades. In this work, a 22.5% carrier rate for S. aureus and 16.6% for MRSA was determined among the healthy population. hese results are consistent with the other studies from India, where 23% to 52.2% S. aureus colonization has been reported among healthy individuals9-12.
hough few studies from India observed no MRSA in the community, a prevalence of 16.6% was determined, which is similar to reports by Saxena et al9, from Delhi (18%) and Majumdar et al (24%) from
Sikkim9,11. However, a previous study by Onanuga et al from Nigeria
reported 69% of MRSA among healthy women in Zaria, Nigeria13.
In contrast, studies from the USA, Greece and Malaysia have shown less than 1% colonization of MRSA in healthy individuals14-16. hus
MRSA prevalence shows high regional variance. It was quite alarming to note a high incidence of MRSA (54.5%)colonization among children below 5 years of age.
Vancomycin resistance was observed in 1.4% of S. aureus isolates, which was conirmed by PCR ampliication of vanA. Worthy of note
was the fact that all the vancomycin resistant strains were resistant to methicillin, except one; ; i.e., one VRSA strain that was sensitive to methicillin was detected, similar to a case reported by Pillai et al4.
Vancomycin has been the standard of care for serious infections and many studies show 100% positive clinical outcome16,17. However,
this study determined a 1.8% incidence of vancomycin resistance in the population also presenting MRSA. hese indings support the recent increasing emergence of vancomycin-resistant S. aureus worldwide18.
his is also the irst report of VRSA in the area studied. Researchers had predicted that the spread of vancomycin resistance was advancing, but the observation of 1.4% resistance in this study conirms the establishment of the resistant strain in this region of southern India. Previous indings concerning high vancomycin-resistant MRSA were reported by Prakash et al in Tamil nadu, southern India2.
he increased incidence of MRSA and VRSA colonization in the healthy community can be attributed to the indiscriminate use of antibiotics. his is of utmost concern, since S. aureus is an opportunistic pathogen that has been implicated as a causative agent in acute food poisoning episodes, toxic shock syndrome, impetigo, scalded skin syndrome, cellulitis, folliculitis and furuncles.
Resistance in MRSA is related to a chromosomal mecA gene that speciies the production of an abnormal penicillin binding protein called PBP2a or PBP21. PBP2a shows decreased ainity for binding beta-lactam antibiotics resulting in resistance not only to methicillin, but to all beta-lactams, including penicillins and cephalosporins19. he mecA
312
he authors declare that there is no conlict of interest.
CONFLICT OF INTEREST
REFERENCES
he presence of type 8 capsular polysaccharide antigen occurred more frequently than type 5 in both the S. aureus and MRSA, in agreement with the indings of Paul et al8.
In conclusion, analysis of the results of this study conirms the need to reassess policies regarding antibiotic use for Staphylococcal infection. Injudicious use of antibiotics will lead to development of multiple drug resistance. Furthermore, regular surveillance of hospital associated infections, including monitoring antibiotic sensitivity patern of MRSA, and the formulation of a deinitive antibiotic policy may be helpful in reducing the incidence of MRSA infection.
1. Vandenesch F, Naimi T, Enright MC, Lina G, Nimmo GR, Hefernan H, et al. Community-acquired methicillin-resistant Staphylococcus aureus carrying Panton-Valentine leukocidin genes: worldwide emergence. Emerg Infect Dis 2003; 9:978-984.
2. Prakash M, Rajasekar K, Karmegam N. Prevalence of Methicillin Resistant Staphylococcus aureus in Clinical Samples Collected from Kanchipuram Town, Tamil Nadu, South India. J Appl Sci Res 2007; 3:1705-1709.
3. Olayinka BO, Olayinka AT, Onaolapo JA, Olurinola PF. Patern of resistance to vancomycin and other antimicrobial agents in staphylococcal isolates in a university teaching hospital. Afr Clin Exper Microbiol 2005; 6:46-52. 4. Pillai SK, Wennersten C, Venkataraman L, Eliopoulos GM, Moellering RC,
Karchmer AW. Development of reduced vancomycin susceptibility in methicillin susceptible Staphylococcus aureus. Clin Inf Dis 2009; 49:1169-1173.
5. Betty AF, Daniel FS, Alice SW. Staphylococcus, Micrococcus and Similar Organisms. In: Bety AF, Daniel FS, Alice SW, editors. Baily and Scot’s Diagnostic Microbiology. 11th ed. St. Louis: Mosby Inc; 2002. p. 284.
6. National Commitee for Clinical Laboratory Standards. Performance standards for antimicrobial disc susceptibility tests. Document M2- A6. 6th ed. Wayne,
Pennsylvania: National Committee for Clinical Laboratory Standards; 1997. p. 19087-19098.
7. Tiwari HK, Sen MR. Emergence of vancomycin resistant Staphylococcus aureus (VRSA) from a tertiary care hospital from northern part of India. BMC Infect Dis 2006; 6:156.
8. Paul SM, Belkum AV, Shivannavar CT, Gaddad SM. Carriage of capsulated strains of Staphylococcus aureus: a population-based study performed in Gulbarga, South India. Epidemiol Infect 2004; 132:831-838.
9. Saxena S, Singh K, Talwar V. Methicillin Resistant Staphylococcus aureus prevalence in community in the East Delhi area. Jpn J Infect Dis 2003; 56:54-56. 10. Santhosh DV, Shobha KL, Bairy I, Rao G, Anand KM, D’Souza J. Nasal screening and survey of pre-clinical medical students from Malaysia for nasal carriage of coagulase positive MRSA and rate of nasal colonization with Staphylococcus species. J Clin Diagn Res 2007; 6:494-499.
11. Majumdar D, Barua A, Paul B. Nasal carriage of methicillin resistant Staphylococci in healthy population of East Sikkim. Ind J Comm Med 2009; 34:364-365. 12. Parasa LS, Kumar LCA, Para S, Atluri VSR, Kumar PR, Shety CR. Reviews in
Infection 2010; 1:117-123.
13. Onanuga A, Oyi AR, Olayinka BO, Onaolapo JA. Prevalence and susceptibility patern of methicillin resistant Staphylococcus aureus isolates among healthy women in Zaria, Nigeria. Afr J Biotechnol 2005; 4:1321-1324.
14. Kuenhnert MJ, Kruszan-Morin D, Hill HA, McQuillan G, McAllister SK, Fosheim G, et al. Prevalence of Staphylococcus aureus nasal colonization in the United States, 2001-2002. J Infect Dis 2006; 193:172-179.
15. Karapsias S, Piperaki ET, Spiliopoulou I, Katsanis G, Tseleni-Kotsovili A. Methicillin resistant Staphylococcus aureus nasal carriage among healthy employees of the Hellenic air force. Eurosurveillance 2008; 13:1-3.
16. Choi CS, Yin CS, Baker AA, Sakewi Z, Naing NN, Jamal F, et al. Nasal carriage of Staphylococcus aureus among healthy adults. J Microbiol Immunol Infect 2006; 39:458-464.
17. Anupurba S, Sen MR et al. Prevalence of methicillin resistant Staphylococcus aureus in a tertiary referral hospital in eastern Utar Pradesh. Ind J Med Microbiol 2003; 21:49-51.
18. Rajaduraipandi K, Mani KR, Panneerselvam K, Mani M, Bhaskar M, Manikandan P. Prevalence and antimicrobial susceptibility pattern of methicillin resistant Staphylococcus aureus: a multicentre study. Ind J Med Microbiol. 2006; 24:34-38. 19. Fridkin SK. Vancomycin-intermediate and resistant Staphylococcus aureus: what the infectious disease specialist need to know. Clin Infect Dis 2001; 32: 108-115. 20. Weems JJ. he many faces of Staphylococcus aureus infections. Postgrad Med