HOME BLOOD GLUCOSE MONI TORI NG I N TYPE 1 DI ABETES MELLI TUS
1Sonia Aur or a Alv es Gr ossi2 Sim ão August o Lot t enber g3 Ana Mar ia Lot t enber g3 Thaís Della Manna3 Hilt on Kuper m an3
Gr ossi SAA, Lot t enber g SA, Lot t enber g AM, Manna TD, Kuper m an H. Hom e blood glucose m onit or ing in t ype 1 Diabet es Mellit us. Rev Lat ino- am Enfer m agem 2 0 0 9 m ar ço- abr il; 1 7 ( 2 ) : 1 9 4 - 2 0 0 .
Obj ect iv e: To det er m ine w hich of t w o sim plified blood glucose m onit or ing schem es pr om ot es bet t er m et abolic cont r ol in t ype1 diabet ic pat ient s dur ing 12 m ont hs of par t icipat ion in educat ional gr oups. Met hods: A cr ossover clinical t r ial involving 21 pat ient s divided int o t w o gr oups w as conduct ed. They w er e subm it t ed t o a t w o m onit or ing schem es: 2 alt er nat e daily pr epr andial m easur em ent s and 2 alt er nat e daily pr e- and post pr andial m easur em ent s. The effect iveness of t he schem es w as evaluat ed based on HbA1c. Var iat ions in m ean HbA1c w er e analyzed by Fr ied m an t est . Resu lt s: Th e g r ou p s w er e h om og en ou s in t er m s of sociod em og r ap h ic an d clin ical v ar iab les ( p> 0.05) . Mean HbA1c lev els r anged fr om 8.48 ( ± 1.00) t o 7.37 ( ± 0.99) ov er t im e in Gr oup A and fr om 9.89 ( ± 0.86) t o 8.34 ( ± 1.06) in Gr oup B. The analysis of t he HbA1c show ed a significant r educt ion in t he fir st and last 6 m ont hs and over t he 12 m ont hs of t he st udy in t w o gr oups ( p< 0.05) . The pr epr andial schem e dem onst r at ed t h e lar gest n u m ber an d h igh est per cen t age of sign if ican t dr ops in HbA1 c. Con clu sion s: Th e t w o m on it or in g im pr ov ed t he m et abolic cont r ol and t he pr epr andial schem e w as m or e effect iv e.
DESCRI PTORS: diabet es m ellit us, t y pe 1; blood glucose self- m onit or ing; nur sing
MONI TORI ZACI ÓN, EN EL DOMI CI LI O, DE LA GLUCEMI A EN PACI ENTES CON
DI ABETES MELLI TUS TI PO 1
Obj et ivo: I dent ificar cual de los dos esquem as de m onit or ización pr opuest os posibilit a r ealizar un m ej or cont r ol m et ab ólico, en d iab ét icos d el t ip o1 , d u r an t e los 1 2 m eses d e p ar t icip ación en gr u p os ed u cat iv os. Mét od o: Ensay o clínico cr uzado con 2 1 pacient es div ididos en dos gr upos y som et idos a dos difer ent es esquem as de m on it or ización . La ef ect iv id ad d e los esq u em as f u e ev alu ad a p or m ed io d e la Hb A1 c. La v ar iación d e los pr om edios de HbA1c fue analizada con la pr ueba de Fr iedm an. Result ados: Dur ant e t odo el est udio la var iación de los pr om edios de HbA1c, par a el gr upo A, fue de 8,48( ± 1,00) la 7,37( ± 0,99) y de 9,89( ± 0,86) la 8,34( ± 1,06) par a el gr u po B. Los an álisis de la v ar iación de la HbA1 c colocar on en ev iden cia u n a r edu cción sign ificat iv a ( p< 0,05) en los dos gr upos, en los 3 per iodos evaluados: pr im er os y últ im os 6 m eses y dur ant e los 12 m eses d e est u d io. Con clu sion es: Los d os esq u em as m ej or ar on el con t r ol m et ab ólico y el esq u em a an t es d e las com idas fu e m ás efect iv o.
DESCRI PTORES: diabet es m ellit us t ipo 1; aut om onit or ización de la glucosa sanguínea; enfer m er ía
MONI TORI ZAÇÃO DOMI CI LI AR DA GLI CEMI A EM PACI ENTES COM DI ABETES
MELLI TUS DO TI PO 1
Obj et ivo: I dent ificar qual de dois esquem as sim plificados de m onit or ização da glicem ia viabiliza m elhor cont r ole m et ab ólico, em p acien t es com d iab et es m ellit u s t ip o 1 , ao lon g o d e 1 2 m eses d e p ar t icip ação em g r u p os educat ivos. Mét odo: Ensaio clínico cr uzado, com 21 pacient es divididos em dois gr upos. Eles for am subm et idos a dois esquem as de m onit or ização: duas m edidas diár ias pr é- pr andiais alt er nadas e duas m edidas diár ias pr é e pós- pr an diais alt er n adas. A ef et iv idade dos esqu em as f oi av aliada pelos n ív eis de HbA1 c. Par a est u dar a v ar iação das m édias das HbA1c aplicou- se o t est e não par am ét r ico de Fr iedm an. Result ados: Os gr upos er am h om ogên eos ao in ício do est u do com r elação às v ar iáv eis sócio- dem ogr áficas e clin icas( p> 0 , 0 5 ) . A v ar iação das m édias de HbA1c, ao longo do t em po par a o gr upo A foi de 8,48( ± 1,00) a 7,37( ± 0,99) e par a o gr upo B de 9 , 8 9 ( ± 0 , 8 6 ) a 8 , 3 4 ( ± 1 , 0 6 ) . O r esu lt ado da an álise da v ar iação da HbA1 c m ost r ou r edu ção sign ificat iv a n os dois gr upos, nos pr im eir os e últ im os 6 m eses e ao longo dos 12 m eses nos dois gr upos ( p< 0,05) . O Esquem a d e m o n i t o r i z a ç õ e s p r é - p r a n d i a i s p o s s i b i l i t o u o m a i o r n ú m e r o e o s m a i o r e s p e r c e n t u a i s d e q u e d a s est at ist icam ent e significat iv as nos nív eis de hem oglobina glicada. Conclusões: Os dois esquem as m elhor ar am o cont r ole m et abólico e esquem a pr é- pr andial foi m ais efet iv o.
DESCRI TORES: diabet es m ellit us t ipo 1 ; aut om onit or izacão da glicem ia; enfer m agem
1
Suppor t ed by Fundação de Am par o à Pesquisa do Est ado de São Paulo, FAPESP; 2PhD, Facult y, Escola de Enfer m agem da Univer sidade de São Paulo, Brazil, e- m ail: sogr [email protected] ; 3PhD, Faculdade de Medicina da Univer sidade de São Paulo, Brazil, e- m ail: lot t enb@at t global.net ; t haisdm @icr.hcnet .usp.br, hkuper m an@t er ra.com .br.
I NTRODUCTI ON
O
ne of t he m ost significant st udies t o t est t he proposal t hat com plicat ions of Type 1 Diabet es Mellit us( DM1) are relat ed t o a chronic increase in blood glucose
w a s t h e D i a b et es Co n t r o l a n d Co m p l i ca t i o n s Tr i a l
( DCCT)( 1 ). Th e DCCT sh ow ed t h at in t en siv e in su lin t her apy t o m aint ain glucose lev els close t o nor m al is
cert ainly effect ive in m inim izing t he developm ent and
progression of com plicat ions of DM( 1).
Many quest ions have been raised regarding t he
d i f f i cu l t i e s i n i m p l e m e n t i n g t h e r i g i d co n t r o l s
r ecom m ended by t he DCCT and also r egar ding t heir
im plicat ions in clinical pract ice, educat ional program s,
self - m on it or in g, qu alit y of lif e an d t r eat m en t cost s,
especially at ser v ices w her e no r esour ces or t r ained
pr ofessionals ar e av ailable. Alt er nat iv e st r at egies for
t h e con t r ol of DM t h at t ak e in t o accou n t in d iv id u al
lim it at ions and deficit s in t he healt h syst em relat ed t o
hum an and financial resources are necessary and are
t he m ain obj ect ive of t he present st udy. The obj ect ive
of t he present st udy was t o evaluat e t he effect iveness
of t wo different hom e blood glucose m onit oring schem es
in im p r ov in g g lu cose con t r ol in p at ien t s w it h DM1
undergoing a m ont hly t herapeut ic adj ust m ent regim en
over a period of 12 m ont hs of part icipat ion in educat ional
gr ou ps.
PATI ENTS AND METHODS
This r andom ized cr ossover st udy w as car r ied
out at t he out pat ient clinic of t he “ League of Diabet es”,
D i sci p l i n e o f En d o cr i n o l o g y, HC- FMUSP. Th e st u d y
populat ion consist ed of subj ect s w it h DM1 enr olled in
t he ser v ice w ho com plied w it h t he follow ing inclusion
crit eria: age older t han 2 years, m ot ivat ion t o m onit or
blood glucose t wice a day for a period of 12 m ont hs,
an d t h e b asic socioecon om ic- cu lt u r al an d cog n it iv e
condit ions necessary t o at t end t he educat ional groups
and t o part icipat e in t he act ivit ies developed. Excluded
w er e pat ient s w it h less t han 2 y ear s of t he disease,
p a t i e n t s sp o r a d i ca l l y o r co n t i n u o u sl y u si n g
hyperglycem ic drugs, pat ient s wit h ot her DM- associat ed
endocr inopat hies, and subj ect s w ho did not agr ee t o
par t icipat e in t he st udy. The sam ple consist ed of 21
pat ient s w ho alr eady m onit or ed blood glucose lev els
once a day and who fulfilled t he crit eria described above.
The pat ient s were t hen random ly divided int o
t w o groups by draw ing lot s. Group A used Schem e 1
for m onit oring blood glucose during t he first 6 m ont hs
of t he st udy and Schem e 2 dur ing t he subsequent 6
m on t h s. Gr ou p B u sed Sch em e 2 du r in g t h e f ir st 6
m ont hs of t he st udy and Schem e 1 during t he subsequent
6 m ont hs. I n Schem e 1, t he pat ient s self- m onit or ed
capillary blood glucose levels t wice a day at preprandial
t im es ( 30 m in before m eals) , at bedt im e and at 3 am
every 2 weeks over a period of 6 m ont hs. I n Schem e
2, t he pat ient s self- m onit or ed capillar y blood glucose
levels t wice a day at preprandial ( 30 m in before m eals)
and post prandial t im es ( 90 t o 120 m in aft er m eals) and
at 3 am every 2 weeks over a period of 6 m ont hs. The
effect iveness of t he m onit oring schem es in prom ot ing
m et abolic cont rol w as evaluat ed by t he m easurem ent
of glycat ed hem oglobin ( HbA1c) concent rat ion and t he
r esult s obt ained dur ing 12 m ont hs w er e com par ed t o
baseline values ( Novem ber 2003) . The pat ient s and t heir
car egiv er s par t icipat ed in m ont hly educat ional gr oup
m eet ings wit h t he m ult i- professional t eam . The m eet ings
of gr oups A and B w er e held on differ ent day s. The
i n su l i n r e g i m e n s u se d co n si st e d o f 2 t o 4 d a i l y
applicat ion s ( bef or e br eak f ast , bef or e lu n ch , bef or e
dinner, and at bedt im e) of int er m ediat e- act ing ( NPH)
and ult rarapid- act ing insulin ( Lispro) . Lispro insulin was
a p p l i e d 1 5 m i n b e f o r e m e a l s. I n o r d e r t o cr e a t e
ob j ect iv e cr it er ia f or t h e t h er ap eu t ic ad j u st m en t of
insulin, one week of int ensive m onit oring consist ing of
8 daily pr e- and post pr andial m easur em ent s ( r un in)
was perform ed at t he beginning of t he st udy t o det erm ine
fact or s in dicat in g in su lin sen sit iv it y an d t o calcu lat e
correct ion fact ors t o be applied during t he st udy when
t he num ber of glucose t est s w as r educed t o t w ice a
day. The sam e schem e w as r epeat ed at t he t im e of
inversion of t he groups as wash- out . The proj ect was
a p p r o v e d b y t h e Et h i cs Co m m i t t e e o f HC- FMUSP
( pr ocess No.521/ 01) .
Th e dat a of t h is st u dy w er e collect ed u sin g
seven differ ent inst r um ent s cont aining dat a r egar ding
ident ificat ion, socio- dem ographic and clinical variables,
insulin t r eat m ent r egim en and adj ust m ent s, capillar y
blood glucose lev els, daily pr oblem s, glucose pr ofile,
ant hr opom et r ic m easur em ent s, and diet ar y r ecor d.
Blood was collect ed from pat ient s of groups A
and B for t he m easur em ent of HbA1c ( HPLC, nor m al
range: 4.1 t o 6.5% ) before ( baseline values) and 2, 4,
6, 8, 10 and 12 m ont hs aft er t he beginning of t he st udy.
As a cont r ol par am et er, all pat ient s had t heir HbA1c
levels com pared t o baseline values. The pat ient s were
inst ruct ed regarding t he correct t echnique for capillary
blood glucose t est ing. Finger punct ures were perform ed
wit h Soft Touch Lancet s and Advant age Syst em st rips
w er e used for glucose t est ing ( bot h fr om Boehr inger
Man n h eim Cor p or at ion ) . Th e q u alit y of t h e g lu cose
m e a su r e m e n t s w a s d e t e r m i n e d a cco r d i n g t o t h e
r e co m m e n d a t i o n s o f t h e Am e r i ca n D i a b e t e s
The dat a were analyzed under t he supervision
of a st at ist ician, using SPSS for Windows, version 10.0.
Result s pr esent ing a p value < 0.05 w er e consider ed
significant . The following t est s were applied t o det erm ine
t he hom ogeneit y of t he groups at t he beginning of t he
st udy : nonpar am et r ic Mann- Whit ney t est for HbA1 c,
fam ily incom e, household m em bers, St udent t - t est for
age and BMI , and Fisher ’s t est for gender, educat ional
level and housing condit ions. Along t he st udy, all ot her
analy ses consist ed of t he int er pr et at ion of int r agr oup
dat a. The nonparam et ric Friedm an t est was applied t o
st udy t he variat ion in HbA1c and m ean glucose levels
bet w een t h e differ en t per iods an d ov er t im e. Th ese
an aly ses w er e per f or m ed separ at ely f or each gr ou p
during t he course of t he t wo schem es. When a significant
d i f f e r e n ce i n Hb A1 c co n ce n t r a t i o n w a s d e t e ct e d ,
Bon f er r on i m u lt iple com par ison s w er e per f or m ed t o
id en t if y b et w een w h ich t w o m on t h s t h e d if f er en ce
occur r ed. The Wilcox on t est w as used for int r agr oup
com parisons of t wo schem es.
RESULTS
The charact erist ics of groups A and B are shown
in Table 1.
Table 1 - Charact erist ics of groups A and B
s c i t s i r e t c a r a h C ) 1 2 = n
( GroupA GroupB p-value
s c i t s i r e t c a r a h C ) 1 2 = n
( GroupA GroupB p-value
s r a e y n i e g
A FamliyincomeinR$ ) D S ( n a e
M 11.82(3.19) 9.40(2.8) 0.082* Mean(SD) 1200.00(512.08)1075.00(973.21) r
e d n e
G Median 1100.00 500.00 e
l a
M 4(36.4%) 3(30.0%) Range 500-2000 350-2900 0.221*** e
l a m e
F 7(63.6%) 7(70.0%) 0.999** No.ofhouseholdmembers l e v e l l a n o it a c u d
E Mean(SD) 3.80(0.63) 4.14(1.57) l o o h c s y r a m i r p e t e l p m o c n
I 5(50.0%) 7(100.0%) Median 4.00 4.00 l o o h c s y r a m i r p e t e l p m o
C 1(10.0%) Range 3-5 2-6 0.719*** l o o h c s e l d d i m e t e l p m o c n
I 2(20.0%) BaseilneHbA1c l o o h c s e l d d i m e t e l p m o
C 2(20.0%) 0.233** Mean(SD) 8.51(1.26) 8.92(1.83) 0.548*** g n il l e w d e h t n i s m o o r f o . o
N Chroniccompilcaitons n
a e
M 4.10 4.00 Yes n
a i d e
M 4.00 5.00 No 11(100.00%) 10(100.00) e
g n a
R 1.10 1.63 0.920** BMI ) D S ( n a e
M 19.79(3.92) 17.58(1.80) e
g n a
R 15.3-26.7 15.5-21.4 0.129*
SD: st andar d deviat ion; BMI : body m ass index; * St udent t - t est ; * * Fisher ’s exact t est ; * * * Mann- Whit ney t est .
Th e M a n n - W h i t n e y t e s t c o n f i r m e d t h e
hom ogeneit y of t he sam ple in t er m s of HbA1c lev els
at baselin e ( p= 0 . 5 4 8 ) . Th ese v alu es w er e u sed as a
cont r ol par am et er for t he subsequent analy ses. Wit h
r e sp e ct t o t h e g l y ce m i c p r o f i l e s, m e a n p r e - a n d
p ost p r an d ial g ly cem ic lev els an d g ly cem ic v ar iat ion
w er e higher t han desir ed in t he t w o gr oups over t im e
and no significant differ ence w as obser v ed ov er t im e
in eit h er g r ou p or b et w een p er iod s ( n on p ar am et r ic
Fr iedm an t est , p> 0. 05) .
# baseline; * schem e 1; * * schem e2; Fr iedm an t est : p< 0.001
Table 2 . Var iat ion in HbA1 c con cen t r at ion ov er t im e
in gr oup A
Th e low est m ean w as ob t ain ed d u r in g t h e
last m easur em ent in Schem e 1 and t he poor est m ean
w as obser v ed w hen t he pat ient s changed t o Schem e
2 . T h e n o n p a r a m e t r i c Fr i e d m a n t e s t s h o w e d a
sign if ican t decr ease of m ean HbA1 c lev els in gr ou p
A ov er t im e.
Table 3 . Var iat ion in HbA1 c con cen t rat ion ov er t im e
in gr oup B
n a e
M SD 25th
e l i t n e c r e
P Median
h t 5 7 e l i t n e c r e
P Count
3 0 v o N / c 1 A b
H 8.93# 1.94 7.10 8.90 10.55 9 4 0 n a J / c 1 A b
H 9.89* .86 9.35 10.00 10.55 9 4 0 h c r a M / c 1 A b
H 9.06* 1.14 8.60 9.10 10.05 9 4 0 y a M / c 1 A b
H 8.81* 1.20 7.80 9.00 9.65 9 4 0 y l u J / c 1 A b
H 9.11** 1.35 8.50 8.90 10.05 9 4 0 t p e S / c 1 A b
H 8.34** 1.06 7.90 8.50 8.80 9 4 0 v o N / c 1 A b
H 8.51** 1.16 7.90 8.60 9.25 9
# baseline; * schem e 2; * * schem e1; Fr iedm an t est : p= 0.002
A sig n if ican t d eclin e in m ean Hb A1 c lev els
ov er t im e w as also obser v ed in gr oup B.
n a e
M SD 25th
e l i t n e c r e
P Median
h t 5 7 e l i t n e c r e
P Count
3 0 v o N / c 1 A b
H 8.20# 1.04 7.15 8.30 9.05 9 4 0 n a J / c 1 A b
H 8.39* .58 7.80 8.60 8.90 9 4 0 h c r a M / c 1 A b
H 7.50* .73 7.05 7.40 8.20 9 4 0 y a M / c 1 A b
H 7.37* .99 6.80 7.30 8.20 9 4 0 y l u J / c 1 A b
H 8.48** 1.00 7.65 8.20 9.35 9 4 0 t p e S / c 1 A b
H 7.47** 1.31 6.35 7.40 8.55 9 4 0 v o N / c 1 A b
A n a l y s i s o f t h e v a r i a t i o n i n H b A 1 c
concent r at ion over t im e by t he Fr iedm an t est show ed
a sig n if ican t d if f er en ce in t h e f ir st ( p = 0 . 0 0 0 4 ) an d
last 6 m on t h s ( p= 0 . 0 0 2 ) an d alon g t h e 1 2 m on t h s
( p< 0.001) of t he st udy in gr oup A, and a significant
dif f er en ce in t h e f ir st ( p= 0 . 0 2 8 ) an d last 6 m on t h s
( p= 0.006) and along t he 12 m ont hs ( p= 0.002) of t he
st udy in gr oup B, ir r espect ive of t he cur r ent schem e.
Ta b l e s 4 a n d 5 s h o w b a s a l , i n t r a - a n d
i n t e r s c h e m e c o m p a r i s o n s o f m e a n H b A 1 c
concent r at ion bet w een t he differ ent m ont hs ov er t he
12 m ont hs of t he st udy. Com par isons of basal/ Schem e
1 a n d i n t r a s c h e m e 1 s h o w e d t h a t t h i s s c h e m e
p r o m o t ed t h r ee n o n si g n i f i can t i n cr eases o f Hb A1 c
lev els in gr ou ps A an d B an d n in e declin es, f ou r of
t h em b ei n g si g n i f i ca n t . Th e sa m e co m p a r i so n f o r
Schem e 2 also show ed t hr ee nonsignificant incr eases
and nine declines, one of t hem significant . I nt erschem e
co m p a r i so n s r ev ea l ed si x i n cr ea ses, t w o o f t h em
significant and t hree declines, one of t hem significant
w h en ch an gin g f r om Sch em e 1 t o Sch em e 2 ( Table
4) . When changing fr om Schem e 2 t o Schem e 1, t he
co m p ar i so n s sh o w ed sev en d ecl i n es, t w o o f t h em
sig n if ican t , an d t w o n on sig n if ican t in cr eases ( Tab le
5) . Schem es 1 and 2 w er e com par ed w it hin each gr oup
b y t h e n o n p a r a m e t r i c W i l c o x o n t e s t f o r p a i r e d
sam ples. The r esult s show ed no significant differ ence
in m ean HbA1 c lev els bet w een sch em es in gr ou p A
( p= 0.79) , w her eas in gr oup B Schem e 1 significant ly
im pr ov ed gly cem ic lev els ( p= 0 . 0 2 1 ) .
Table 4. Multiple com parisons of m ean HbA1c in group A
* St at ist ically significant ; * * Change fr om Schem e 1 t o Schem e 2
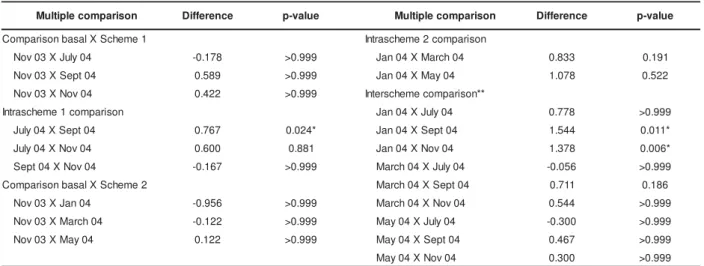
Table 5. Multiple com parisons of m ean HbA1c in group B
* St at ist ically significant ; * * Change fr om Schem e 2 t o Schem e 1
n o s i r a p m o c e l p i t l u
M Difference p-value Multiplecomparison Difference p-value
1 e m e h c S X l a s a b n o s i r a p m o
C Intrascheme2comparison 4 0 n a J X 3 0 v o
N -0.189 >0.999 July04XSept04 1.011 0.097 4 0 h c r a M X 3 0 v o
N 0.700 0.080 July04XNov04 0.922 0.001* 4 0 y a M X 3 0 v o
N 0.833 0.049* Sept04XNov04 -0.089 >0.999 n o s i r a p m o c 1 e m e h c s a r t n
I Interschemecomparison** 4 0 h c r a M X 4 0 n a
J 0.889 0.008* Jan04XJuly04 -0.089 >0.999 4 0 y a M X 4 0 n a
J 1.022 0.017* Jan04XSept04 0.922 0.238 4 0 y a M X 4 0 h c r a
M 0.133 >0.999 Jan04XNov04 0.833 0.049* 2 e m e h c S X l a s a b n o s i r a p m o
C March04XJuly04 -0.978 0.041* 4 0 y l u J X 3 0 v o
N 0.278 >0.999 March04XSept04 0.033 >0.999 4 0 t p e S X 3 0 v o
N 0.733 0.937 March04XNov04 -0.056 >0.999 4 0 v o N X 3 0 v o
N 0.644 0.219 May04XJuly04 -1.111 0.008* 4 0 t p e S X 4 0 y a
M -0.100 >0.999 4 0 v o N X 4 0 y a
M -0.189 >0.999
n o s i r a p m o c e l p i t l u
M Difference p-value Multiplecomparison Difference p-value
1 e m e h c S X l a s a b n o s i r a p m o
C Intrascheme2comparison 4 0 y l u J X 3 0 v o
N -0.178 >0.999 Jan04XMarch04 0.833 0.191 4 0 t p e S X 3 0 v o
N 0.589 >0.999 Jan04XMay04 1.078 0.522 4 0 v o N X 3 0 v o
N 0.422 >0.999 Interschemecomparison** n o s i r a p m o c 1 e m e h c s a r t n
I Jan04XJuly04 0.778 >0.999 4 0 t p e S X 4 0 y l u
J 0.767 0.024* Jan04XSept04 1.544 0.011* 4 0 v o N X 4 0 y l u
J 0.600 0.881 Jan04XNov04 1.378 0.006* 4 0 v o N X 4 0 t p e
S -0.167 >0.999 March04XJuly04 -0.056 >0.999 2 e m e h c S X l a s a b n o s i r a p m o
C March04XSept04 0.711 0.186 4 0 n a J X 3 0 v o
N -0.956 >0.999 March04XNov04 0.544 >0.999 4 0 h c r a M X 3 0 v o
N -0.122 >0.999 May04XJuly04 -0.300 >0.999 4 0 y a M X 3 0 v o
N 0.122 >0.999 May04XSept04 0.467 >0.999 4 0 v o N X 4 0 y a
DI SCUSSI ON
Alt hough analysis of glycem ic profiles did not
r ev ea l si g n i f i ca n t i m p r o v em en t , m et a b o l i c co n t r o l
im p r ov ed in t h e t w o g r ou p s st u d ied ir r esp ect iv e of
t he schem e used. Alt hough m ean glycat ed hem oglobin
concent r at ion r em ained abov e t he upper lim it of t he
m et hod, w hich is 6.5% , disagr eeing w it h t he pat t er ns
recom m ended in t he lit erat ure, w hich classifies values
of up t o 10% above t he upper lim it of t he m et hod as
sat isfact or y( 1), analy sis of HbA1 c v ar iat ion show ed a significant reduct ion in t he first and last 6 m ont hs and
along t he 12 m ont hs of t he st udy in t he t w o gr oups. I t
is possible t hat t he t her apeut ic adj ust m ent s t he t eam
p e r f o r m e d m o n t h l y b a se d o n i n d i v i d u a l g l y ce m i c
p r o f i l e s i m p r o v e d g l y c e m i c l e v e l s a t t i m e s n o t
c o n t e m p l a t e d i n t h e s c h e m e s p r o p o s e d , a n
im pr ov em ent r eflect ed in HbA1c lev els. The fact t hat
t his im pr ovem ent occur r ed ir r espect ive of t he schem e
u sed su g g est s t h at t h e t w o m o n i t o r i n g st r at eg i es
cont r ibut ed t o t his im pr ov em ent . As dem onst r at ed in
o t h er st u d i es, t h ese r esu l t s co n f i r m t h at , w h en a
m o n i t o r i n g p r o g r a m i s e n c o u r a g e d( 3 - 5 ) o r w h e n glycem ic values are used t o under st and t he int er act ion
b et w een in su lin t h er ap y, d iet , p hy sical act iv it y an d
com plicat ions and t o guide t r eat m ent , blood glucose
m onit or ing effect ively im pr oves m et abolic cont r ol and
t r eat m en t com p lian ce in cr eases b ot h am on g y ou n g
pat ient s and am ong t hose above t he age of 60( 5- 7). I t has been w ell docum ent ed in t he lit er at ur e
t hat , t he lar ger t he num ber of glucose t est s per for m ed,
t h e gr eat er t h e oppor t u n it ies f or in su lin adj u st m en t
and t he bet t er t he gly cem ic cont r ol( 3 , 7 - 9 ). I n a st udy ev alu at in g t h e ef f ect of an in su lin t h er apy r egim en
o n m e t a b o l i c c o n t r o l i n 2 2 9 c h i l d r e n , i t w a s
d em on st r at ed t h at an in cr ease in t h e f r eq u en cy of
blood glucose m onit or ing ( 1 t o 6 t im es per day) w as
cor r elat ed w it h low er HbA1c ( r = - 0.15, p= 0.006) , w it h
each addit ional daily m onit or ing r esult ing in a 0 . 4 %
decr ease in HbA1c concent r at ion, and t hat t he num ber
of insulin t y pes and applicat ions w as cor r elat ed w it h
incr eased HbA1c ( r = 0.2, p= 0.02) , w it h each addit ional
insulin dose r esult ing in a 0 . 4 6 % incr ease in HbA1 c
c o n c e n t r a t i o n( 1 0 ). O t h e r s t u d i e s h a v e a l s o dem onst r at ed a cor r elat ion bet w een low er HbA1c and
t h e f r e q u e n c y o f d a i l y t e s t s f o r b l o o d g l u c o s e
m on it or in g( 8 - 1 2 ). Som e st u d ies f ou n d n o associat ion bet w een t h e f r equ en cy of blood glu cose m on it or in g
and bet t er m et abolic cont r ol( 4,13).I n a populat ion st udy, d a t a o n t h e f r e q u e n cy o f d a i l y m o n i t o r i n g w e r e
obt ained by quest ionnair es and t he aim of t hat st udy
w as not t o use blood glucose t est ing as a t her apeut ic
st r at egy but only t o inv est igat e it s r elat ionship w it h
HbA1c concent r at ion( 13). Anot her st udy w as conduct ed o n 6 0 p a t i e n t s w i t h D M1 w h o p a r t i ci p a t e d i n a n
encour aged long- t er m self- m onit or ing pr ogr am . High
com p lian ce w it h t h e p r og r am w as ob ser v ed d u r in g
t h e f ir st 6 m on t h s, w it h a f r eq u en cy of ab ou t f ou r
d a i l y m o n i t o r i n g s, b u t o n l y 5 0 % o f t h e su b j e ct s
co n t i n u ed i n t h e p r o g r am f o r m o r e t h an 3 y ear s.
Dur ing a cr it ical per iod of t he st udy, com pr ising t he
8 t h t o 1 1 t h sem est er, a h ig h er f r eq u en cy of d aily
m onit oring w as correlat ed w it h glycem ic levels higher
t han 180 m g/ dl and poor HbA1c values( 4).The aut hors con clu d ed t h at t h e w or sen in g of m et ab olic con t r ol
dem on st r at ed by t h e in cr eased HbA1 c an d capillar y
glucose t ends t o incr ease t he fr equency of m onit or ing.
We agr ee w it h t his conclusion.
When no int ensive or ideal glucose m onit oring
is possible, which is t he case for m ost healt h services
in developing count ries, alt ernat ive and less expensive
st r at egies for blood glucose m onit or ing such as t hat
proposed here can be adopt ed. Alt hough not ideal, t he
pr esent pr oposal per m it t ed t o im pr ov e t he condit ion
o f t h e p a r t i ci p a n t s, w i t h t w o d a i l y g l u co se t e st s.
I m p r o v em en t o f m et a b o l i c co n t r o l w i t h t w o d a i l y
m onit orings on average has also been docum ent ed in
a long- t er m follow - up st udy aft er t he 12t h sem est er
and aft er a period of det eriorat ion of glycem ic cont rol,
w hen t he par t icipant s r eadj ust ed t o t he r equir em ent s
of t he program( 4).We found no st udies in t he lit erat ure report ing glycem ic profiles obt ained wit h t he applicat ion
of sim plified m onit oring st rat egies in pat ient s wit h DM1.
Many of t he invest igat ions m ent ion such st rat egies but
t he st udy is focused on ot her variables. An int erest ing
st udy ev aluat ing gly cem ic pr ofiles w as conduct ed on
150 pat ient s w it h st able t y pe 2 diabet es in or der t o
det er m ine t he effect iv eness of once- and t w ice- daily
sel f - m o n i t o r ed b l o o d g l u co se t est i n g st r at eg i es i n
det ect ing hy per gly cem ia and hy pogly cem ia. The pr
e-br eak fast and pr e- lunch m easur em ent s det ect ed t he
lar gest pr opor t ion ( 63.6% ) of hypoglycem ic r eadings,
pr e- dinner and bedt im e m easur em ent s det ect ed t he
largest proport ion ( 66.2% ) of hyperglycem ic readings,
and pre- lunch and pre- dinner m easurem ent s det ect ed
t he largest proport ion ( 57.7% ) of all hypoglycem ic and
h y p er g ly cem ic r ead in g s( 1 4 ). Th ese d at a su p p or t ou r i n t e n t i o n t o co n t i n u e i n v e st i g a t i n g a n d a d o p t i n g
s i m p l i f i e d m o n i t o r i n g s t r a t e g i e s i n l o w - i n c o m e
D e t e r i o r a t i o n o f m e t a b o l i c c o n t r o l w a s
obser ved in t he t w o gr oups w hen changing fr om one
sch em e t o t h e ot h er ( Ju ly ) , a f in d in g in d icat in g an
adapt iv e ph ase du r in g t h e n ew sch em e. We believ e
t hat blood glucose m onit or ing consist ing of t w o daily
t est s w a s n o t t h e o n l y f a ct o r r esp o n si b l e f o r t h e
im pr ov ed m et abolic cont r ol of t he par t icipant s in t his
st udy. Mont hly par t icipat ion in t he educat ional gr oup,
in div idu al n u t r it ion al car e an d t h e bon d est ablish ed
w it h t he t eam surely cont ribut ed t o t his finding, since
sig n if ican t r ed u ct ion s in g ly cat ed h em og lob in w er e
alr ead y ob ser v ed at t h e en d of t h e f ir st 6 m on t h s
( May) in t he t w o gr oups and dur ing t he last 6 m ont hs
of t he t w o schem es ( Nov em ber ) .
Th e i m p o r t a n c e o f e d u c a t i o n a n d
com pr eh en siv e t h er apeu t ic su ppor t of pat ien t s w it h
c h r o n i c d i s e a s e s h a s b e e n r e p o r t e d i n s o m e
st udies( 13,15- 16).The r equir em ent s for self- car e and t he p s y c h o s o c i a l a s p e c t s i n v o l v e d i n t h e d a i l y
m anagem ent of diabet es ar e a sour ce of st r ess, w hich
m igh t be m in im ized by per son al en gagem en t in t h e
dev elopm en t of k n ow ledge an d adequ at e beh av ior s
t o co p e w i t h t h e se si t u a t i o n s( 1 7 ). Th e r o l e o f t h e healt hcar e t eam in t r aining and educat ion pr ogr am s
is t o ad op t st r at eg ies t o im p r ov e t h e w ay d iab et ic
p a t i e n t s c o p e w i t h d a i l y s i t u a t i o n s a n d
com plicat ion s( 1 7 ). I n t h is r espect , t h er e w as con st an t concer n on t he par t of t he pr ofessionals inv olv ed in
t h e ed u cat ion al g r ou p s an d in d iv id u al m eet in g s t o
enable and pr ovide specific suppor t t o t he par t icipant s
in or der t o m ak e decision s r egar din g diet , ex er cise,
insulin adj ust m ent , and m anagem ent of hypoglycem ia
a n d o t h e r co m p l i ca t i o n s. Th e p a t i e n t s a n d t h e i r
r elat ives w er e encour aged t o under st and t he glycem ic
pr ofiles and t o discuss pr ocedur es w it h t he t eam and
co u l d f r eel y ex p r ess t h ei r o p i n i o n an d d i f f i cu l t i es.
Su b m issiv e b eh av ior s w er e d iscou r ag ed . Th e b on d
est ablished bet w een pat ient s, r elat iv es and t he t eam
w as m aint ained t hr oughout t he 12 m ont hs, including
t elep h on e con t act . We b eliev e t h at t h e k n ow led g e
acquir ed and t he appr oach est ablished in educat ional
p r act i ce su b st an t i al l y con t r i b u t ed t o t h e i m p r ov ed
m et abolic cont r ol obser v ed in t he t w o gr oups.
The im por t ance of t his t ype of under st anding
a p p r o a c h o b j e c t i v e l y d i r e c t e d a t s o l v i n g d a i l y
pr oblem s r elat ed t o t he lack of gly cem ic cont r ol has
been w ell descr ibed in a st udy involving 842 diabet ic
adu lt s t r eat ed w it h in su lin . Th e au t h or s em ph asized
t hat blood glucose m onit oring is not sufficient but t hat
t h e p at ien t s sh ou ld b e ab le t o m an ag e t h e lack of
glycem ic cont r ol w it h t he help of t he t eam , w hich plays
a fundam ent al r ole in t he t eaching and cor r ect ion of
j u d g m en t er r or s r elat ed t o d isease m an ag em en t( 6 ). Th e f i n d i n g s o f a n A m e r i c a n m u l t i c e n t e r s t u d y
in clu d in g 3 5 6 7 ad u lt p at ien t s w it h t y p e 2 d iab et es
suggest t hat hom e blood glucose self- m onit or ing plays
an im por t ant r ole in m et abolic cont r ol only if it is an
i n t e g r a l p a r t o f e d u ca t i o n a l st r a t e g i e s a i m e d a t
pr om ot ing pat ient aut onom y( 13). Alt hough t he pr esent st u dy in v olv ed ch ildr en an d adolescen t s, w e believ e
t h at f av or in g au t on om y is a f u n dam en t al aspect of
t r eat m ent com pliance in chr onic diseases, especially
in adolescen t s.
I n or der t o bet t er u n der st an d t h e beh av ior
of t he gr oups r egar ding t he t w o differ ent m onit or ing
st r at eg ies p r op osed h er e, m u lt ip le com p ar ison s of
m ean HbA1 c concent r at ion w er e per for m ed bet w een
t h e d i f f er en t m o n t h s ( Tab l es 4 an d 5 ) . Basal an d
int r aschem e com par isons dem onst r at ed a super ior it y
of Schem e 1 in t er m s of im pr ov ing m et abolic cont r ol
in t h e t w o gr ou ps, sin ce fou r st at ist ically sign ifican t
d ecl i n es w er e o b ser v ed d u r i n g t h e co u r se o f t h i s
sch em e v er su s on ly on e sig n if ican t d eclin e d u r in g
Sch em e 2 . Th e g r eat er ef f ect iv en ess of Sch em e 1
w a s d em o n st r a t ed b y t h e si g n i f i ca n t r ed u ct i o n o f
g l y ca t ed h em o g l o b i n l ev el s i n g r o u p B ( Ta b l e 5 ) .
I n t e r sch e m e co m p a r i so n s r e v e a l e d w o r se n i n g o f
m et abolic con t r ol w h en ch an gin g fr om Sch em e 1 t o
Schem e 2, w it h six incr eases in HbA1c, t w o of t hem
sign ifican t ( Table 4 ) . Wh en ch an gin g fr om Sch em e 2
t o Sch em e 1 , Hb A1 c lev els im p r ov ed as con f ir m ed
b y t h e ob ser v at ion of sev en d eclin es, t w o of t h em
si g n i f i ca n t ( Ta b l e 5 ) . Th e h i g h e r e f f e ct i v e n e ss o f
Schem e 1 can also be dem onst r at ed w hen com par ing
t h e p e r ce n t a g e r e d u ct i o n i n Hb A1 c co n ce n t r a t i o n
b e t w e e n t h e b e g i n n i n g a n d e n d o f t h e sch e m e s.
Du r in g Sch em e 1 , a 0 . 8 3 % r edu ct ion w as obser v ed
in g r ou p A d u r in g t h e f ir st 6 m on t h s an d a 0 . 3 0 %
r ed u ct i o n w as n o t ed i n g r o u p B d u r i n g t h e l ast 6
m o n t h s. D u r i n g Sch e m e 2 , H b A1 c co n ce n t r a t i o n
declined by 0.12% in gr oup B dur ing t he fir st 6 m ont hs
and incr eased by 0.19% in gr oup A dur ing t he last 6
m on t h s. Sin ce, du r in g Sch em e 1 , t h e pat ien t s on ly
adj ust ed pr epr andial insulin doses, t he possibilit y of
a d j u s t m e n t s w a s g r e a t e r, a f a c t t h a t c e r t a i n l y
cont r ibut ed t o t he higher effect iveness of t his st rat egy.
Th u s, i n t h e p r e se n t st u d y, i n w h i ch p r e p r a n d i a l
ad j u st m en t w as u sed , it is p ossib le t o af f ir m t h at
Sch e m e 1 w a s m o r e e f f e ct i v e t h a n Sch e m e 2 i n
CONCLUSI ONS
Th e t w o m o n i t o r i n g s c h e m e s p e r m i t t e d
t h er ap eu t i c ad j u st m en t s t h at p r om ot ed si g n i f i can t
im pr ov em ent of m et abolic cont r ol in t he t w o gr oups
a s m e a su r e d b y Hb A1 c l e v e l s. Th i s i m p r o v e m e n t
se e m s t o b e r e l a t e d t o a n i n cr e a se d n u m b e r o f
oppor t unit ies for t her apeut ic adj ust m ent pr ov ided by
t he m ont hly m eet ings, m onit or ing and t he educat ional
p r o g r a m d e v e l o p e d . S c h e m e 1 c o n s i s t i n g o f
p r ep r an d ial m on it or in g of b lood g lu cose associat ed
w it h t he adj ust m ent of insulin doses befor e m eals w as
m ore effect ive in prom ot ing m et abolic cont rol since it
per m it t ed a lar ger n u m ber of sign if ican t declin es in
Hb A1 c. Th e p er cen t ag e o f t h ese d ecl i n es w as al so
h igh er du r in g t h is sch em e. Gr ou p A pr esen t ed less
v ar iabilit y an d bet t er HbA1 c in dices t h r ou gh ou t t h e
st udy, but t her e w as no st at ist ical explanat ion for t he
bet t er per for m ance of t his gr oup. I t is possible t hat
s o m e i n t r i n s i c c h a r a c t e r i s t i c s o f t h i s g r o u p n o t
evaluat ed in t he present st udy influenced t he result s,
such as great er int erest , com pliance and part icipat ion.
REFERENCES
1. Diabet es Cont r ol and Com plicat ions Tr ial Resear ch Gr oup.
Th e e f f e c t o f i n t e n s i v e t r e a t m e n t o f d i a b e t e s o n t h e
dev elopm en t an d pr ogr ession of lon g- t er m com plicat ion s in
i n su l i n - d ep en d en t d i ab et es m el l i t u s. N En g l J Med 1 9 9 3 ;
3 2 9 ( 1 4 ) : 9 7 7 - 8 6 .
2. Am er ican Diabet es Associat ion. St andar ds of m edical car e
f o r p at i en t s w i t h d i ab et es m el l i t u s. D i ab et es Car e 2 0 0 3 ;
2 6 ( Su p p l 1 ) : 3 3 - 5 0 .
3 . Ozm e n B, Bo y v a d a S. Th e r e l a t i o n sh i p b e t w e e n se l f
-m o n i t o r i n g o f b l o o d g l u c o s e c o n t r o l a n d g l y c o s y l a t e d
haem oglobin in pat ient s w it h t ype 2 diabet es w it h and w it hout
diabet ic r et inopat hy. J Diabet es Com plicat ions 2 0 0 3 ; 1 7 ( 3 ) :
1 2 8 - 3 4 .
4. Lit w ak LE, Vaglio RM, Alv ar ez A, Gut m an RA. Aut ocont r ol
de la glucem ia capilar : evaluacion del r esult ado a lar go plazo
( 3 a 7 an os) . Medicin a ( Bu en os Air es) 1 9 9 9 ; 5 9 ( 1 ) : 7 1 - 8 .
5 . G r o s s i S A A , Ci a n c i a r u l l o T I , D e l l a M a n n a T.
Ca r a ct e r i za çã o d o s p e r f i s g l i cê m i co s d o m i ci l i a r e s co m o
est r at ég ia p ar a os aj u st es in su lin ot er áp icos em p acien t es
com diabet es m ellit u s do t ipo 1 . Rev Esc En fer m agem USP
2 0 0 3 ; 3 7 ( 1 ) : 6 2 - 7 1 .
6. Schiel R, Müller UA, Rauchfub J, Spr ot t H, Müller R.
Blood-g lu cose self - m on it or in Blood-g in in su lin t r eat ed t y p e 2 d iab et es
m ellit us: a cr oss- sect ional st udy w it h an int er v ent ion gr oup.
Diab et es & Met ab olism ( Par is) 1 9 9 9 ; 2 5 : 3 3 4 - 4 0 .
7 . Halim i S, Ch ar pen t ier G, Gr im aldi A, Gr en ier JL, Bau t F,
Ger m ain B, et al. Effect on com pliance, accept abilit y of blood
g l u co se se l f - m o n i t o r i n g a n d Hb A1 c o f a se l f - m o n i t o r i n g
sy st em dev eloped accor din g t o pat ien t ’s w ish es. Th e accor d
st u dy. Diabet es Met ab ( Par is) 2 0 0 1 ; 2 7 : 6 8 1 - 7 .
8 . St r o w i g SM, Ra sk i n P. I m p r o v e d g l y ce m i c co n t r o l i n
int ensively t r eat ed t ype 1 diabet ic pat ient s using blood glucose
m e t e r s w i t h st o r a g e ca p a b i l i t y a n d co m p u t e r - a ssi st e d
an aly ses. Diab et es Car e 1 9 9 8 ; 2 1 ( 1 0 ) : 1 6 9 4 - 8 .
9. Ny om ba BLG, Ber ar d L, Mur phy LJ. Facilit at ing access t o
glucom et er r eagent s incr eases blood glucose self- m onit or ing
f r eq u en cy an d im p r ov es g ly caem ic con t r ol: a p r osp ect iv e
st u dy in in su lin - t r eat ed diabet ic pat ien t s. Diabet ic Medicin e
2 0 0 3 ; 2 1 : 1 2 9 - 3 5 .
10. Haller MJ, St alvey MS, Silver st ein JH. Pr edict or s of cont r ol
o f d i a b et es: m o n i t o r i n g m a y b e t h e k ey. Th e Jo u r n a l o f
Ped i at r i cs 2 0 0 4 ; 1 4 4 ( 5 ) : 6 6 0 - 1 .
11. Lev ine B, Ander son BJ, But ler JE, Ant isdel JE, Laffel LM.
Predict ors of glycem ic cont rol and short - t erm adverse out com es
in yout h wit h t ype 1 diabet es. J Pediat r.2001; 139: 174- 6.
12. Kar t er AJ, Ack er son LM, Dar binian JA, D’Agost ino RB Jr,
Fer r ar a A, Liu J, et al. Self- m onit or ing of blood glucose levels
a n d g l y c e m i c c o n t r o l : t h e N o r t h e r n Ca l i f o r n i a K a i s e r
Per m an en t Diabet es Regist r y. Am J Med 2 0 0 1 ; 1 1 1 : 1 - 9 .
1 3 . Fr a n ci o si M, Pel l eg r i n i F, D e Ber a r d i s G, Bel f i g l i o M,
Cav alier e D, Di Nar do B et al. The im pact of blood glucose
self- m onit or ing on m et abolic cont r ol and qualit y of life in t ype
2 d iab et ic p at ien t s. Diab et es Car e 2 0 0 1 ; 2 4 ( 1 1 ) : 1 8 7 0 - 7 .
1 4 . Har r i s MI . Fr eq u en cy o f b l o o d g l u co se m o n i t o r i n g i n
r elat ion t o gly cem ic cont r ol in pat ient s w it h t y pe 2 diabet es.
Diab et es Car e 2 0 0 1 ; 2 4 ( 6 ) : 9 7 9 - 8 2 .
1 5 . Fu n n e l l MM, An d e r so n RM. Em p o w e r m e n t a n d se l f
-m a n a g e -m e n t o f d i a b e t e s . Cl i n i c a l D i a b e t e s 2 0 0 4 ;
2 2 ( 3 ) : 1 2 3 - 2 7 .
1 6 . Zan et t i ML, Men d es I AC, Rib eir o KP. O d esaf io p ar a o
con t r ole d om iciliar em cr ian ças e ad olescen t es d iab ét icas
t ipo 1. Rev Lat ino- am Enfer m agem 2001; 9( 4) : 32- 6.
17. Turan B, Osar Z, Turan JM, Dam ci T, I lkowa H. The r ole of
coping w it h disease in adher ence t o t r eat m ent r egim en and
disease cont r ol in t y pe1 and insulin t r eat ed t y pe 2 diabet es
m ellit u s. Diab et es Met ab 2 0 0 2 ; 2 8 : 1 8 6 - 9 3 .