2019/2020
António Luis Felgueira de Andrade
Dynamic Transcranial Doppler Assessment in Heart Failure patients
Avaliação Dinâmica por Doppler Transcraniano em pacientes com
Insuficiência Cardíaca
Mestrado Integrado em Medicina
Área: Neurologia
Tipologia: Dissertação
Trabalho efetuado sob a Orientação de:
Doutor Pedro Miguel Araújo Campos Castro
E sob a Coorientação de:
Dr. Ana Luísa Aires Silva
Trabalho organizado de acordo com as normas da revista:
Brain Sciences
António Luis Felgueira de Andrade
Dynamic Transcranial Doppler Assessment in Heart Failure patients
Avaliação Dinâmica por Doppler Transcraniano em pacientes com
Insuficiência Cardíaca
Dedicatória
À minha família, por todo o seu apoio e benevolência
Aos meus amigos, pela nossa desmedida vivência
À Francisca, pela incansável paciência
Brain Sci. 2020, 10, x; doi: FOR PEER REVIEW www.mdpi.com/journal/brainsci
Article
1
Dynamic transcranial Doppler assessment in heart
2
failure patients
3
António Andrade 1, Ana Aires 2, Elsa Azevedo 3, Gilberto Pereira 4, Filipa Gomes 5, Paulo Araújo 5
4
and Pedro Castro 6,*
5
1 Department of Clinical Neurosciences and Mental Health, Faculty of Medicine, University of Porto, Porto,
6
Portugal; [email protected]
7
2 Department of Neurology, Centro Hospitalar Universitário São João, Faculty of Medicine of University of
8
Porto, Porto, Portugal; [email protected]
9
3 Department of Neurology, Centro Hospitalar Universitário São João, Faculty of Medicine of University of
10
Porto, Porto, Portugal; [email protected]
11
4 Department of Neurology, Centro Hospitalar Universitário São João, Porto, Portugal;
12
13
5 Department of Internal Medicine, Centro Hospitalar Universitário São João, Faculty of Medicine of
14
University of Porto, Porto, Portugal;
15
6 Department of Neurology, Centro Hospitalar Universitário São João, Faculty of Medicine of University of
16
Porto, Porto, Portugal; [email protected]
17
18
* Correspondence: [email protected]
19
Received: date; Accepted: date; Published: date
20
Abstract: Heart failure (HF) is a prevalent disease but few is understood in its repercussion in
21
cerebral hemodynamics mechanisms and cognitive decline. We monitored cerebral blood flow
22
velocity (CBFV) with transcranial Doppler (TCD) in HF patients and healthy controls. Cerebral
23
autoregulation (CA) was assessed by transfer function from the spontaneous oscillations of blood
24
pressure to CBFV and vasoreactivity (VR) with inhalation of CO2 at 5% and hyperventilation.
25
MoCA was measured and associated with each cerebrovascular regulatory component. No
26
differences were detected in VR. HF patients showed a better CA response. (Middle cerebral artery
27
(MCA): very low frequency (VLF) gain 0.47±0.15 vs 0.88±0.19 %/mmHg, p=0.001; low frequency (LF)
28
gain 0.60±0.23 vs 1.28±0.05 %/mmHg, p=0.000; VLF phase 2.05±0.59 vs 1.12±0.12 radians, p=0.021;
29
Posterior cerebral artery (PCA): VLF gain 0.47±0.25 vs 1.11±0.24 %/mmHg, p=0.000; LF gain
30
0.66±0.32 vs 1.83±0.45 %/mmHg, p=0.000). None of the cerebrovascular parameters correlated
31
significantly with MoCA score. Cerebrovascular hemodynamics could have a major role in the
32
proper management of HF patients.
33
Keywords: Heart Failure; Cerebral autoregulation; Vasoreactivity; Transcranial Doppler; MoCA;
34
35
1. Introduction
36
Heart failure (HF) is an epidemic disease [1] with a high morbidity and mortality rate [2]. HF
37
leads to cerebrovascular injury [3] where patients may display cognitive, autonomic and
38
neuropsychological disturbances [4]. This neurologic impairment is thought to have two main
39
mechanisms: stroke and cerebral hypoperfusion [5]. Cerebral hypoperfusion and impairment of
40
cerebral regulation have been implicated either in relevant cognitive deficits [4,6] and brain structural
41
abnormalities [7]. Therefore, impairment of cerebrovascular regulatory mechanisms in HF is of great
Brain Sci. 2020, 10, x FOR PEER REVIEW 2 of 10 importance to better understand the heart-brain dysfunction in this disease. Additionally,
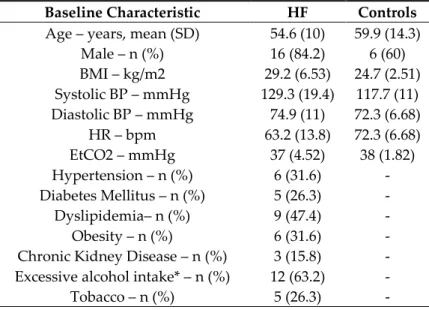
43
cerebrovascular markers can predict future cognitive impairment and help preventing it [8,9].
44
This study aims to evaluate the influence of HF in cerebral hemodynamic mechanisms and its
45
repercussions in cognition.
46
2. Materials and Methods
47
2.1. Study Design
48
All patients were recruited at the Centro Hospitalar Universitário de São João (CHUSJ), Porto
49
from the HF outpatient clinic.
50
Patients were considered appropriate to participate in the study if they fulfilled the inclusion
51
criteria: 1) able to contribute throughout the entire duration of the study, 2) age >18y and ≤75y, 3)
52
diagnosed with systolic heart failure, 4) followed in expert outpatient clinic.
53
Exclusion criteria were: previous history of stroke, dementia or other central nervous system
54
disease that led to cognitive sequels, inadequate temporal window for transcranial Doppler (TCD),
55
intracranial stenosis >50% detected by TCD, stenosis >50% (NASCET method) of the common carotid,
56
internal carotid and vertebral arteries detected by cervical echo-Doppler, atrial fibrillation, severe
57
aortic stenosis (mean gradient ≥40mmHg), mechanic or biologic aortic valvular prosthesis, and other
58
severe valvular disease capable of interfering significantly with cardiac output or associated with
59
high risk of cerebral embolization.
60
10 healthy controls without heart failure were matched with similar age and sex distribution.
61
The study was approved by the local medical ethics committee and all subjects gave their written
62
informed consent.
63
2.2. Medical evaluation
64
Medical history and physical examination were performed in all participants, including
65
measurement of weight, height and blood pressure.
66
All heart failure patients underwent a transthoracic echocardiogram within 3 months of cerebral
67
hemodynamic evaluation. Left ventricular ejection fraction was evaluated according to guidelines
68
[10], as well as cardiac chambers dimensions, transmitral flow and diastolic dysfunction.
69
Neuropsychological evaluation of all participants was obtained with the Portuguese version of
70
Montreal Cognitive Assessment (MoCA). It has been validated in the Portuguese population [11].
71
2.3. Cerebral hemodynamic procedure
72
Cerebral hemodynamic evaluation was performed with TCD at the Neurology Department in
73
CHUSJ and FMUP.
74
Two 2-MHz TCD probes were placed with a signal depth of 50mm on the right and 60mm of the
75
left temporal window. With the intention of obtaining an optimal recording of the cerebral brain flow
76
velocity (CBFV), TCD recorded in the M1 segment of the right middle cerebral artery (MCA) and the
77
P2 segment of the left posterior cerebral artery (PCA). Furthermore, blood pressure (BP) was recorded
78
non-invasively and continuously with Finapres and end-tidal carbon dioxide (EtCO2) was recorded
79
with capnography. DII derivation of 3-lead electrocardiogram evaluated heart rate. Data were
80
synchronized, digitalized and stored for further analysis.
Brain Sci. 2020, 10, x FOR PEER REVIEW 3 of 10 2.3.1. Cerebral Autoregulation
82
For the purpose of analysis of cerebral dynamic autoregulation, a 7-minute period of resting data
83
was recorded. Transfer function analysis allowed the calculation of the gain and phase parameters
84
between the mean BP spectrum and CBFV of MCA and PCA [12].
85
2.3.2. Vasoreactivity
86
Subjects were exposed to a gas mix of 5% CO2 (hypercapnic state) for 2 minutes. After the
87
removal of the inhalation mask, EtCO2 values returned to normal. Afterward, participants
88
hyperventilated reaching an EtCO2 of 25mmHg (hypocapnic state) for 2 minutes.
89
Meanwhile, CBFV variations in MCA and PCA were analyzed for each CO2 value and cerebral
90
VR was measured as the slope of this association and expressed as CBFV variations per mmHg in
91
EtCO2 variation.
92
2.4. Statistics
93
Shapiro-Wilk test was used to assess the normality of the variables. Mean and standard
94
deviation of normal distributed parameters were determined, and heart failure and control groups
95
were compared with Student’s T-test. Non-normal distributed criteria were studied using the
Mann-96
Whitney test and its median and interquartile range were calculated. Categorical baseline
97
characteristics were compared with χ2 test. Statistical analyses were executed using SPSS Statistics,
98
version 25 (IBM, Armonk, NY, USA). A P‐value of <0.05 (two‐sided) was considered statistically
99
significant.
100
3. Results
101
We screened 20 heart failure patients to undertake the full procedure. 19 subjects were able to
102
provide substantial information gathering all or most of the sought parameters while 1 patient was
103
excluded due to carotid stenosis detection.
104
Baseline characteristics comparison of HF patients and healthy controls are described in Table
105
1. 10 controls, with similar age and sex distribution, showed higher heart rate (HR) (63.2±13.8 vs
106
72.3±6.68 bpm, p=0.045).
107
Table 1. Comparison of baseline characteristics of heart failure patients (HF; n = 19) and healthy
108
controls (Controls; n = 10).
109
Baseline Characteristic HF Controls Age – years, mean (SD) 54.6 (10) 59.9 (14.3)
Male – n (%) 16 (84.2) 6 (60) BMI – kg/m2 29.2 (6.53) 24.7 (2.51) Systolic BP – mmHg 129.3 (19.4) 117.7 (11) Diastolic BP – mmHg 74.9 (11) 72.3 (6.68) HR – bpm 63.2 (13.8) 72.3 (6.68) EtCO2 – mmHg 37 (4.52) 38 (1.82) Hypertension – n (%) 6 (31.6) - Diabetes Mellitus – n (%) 5 (26.3) - Dyslipidemia– n (%) 9 (47.4) - Obesity – n (%) 6 (31.6) - Chronic Kidney Disease – n (%) 3 (15.8) - Excessive alcohol intake* – n (%) 12 (63.2) - Tobacco – n (%) 5 (26.3) -
Brain Sci. 2020, 10, x FOR PEER REVIEW 4 of 10 Antihypertensives drugs – n (%) ACEI/ARB 17 (89.5) - Beta-blockers 19 (100) - Diuretics 7 (37) - MRA 10 (52.6) - Sacubitril/Valsartan 1 (5.3) - Ivabradin 6 (31.6) - NYHA Class – n (%) I 12 (63.2) - II 4 (21.1) - III 2 (10.5) - U 1 (5.26) - NYHA Class – n (%) CMD Idiopathic 7 (36.8) - Alcoholic 7 (36.8) - Hypertensive 1 (5.26) - Ischemic 1 (5.26) - Tachycardiomyopathy 1 (5.26) - Myocarditis 1 (5.26) - Chemotherapy-induced 1 (5.26) -
ACEI/ARB: angiotensin converting enzyme inhibitors/angiotensin II receptor blockers BMI: body mass index;
110
BP: blood pressure; bpm: beats per minute; CMD: cardiomyopathy dilated; EtCO2: end-tidal carbon dioxide;
111
HF: heart failure; HR: heart rate; IQR: interquartile range; MRA: mineralocorticoid receptor antagonist
112
NYHA: New York Heart Association; SD: standard deviation; U: unknown. *excess alcohol intake was
113
considered: for men ≥4 drinks per day, for women ≥3 drinks per day.
114
Cerebral hemodynamic values are compared between HF patients and controls in Table 2. There
115
was no difference between the two groups concerning vasoreactivity. However, several parameters
116
(5/11) related to cerebral autoregulation presented statistically significant differences (MCA: VLF
117
gain 0.47±0.15 vs 0.88±0.19 %/mmHg, p 0.001; LF gain 0.60±0.23 vs 1.28±0.05 %/mmHg, p<0.001; VLF
118
phase 2.05±0.59 vs 1.12±0.12 radians, p=0.021; PCA: VLF gain 0.47±0.25 vs 1.11±0.24 %/mmHg,
119
p<0.001; LF gain 0.66±0.32 vs 1.83±0.45 %/mmHg, p<0.001).
120
Table 1. Comparison of cerebrovascular regulatory parameters between heart failure patients (HF; n = 19) and
121
healthy controls (Controls; n = 10).
122
HF Controls MCA mean FV – cm/s 51.6 (13.5) 57.2 (22.1) PCA mean FV– cm/s 35.9 (6.25) 35.1 (26.8)Cerebral Autoregulation
MCA PCA HF Controls HF Controls VLF Gain – %/mmHg 0.47 (0.15) 0.88 (0.19) 0.47 (0.25) 1.11 (0.24) LF Gain – %/mmHg 0.60 (0.23) 1.28 (0.05) 0.66 (0.32) 1.83 (0.45) VLF Phase – radians 2.05 (0.59) 1.12 (0.12) 1.90 (0.59) 1.33 (0.39) LF Phase – radians 1.02 (0.49) 0.61 (0.17) 1.11 (0.50) 0.66 (0.14)Vasoreactivity
MCA PCA HF Controls HF ControlsBrain Sci. 2020, 10, x FOR PEER REVIEW 5 of 10 CO2 Inhalation – %/mmHg 4.65 (3.70) 3.80 (1.40) 3.85 (3.68) 4.10 (3.84) Hyperventilation – %/mmHg 2.55 (2.05) 3.23 (0.88) 2.14 (3.04) 3.51 (1.42) Global VR – %/mmHg 1.83 (1.35) 1.69 (0.65) 1.11 (0.48) 1.07 (0.47) cm/s: centimetre per second; FV: flow velocity; HF: heart failure; Hz: Hertz; LF: low frequency (0.07–0.2 Hz);
123
MCA: middle cerebral artery; mmHg: millimetres of mercury; PCA: posterior cerebral artery; VLF: Very-low
124
frequency (0.03–0.07 Hz);
125
As depicted in Table 3, none of a total of 16 parameters of cerebral hemodynamic has shown a
126
significant correlation with the MoCA score.
127
Table 3. Correlation of cerebrovascular regulatory parameters and MOCA in heart failure patients.
128
R (p-value) MCA mean FV -0.514 (0.087) PCA mean FV 0.049 (0.880)Cerebral Autoregulation
MCA PCA VLF Gain -0.046 (0.888) 0.381 (0.222) LF Gain 0.353 (0.260) 0.400 (0.198) VLF Phase -0.330 (0.425) 0.021 (0.951) LF Phase -0.100 (0.758) -0.365 (0.243)Vasoreactivity
MCA PCA CO2 Inhalation -0.278 (0.357) -0.307 (0.308) Hyperventilation -0.363 (0.223) -0.119 (0.698) Global VR -0.270 (0.373) -0.301 (0.317)FV: flow velocity; HF: heart failure; Hz: Hertz; LF: low frequency (0.07–0.2 Hz); MCA: middle cerebral artery;
129
mmHg: millimetres of mercury; PCA: posterior cerebral artery; VLF: Very-low frequency (0.03–0.07 Hz);
130
4. Discussion
131
Our study compares 19 HF patients with controls and reveals that CA mechanisms appear to be
132
more efficient.
133
The more efficient CA mechanisms in these patients might signify an adaptive response of these
134
patients to low blood pressure either caused by HF itself or its associated antihypertensive
135
medication. Of particular interesting, since is the fact that phase was significantly different at the
136
VLF range. A possible explanation to our results might derive from the fact that chronic brain
137
hypoperfusion in HF patients could induce some direct or remote preconditioning effects at cerebral
138
level rendering it more resistant to ischemia [13]. Hypoxia-inducible factor-1 (HIF-1) is increased in
139
HF patients even with preserved LVEF and correlates with the increased troponin I levels at the
140
admission of decompensated HF [14]. HIF-1-activation pathway reacts to ischemia by increasing
141
serum neurotrophins, vascular endothelial growth factor and erythropoietin concentrations, which
142
are potent neuroprotective agents and involved in cerebrovascular processes, such as collateral
143
vascularization and microvascular angiogenesis [15,16].
Brain Sci. 2020, 10, x FOR PEER REVIEW 6 of 10 Hypoxia stabilizes its active subunit, HIF-1α, through oxygen-sensing mechanism [17]. The
145
protective role of HIF-1 activation in brain vascular disease has been confirmed in animal models of
146
acute ischemic stroke and subarachnoid hemorrhage, using iron chelation agents such as
147
deferoxamine [18]. The way that deferoxamine works is complex but, besides inducing HIF-1 DNA
148
binding and transcription of erythropoietin in vivo and in vitro [18], it also stabilizes HIF-1α,
149
preventing its continuous and rapid proteossomic degradation [19]. Interestingly, recent work in
150
humans, elegantly demonstrated that activation of the HIF-1 regulated pathway with deferoxamine
151
also improved cerebrovascular vasoreactivity and dynamic CA exactly at the VLF range [15].
152
This study suggests that a more efficient cerebrovascular regulation maybe one of the
153
mechanisms by which HIF-1 activation contributes to ischemia tolerance. One possible explanation
154
relies on the expression of other HIF-1-regulated genes like nitric oxide synthase. Nitric oxide, a
155
potent vascular modulator, plays an important role in cerebrovascular function by enhancing CBFV
156
reactivity [20]. For example, in humans, dynamic CA efficiency is reduced by nitric oxide synthase
157
inhibition via l-NMMA (NG-methyl-L-arginine) [20].
158
Therefore, a higher dynamic CA response of HF patients can be an expression of the
hypoxic-159
ischemic preconditioning caused by the HF itself. It should be noticed, however, that this could not
160
be explained by low peripheral BP levels since they were similar in both groups. Finally, we cannot
161
rule out the influence of chronic antihypertensive medication on dynamic CA status of HF patients,
162
particularly, the use of beta-blockers. These drugs can possibly affect dynamic CA through
163
autonomic modulation and decreased sympathetic activity can if fact alter cerebrovascular regulation
164
[21,22].
165
Our CA data does not agree with a study done previously as it states a reduced dynamic CA in
166
ischemic HF patients [23]. However, such contrast in outcome can be the result of differences in the
167
protocol. Unlike Caldas et al., our study excludes severe cases of either intracranial or extracranial
168
stenosis. Therefore, data collected could be influenced as cranial artery stenosis significantly impairs
169
CA [24-27]. Furthermore, the study previously mentioned included only ischemic heart failure
170
patients, while this pilot study does not have such inclusion criteria and solely includes one case of
171
such etiology. Such difference could have major implications as an underlying ischemic environment
172
is frankly associated with white matter lesions [28] which leads to CA impairment [29].
173
However, antihypertensive therapy could have had a major role in these findings. Although it
174
is reported that CA is affected in HF patients, it is as well stated that antihypertensives improve CA
175
[30]. Evidence regarding beta-blockers and calcium channels blockers role in CA is well documented
176
[31-33]. However, studies related to renin-angiotensin-aldosterone system inhibitors provide better
177
results, with some authors stating that cerebral hemodynamic in HF patients are restored after
178
captopril treatment [34].
179
No differences were found in VR parameters in HF patients and healthy controls. This outcome
180
is discordant with a similar study in which the authors conclude that VR is impaired in HF patients
181
[35]. The study previously mentioned only included cases classified as class II, III and IV according
182
to New York Heart Association. Therefore, it is expected that our conclusions were divergent as our
183
study did not have such inclusion criteria and the majority of HF patients were NYHA class I. Our
Brain Sci. 2020, 10, x FOR PEER REVIEW 7 of 10 results show that HF should not have an intrinsic disturbance in vasomotor function to a metabolic
185
stimulus at least in initial course of the disease.
186
MoCA analysis allows us to understand which mechanism modification could be the foundation
187
of cognitive impairment. Based on our results, we may assume that CA and VR are not major factors
188
affecting the cognitive decline in HF. However, this must be clarified by further longitudinal studies
189
This pilot study has some limitations. A noticeable limitation of this study is its small sample
190
size. Nevertheless, our analysis rather focuses on multiple cerebrovascular regulatory components
191
which allowed a detailed study of such a complex phenomenon in its several dimensions. Moreover,
192
HF is a multifaceted disease with a large spectrum in terms of severity and comorbidities. Therefore,
193
each HF has a specific burden in the cerebrovascular mechanism regulation which complicates its
194
analysis and generalization. However, due to the lack of restrictions in the selection of HF patients,
195
it has a more successful application in clinical practice.
196
5. Conclusions
197
Mechanisms of cerebrovascular control are preserved, like CA and VR. Future research is
198
warranted to understand how HF development could lead to the dysfunction at the neurovascular
199
unit which could have an impact on the prevention of cognitive impairment.
200
201
Author Contributions: Conceptualization, E.A., P.A., F.G., P.C.; methodology, E.A., P.A.,G.P., F.G., P.C.;
202
software, E.A., P.A.,G.P., F.G., P.C.; validation, E.A., P.A., F.G., P.C.; formal analysis, A.Andrade, A.Aires, P.C.;
203
investigation, A.Andrade, A.Aires, P.C.; resources A.Andrade, F.G., P.C.; data curation, A.Andrade., P.C.;
204
writing—original draft preparation, A.Andrade; writing—review and editing, A.Andrade, A.Aires, P.C.;
205
visualization, A.Andrade, A.Aires, P.C.; supervision, P.C., E.A.,P.A.; project administration, E.A., P.A., F.G., P.C.
206
; funding acquisition, E.A., P.A., F.G., P.C. All authors have read and agreed to the published version of the
207
manuscript.
208
Funding: This research received no external funding.
209
Acknowledgments: None.
210
Conflicts of Interest: The authors declare no conflict of interest.
211
References
212
1. Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Cardiac failure review 2017, 3,
7-213
11, doi:10.15420/cfr.2016:25:2.
214
2. Levy, D.; Kenchaiah, S.; Larson, M.G.; Benjamin, E.J.; Kupka, M.J.; Ho, K.K.; Murabito, J.M.; Vasan, R.S.
215
Long-term trends in the incidence of and survival with heart failure. The New England journal of medicine
216
2002, 347, 1397-1402, doi:10.1056/NEJMoa020265.
217
3. Havakuk, O.; King, K.S.; Grazette, L.; Yoon, A.J.; Fong, M.; Bregman, N.; Elkayam, U.; Kloner, R.A.
218
Heart Failure-Induced Brain Injury. Journal of the American College of Cardiology 2017, 69, 1609-1616,
219
doi:10.1016/j.jacc.2017.01.022.
220
4. Ogren, J.A.; Fonarow, G.C.; Woo, M.A. Cerebral impairment in heart failure. Current heart failure reports
221
2014, 11, 321-329, doi:10.1007/s11897-014-0211-y.
222
5. Kim, M.S.; Kim, J.J. Heart and brain interconnection - clinical implications of changes in brain function
223
during heart failure. Circulation journal : official journal of the Japanese Circulation Society 2015, 79, 942-947,
224
doi:10.1253/circj.CJ-15-0360.
225
Brain Sci. 2020, 10, x FOR PEER REVIEW 8 of 10
6. Roman, G.C. Brain hypoperfusion: a critical factor in vascular dementia. Neurological research 2004, 26,
226
454-458, doi:10.1179/016164104225017686.
227
7. Kumar, R.; Yadav, S.K.; Palomares, J.A.; Park, B.; Joshi, S.H.; Ogren, J.A.; Macey, P.M.; Fonarow, G.C.;
228
Harper, R.M.; Woo, M.A. Reduced regional brain cortical thickness in patients with heart failure. PloS
229
one 2015, 10, e0126595, doi:10.1371/journal.pone.0126595.
230
8. Beishon, L.; Haunton, V.J.; Panerai, R.B.; Robinson, T.G. Cerebral Hemodynamics in Mild Cognitive
231
Impairment: A Systematic Review. Journal of Alzheimer's disease : JAD 2017, 59, 369-385,
doi:10.3233/jad-232
170181.
233
9. Mataro, M.; Soriano-Raya, J.J.; Lopez-Oloriz, J.; Miralbell, J.; Dacosta-Aguayo, R. Cerebrovascular
234
markers in lowered cognitive function. Journal of Alzheimer's disease : JAD 2014, 42 Suppl 4, S383-391,
235
doi:10.3233/jad-141443.
236
10. Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster,
237
E.; Goldstein, S.A.; Kuznetsova, T., et al. Recommendations for cardiac chamber quantification by
238
echocardiography in adults: an update from the American Society of Echocardiography and the
239
European Association of Cardiovascular Imaging. Journal of the American Society of Echocardiography :
240
official publication of the American Society of Echocardiography 2015, 28, 1-39.e14,
241
doi:10.1016/j.echo.2014.10.003.
242
11. Freitas, S.; Simoes, M.R.; Alves, L.; Santana, I. Montreal Cognitive Assessment (MoCA): normative
243
study for the Portuguese population. Journal of clinical and experimental neuropsychology 2011, 33,
989-244
996, doi:10.1080/13803395.2011.589374.
245
12. Claassen, J.A.; Meel-van den Abeelen, A.S.; Simpson, D.M.; Panerai, R.B. Transfer function analysis of
246
dynamic cerebral autoregulation: A white paper from the International Cerebral Autoregulation
247
Research Network. Journal of cerebral blood flow and metabolism : official journal of the International Society
248
of Cerebral Blood Flow and Metabolism 2016, 36, 665-680, doi:10.1177/0271678x15626425.
249
13. Koch, S.; Della-Morte, D.; Dave, K.R.; Sacco, R.L.; Perez-Pinzon, M.A. Biomarkers for ischemic
250
preconditioning: finding the responders. Journal of cerebral blood flow and metabolism : official journal of the
251
International Society of Cerebral Blood Flow and Metabolism 2014, 34, 933-941, doi:10.1038/jcbfm.2014.42.
252
14. Li, G.; Lu, W.H.; Wu, X.W.; Cheng, J.; Ai, R.; Zhou, Z.H.; Tang, Z.Z. Admission hypoxia-inducible factor
253
1alpha levels and in-hospital mortality in patients with acute decompensated heart failure. BMC
254
cardiovascular disorders 2015, 15, 79, doi:10.1186/s12872-015-0073-6.
255
15. Sorond, F.A.; Tan, C.O.; LaRose, S.; Monk, A.D.; Fichorova, R.; Ryan, S.; Lipsitz, L.A. Deferoxamine,
256
Cerebrovascular Hemodynamics, and Vascular Aging: Potential Role for Hypoxia-Inducible
257
Transcription Factor-1-Regulated Pathways. Stroke 2015, 46, 2576-2583,
258
doi:10.1161/strokeaha.115.009906.
259
16. Fernando, M.S.; Simpson, J.E.; Matthews, F.; Brayne, C.; Lewis, C.E.; Barber, R.; Kalaria, R.N.; Forster,
260
G.; Esteves, F.; Wharton, S.B., et al. White matter lesions in an unselected cohort of the elderly:
261
molecular pathology suggests origin from chronic hypoperfusion injury. Stroke 2006, 37, 1391-1398,
262
doi:10.1161/01.Str.0000221308.94473.14.
263
17. Bernaudin, M.; Sharp, F.R. Methods to detect hypoxia-induced ischemic tolerance in the brain. Methods
264
Enzymol 2004, 381, 399-416, doi:10.1016/s0076-6879(04)81027-9.
265
18. Prass, K.; Ruscher, K.; Karsch, M.; Isaev, N.; Megow, D.; Priller, J.; Scharff, A.; Dirnagl, U.; Meisel, A.
266
Desferrioxamine induces delayed tolerance against cerebral ischemia in vivo and in vitro. Journal of
267
Brain Sci. 2020, 10, x FOR PEER REVIEW 9 of 10 cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and
268
Metabolism 2002, 22, 520-525, doi:10.1097/00004647-200205000-00003.
269
19. Chu, K.; Jung, K.H.; Kim, S.J.; Lee, S.T.; Kim, J.; Park, H.K.; Song, E.C.; Kim, S.U.; Kim, M.; Lee, S.K., et
270
al. Transplantation of human neural stem cells protect against ischemia in a preventive mode via
271
hypoxia-inducible factor-1alpha stabilization in the host brain. Brain research 2008, 1207, 182-192,
272
doi:10.1016/j.brainres.2008.02.043.
273
20. White, R.P.; Vallance, P.; Markus, H.S. Effect of inhibition of nitric oxide synthase on dynamic cerebral
274
autoregulation in humans. Clinical science (London, England : 1979) 2000, 99, 555-560.
275
21. Azevedo, E.; Castro, P.; Santos, R.; Freitas, J.; Coelho, T.; Rosengarten, B.; Panerai, R. Autonomic
276
dysfunction affects cerebral neurovascular coupling. Clinical autonomic research : official journal of the
277
Clinical Autonomic Research Society 2011, 21, 395-403, doi:10.1007/s10286-011-0129-3.
278
22. Castro, P.M.; Santos, R.; Freitas, J.; Panerai, R.B.; Azevedo, E. Autonomic dysfunction affects dynamic
279
cerebral autoregulation during Valsalva maneuver: comparison between healthy and autonomic
280
dysfunction subjects. Journal of applied physiology (Bethesda, Md. : 1985) 2014, 117, 205-213,
281
doi:10.1152/japplphysiol.00893.2013.
282
23. Caldas, J.R.; Panerai, R.B.; Haunton, V.J.; Almeida, J.P.; Ferreira, G.S.; Camara, L.; Nogueira, R.C.;
Bor-283
Seng-Shu, E.; Oliveira, M.L.; Groehs, R.R., et al. Cerebral blood flow autoregulation in ischemic heart
284
failure. American journal of physiology. Regulatory, integrative and comparative physiology 2017, 312,
R108-285
r113, doi:10.1152/ajpregu.00361.2016.
286
24. Chen, J.; Liu, J.; Xu, W.H.; Xu, R.; Hou, B.; Cui, L.Y.; Gao, S. Impaired dynamic cerebral autoregulation
287
and cerebrovascular reactivity in middle cerebral artery stenosis. PloS one 2014, 9, e88232,
288
doi:10.1371/journal.pone.0088232.
289
25. Gong, X.P.; Li, Y.; Jiang, W.J.; Wang, Y. Impaired dynamic cerebral autoregulation in middle cerebral
290
artery stenosis. Neurological research 2006, 28, 76-81, doi:10.1179/016164106x91915.
291
26. Wang, S.; Guo, Z.N.; Xing, Y.; Ma, H.; Jin, H.; Liu, J.; Yang, Y. Dynamic Cerebral Autoregulation in
292
Asymptomatic Patients With Unilateral Middle Cerebral Artery Stenosis. Medicine 2015, 94, e2234,
293
doi:10.1097/md.0000000000002234.
294
27. White, R.P.; Markus, H.S. Impaired dynamic cerebral autoregulation in carotid artery stenosis. Stroke
295
1997, 28, 1340-1344, doi:10.1161/01.str.28.7.1340.
296
28. Lin, J.; Wang, D.; Lan, L.; Fan, Y. Multiple Factors Involved in the Pathogenesis of White Matter Lesions.
297
BioMed research international 2017, 2017, 9372050, doi:10.1155/2017/9372050.
298
29. Purkayastha, S.; Fadar, O.; Mehregan, A.; Salat, D.H.; Moscufo, N.; Meier, D.S.; Guttmann, C.R.; Fisher,
299
N.D.; Lipsitz, L.A.; Sorond, F.A. Impaired cerebrovascular hemodynamics are associated with cerebral
300
white matter damage. Journal of cerebral blood flow and metabolism : official journal of the International Society
301
of Cerebral Blood Flow and Metabolism 2014, 34, 228-234, doi:10.1038/jcbfm.2013.180.
302
30. Lipsitz, L.A.; Gagnon, M.; Vyas, M.; Iloputaife, I.; Kiely, D.K.; Sorond, F.; Serrador, J.; Cheng, D.M.;
303
Babikian, V.; Cupples, L.A. Antihypertensive therapy increases cerebral blood flow and carotid
304
distensibility in hypertensive elderly subjects. Hypertension (Dallas, Tex. : 1979) 2005, 45, 216-221,
305
doi:10.1161/01.Hyp.0000153094.09615.11.
306
31. Shinyama, H.; Nagai, H.; Kawamura, T.; Narita, Y.; Nakamura, N.; Kagitani, Y. Effects of long-term
307
treatment with the calcium antagonist AE0047 on cerebrovascular autoregulation and hypertrophy in
308
spontaneously hypertensive rats. Journal of cardiovascular pharmacology 1997, 30, 616-622,
309
doi:10.1097/00005344-199711000-00012.
310
Brain Sci. 2020, 10, x FOR PEER REVIEW 10 of 10
32. Ikeda, J.; Yao, K.; Matsubara, M. Effects of benidipine, a long-lasting dihydropyridine-Ca2+ channel
311
blocker, on cerebral blood flow autoregulation in spontaneously hypertensive rats. Biological &
312
pharmaceutical bulletin 2006, 29, 2222-2225, doi:10.1248/bpb.29.2222.
313
33. Sadoshima, S.; Okada, Y.; Ooboshi, H.; Shiokawa, O.; Fujishima, M. [Effects of alpha- and
beta-314
adrenergic blockers on the lower limits of cerebral blood flow autoregulation in spontaneously
315
hypertensive rats]. Fukuoka igaku zasshi = Hukuoka acta medica 1990, 81, 204-208.
316
34. Rajagopalan, B.; Raine, A.E.; Cooper, R.; Ledingham, J.G. Changes in cerebral blood flow in patients
317
with severe congestive cardiac failure before and after captopril treatment. The American journal of
318
medicine 1984, 76, 86-90, doi:10.1016/0002-9343(84)90891-x.
319
35. Georgiadis, D.; Sievert, M.; Cencetti, S.; Uhlmann, F.; Krivokuca, M.; Zierz, S.; Werdan, K.
320
Cerebrovascular reactivity is impaired in patients with cardiac failure. European heart journal 2000, 21,
321
407-413, doi:10.1053/euhj.1999.1742.
322
323
© 2020 by the authors. Submitted for possible open access publication under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Normas de Publicação – Brain Sciences
Manuscript Submission Overview
Types of Publications
Brain Sciences has no restrictions on the length of manuscripts, provided that the text is concise and
comprehensive. Full experimental details must be provided so that the results can be reproduced. Brain
Sciences requires that authors publish all experimental controls and make full datasets available where
possible (see the guidelines on Supplementary Materials and references to unpublished data).
Manuscripts submitted to Brain Sciences should neither been published before nor be under consideration for publication in another journal. The main article types are as follows:
• Articles: Original research manuscripts. The journal considers all original research manuscripts
provided that the work reports scientifically sound experiments and provides a substantial amount of new information. Authors should not unnecessarily divide their work into several related manuscripts, although Short Communications of preliminary, but significant, results will be considered. Quality and impact of the study will be considered during peer review.
• Reviews: These provide concise and precise updates on the latest progress made in a given area of
research. Systematic reviews should follow the PRISMA guidelines.
• Case reports: Case reports present detailed information on the symptoms, signs, diagnosis, treatment
(including all types of interventions), and outcomes of an individual patient. Case reports usually describe new or uncommon conditions that serve to enhance medical care or highlight diagnostic approaches.
Submission Process
Manuscripts for Brain Sciences should be submitted online at susy.mdpi.com. The submitting author, who is generally the corresponding author, is responsible for the manuscript during the submission and peer-review process. The submitting author must ensure that all eligible co-authors have been included in the author list (read the criteria to qualify for authorship) and that they have all read and approved the submitted version of the manuscript. To submit your manuscript, register and log in to the submission website. Once you have registered, click here to go to the submission form for Brain Sciences. All co-authors can see the manuscript details in the submission system, if they register and log in using the e-mail address provided during manuscript submission.
Accepted File Formats
Authors must use the Microsoft Word template or LaTeX template to prepare their manuscript. Using the template file will substantially shorten the time to complete copy-editing and publication of accepted
manuscripts. The total amount of data for all files must not exceed 120 MB. If this is a problem, please contact the editorial office [email protected]. Accepted file formats are:
• Microsoft Word: Manuscripts prepared in Microsoft Word must be converted into a single file before
submission. When preparing manuscripts in Microsoft Word, the Brain Sciences Microsoft Word
template file must be used. Please insert your graphics (schemes, figures, etc.) in the main text after the paragraph of its first citation.
• LaTeX: Manuscripts prepared in LaTeX must be collated into one ZIP folder (include all source files
and images, so that the Editorial Office can recompile the submitted PDF). When preparing
manuscripts in LaTeX, please use the Brain Sciences LaTeX template files. You can now also use
the online application writeLaTeX to submit articles directly to Brain Sciences. The MDPI LaTeX template file should be selected from the writeLaTeX template gallery.
• Supplementary files: May be any format, but it is recommended that you use common,
Cover Letter
A cover letter must be included with each manuscript submission. It should be concise and explain why the content of the paper is significant, placing the findings in the context of existing work and why it fits the scope of the journal. Confirm that neither the manuscript nor any parts of its content are currently under consideration or published in another journal. Any prior submissions of the manuscript to MDPI journals must be
acknowledged. The names of proposed and excluded reviewers should be provided in the submission system, not in the cover letter.
Note for Authors Funded by the National Institutes of Health (NIH)
This journal automatically deposits papers to PubMed Central after publication of an issue. Authors do not need to separately submit their papers through the NIH Manuscript Submission System
(NIHMS, http://nihms.nih.gov/). [Return to top]
Manuscript Preparation
General Considerations
• Research manuscripts should comprise:
o Front matter: Title, Author list, Affiliations, Abstract, Keywords
o Research manuscript sections: Introduction, Materials and Methods, Results, Discussion, Conclusions (optional).
o Back matter: Supplementary Materials, Acknowledgments, Author Contributions, Conflicts of Interest, References.
• Review manuscripts should comprise the front matter, literature review sections and the back matter. The template file can also be used to prepare the front and back matter of your review manuscript. It is not necessary to follow the remaining structure. Structured reviews and meta-analyses should use the same structure as research articles and ensure they conform to the PRISMA guidelines.
• Case reports should include a succinct introduction about the general medical condition or relevant
symptoms that will be discussed in the case report; the case presentation including all of the relevant de-identified demographic and descriptive information about the patient(s), and a description of the symptoms, diagnosis, treatment, and outcome; a discussion providing context and any necessary explanation of specific treatment decisions; a conclusion briefly outlining the take-home message and the lessons learned.
• Graphical abstract: Authors are encouraged to provide a graphical abstract as a self-explanatory
image to appear alongside with the text abstract in the Table of Contents. Figures should be a high quality image in any common image format. Note that images displayed online will be up to 11 by 9 cm on screen and the figure should be clear at this size.
• Abbreviations should be defined in parentheses the first time they appear in the abstract, main text,
and in figure or table captions and used consistently thereafter.
• SI Units (International System of Units) should be used. Imperial, US customary and other units
should be converted to SI units whenever possible
• Accession numbers of RNA, DNA and protein sequences used in the manuscript should be
provided in the Materials and Methods section. Also see the section on Deposition of Sequences
and of Expression Data.
• Equations: If you are using Word, please use either the Microsoft Equation Editor or the MathType
• Research Data and supplementary materials: Note that publication of your manuscript implies that
you must make all materials, data, and protocols associated with the publication available to readers. Disclose at the submission stage any restrictions on the availability of materials or information. Read the information about Supplementary Materials and Data Deposit for additional guidelines. • Preregistration: Where authors have preregistered studies or analysis plans, links to the
preregistration must be provided in the manuscript.
• Guidelines and standards: MDPI follows standards and guidelines for certain types of research.
See https://www.mdpi.com/editorial_process for further information. [Return to top]
Front Matter
These sections should appear in all manuscript types
• Title: The title of your manuscript should be concise, specific and relevant. It should identify if the
study reports (human or animal) trial data, or is a systematic review, meta-analysis or replication study. When gene or protein names are included, the abbreviated name rather than full name should be used.
• Author List and Affiliations: Authors' full first and last names must be provided. The initials of any
middle names can be added. The PubMed/MEDLINE standard format is used for affiliations: complete address information including city, zip code, state/province, and country. At least one author should be designated as corresponding author, and his or her email address and other details should be included at the end of the affiliation section. Please read the criteria to qualify for authorship.
• Abstract: The abstract should be a total of about 200 words maximum. The abstract should be a
single paragraph and should follow the style of structured abstracts, but without headings: 1)
Background: Place the question addressed in a broad context and highlight the purpose of the study; 2) Methods: Describe briefly the main methods or treatments applied. Include any relevant
preregistration numbers, and species and strains of any animals used. 3) Results: Summarize the article's main findings; and 4) Conclusion: Indicate the main conclusions or interpretations. The abstract should be an objective representation of the article: it must not contain results which are not presented and substantiated in the main text and should not exaggerate the main conclusions.
• Keywords: Three to ten pertinent keywords need to be added after the abstract. We recommend that
the keywords are specific to the article, yet reasonably common within the subject discipline.
Research Manuscript Sections
• Introduction: The introduction should briefly place the study in a broad context and highlight why it is
important. It should define the purpose of the work and its significance, including specific hypotheses being tested. The current state of the research field should be reviewed carefully and key publications cited. Please highlight controversial and diverging hypotheses when necessary. Finally, briefly mention the main aim of the workand highlight the main conclusions. Keep the introduction comprehensible to scientists working outside the topic of the paper.
• Materials and Methods: They should be described with sufficient detail to allow others to replicate
and build on published results. New methods and protocols should be described in detail while well-established methods can be briefly described and appropriately cited. Give the name and version of any software used and make clear whether computer code used is available. Include any pre-registration codes.
• Results: Provide a concise and precise description of the experimental results, their interpretation as
well as the experimental conclusions that can be drawn.
• Discussion: Authors should discuss the results and how they can be interpreted in perspective of
previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible and limitations of the work highlighted. Future research directions may also be mentioned. This section may be combined with Results.
• Conclusions: This section is not mandatory, but can be added to the manuscript if the discussion is
unusually long or complex.
• Patents: This section is not mandatory, but may be added if there are patents resulting from the work
reported in this manuscript. [Return to top]
Back Matter
• Supplementary Materials: Describe any supplementary material published online alongside the
manuscript (figure, tables, video, spreadsheets, etc.). Please indicate the name and title of each element as follows Figure S1: title, Table S1: title, etc.
• Acknowledgments: All sources of funding of the study should be disclosed. Clearly indicate grants
that you have received in support of your research work and if you received funds to cover publication costs. Note that some funders will not refund article processing charges (APC) if the funder and grant number are not clearly and correctly identified in the paper. Funding information can be entered separately into the submission system by the authors during submission of their manuscript. Such funding information, if available, will be deposited to FundRef if the manuscript is finally published.
• Author Contributions: Each author is expected to have made substantial contributions to the
conception or design of the work; or the acquisition, analysis, or interpretation of data; or the creation of new software used in the work; or have drafted the work or substantively revised it; AND has approved the submitted version (and version substantially edited by journal staff that involves the author’s contribution to the study); AND agrees to be personally accountable for the author’s own contributions and for ensuring that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and documented in the literature.
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used "Conceptualization, X.X. and Y.Y.; Methodology, X.X.; Software, X.X.; Validation, X.X., Y.Y. and Z.Z.; Formal Analysis, X.X.;
Investigation, X.X.; Resources, X.X.; Data Curation, X.X.; Writing – Original Draft Preparation, X.X.; Writing – Review & Editing, X.X.; Visualization, X.X.; Supervision, X.X.; Project Administration, X.X.; Funding Acquisition, Y.Y.”, please turn to the CRediT taxonomy for the term explanation. For more background on CRediT, see here. "Authorship must include and be limited to those who have
contributed substantially to the work. Please read the section concerning the criteria to qualify for authorship carefully".
• Conflicts of Interest: Authors must identify and declare any personal circumstances or interest that
may be perceived as inappropriately influencing the representation or interpretation of reported research results. If there is no conflict of interest, please state "The authors declare no conflict of interest." Any role of the funding sponsors in the choice of research project; design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript; or in the decision to publish the results must be declared in this section. Brain Sciences does not publish studies funded by the tobacco industry. Any projects funded by pharmaceutical or food industries must pay special attention to the full declaration of funder involvement. If there is no role, please state “The sponsors had no role in the design, execution, interpretation, or writing of the study”.
• References: References must be numbered in order of appearance in the text (including table
captions and figure legends) and listed individually at the end of the manuscript. We recommend preparing the references with a bibliography software package, such
as EndNote, ReferenceManager or Zotero to avoid typing mistakes and duplicated references. We encourage citations to data, computer code and other citable research material. If available online, you may use reference style 9. below.
• Citations and References in Supplementary files are permitted provided that they also appear in the main text and in the reference list.
In the text, reference numbers should be placed in square brackets [ ], and placed before the punctuation; for example [1], [1–3] or [1,3]. For embedded citations in the text with pagination, use both parentheses and brackets to indicate the reference number and page numbers; for example [5] (p. 10). or [6] (pp. 101–105).
The reference list should include the full title, as recommended by the ACS style guide. Style files for Endnote and Zotero are available.
References should be described as follows, depending on the type of work:
• Journal Articles:
1. Author 1, A.B.; Author 2, C.D. Title of the article. Abbreviated Journal
Name Year, Volume, page range.
• Books and Book Chapters:
2. Author 1, A.; Author 2, B. Book Title, 3rd ed.; Publisher: Publisher Location, Country,
Year; pp. 154–196.
3. Author 1, A.; Author 2, B. Title of the chapter. In Book Title, 2nd ed.; Editor 1, A.,
Editor 2, B., Eds.; Publisher: Publisher Location, Country, Year; Volume 3, pp. 154–196.
• Unpublished work, submitted work, personal communication:
4. Author 1, A.B.; Author 2, C. Title of Unpublished Work. status (unpublished;
manuscript in preparation).
5. Author 1, A.B.; Author 2, C. Title of Unpublished Work. Abbreviated Journal
Name stage of publication (under review; accepted; in press).
6. Author 1, A.B. (University, City, State, Country); Author 2, C. (Institute, City, State,
Country). Personal communication, Year.
• Conference Proceedings:
7. Author 1, A.B.; Author 2, C.D.; Author 3, E.F. Title of Presentation. In Title of the
Collected Work (if available), Proceedings of the Name of the Conference, Location of
Conference, Country, Date of Conference; Editor 1, Editor 2, Eds. (if available); Publisher:
City, Country, Year (if available); Abstract Number (optional), Pagination (optional).
• Thesis:
8. Author 1, A.B. Title of Thesis. Level of Thesis, Degree-Granting University, Location of
University, Date of Completion.
• Websites:
9. Title of Site. Available online: URL (accessed on Day Month Year).
Unlike published works, websites may change over time or disappear, so we encourage you
create an archive of the cited website using a service such as
WebCite
. Archived websites
should be cited using the link provided as follows:
10. Title of Site. URL (archived on Day Month Year).
See the Reference List and Citations Guide for more detailed information. [Return to top]
Preparing Figures, Schemes and Tables
• File for Figures and Schemes must be provided during submission in a single zip archive and at a sufficiently high resolution (minimum 1000 pixels width/height, or a resolution of 300 dpi or higher). Common formats are accepted, however, TIFF, JPEG, EPS and PDF are preferred.
• Brain Sciences can publish multimedia files in articles or as supplementary materials. Please contact
the editorial office for further information.
• All Figures, Schemes and Tables should be inserted into the main text close to their first citation and must be numbered following their number of appearance (Figure 1, Scheme I, Figure 2, Scheme II, Table 1, etc.).
• All table columns should have an explanatory heading. To facilitate the copy-editing of larger tables, smaller fonts may be used, but no less than 8 pt. in size. Authors should use the Table option of Microsoft Word to create tables.
• Authors are encouraged to prepare figures and schemes in color (RGB at 8-bit per channel). There is no additional cost for publishing full color graphics.
[Return to top]
Supplementary Materials, Data Deposit and Software Source
Code
Data Availability
In order to maintain the integrity, transparency and reproducibility of research records, authors must make their experimental and research data openly available either by depositing into data repositories or by publishing the data and files as supplementary information in this journal.
Computer Code and Software
For work where novel computer code was developed, authors should release the code either by depositing in a recognized, public repository or uploading as supplementary information to the publication. The name and version of all software used should be clearly indicated.
Supplementary Material
Additional data and files can be uploaded as "Supplementary Files" during the manuscript submission process. The supplementary files will also be available to the referees as part of the peer-review process. Any file format is acceptable, however we recommend that common, non-proprietary formats are used where possible.
Unpublished Data
Restrictions on data availability should be noted during submission and in the manuscript. "Data not shown" should be avoided: authors are encouraged to publish all observations related to the submitted manuscript as Supplementary Material. "Unpublished data" intended for publication in a manuscript that is either planned, "in preparation" or "submitted" but not yet accepted, should be cited in the text and a reference should be added in the References section. "Personal Communication" should also be cited in the text and reference added in the References section. (see also the MDPI reference list and citations style guide).
Remote Hosting and Large Data Sets
Data may be deposited with specialized service providers or institutional/subject repositories, preferably those that use the DataCite mechanism. Large data sets and files greater than 60 MB must be deposited in this way. For a list of other repositories specialized in scientific and experimental data, please consult databib.org or re3data.org. The data repository name, link to the data set (URL) and accession number, doi or handle number of the data set must be provided in the paper. The journal Data also accepts submissions of data set papers.
Deposition of Sequences and of Expression Data
New sequence information must be deposited to the appropriate database prior to submission of the manuscript. Accession numbers provided by the database should be included in the submitted manuscript. Manuscripts will not be published until the accession number is provided.
• New nucleic acid sequences must be deposited in one of the following databases: GenBank, EMBL,
or DDBJ. Sequences should be submitted to only one database.
• New high throughput sequencing (HTS) datasets (RNA-seq, ChIP-Seq, degradome analysis, …) must
be deposited either in the GEO database or in the NCBI’s Sequence Read Archive.
• New microarray data must be deposited either in the GEO or the ArrayExpress databases.The
"Minimal Information About a Microarray Experiment" (MIAME) guidelines published by the Microarray Gene Expression Data Society must be followed.
• New protein sequences obtained by protein sequencing must be submitted to UniProt (submission
tool SPIN).
All sequence names and the accession numbers provided by the databases should be provided in the Materials and Methods section of the article.
References in Supplementary Files
Citations and References in Supplementary files are permitted provided that they also appear in the reference list of the main text.