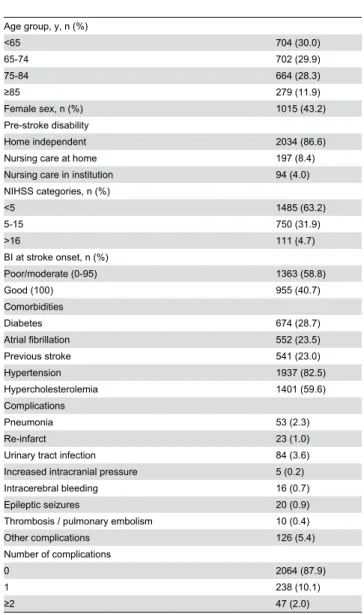
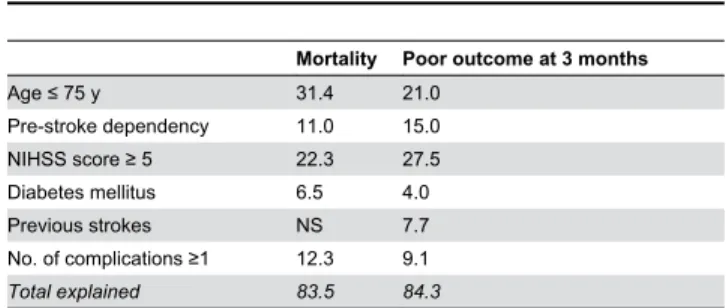
Influence of acute complications on outcome 3 months after ischemic stroke.
Texto
Imagem
Documentos relacionados
Demographic socio-economic data, cardiovascular risk factors, Causative Classiication System for Ischemic Stroke, Trial of Org 10172 in Acute Stroke Treatment and National
2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the early management of patients with acute ischemic stroke
As observed during the review, the proposed tools and tech- niques aim to encode knowledge on structural, functional, mechani- cal properties and manufacturing processes to support
Diante de tal quadro, a Secretaria da Identidade e da Diversidade Cultural (2007) continuará trabalhando, com base nas propostas e nos resultados apontados pelo Grupo de Trabalho
Equívocos”, in MONTEIRO, Francisco; MARTINGO, Ângelo (eds.) Interpretação Musical: Teoria e Prática, (“Ensaios Musicológicos, 3”). Lisboa: Edições Colibri.. elitista e
Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American
A apresentação de uma hipótese de modelo de análise original adequado à realidade que se pretende observar (conteúdos das páginas do Facebook produzidos por
