www.jped.com.br
ORIGINAL
ARTICLE
Painful
procedures
and
analgesia
in
the
NICU:
what
has
changed
in
the
medical
perception
and
practice
in
a
ten-year
period?
夽
,
夽夽
Ana
Claudia
Yoshikumi
Prestes
a,
Rita
de
Cássia
Xavier
Balda
a,
Gianni
Mara
Silva
dos
Santos
b,
Ligia
Maria
Suppo
de
Souza
Rugolo
c,
Maria
Regina
Bentlin
c,
Mauricio
Magalhães
d,e,
Paulo
Roberto
Pachi
d,
Sergio
Tadeu
Martins
Marba
f,
Jamil
Pedro
de
Siqueira
Caldas
g,
Ruth
Guinsburg
a,∗aDivisionofNeonatalMedicine,EscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,
SP,Brazil
bUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
cDepartmentofPediatrics,FaculdadedeMedicinadeBotucatu(FMB),UniversidadeEstadualPaulistaJúliodeMesquitaFilho
(UNESP),Botucatu,SP,Brazil
dDepartmentofPediatrics,FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil eServiceofNeonatology,FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil fDepartmentofPediatrics,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
gDivisionofNeonatology,HospitaldaMulherProf.Dr.JoséAristodemoPinotti,CentrodeAtenc¸ãoIntegralàSaúdedaMulher
(CAISM),UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
Received12March2015;accepted27April2015 Availableonline9October2015
KEYWORDS
Painmeasurement; Painperception; Painmanagement;
Abstract
Objective: Tocomparetheuseofanalgesiaversusneonatologists’perceptionregarding
anal-gesicuseinpainfulproceduresintheyears2001,2006,and2011.
Methods: This was a prospective cohort study of all newborns admitted to four university
neonatalintensive careunits duringonemonth in2001, 2006,and 2011.The frequencyof
夽 Pleasecitethisarticleas:PrestesAC,BaldaRC,dosSantosGM,RugoloLM,BentlinMR,MagalhãesM,etal.Painfulproceduresand
analgesiaintheNICU:whathaschangedinthemedicalperceptionandpracticeinaten-yearperiod?JPediatr(RioJ).2016;92:88---95. 夽夽StudyconductedatFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil;UniversidadeEstadual
deCampinas(UNICAMP),Campinas,SP,Brazil;FaculdadedeMedicinadeBotucatu(FMB),UniversidadeEstadualPaulistaJúliodeMesquita Filho(UNESP),Botucatu,SP,Brazil;andEscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP, Brazil.
∗Correspondingauthor.
E-mail:[email protected](R.Guinsburg).
http://dx.doi.org/10.1016/j.jped.2015.04.009
Neonatalintensive careunits; Newborn
analgesic prescription forpainfulprocedureswas evaluated.Ofthe202 neonatologists,188 answeredaquestionnairegivingtheiropinionontheintensityofpainduringlumbarpuncture, tracheal intubation, mechanicalventilation, and postoperative period using a10-cm visual analogicscale(VAS;pain>3cm).
Results: Forlumbarpuncture,12%(2001),43%(2006),and36%(2011)wereperformedusing
analgesia.Amongtheneonatologists,40---50%reportedVAS>3forlumbarpunctureinallstudy periods.Forintubation,30%receivedanalgesiainthestudyperiods,and35%(2001),55%(2006), and73%(2011)oftheneonatologistsreportedVAS>3 andwouldprescribeanalgesiafor this procedure.Asformechanicalventilation,45%(2001),64%(2006),and48%(2011)of patient-dayswereunderanalgesia;56%(2001),57%(2006),and26%(2011)ofneonatologistsreported VAS>3 andsaidtheywoulduse analgesiaduringmechanicalventilation.For thefirst three post-operativedays,37%(2001),78%(2006),and89%(2011)ofthepatientsreceivedanalgesia andmorethan90%ofneonatologistsreportedVAS>3formajorsurgeries.
Conclusions: Despiteanincreaseinthemedicalperceptionofneonatalpainandinanalgesic
useduringpainfulprocedures,thegapbetweenclinicalpracticeandneonatologistperception ofanalgesianeeddidnotchangeduringtheten-yearperiod.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Medic¸ãodador; Percepc¸ãodador; Manejodador; Unidadesdeterapia intensivaneonatal; Recém-nascido
ProcedimentosdolorososeanalgesiaemUTINeonatal:oquemudounaopinião enapráticaprofissionalemdezanos?
Resumo
Objetivo: Confrontar o uso de analgesia versus a percepc¸ão de neonatologistas quanto ao
empregodeanalgésicosparaprocedimentosdolorososnosanosde2001,2006e2011.
Métodos: Coorteprospectivadetodosrecém-nascidosinternadosemquatrounidades
univer-sitárias.Avaliou-seafrequênciadoempregodeanalgésicosparaprocedimentosdolorosospor um mêsdos anosde estudo.Dos202neonatologistasatuantes nasunidades nostrês perío-dos, 188assinalaramem escala analógicavisual de 10cm(dor >3cm) aintensidadeda dor sentida pelo recém-nascido na punc¸ão lombar, intubac¸ão traqueal, ventilac¸ão mecânica e pós-operatório.
Resultados: ParaPL,12%,43%e36%foramrealizadascomanalgesiaem2001,2006e2011e
40-50%dosneonatologistasreferiamindicaranalgésicosnapunc¸ãolombarnostrêsperíodos. Naintubac¸ão,30%foramrealizadassobanalgesianostrêsperíodose35%(2001),55%(2006)e 73%(2011)dosmédicosdiziamindicaranalgésicos.Quantoàventilac¸ãomecânica,45-64%dos ventilados-diaestavamsobanalgesianostrêsperíodose56%(2001),57%(2006)e26%(2011) dosneonatologistasdiziamusaranalgésicos.Dospacientes-dianostrêsprimeirosdiasde pós-operatório,37%(2001),78%(2006)e89%(2011)receberamalgumadosedeanalgésico,sendo quemaisde90%dosmédicosreferiamusaranalgesiaparaessasituac¸ão.
Conclusões: Entre2001e2011,ocorreuaumentonousodeanalgésicos paraprocedimentos
dolorososnasunidadesneonataiseumapercepc¸ãomaisacentuadaporpartedosmédicosde queorecém-nascidosentedor,masolapsoentreapráticaclínicaeapercepc¸ãomédicaquanto àpresenc¸adedorpersistiu.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Painfuleventsarecommoninnewbornswhorequire inten-sivecare.Simonsetal.1observed151newbornsinthefirst
14 daysof admission tothe intensive care unit (ICU) and eachwassubmittedtoanaverageof14painfulprocedures aday.Prestesetal.2verifiedthatthreetofivepotentially
painfulprocedureswereperformedperpatient/dayin uni-versityneonatalunitsinSãoPaulo.Carbajaletal.3assessed
430 newborns in the Paris region in the first 14 days of life and observed, on average, ten painful procedures a
day. Cignacco et al.4 studied 120 infants on mechanical
ventilationduringthefirst14daysoflifeintwoSwissunits andfound23painfulprocedures/dayperpatient.
Despitethisscenario,theuseofmeasurestorelievethe painduringpotentially painful proceduresis unusual,and it is estimated that only 3% of newborns receive specific analgesiafortheprocedureandthat,in30%,adjuvant tech-niquesareappliedtominimizepain.1---3 InItaly,fiveyears
units for tracheal intubation,47% for mechanical ventila-tion,33% for lumbarpuncture, and 64%for postoperative pain.5
Therefore,aparadoxisobservedbetweenthefrequency ofconditionsthatcause painincritically illneonatesand theuseofanalgesiainneonatalunits.Themostoftencited causesfor thisparadox aretheseveralmyths surrounding thepainfulexperienceintheneonatalpopulation, particu-larlytheperceptionthatthenewbornistooimmaturetofeel pain.6---8Itisknownthattheknowledgeaboutthepresence
ofpaininnewbornshasgreatlyincreasedamonghealth pro-fessionalsresponsibleforneonatalcare,9butitisnotknown
howeachprofessionalputssuchknowledgeintopractice. The aim of this study was to compare the perception ofphysiciansworkinginuniversityneonatalintensivecare units(NICUs)regardingthepainfulproceduresandthe anal-gesia versus the use of analgesics for potentially painful procedures performed in critically ill newborns in these units,inthreedifferenttimesoveraten-yearperiod.
Methods
This was a multicenter observational study consisting of threeprospectivecohortsofallnewbornsadmittedtofour university NICUs and the neonatologists working in these unitswithintheperiodofOctober1stto31stoftheyears 2001,2006,and2011.Thechoiceofmonthandtheyear2001 wasfor convenience, and the repetition every five years wasconsideredbecausecloseto100%ofmedicalknowledge isrenewed every tenyears,with an obsolescence rateof medicaljournalsofabout50%everyfiveyears.
The following neonatalunits wereassessed: Faculdade deCiênciasMédicasdaSantaCasadeSãoPaulo, Universi-dadeEstadualdeCampinas,UniversidadeEstadualPaulista Júliode Mesquita Filho, and Universidade Federal de São Paulo---Escola Paulista de Medicina. The research protocol wasapproved by the Research Ethics Committee of each institution.Theneedforinformedconsentfromnewborns’ familymembers waswaived. Each participating physician signedaninformedconsentform.
Allneonates admittedtothefourunits wereincluded, according tothe criteriaof the intensive care of each of them.Inordertoanswerthepainperceptionquestionnaire, theinclusioncriterionwastobeaphysicianatoneofthe participatingunits,withpowertomakeclinical decisions. Residentsfromthe pediatricsandneonatology units were notincluded.
The head of the neonatal intensive care unit of each institutionfilledoutaquestionnairewithinformationabout thegeneralcharacteristicsoftheunit,presenceofroutine assessment,treatment,andeducationonpainandanalgesia intheneonatalperiod.
Datacollectionofthehospitalizednewbornswascarried outbya neonatologist ofeach institution. Information on thetotalnumberofpatientsandpatient-daysineachunit wereobtained.Theperformedpainfulprocedureswere reg-isteredinamedicalfileatthebedside,filledbydoctorsand nurseswhocared for thepatients. Forthe present study, the following procedures were considered: lumbar punc-ture,tracheal intubation,time ofmechanical ventilation,
and postoperative period.The same team of researchers collecteddatainthethreestudyperiods.
To evaluate the use of analgesics in newborns in the threeperiodsofthestudy,thefollowingdatawereanalyzed: patient-daysonanalgesia(sumofallpatientswhoreceived at leastone doseof analgesic for eachday ofthe study); numberoflumbarpunctureandtrachealintubation proce-duresunderanalgesiaforeachdayoftheevaluatedmonth andyear;postoperativeperiodunderanalgesia(itwas veri-fied,ateachdayofthestudy,whichpatientswerereceiving any dose of analgesia on the three first days after some surgical procedure),and ventilation-days(sumof patients undergoingmechanicalventilationineverydayofthestudy, whetherunderanalgesiaornot).
Allphysicianswhoworkedattheuniversityneonatalunits answeredan anonymousquestionnaire,which consistedof personalcharacteristics, knowledge regardingpain assess-ment, and personal opinion about the aspects related to pain in invasive procedures.In this regard, the physician wasaskedregardingwhethernewbornsfeelpainduring lum-bar puncture, intubation, mechanical ventilation, and in the postoperativeperiodof minor(inguinal hernia repair) andmajor(laparotomy)surgeries. Ifthe answerwas posi-tive,theprofessionalwasaskedtostatehowmuchpainhe thoughtthenewbornfeltineach procedureusinga10-cm horizontalvisual analogicscale(VAS).Suchascale ranged fromnopain(zero)toseverepain(10cm);painwas consid-eredtobepresentwhenthemarkeddistancewasgreater than3.0cm.10Eachphysicianwasalsoaskedwhetherhe/she
thoughtitwasadequatetoprescribeanalgesiafortheabove procedures;theonlypossibleanswerswereyesorno.
Data were compared in the three study periods by descriptiveanalysis,usingPearson’spartitioningchi-squared testforcategoricalvariables,orFisher’sexacttest.Forthe quantitativevariables,comparisonwasmadebyanalysisof variancewithTukey’sposthoctest.Asallpatientsadmitted tothefourunitsandallphysiciansfromeachoftheunitsin threeperiodsofthestudywereanalyzed,thesamplepost hocpowerwasverifiedonlyforthenumberofpainful pro-ceduresperformedunderanalgesia.TheSPSSsoftwarefor Windows,version19(StatisticalPackageforSocialSciences, Chicago,IL,USA)wasusedforthestatisticalanalysis.
Results
The characteristics of the four units in the three study periods areshown inTable 1.Allof them werereference units for high-risk pregnancies and included residents in Pediatrics and Neonatology. Regarding teaching on pain and analgesia in the neonatal period, only one institu-tionreportedhavingaformaltheoreticalprogramin2001, althoughtheheadsoftheNICUsreportedhavingdiscussed painandanalgesiaatbedsideinallunits.In2006and2011, allunitsreportedtheoreticallecturesandpractical discuss-ionsonthetopic.
Table1 Characteristicsoftheunitsregardingthetotalnumberofbeds,physicalarea,monthlymeannumberofbirthsand admissions,personnelinvolvedeverydayinneonatalcareintheneonatalICUs(numberofundergraduatestudents,residentsin pediatricsandneonatology,graduatestudents,anddoctors),educationregardingpainandanalgesiaintheneonatalperiod.
InstitutionA InstitutionB InstitutionC InstitutionD
2001 2006 2011 2001 2006 2011 2001 2006 2011 2001 2006 2011
Birth/month 300 300 300 100 95 95 120 120 170 270 200 200
Totalofavailablebeds 60 59 59 37 29 29 44 66 56 59 50 50
NeonatalICUbed 12 15 15 11 8 8 15 17 17 6 18 18
NeonatalICUarea(m2) 240 500 500 96 96 96 600 700 650 120 180 180
ICUadmissions/month 50---60 50---60 50---60 20---30 20---30 20 30 30 30 20 20 20
PhysiciansinICU/shift 3 2 2 1 1 1 4 6 4 1 2 2
Postgraduatestudentin
ICU/shift
0 0 0 2 2 2 0 0 0 0 0 0
RinneonatologyinICU/shift 2 1 1 4 4 4 2---4 4 3 1 4 4
RinpediatricsinICU/shift 2 1 1 1 1 1 1 1---2 1 2 2 2
Undergraduatestudentin
ICU/shift
1 1 1 0 0 0 1 1 0 1 1 1
Educationrelatedtopain
-Theoreticallectures No Yes Yes Yes Yes Yes No Yes Yes No Yes Yes
-Duration(hours) - 1 1 6 6 6 - 1 2 - 2 2
-Annualfrequency - 4 4 2 2 2 - 1 1 - 1 1
-Discussionsatthebedside Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
ICU,intensivecareunit;R,residents.
in 2006,andin 2011, 125newborns totaled1366 patient-days. As for the four assessed painful situations (lumbar puncture,trachealintubation,mechanicalventilation,and thefirstthreepostoperativedays),therewasanincreaseof analgesic usein 2006when comparedwith2001.In2011,
compared with 2006, there was a reduction of analgesia prescribedtopatientsreceivingmechanicalventilationand lumbarpuncture andtherewerenomodifications for tra-cheal intubation. As for the postoperative period (three days),therewasasignificantandprogressiveincreaseinthe
Table2 Clinicalcharacteristicsofnewbornsassessedinthefourneonatalintensivecareunitsforamonth,withafive-year
interval.
2001(n=91) 2006(n=114) 2011(n=125) p
Birthweight(g) 0.347a
Mean±SD 1889±879 2058±977 1915±909
Median 1880 1920 1740
Range 590---4090 590---4255 574---3975
Weightatstudyentry(g) 0.426a
Mean±SD 1985±1016 2145±966 2010±945
Median(range) 1925 1987 1800
Range 590---6700 495---4445 575---4060
Daysoflifeattheenrollment 0.862b
Mean±SD 15±30 12±23 14±31
Median 1 1 1
Range 0---218 1---152 1---224
Malegender 50(56%) 67(59%) 65(52%) 0.568c
Morbidities
Respiratorydisease,n(%) 47(52%) 46(40%) 68(54%) 0.077c
Infection,n(%) 33(36%) 31(27%) 30(24%) 0.133c
Cardiovasculardisease,n(%) 13(15%) 07(06%) 22(18%) 0.025c
Malformation,n(%) 20(22%) 24(21%) 25(20%) 0.939c
Death,n(%) 16(18%) 08(07%) 09(07%) 0.018c
a ANOVAwithfixedfactor. b Kruskal---Wallis.
Table3 Numberofpatient-days,patient-daysundergoingpainfulprocedures,andpatient-daysthatwereunderanalgesiain thefourneonatalintensivecareunitsintheassessedyears.
2001(n=91) 2006(n=114) 2011(n=125) p-Value Samplepower
Patient-days
Number 1025 1112 1366
Patient-daysunderanalgesia 255(25%) 312(28%) 294(22%) 0.002a 0.887
Lumbarpuncture(LP)
Lumbarpunctures 34 51 45
LPunderanalgesia 4(12%) 22(43%) 16(36%) 0.009a 0.795
Trachealintubation(TI)
Trachealintubations 109 62 74
TIunderanalgesia 28(26%) 20(32%) 24(32%) 0.523a 0.159
Mechanicalventilation(MV)
PatientsinMV 440 362 376
Ventilated-days/patient-days 43% 33% 27%
MVunderanalgesia 200(45%) 233(64%) 180(48%) <0.001a 0.999
Threedayspostoperatively(PO)
NBsubmittedtosurgery 18 14 36
Patient-daysuptothirdPO 16 45 55
POunderanalgesia 6(37%) 35(78%) 49(89%) <0.001a 0.980
aPearson’sChi-squaredtest,Fisher’sexacttestoritsextension.
useofanalgesiaovertheyears(Table3).Foralltheanalyzed situations,thesamplepowerwasgreaterthan80%,except fortrachealintubationunderanalgesia.
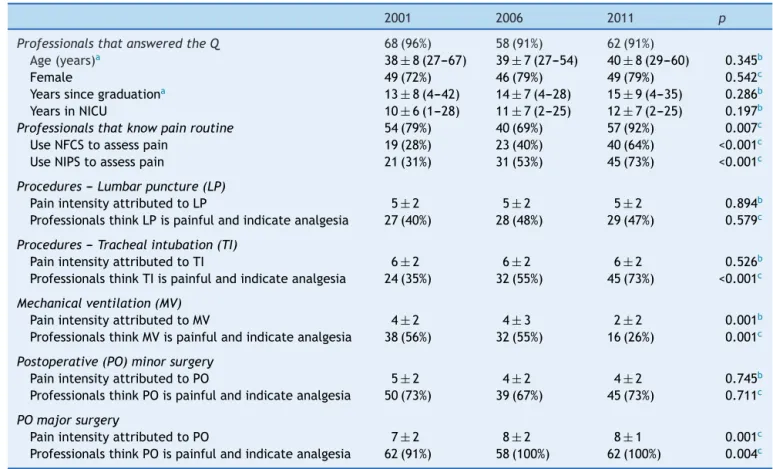
Regardingthe medicalopinion, 68(96%)neonatologists answeredthequestionnairein2001,58(91%)in2006,and62 (91%)in2011.Therewasnosignificantdifferenceregarding the demographicdata of the professionals in these three periods(Table4).Overtime,therewasanincreaseinthe numberofprofessionalswhostatedtheyknewtheunitpain routineandusedtheNeonatalFacialCodingSystem(NFCS) and/orNeonatalInfantPainScale(NIPS)painscales.
Asfor theintensity ofpainattributedtopainful proce-dures,therewasnodifferencebetween thethreeperiods forlumbarpunctureandintubation.Therewasareduction intheintensityofpainattributedtomechanicalventilation between2001/2006and2011andtheoppositeoccurredfor majorsurgery(Table4).
Regardingthe practiceofanalgesiain thethree evalu-ated periods,only 12% of lumbar puncturesin 2001 were performed under adequate analgesia for the procedure. After five years (2006), there wasan increase in analge-sia indicationin the units, witha slight decreasein 2011 (Table 3). In the three studied periods, 40---50% of physi-ciansthoughtthatthepaincausedbylumbarpuncturewas atleastmoderate(VAS>3)andstatedthatintheory, they indicatedtheanalgesiafortheprocedure(Table4).
Regarding tracheal intubation, nearly 30% of the pro-cedureswere performed underanalgesia in threeperiods ofthestudy (Table3).Ofthe respondents,35%,55%,and 73% in 2001, 2006, and 2011, respectively, reported VAS >3andstatedtheyusedanalgesicsfortrachealintubation (p<0.001;Table4).
For patients on mechanical ventilation, 45% of
ventilated-dayswereunderanalgesiain2001,64%in2006, and 48% in 2011 (p<0.001; Table 3). For this situation,
there was a significant decrease in neonatologists that reported VAS >3 and stated they used analgesia between 2001---2006and2011(p=0.002;Table4).
Finally,inthefirstthreepostoperativedays,37%, 78%, and89%ofpatientsreceivedanalgesicsrespectivelyin2001, 2006, and 2011 (p=0.013; Table 3). Regarding the physi-cians, for a smallsurgery, 73% in 2001, 67% in 2006, and 73% in 2011, considered the postoperativepain moderate to severe and said they prescribed analgesics (p<0.001;
Table 4). For major surgeries, 91% in 2001, and 100% in 2006 and 2011 considered the postoperative pain moder-atetosevereandsaidtheyprescribedanalgesics(p<0.001;
Table4).
Discussion
The present study demonstrated, for almost all analyzed painful situations,adistance between theneonatologists’ theoreticalattitudeandtherealpracticeinneonatalunits, although there has been an increase in the awareness aboutthepresenceofpainincriticallyillnewbornsmainly between2001and2006,accompaniedbymorefrequentuse of analgesics in clinical practice for some of the painful procedures.Thestudyfindingsconfirmtheliterature3,4and
indicatethatcriticallyillnewbornsaresubmittedtoseveral potentiallypainfulprocedures,andthattheirmanagement remainsinadequate.Themostfrequentperceptionofpain byprofessionalsandthegreateruseofanalgesiaforpainful procedures in clinical practice between 2001 and 2006 appeartoreflecttheknowledgeimprovementinthisarea.11
Table4 Characteristicsofprofessionalsworkinginfourunitsassessedtogether,theirknowledgeofthepainroutineintheir unitsandtheiropinionsaboutthepotentiallypainfulprocedures(lumbarpuncture,intubation,mechanicalventilation, and minorandmajorpostoperative).
2001 2006 2011 p
ProfessionalsthatansweredtheQ 68(96%) 58(91%) 62(91%)
Age(years)a 38±8(27---67) 39±7(27---54) 40±8(29---60) 0.345b
Female 49(72%) 46(79%) 49(79%) 0.542c
Yearssincegraduationa 13±8(4---42) 14±7(4---28) 15±9(4---35) 0.286b
YearsinNICU 10±6(1---28) 11±7(2---25) 12±7(2---25) 0.197b
Professionalsthatknowpainroutine 54(79%) 40(69%) 57(92%) 0.007c
UseNFCStoassesspain 19(28%) 23(40%) 40(64%) <0.001c
UseNIPStoassesspain 21(31%) 31(53%) 45(73%) <0.001c
Procedures---Lumbarpuncture(LP)
PainintensityattributedtoLP 5±2 5±2 5±2 0.894b
ProfessionalsthinkLPispainfulandindicateanalgesia 27(40%) 28(48%) 29(47%) 0.579c
Procedures---Trachealintubation(TI)
PainintensityattributedtoTI 6±2 6±2 6±2 0.526b
ProfessionalsthinkTIispainfulandindicateanalgesia 24(35%) 32(55%) 45(73%) <0.001c
Mechanicalventilation(MV)
PainintensityattributedtoMV 4±2 4±3 2±2 0.001b
ProfessionalsthinkMVispainfulandindicateanalgesia 38(56%) 32(55%) 16(26%) 0.001c
Postoperative(PO)minorsurgery
PainintensityattributedtoPO 5±2 4±2 4±2 0.745b
ProfessionalsthinkPOispainfulandindicateanalgesia 50(73%) 39(67%) 45(73%) 0.711c
POmajorsurgery
PainintensityattributedtoPO 7±2 8±2 8±1 0.001c
ProfessionalsthinkPOispainfulandindicateanalgesia 62(91%) 58(100%) 62(100%) 0.004c
Q,questionnaire;NICU,neonatalintensivecareunit;NFCS,neonatalfacialcodingsystem;NIPS,neonatalinfantpainscale.
a Mean±standarddeviation(range). b ANOVAwithfixedfactor.
c Pearson’sChi-squaredtest,Fisher’sexacttest,oritsextension.
period,seem to bedue to thepublication of undesirable effectsofanalgesicsintheneonatalperiod.12,13
The procedures analyzed here were chosen as they are part of the daily routine of a NICU and also because they cause pain, according to consolidated data in the literature14---18; in addition, there are published protocols
for drug analgesia in these procedures.11,18---21 Regarding
tracheal intubation, Bonow et al.,22 in 2004, evaluated
297proceduresintwoneonatalintensivecareandtwo pedi-atric units for six months. Medications for sedation and analgesia were used in 89% of intubations performed in the Pediatric ICU, and 24% of those in the NICU. In the same year, Simon et al.23 analyzed the use of
premedi-cation for intubation in 75 French pediatric and neonatal unitsandshowedthat37%ofnewborns,67%ofinfants,and 92%ofolderchildrenreceivedanalgesicsand/orsedatives prior to the procedure. The evidence-basedinternational consensus11concludedthattrachealintubationwithoutthe
useofanalgesiaandsedationshouldbeperformedonlyin neonatal resuscitation in the delivery room or in urgency situations without available venous access; in 2010, the AmericanAcademyofPediatrics19recommendedtheuseof
premedication for trachealintubation inneonates. In this study,itwasobservedthat,evenwithprogressiveincrease ofthephysician’sperceptionthatintubationcausespain,a
significantpercentageofpatientswerestillintubated with-outanypain relief.Oneexplanationfor this wouldbe its performanceinemergencysituations;however,outsidethe deliveryroom,suchsituationsarerareand,inmostcases, itispossiblethat,whileaprofessionalpreparesthe mate-rialforintubation,theothermanagestheanalgesics.24The
beneficialeffectsofsedationandanalgesiaonintracranial pressure,airwayinjury,reduction ofprocedure time,and patientcomfortshouldbeconsidered.25
Asforlumbarpuncture,alocalinfiltrationoflidocainein neonatesis recommended.21 SabrineandSinha26 observed
theregular use of analgesics for lumbar puncture in only 9%ofthesurveyedEnglishNICU.Porteretal.27 studied140
lumbarpunctures,andonlyin4%specificanalgesic medica-tionwasprescribedfor theprocedure.Inthisstudy,inall years,lessthanhalfof thenewborns submittedtolumbar puncture received some type of analgesic for the proce-dure.Thisfindingistroublingwhencomparedtowhatoccurs inchildren andadults,in whomtheuse of local anesthe-siafor thepuncture is usual.28 It isnoteworthy that over
50%ofinterviewedphysiciansfeltthatthepaincausedby thelumbarpuncturewouldnotbeintenseenoughtojustify analgesia.
worseneurologicaloutcomeinpreterminfantson mechani-calventilationwhoreceivedmorphinewithinthefirsthours oflife,forapproximately14days,withassociationbetween this unfavorable outcome and the presence of hypoten-sionpriortoopioidinfusion.12,13 Ameta-analysis29 didnot
showsufficientevidencetorecommendtheroutineuseof opioidsfornewbornsonmechanicalventilation.The incor-porationofthisknowledgeprobablyexplainsthehuge dis-crepancy of data between perception and practice of neonatologistsregardingpainandanalgesiaformechanical ventilationin 2011. It shouldbe notedthat, inthat year, neonatologistsattributedlesspaintomechanicalventilation thaninthepreviousyearsandstatedtheyindicated analge-sialessfrequently.However,inpractice,althoughtheuse ofanalgesia for ventilatedpatients hasdecreased, it was muchhigherthantheneonatologists’theoreticalintention touseit.
Finally, regarding the postoperative period, it wasthe undertreatment of pain in neonates undergoing surgical procedures that triggered the interest of the scientific communityonthesubject.30Thereisnodoubtthat
postop-erativepainincreasesneonatalmorbidityandmortality.31,32
Thepresentstudydemonstratedthatmedicalknowledgein thisregard hasimproved; in2006 and2011, all neonatol-ogistsconsideredthepostoperativeperiodapainfulevent andstatedtheyprescribedanalgesia.Theclinicalpractice, however, can be analyzed fromtwo points of view:one, optimistic,observingthatthepostoperativeuseofanalgesia increasedfrom33%in2001to89%in2011,bringingthe theo-reticalknowledgeofneonatologistsclosertotheirpractice. Underthe pessimisticviewpoint,it canbe observedthat, althoughalltheneonatologistsfeelthatpostoperative new-bornsneedanalgesics,over10%ofhospitalizedpatientsin thefouruniversityunitsin2011didnotreceiveanyanalgesic doseinthefirstthreedayspostoperatively.Medical knowl-edge,especiallywithregardtotherapeuticproceduresand medicalposture,dependsmoreonwhatstudentsinferbased ontheperformanceoftheirmentors,thanonthe transmis-sionof theirtheoreticalknowledge.33 Inthis context,the
gapbetweenmedicalknowledgeandpracticeinuniversity hospitals,whereappropriateandupdatedtrainingofhuman resourcesisasmuchapriorityasthehighstandardcareto theirpatients,isofconcern.
Itis noteworthythat,tounderstand thepresent study, itisnecessarytocriticallyreviewitsmajorlimitation:the research compared neonatologists’ perceptions about thepresence,intensity,andneedtotreatpaintriggeredby procedures,withthefrequencyofanalgesicuseinnewborns undergoingsuchprocedures,anditwasnotpossibleto indi-viduallypointoutthediscrepancybetweenthetheoretical knowledge and practical performance of each responding healthcareprofessional.Thestudywaslimitedtoanalyzing the prescription of pharmacological analgesia, regardless ofnonpharmacologicalmeasures,whichcouldhelprelieve paininseveral procedures.Finally, whenconsidering only a month of each assessed year, the survey had limited statistical power to detect differences in the practice of analgesiafortrachealintubation.Nevertheless,thescenario shown here indicates the need to improvethe models of continuingeducationregarding neonatalpain,sothatthe universityneonatalunitshaveprofessionalsthatcanapply theirknowledgeatthebedsideandmodifysuchknowledge
inaccordancewiththedynamicacquisitionofinformation thatisbuiltfromthecriticalreadingofscientificliterature onthesubject.
Itcanbeconcludedthat,overaten-yearperiod,there was an increase in the use of analgesics for the assessed painful procedures andan increasedperception by physi-ciansthatnewbornsfeelpain.Thegapbetweentheactual use of analgesicsin clinical practice andmedical percep-tionabouttheneedforanalgesiaduringpainfulprocedures persistedinthefourassessedintensivecareunits.Itis essen-tialtoanalyzethefactorsthatinterfereinmedicalpractice anddevelopstrategiestotreatpainassociatedwithinvasive proceduresintheneonatalperiod.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.SimonsSH, vanDijk M, Anand KS,Roofthooft D,van Lingen RA,TibboelD.Dowestillhurtnewbornbabies?Aprospective studyofproceduralpainandanalgesiainneonates.ArchPediatr AdolescMed.2003;157:1058---64.
2.PrestesAC,GuinsburgR,BaldaRC,MarbaST,RugoloLM,Pachi PR, et al. The frequency of pharmacological pain relief in university neonatal intensive care units. J Pediatr (Rio J). 2005;81:405---10.
3.CarbajalR,RoussetA,DananC,CoqueryS,NolentP,Ducrocq S,etal.Epidemiologyandtreatmentofpainfulproceduresin neonatesinintensivecareunits.JAMA.2008;300:60---70. 4.CignaccoE,HamersJ,vanLingenRA,StoffelL,BuchiS,Muller
R,etal.Neonatalproceduralpainexposureandpain manage-mentinventilatedpreterminfantsduringthefirst14daysof life.SwissMedWkly.2009;139:226---32.
5.LagoP,Garetti E,Bocuzzo G, MerazziD, PirelliA, Pieragos-tiniL,etal.Proceduralpaininneonates:theestateoftheart intheimplementationofnationalguidelinesinItaly.Paediatr Anaesth.2013;23:407---8.
6.StevensBJ,FranckLS.Assessmentandmanagementofpainin neonates.PaediatrDrugs.2001;3:539---58.
7.Abu-SaadHH,BoursGJ,StevensB,HamersJP. Assessmentof painintheneonate.SeminPerinatol.1998;22:402---16. 8.Slater R,Cantarella A, FranckL, MeekJ,FitzgeraldM. How
welldoclinicalpainassessmenttoolsreflectpainininfants? PLoSMed.2008;5:e129.
9.AkumaAO,JordanS.Painmanagementinneonates:asurveyof nursesanddoctors.JAdvNurs.2012;68:1288---301.
10.VanDijkM,KootHM,SaadHH,TibboelD,PasschierJ. Observa-tionalvisualanalogscaleinpediatricpainassessment:useful toolorgoodriddance?ClinJPain.2002;18:310---6.
11.Anand KJ. International evidence-based group for neonatal pain. Consensus statement for the prevention and manage-ment of pain in the newborn. Arch Pediatr Adolesc Med. 2001;155:173---80.
12.AnandKJ,HallRW,DesaiN,ShephardB,Bergqvist LL,Young TE,etal.Effectsofmorphineanalgesiainventilatedpreterm neonates: primary outcomes from the NEOPAIN randomised trial.Lancet.2004;363:1673---82.
13.HallRW,KrinsbergSS,BartonBA,KaiserJR,AnandKJ,NEOPAIN Trial Investigators Group.Morphine hypotension and adverse outcomesamongpretermneonates:who’stoblame?Secondary resultsfromtheNEOPAINtrial.Pediatrics.2005;115:1351---9. 14.MatherL,MackieJ.Theincidenceofpostoperativepainin
15.BaxterAL,Welch JC,Burke BL, IsaacmanDJ. Pain,position, and stylet styles: infant lumbarpuncture practices of pedi-atric emergency attending physicians. Pediatr Emerg Care. 2004;20:816---20.
16.AnandKJ,HansenDD,HickeyPR. Hormonal-metabolicstress responsesinneonatesundergoingcardiacsurgery. Anesthesiol-ogy.1990;73:661---70.
17.GuinsburgR, KopelmanBI, Anand KJ,Almeida MF,PeresCA, MiyoshiMH.Physiological,hormonalandbehavioralresponses toasinglefentanyldoseinintubatedandventilatedpreterm neonates.JPediatr.1998;132:954---9.
18.WalkerSM.Neonatalpain.PaediatrAnaesth.2014;24:39---48. 19.AmericanAcademyofPediatrics.Clinicalreport:premedication
for nonemergency endotracheal intubation in the neonate. Pediatrics.2010;125:608---15.
20.DurrmeyerX,Vutskits L, AnandKJ,RimensbergerPC. Useof analgesicandsedativedrugsintheNICU:integratingclinical trialsandlaboratorydata.PediatrRes.2010;67:117---27. 21.AmericanAcademyofPediatrics,CommitteeonFetusand
New-bornand SectiononSurgery,CanadianPaediatricSocietyand FetusandNewbornCommittee.Preventionandmanagementof painintheneonate:anupdate.Pediatrics.2006;118:2231---41. 22.BonowFP, Piva JP, GarciaPC, Eckert GU. Avaliac¸ão do pro-cedimentode intubac¸ãotraquealem unidades dereferência deterapiaintensivapediátricaseneonatais.JPediatr(RioJ). 2004;80:355---62.
23.SimonL,Trifa M,MokhtariM,Hamza J,TreluyerJM. Preme-dication for tracheal intubation: a prospective survey in 75 neonatal and pediatric intensive care units. Crit Care Med. 2004;32:565---8.
24.KelleherJ,MallyaP,WyllieJ.Premedicationbeforeintubation inUKneonatalunits:adecadeofchange?ArchDisChildFetal NeonatalEd.2009;94:332---5.
25.AllenKA.Premedicationforneonatalintubation:which med-ications are recommended and why. Adv Neonatal Care. 2012;12:107---11.
26.Sabrine N, Sinha S. Pain in neonates. Lancet. 2000;355: 932---3.
27.PorterFL,MillerPJ,ColeFS,MarshallRE.Controlledclinical trialoflocalanesthesiaforlumbarpuncturesinnewborn. Pedi-atrics.1991;88:663---9.
28.HayesJA,LopezAV,PehoraCM,RobertsonJM,AblaO, Craw-ford MW. Coadministration of propofol and remifentanil for lumbar puncture in children dose---response and an evalu-ation of two dose combinations. Anesthesiology. 2008;109: 613---8.
29.BelluR,deWaalKA,ZaniniR.Opioidsforneonatesreceiving mechanicalventilation.CDSRev.2008:CD004212.
30.AnandKJ, Aynsley-Green A.Metabolic andendocrine effects of surgical ligation of patent ductus arteriosus in the human preterm neonate: are there implications for further improvement ofpostoperative outcome?Mod Probl Paediatr. 1985;23:143---57.
31.BouwmeesterNJ,AnandKJ,vanDijkM,HopWC,BoomsmaF, TibboelD.Hormonalandmetabolicstressresponsesaftermajor surgeryinchildrenaged0---3years:adouble-blind,randomized trialcomparingtheeffects ofcontinuousversus intermittent morphine.BrJAnaesth.2001;87:390---9.
32.SimonsSH,vanDijkM,vanLingenRA,RoofthooftD,Boomsma F,vandenAnkerJN,etal.Randomisedcontrolledtrial evalu-atingeffectsofmorphineonplasmaadrenaline/noradrenaline concentrationsinnewborns.ArchDisChildFetalNeonatalEd. 2005;90:F36---40.