Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
www.revportcardiol.org
ORIGINAL
ARTICLE
Alcohol
septal
ablation
in
obstructive
hypertrophic
cardiomyopathy:
Four
years
of
experience
at
a
reference
center
夽
António
Fiarresga
∗,
Duarte
Cacela,
Ana
Galrinho,
Ruben
Ramos,
Lídia
de
Sousa,
Luís
Bernardes,
Lino
Patrício,
Rui
Cruz
Ferreira
Servic¸odeCardiologia,HospitaldeSantaMarta,CentroHospitalardeLisboaCentral,EPE,Lisboa,Portugal
Received13March2013;accepted25April2013 Availableonline11February2014
KEYWORDS Obstructive hypertrophic cardiomyopathy; Percutaneous treatment; Alcoholseptal ablation Abstract
Introduction:We describeourcenter’sinitial experiencewith alcoholseptalablation(ASA) forthetreatmentofobstructivehypertrophiccardiomyopathy.Theprocedure,itsindications, resultsandclinicaloutcomeswillbeaddressed,aswillitscurrentpositioncomparedtosurgical myectomy.
Objective: ToassesstheresultsofASAinallpatientstreatedinthefirstfouryearsofactivity atourcenter.
Methods:WeretrospectivelystudiedallconsecutiveandunselectedpatientstreatedbyASA betweenJanuary2009andFebruary2013.
Results:Inthefirstfouryearsofexperience40patientsweretreatedinourcenter.Inthree patients(7.5%)theinterventionwasrepeated.Proceduralsuccesswas84%.Minorcomplications occurredin7.5%.Twopatientsreceivedapermanentpacemakerforatrioventricularblock(6% ofthosewithoutpreviouspacemaker).Themajorcomplicationratewas5%.Therewere no in-hospitaldeaths;duringclinicalfollow-up(22±14months)cardiovascularmortalitywas2.5% andoverallmortalitywas5%.
DiscussionandConclusion: Theresultspresentedreflecttheinitialexperienceofourcenter with ASA. The success rate was high and inline with published results,but with room to improve with betterpatient selection.ASA was shownto besafe, withalow complication rateandnoprocedure-relatedmortality.OurexperienceconfirmsASAasapercutaneous alter-nativetomyectomyforthetreatmentofsymptomaticpatientswithobstructivehypertrophic cardiomyopathyrefractorytomedicaltreatment.
© 2013 Sociedade Portuguesa de Cardiologia Published by Elsevier España, S.L. All rights reserved.
夽 Pleasecitethisarticleas:FiarresgaA,CacelaD,GalrinhoA,etal.Ablac¸ãoseptalalcoólicanotratamentodacardiomiopatiahipertrófica obstrutivaexperiênciadequatroanosdeumcentro.RevPortCardiol.2014;33:1---10.
∗Correspondingauthor.
E-mailaddresses:antoniojosefi[email protected],a.fi[email protected](A.Fiarresga).
PALAVRAS-CHAVE Cardiomiopatia hipertrófica obstrutiva; Tratamento percutâneo; Ablac¸ãoseptal alcoólica
Ablac¸ãoseptalalcoólicanotratamentodacardiomiopatiahipertróficaobstrutiva
experiênciadequatroanosdeumcentro
Resumo
Introduc¸ão:Aablac¸ãoseptalalcoólica(ASA)éaformapercutâneadetratamentoinvasivoda cardiomiopatiahipertróficaobstrutiva(CMHO).Apropósitodadescric¸ãodaexperiêncianonosso centro,procurar-se-áreverasindicac¸ões,osaspetostécnicosepráticoseosresultadosdaASA, assimcomoasuaposic¸ãoatualemcomparac¸ãocomamiectomiacirúrgica.
Objetivo:Avaliar os resultados da ASA numa série de doentes consecutivos tratados nos primeirosquatroanosdeatividade.
Métodos: Estudoretrospetivodetodososdoentes,consecutivosenãoselecionados,comCMHO, tratadosporASA,entrejaneirode2009efevereirode2013.
Resultados: Durante o período de quatro anos foram tratados com ASA 40 doentes. Em três doentes (7,5%) repetiu-se o procedimento. A taxa de sucesso foi de 84%. A taxa de complicac¸õesminorfoide7,5%.Foinecessárioimplantarpacemakerdefinitivopor bloqueio-auriculoventricular em dois doentes (6%, do subgrupo sem pacemaker prévio). A taxa de complicac¸õesmajorfoide5%.Nãohouvemortalidadeintra-hospitalarnestapopulac¸ão.Durante oseguimentoclínico(22±14meses)amortalidadecardiovascularfoide2,5%.Amortalidade totalfoide5%.
Discussãoeconclusão:Osresultadosapresentadosrefletemaexperiênciainicialdotratamento comASAnonossocentro.Oprocedimentofoibem-sucedidonamaioriadosdoentes,sendo ataxade sucesso semelhanteàdescritaem outras séries,mas ainda compossibilidadede beneficiardeumamelhorselec¸ãodosdoentes.Aintervenc¸ãotambémserevelousegura,com umabaixaocorrênciadecomplicac¸õesesemmortalidadeassociada.AASAéumaalternativa percutâneanotratamentoinvasivodosdoentescomCMHOrefratáriaàterapêuticamédica. © 2013 SociedadePortuguesa de Cardiologia. Publicado por Elsevier España, S.L.Todos os direitosreservados.
Introduction
Hypertrophiccardiomyopathy(HCM)wasfirstdescribedover 50yearsago,1anditwassoonclearthatoneofitsmost
char-acteristicfeatureswasthepresence ofdynamic subaortic obstructioninasignificantnumberofpatients.2
Thegeneticandphenotypicheterogeneityofthisprimary cardiomyopathycomplicatesclinicalassessmentand treat-ment,andhasgivenrisetoconsiderabledebate.3Oneofthe
morerecent controversies concernsinvasive treatment of obstructivehypertrophiccardiomyopathy(OHCM);the intro-ductionofpercutaneousalcoholseptalablation(ASA)asan alternativetotheestablishedsurgical techniqueof septal myectomyled tomuch discussionconcerning the relative meritsofthetwotreatmentsthatcontinuestothisday.
MostpatientswithHCMpresentsignificant intraventric-ular obstruction at rest or with provocation, usually the Valsalvamaneuver(or,strictlyspeaking,theeffortrequired forthemaneuver).4This obstructionis causedby the
sys-tolic anteriormotion (SAM) of the anterior leaflet of the mitralvalve, which results from the force of left ventri-cular (LV) ejection and the narrowing of the LV outflow tract (LVOT); elongation of the mitral valve leaflets may alsocontribute in some cases.5 The obstruction increases
intracardiac pressure, oxygen consumption and cardiac work,andisalsooftenassociatedwithmitralregurgitation, coronaryflowabnormalitiesanddiastolicdysfunction.The degreeofobstructioncorrelateswithsymptomseverityand worsesurvival.6
Identification of patients with OHCM is important, because the obstruction is itself a therapeutic target;
reducingitfrequentlyresultsinimprovementorcomplete resolution of symptoms. Medical therapy is effective in most cases and should therefore be the first-line treat-ment, using inotropic depressors such as beta-blockers, non-dihydropyridine calciumchannel blockersor disopyra-mide(thelatterunavailableinPortugal).
However,in 5---10% ofpatients medicaltherapy is inef-fective,nottoleratedorcontraindicated.7Insuchcases,an
invasiveapproachisanalternativeforsymptomaticpatients withimpairedqualityoflife.Theaimistoreducethe thick-nessofthebasalportionoftheinterventricularseptumand hencetheobstruction.Thefirsttechniqueusedwassurgical myectomy,inwhichapartoftheseptalmuscleisexcised; thiswasthe onlyoption for decades.Inexperienced cen-ters,mortalityis≤2%inyoungpatientswithoutsignificant comorbidities.8Itisnotconsideredaneasyprocedure,since
thesurgeonfacesconsiderablevariationinthemorphology of the LVOT with limited transaortic access. However, in centerswithdecadesofexperiencethathavetreated hun-dredsofcasestheprocedureishighlyeffective,significantly reducinggradientsandsymptomsin90---95%ofpatients.7
The need for another therapeutic option for patients withcontraindicationorhighriskforsurgerypromptedthe developmentofapercutaneousalternative.ASAconsistsof injectionofalcoholintoacoronaryarteryinordertocause limitedmyocardialnecrosisinthebasalseptum,whichwhen healed reduces septal thickness and hence the subaortic gradient. The technique has been the subject of contro-versysinceitsintroduction,butitsresultsaresuchthatit has become a viable alternative to surgical treatment of patientswithOHCM.
Objective
The aimof thisstudyis toassessthe resultsofASA in all patientstreatedinthefirstfouryearsofactivityatasingle cardiologicalreferencecenter.
Methods
Weperformedaretrospectivestudybasedondatacollected prospectively of all consecutive and unselected patients withOHCMandindicationforaninvasiveapproach,treated byASA between thebeginningof activityin January2009 andFebruary2013.
Demographic variables, clinical indications, minor and majorcomplications,proceduralsuccessandlong-term out-come wereassessed.Success wasdefinedassymptomatic improvement (reduction of at least one New York Heart Association[NYHA]orCanadianCardiacSociety[CCS]class) together witha reduction of over 50% in subaortic gradi-entsatrestorwithprovocation.3Majorcomplicationswere
consideredtobethosethatresultedindeathorsignificant morbidityorwerelife-threateningduringtheprocedureor follow-up.
Categorical variables arepresented ascounts and per-centages, and continuous variables as means ± standard deviation.ThestatisticalanalysiswasperformedusingSPSS version20.
Results
Duringthefour-yearstudyperiod,43patientswith indica-tionfor invasivetreatmentwere assessed,threeof whom wereexcludedbecauseatargetvesselwaslackingor per-fusedremotemyocardialsegments.Atotalof43procedures wereperformedin40patients.Themaincharacteristicsof thestudypopulationarepresentedinTable1.
The most frequent indication was exertional dyspnea; onepatient(2.5%)wasinNYHAclassIVandinanother(2.5%) thesoleindicationwasexertionalangina.Sixpatients(15%) hadapreviouslyimplantedpacemaker,onewithaDDD pace-makerimplantedprior totheintervention duetoexisting left bundle branch block, which put her at high risk for completeatrioventricularblock(AVB)followingthe proce-dure.
Mean subaortic gradient at rest was 90±34mmHg and mean septal thickness was 21.6±4 mm. Three patients (7.5%) had a resting gradient of <50 mmHg and in these casestheindicationwasduetothegradientobtainedwith provocation.Tenpatients(30%)wereconsidered notideal formyectomyduetoage,obesityorcomorbidities,andtwo (5%)wereformallyrejectedforsurgery.
Data on the intervention and in-hospital course are presented in Table 2. Alcohol was injected into a single target vessel, which was changed after intramyocardial contrast injection in four cases (10%). Two patients (6% of those without previous pacemaker) received a perma-nent pacemaker for AVB, one late, on the seventh day aftertheprocedureandafterreintroductionofbeta-blocker therapy. In four patients (10%) with AVB after 24 hours the initial approachwas conservative based on their risk score,waitingfor resolutionoftheedemaassociatedwith
Table1 Baselinecharacteristicsofthe studypopulation (n=40).
Age(years) 61.5±12.7
Age≥75years 6(15)
Female 27(70)
NYHAclassIII/IV 39(97.5)
CCSclassII/III 10(25) Syncope 1(2.5) Previoushistory Hypertension 26(65) Diabetes 3(7.5) Coronarydisease 4(10) Atrialfibrillation 7(17.5) LBBB 2(5)
Previouspermanentpacemaker 3(7.5)
PreviousICD 1(2.5)
Echocardiogram
Maximumseptalthickness 21.6±2.66
Gradientatrest 89.6±33.6
Gradientwithprovocation 109±30 Mitralregurgitationgrade≥2 1(2.5) Ejectionfraction<50% 0(0) Therapy
Beta-blocker 29(72.5)
Calciumchannelblocker 27(67.5)
Dualtherapy 17(43)
DDDpacemaker 2(5)
Myectomy 0(0)
Values are counts (%) or means ± standard deviation. CCS: CanadianCardiacSociety;LLLB:leftbundlebranchblock;ICD: implantable cardioverter-defibrillator; NYHA:New YorkHeart Association.
Table2 Interventionandhospitalization(n=40).
No.ofseptalarteries 43
Volumeofalcoholinjected(ml) 2.1±0.3
PeakCK(U/ml) 1130±438
AVBriskscore
Low 27(75a)
Intermediate 7(19a)
High 2(6a)
Permanentpacemaker 2(6a)
Sustainedventriculartachycardia 0(0)
Ventricularfibrillation 1(2.5)
Complicationsduringhospitalization
Major 2(2.5)
Minor 3(7.5)
In-hospitalmortality 0(0)
Valuesarecounts(%)ormeans±standarddeviation.AVB: atrio-ventricularblock;CK:creatininekinase.
Table3 Clinicalcourse(n=39).
Meanfollow-up(months) 22±14
Symptomaticimprovement Dyspnea 31(86a) Angina 9(90a) Syncope 1(100a) Reductioningradient 33(89) SuccessfulASA 31(84) Permanentpacemaker 0(0) ICD 1(2.5) RepeatASA 3(7.5) Myectomy 1(2.5) Nocardiovascularevents 31(78)
Rehospitalizationforcardiaccause 5(12.5)
Mortality
Cardiovascular 1(2.5)
Suddendeath 0(0)
Total 2(5)
Valuesarecounts(%)ormeans±standarddeviation.ASA: alco-holseptalablation;AVB:atrioventricularblock;ICD:implantable cardioverter-defibrillator.
aPercentageforpatientswiththissymptom.
thenecroticareaandre-establishmentof atrioventricular conduction,whichinsomecasesdidnotoccuruntilthefifth day.
Therateofminorcomplicationswas7.5%.Intwopatients infectionswereresolvedby antibiotictherapy,andinone patient rapid atrial fibrillation was controlled with phar-macologicaltherapy.Themajorcomplicationratewas5%, includingonepatientwithtamponadecausedbythe intro-ductionofthecatheterandresolvedbypericardiocentesis andpericardial drainage, andone withan inferior infarc-tioncausedbyrecruitmentofthecollateralsofthetarget vesseltothe posteriorinterventricular branch,leading to anepisodeofventricularfibrillationafew hoursafterthe intervention,resolvedbyshocktherapy.Allpatients under-wentHolterECG monitoringbeforedischarge;nocomplex ventriculararrhythmiasweredocumented.Therewere no in-hospitaldeaths.
Table 3 presents the data on clinical follow-up. Most patientsexperiencedsymptomaticimprovementassociated with a significant reduction in subaortic gradient. Pro-cedural success was 84%. Information on post-procedural gradient is unavailable for four patients, three because theprocedure wasperformed less than threemonthsago and one because of difficulty in repeating echocardiog-raphy due to severe neurological sequelae of a stroke. Twopatients(5%)sufferedstroke,bothmorethan30days after the intervention; four (10%) were readmitted due toparoxysmal atrial fibrillation, one of whom underwent successfulablation. Onepatient(2.5%)wasrehospitalized forimplantationofanimplantablecardioverter-defibrillator duetofaintingandnon-sustained ventriculartachycardia, both documented before ASA. Overall mortality was 5%: one patient died from probable pulmonary embolism 13 monthsafter theintervention andone diedof colon can-cer.
Discussion
SincethefirstprocedureperformedbyUlrichSigwartin1994 anddescribed,withtwoothercases,in1995,9ASAhasbeen
refinedandisnowmoreeffectiveandsafe,tothepointthat itsresultsarenowcomparabletosurgicalmyectomy.Itisno longerseen asapioneeringandpoorly-defined technique, buthasbecomeanestablishedprocedureoverthecourseof nearlytwodecades,duringwhichithasbeenusedtotreat morepatientsthansurgery.10
Patient
selection
Theindications forASAarethesameasforsurgical myec-tomy,although itisimportant tostress thatpatientswith no or mild symptoms are not indicated for any invasive treatment.7 The presence of obstruction is an
indepen-dentprognosticmarkerofprogressiontoheartfailureand mortality,6butthereiscurrentlyinsufficientevidencethat
interventionaltersprognosisinthesepatients;itsroleisto treatsymptomsthatsignificantlyaffectpatients’qualityof life.
Selectedpatientsshouldhaveexertionaldyspnea(NYHA class III or IV), exertional angina (CCS class II or III) or exertionalsyncopeforwhichanarrhythmiccausehasbeen excluded. There should be dynamic obstruction of ≥50 mmHgatrestand/or≥70mmHgwithprovocation,although thecurrenttrendistoconsiderpatientswithlowervalues ---≥30 mmHgatrest and/or ≥50mmHgwithprovocation. In our study population, which reflects our initial experi-ence and hence a learning curve, we opted for a more conservative selection process using the higher values. It shouldbestressedagainthatinvasivetreatmentisonly indi-cated when medical therapy is ineffective, not tolerated or contraindicated. In reference centers, optimization of medicaltherapyinpatientsreferredforinvasivetreatment canimproveclinicalstatusinaconsiderableproportionand removetheinitialindicationforASAormyectomy.11
Giventhe riskof causing an iatrogenicinterventricular communication, basalseptalthicknessshould be≥16mm for both ASA and myectomy. Mitral regurgitation,even if significant, is not a contraindicationfor ASA solong as it isfunctionalandduetoSAM,sincethelatterwillimprove withreductionoftheobstruction.However,primarymitral regurgitation, or another indication for cardiac surgery, is reason to perform myectomy. In patients with severe hypertrophy (>30mm) or inwhom thepapillarymuscle is implanted directly intotheanterior mitralleafletcausing LVOTobstruction,ASAislesslikelytosucceedandsurgery ispreferable.ForASAtobefeasibleitisalsoessentialthat theobstructionshouldbeintheregionofthebasalseptum andthatthereshouldbeoneor moreseptalarteriesthat canbeselectivelycatheterizedandthatirrigateonlythat partoftheseptum.ASAcanbeperformedafterunsuccessful myectomy.12
Althoughcases of ASA inchildren have been reported, manyoperators,includingtheauthors,considerthatthelow surgical risk at pediatric ages and the lack of knowledge ofthelong-termconsequencesofmyocardialnecrosisina young andstill developingheart mean thatsurgery is the preferredoption.
Procedure
Theprocedurebeginswithcoronaryangiographyinorderto identifythetargetvessel,usuallythefirstseptalbranchto thebasal septum,in which systolicmilking isvisible. The target septal branch may arise from a diagonal, the cir-cumflex, or even the right coronary artery, although the latterwasnotobservedinourpopulation.Following assess-mentofthecoronaryanatomy,includingeaseofaccessto and caliberof the target vessel, the material tobe used in the procedure can be selected. In our center we gen-erallyuse 6FJudkinsandEBUguiding catheters,BMW® or
Pilot50®guidewires(AbbottVascular,SantaClara,CA,USA)
and Apex Flex® over-the-wire balloon catheters (Boston
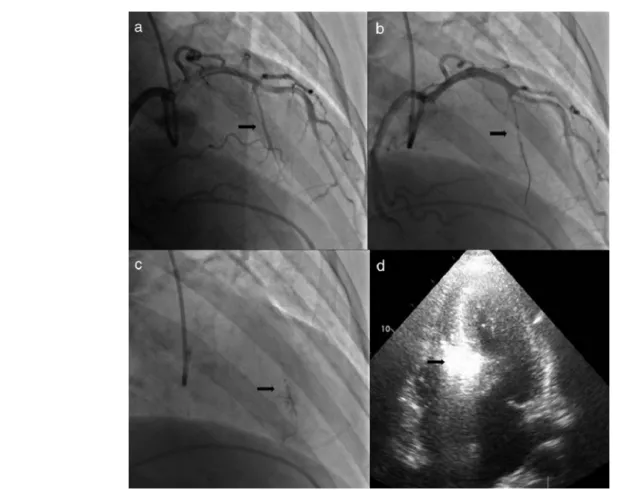
Scientific, Natick, MA, USA). A femoral approach is pre-ferredforgreaterstabilityduringcoronarycatheterization. When significant coronary lesionsare detected with indi-cation for revascularization, we consider that this should be performed first and ASA postponed pending reassess-mentofsymptoms.Inoneofourpatientstheoriginofthe target septalbranch wasclosetoa lesion inthe anterior descending artery and stenting would have compromised subsequentaccess,and soit wasdecidedtoperformASA first and then to treat the lesion in the same procedure (Figures1and2).
All patients shouldundergo priorDoppler echocardiog-raphytoconfirmthediagnosisandtoaccuratelylocateand quantifytheobstruction(Figure3).Whendoubtsremain con-cerningthelatter,hemodynamicassessmentisperformedto recordaorticandintraventricularpressuressimultaneously and to quantify the gradient at rest, with the Valsalva maneuver,andafteraventricularprematurebeat.
During the procedure, transthoracic echocardiographic studyisfirstperformedtoassesstheechogenicityofthe car-diacstructuresfor subsequent comparisonandtoexclude pericardialeffusion. Afterthetarget vesselis identifieda temporarypacingcatheteris placedin theright ventricle via a transvenous femoral or jugular approach. Follow-ingconfirmation that thisis stable andeffective, heparin 70---100U/kgisadministered,thenthetargetseptalartery is approached with a guidewire previously inserted into the balloon catheter. The latter is then introduced over theguidewireintothetargetvessel andpositionedat the desiredlocation,whichisselectedaccordingtothe diame-terofthevesselandtheexistenceofbifurcationsthatmay or maynot besubjectto alcohol injection,depending on theirsizeandcourse.Thediameteroftheballoonshouldbe 0.5mmgreaterthanthatofthetargetvesselatthepoint whereinflationwilltakeplace;asmallerdiametermaynot completelyoccludethevessel,allowingalcoholtoflowback totheanteriordescendingartery,whileanoversizedballoon maybedisplacedduringalcoholinjection.
Following balloon inflation at low pressure (4---6 atm), the guidewire is withdrawn and angiographic contrast is injectedinordertovisualizethedistalcirculationofthe tar-getvessel,excludetheexistenceofcollateralsandconfirm totalocclusionofthevesselwithnobackflowofcontrastto theanteriordescendingartery.Then1---2ccofmyocardial contrastisinjected;initiallyLevovist® (BayerAG,Schering
AG, Germany)wasused,and afterthis wasdiscontinued, SonoVue®(Bracco,Milan,Italy).Transthoracic
echocardiog-raphyisusedtoassessthehyperechogenicityofthetarget
region,thebasal septumwhereSAMoccurs, andflow tur-bulence,andtoexcludetheinvolvementofremoteregions suchastheLVfreewall,therightventricleandthepapillary muscles.
Once the decision is made to go ahead with alcohol ablation,analgesiais administeredwithmorphine (4---6cc intravenously, which is well tolerated in most patients) andthecorrectfunctioningofthetemporarypacemakeris checked.Thisstepisextremelyimportant,sincetransient AVBis common.Slowinjection(1 cc/min)of 1cc alcohol percm thicknessof thetarget septaltissue follows, con-stantlymonitoringthat theballoon iscorrectly positioned andwellinflated.Followingalcoholadministrationandafter a10-minwait,theguidewireisreinsertedintothelumenof theballoon catheter,which isdeflatedandthewhole sys-temisremoved.Afinalangiogramisperformedtoexclude coronarydissectionorimpairedcoronaryflow.
Patientsremain in the coronary care unit for the first 24---48hours,undercontinuousECGsurveillance.The creat-ininekinasecurveismonitoredatfour-hourintervalsuntil itspeak,thetimeofwhichisoneoftheparametersinthe AVBriskscoreusedinourpopulation.13Inlow-riskpatients
thepacingcatheterisremoved24---48hoursafterthe inter-ventionandthepatientreturnstothewardundertelemetric ECG monitoring and restarts his or her previous medica-tion(beta-blockersand/orcalciumchannelblockers),which areusually suspended beforethe procedure. If there are nocomplications,thepatientisdischargedonthesixthor seventhday.
The procedure described aboveundoubtedly differs in smalldetailsfromthatusedbyothercentersandoperators, butthebasicstepswillbecommontoallforwhomsafety isa priority.We highlight threechangesthathave helped improve safety and outcomes compared to the first pub-lishedseries.Firstly,weuseasmallerquantityofalcohol, reducingtheareaofnecrosisandhencetheriskofaffecting atrioventricularconductiontissue.Similarly,theimmediate objectiveofreducingthesubaorticgradient,withrepeated alcoholinjectionsifnecessary,hasbeenabandonedinfavor ofassessingtheresultafterseptalhealingandremodeling. Thesecondchange,introducedbyFaberetal.in1998,was theuseofintraproceduralmyocardialcontrastinjectionand transthoracicechocardiographytodeterminethetarget ves-selandpreventnecrosisinremotemyocardialregions.14This
isnowanimportantstepintheprocedure;inourseriesthe targetvessel waschangedin 10%of cases,and the inter-ventionwasabandoned in threepatients(not included in thestudy)becauseechocardiographicassessmentfailedto identifyasuitablevessel. Thirdly,the introductionof risk scoresfor high-degreeAVB hasmade itpossible to distin-guishpatientsinwhomitisbettertoawaitresolutionofthe acutephaseofseptaledema,afterwhichconduction distur-bancesresolveinthemajorityofcases,fromthoseinwhom apermanentpacemakershouldbeimplantedimmediately.13
Efficacy
Immediate gradient reduction is no longer considered essential for the efficacy of the procedure. Follow-ing ASA, the gradient goes through three stages: immediately after alcohol administration it falls due
Figure1 Procedure:(a)angiography,rightobliquecranialviewoftheleftcoronaryartery,showingthetargetvessel;(b)selective catheterizationofthetargetvessel andplacementofballooncatheter;(c)selectiveangiographyofthetargetvessel,showing injectionofcontrastthroughthelumen oftheballooncatheter; (d) transthoracicechocardiography, 4-chamberview,showing hyperechogenicbasalseptumafterinjectionofcontrast.
tomyocardial stunning; it then rebounds over 5---10 days due to edema in the necrosed area; and finally scarring andremodeling occur after aroundthree months,usually leadingtoimprovementinthegradient uptoayearafter theintervention.15
In 2006, Alam et al. published a meta-analysis of 42 studies on outcomes after ASA in 2959 patients.16 At 12
months,therewasasustaineddecreaseinrestingand pro-vokedLVOTgradient(65.3to15.8mmHgand125.4to31.5 mmHg,respectively)accompaniedbyreductioninbasal sep-talthickness(20.9to13.9mm),improvementinNYHAclass (2.9 to 1.2), and increase in exercise capacity (325.3 to 437.5seconds).ASA isassociated withsustained improve-mentsin symptoms and gradient in >85% of patients.17,18
RepeatASAduetopersistenceorrecurrenceofsymptoms is necessary in around 7% of cases, a similar figure to myectomy.16
ASA results in increased LVOT area and reduced gradient19,20;besidessymptomaticimprovement,its
bene-fitsincludeincreasedcoronaryflowreserve21andLVsizeand
reducedLVmass,22end-diastolicpressure,14leftatrialsize14
andmitralregurgitation.23Theclinicaleffectsobservedare
alsoduetoimprovedLVdiastolicfunction,whichis compa-rabletothatobtainedbymyectomy.24,25
Iftheprocedure isunsuccessful, myectomyremains an option,albeitwithagreaterriskofneedforpermanent pac-ing,duetothe combination ofthe completeright bundle
branchblockthat oftenresultsfromalcoholinjectionand theleftbundlebranchblockcausedbythesurgicalincision intheleftsideoftheseptum.
Safety
and
complications
The most common complication in ASA is irreversible high-degree AVB, but the improvements in the technique describedabovehavereducedthefrequencyofthis compli-cation to <10%, far lowerthan the initial results of some centers.17,18 In some casespersistence of AVB beyondthe
first 24 hoursis due tothe effect of perinecrotic inflam-mation on adjacent conduction tissue, rather than its permanent destruction; our experience confirms that in intermediate-risk patients with persistent AVB it is worth waiting a few days for the inflammation to subside and for intraventricular conduction to be re-established, in which case therewill be no need for a permanent pace-maker.
Other possible complications are related to vascular accessandintravascularcathetermanipulation,similarto percutaneous coronaryintervention, but they are uncom-monifcareistakenwithtechnicalaspectsoftheprocedure. Alametal.describeddissectionoftheanteriordescending arteryin1.8%ofpatients,16whilecardiactamponadecaused
byinsertionofthetemporarypacingcatheterhasareported incidenceof0.6%.16
Alcoholleakagetotheanteriordescendingarteryorvia collateralstoremotetissuesisaseriouscomplicationthat
canleadtoanunconfinedinfarctionoutsidethetargetarea. Leakagecan beavoided by takinggreat careto keepthe
Figure2 Changeinthe targetvessel aftercontrast injection:(a) selectivecatheterization ofthesecond septalbranch;(b) selectivecatheterizationofthefirstseptalbranch;(c)opacificationoftherightsideoftheseptumafterinjectionofcontrastin thesecondseptalbranch;(d)opacificationoftheappropriateregionoftheseptum(belowtheanteriorleafletofthemitralvalve), followingcontrastinjectioninthefirstseptalbranch.
Figure3 Echocardiographicimages:(a)transthoracicechocardiography,4-chamberview,beforetheintervention;(b)continuous Dopplerstudyshowingsubaorticgradientbeforetheintervention;(c)transthoracicechocardiography,4-chamberview,threemonths afterthe intervention,showing decreasedthickness ofthe basalseptum; (d)continuous Doppler studythreemonths afterthe intervention,showingreductioninthesubaorticgradient.
balloon fullyinflated andto maintain thestability of the entiresystemtopreventrefluxofalcohol.Therecruitment ofcollateralsisanunpredictablecomplication,sinceasin ourexperience,they maynot be visualized at the begin-ning of the intervention, but this is rare. In one of the fewpublishedcases,Chowdharyetal.suggestthat recruit-mentofcollaterals maybefacilitatedbylonger occlusion ofthetargetvesselbeforealcoholadministration,26 which
was in fact the case in our patient due to the need to replacetheechocardiographic probe.Sincethen,wehave paidparticularattentiontotheneedtominimizeocclusion time.
Another possible cause for concern is the creation of an intramyocardial septalscar, due toits arrhythmogenic potentialinadiseaseinwhichthereisalreadyasubstrate for arrhythmias. However, after nearly 20 years of expe-rienceand thousands of procedures, this fearhas proved groundless(seefollowingsection).Carefulstratificationof arrhythmicriskis essential,asalways inthetreatment of HCM.
In-hospital mortality associated with ASA is 0---4%,27
lower in centers with greater experience with ASA and percutaneous interventions generally, reflecting the need for a learning period. Kwon et al. reported no intrapro-cedural mortality in patients at high surgical risk.28 In
the review by Alam et al., early (30-day) mortality was 1.5% (0.0---5.0%) and late mortality (>30 days) was 0.5% (0.0---9.3%).16
Comparison
with
myectomy
Aswithotherconditionsforwhichthereareboth percuta-neousandsurgicaltreatmentoptions,eitherasalternatives orcomplementary,therehasbeenconsiderabledebate con-cerningthebestapproach.Itisgenerallyagreedthatthere isunlikelytobealargerandomizedmulticentertrial com-paringthetwostrategies that couldhelpclarify which of thetwoshouldbepreferred.29ThelowprevalenceofOHCM
andthelackoffinancialincentive(nospecialized technol-ogyor intellectual propertyis involved) would makesuch atrial difficult toimplement.We arethus leftwith com-paringthelimitationsofeachtechniqueandtheresultsof observationalstudiesinmeta-analyses.
Proponents of surgery frequently point to the greater long-term experiencewith myectomy, although this argu-ment is becomingweaker asthe years pass; there arein factnowmorepatientstreatedpercutaneouslythan surgi-cally.Surgical treatmentcandealwithcertainanatomical featuresthat ASA cannot,suchasmitral valverepairand casesrequiringalargerquantityofhypertrophiedmuscleto beresected,thusachievingagreaterandmorerapid reduc-tioninintraventriculargradient, butthis doesnot appear toaffectclinicaloutcomes.CompletesustainedAVBisless frequentwithmyectomy(5%asopposedto10%withASA); thisisprobablythemaindifferenceintheresultsofthetwo techniques.16
ASA has the advantages of other percutaneous treat-ments:it is less invasive,does notrequire sternotomy,is associatedwithshorterrecoverytime,andcanbeusedto treatpatientswithrelativeorabsolutecontraindicationsfor surgery,suchaselderlyorobeseindividualsandthosewith
significant comorbidities. Clinical outcomesare similarto thoseofmyectomy,asshownintworecentmeta-analyses, in which theonly differencewastheneed for permanent pacing.30,31Theseresultsreflectthelearningcurverequired
forASA,aswasinitiallyseenformyectomy,althoughnotin recentpublications.
Two of the main limitations of ASA are the need for favorable anatomical conditions and more unpredictable outcomes,althoughthesecanbereducedbycarefulpatient selection.
Thegreatestcontroversyconcernstheriskofventricular arrhythmiaswithASA.Suchfearswereheightenedbysome smallobservationalstudies,32,33butthesewerecontradicted
by other similarstudies that indicated the techniquewas safe.34,35Theseconflictingresults,andthelackofsufficient
evidence,havecreatedconfusionthatcanonlyberesolved bylargestudiesofpatientstreatedbyASAwithlong-term outcomesandbymeta-analysescomparingtheresultsofthe twotechniques. In 2008 Kuhn etal. publishedthe results of644consecutive patientstreatedbyASAovera 10-year period.36Annualcardiacmortalityafterdischargewas0.7%,
a similar percentage to the untreated population, which doesnotsupporttheideathatthesepatientsareatgreater riskofsuddendeath.37Thelatestandlargestmeta-analysis
ofthetwotechniquesanalyzed2207patientstreatedbyASA and1887patients treatedbymyectomyandfound no dif-ferencesinoverallmortalityorsuddendeath,eventhough thepopulationtreatedsurgicallywereyounger.38
Conclusion
Theresultsfromtheinitialexperienceofourcenterconfirm the efficacy andsafety of ASA for the invasivetreatment ofpatients withOHCM refractorytomedicaltherapy.This percutaneous approach is a valid alternative for invasive treatmenttoreducesubaorticobstructioninthesepatients.
Ethical
disclosures
Protection of human and animal subjects.The authors declare that theprocedures followed werein accordance withtheregulationsoftherelevantclinicalresearchethics committeeandwiththoseoftheCodeofEthicsoftheWorld MedicalAssociation(DeclarationofHelsinki).
Confidentialityofdata.Theauthorsdeclarethattheyhave followedtheprotocolsoftheirworkcenteronthe publica-tionofpatientdataandthatallthepatientsincludedinthe studyreceivedsufficientinformationandgavetheirwritten informedconsenttoparticipateinthestudy.
Righttoprivacyandinformedconsent.Theauthorshave obtained the written informedconsent of thepatients or subjectsmentionedinthearticle.Thecorrespondingauthor isinpossessionofthisdocument.
Conflicts
of
interest
References
1.TeareD.Asymmetricalhypertrophyoftheheartinyoungadults. BrHeartJ.1958;20:1---8.
2.BraunwaldE,LambrewCT,MorrowAG,etal.Idiopathic hyper-trophicsubaorticstenosis.Adescriptionofthediseasebased uponan analysis of64 patients. Circulation.1964;29 Suppl. 4:3---119.
3.FiferMA,SigwartU.Controversiesincardiovascularmedicine. Hypertrophicobstructivecardiomyopathy:alcoholseptal abla-tion.EurHeartJ.2011;32:1059---64.
4.Maron MS,Olivotto I,Zenovich AG,et al. Hypertrophic car-diomyopathy is predominantly a disease of left ventricular outflowtractobstruction.Circulation.2006;114:2232---9.
5.OmmenSR,NishimuraRA.Whatcausesoutflowtract obstruc-tioninhypertrophiccardiomyopathy?Heart.2009;95:1725---6.
6.MaronMS,OlivottoI,BetocchiS,etal.Effectofleftventricular outflowtract obstructiononclinicaloutcomeinhypertrophic cardiomyopathy.NEnglJMed.2003;348:295---303.
7.GershBJ, MaronBJ, BonowRO, etal.,Developed in collab-oration with the American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society ofAmerica, Heart RhythmSociety, Society for Cardiovascular Angiography and Interventions,andSocietyofThoracicSurgeons.Collegeof Car-diologyFoundation/AmericanHeartAssociationTaskForceon PracticeGuidelines2011ACCF/AHAGuidelineforthe Diagno-sisandTreatmentofHypertrophicCardiomyopathy:areportof theAmericanCollegeofCardiologyFoundation/AmericanHeart AssociationTaskForceonPracticeGuidelines.JAmCollCardiol. 2011;58:e212---60.
8.FiferMA.Controversiesincardiovascularmedicine.Mostfully informedpatientschooseseptalablationoverseptalmyectomy. Circulation.2007;116:207---16.
9.SigwartU.Nonsurgicalmyocardialreduction forhypertrophic obstructivecardiomyopathy.Lancet.1995;346:211---4.
10.SigwartU.Cathetertreatmentforhypertrophicobstructive car-diomyopathy:forseniorsonly?Circulation.2008;118:107---8.
11.RothmanRD,Baggish AL, O’CallaghanC,et al. Management strategyin249 consecutive patientswithobstructive hyper-trophiccardiomyopathyreferredtoadedicatedprogram.AmJ Cardiol.2012;110:1169---74.
12.Chang SM, Lakkis NM, Franklin J, et al. Predictors of outcome after alcohol septal ablation therapy in patients with hypertrophic obstructive cardiomyopathy. Circulation. 2004;109:824---7.
13.FaberL, Seggewiss H,Welge D,et al. Predictingtherisk of atrioventricularconductionlesions afterpercutaneousseptal ablationforobstructive hypertrophiccardiomyopathy.Z Kar-diol.2003;92:39---47.
14.Faber L, SeggewissH, Gleichmann U. Percutaneous translu-minalseptalmyocardialablation inhypertrophicobstructive cardiomyopathy: results with respect to intraprocedural myocardial contrast echocardiography. Circulation. 1998;98: 2415---21.
15.CarassoS,WooA,YangH,etal.Myocardialmechanicsexplains the time course of benefit for septal ethanol ablation for hypertrophiccardiomyopathy.JAmSocEchocardiogr.2008;21: 493---9.
16.AlamM,DokainishH,LakkisN.Alcoholseptalablationfor hyper-trophic obstructive cardiomyopathy: a systematic review of publishedstudies.JIntervCardiol.2006;19:319---27.
17.Gietzen FH, Leuner CJ, Obergassel L, et al. Transcoronary ablationofseptalhypertrophyforhypertrophicobstructive car-diomyopathy:feasibility,clinicalbenefit,andshorttermresults inelderlypatients.Heart.2004;90:638---44.
18.Faber L, Seggewiss H, Gietzen FH, et al. Catheter-based septal ablation for symptomatic hypertrophic obstructive
cardiomyopathy:follow-upresultsoftheTASH-registryofthe GermanCardiacSociety.ZKardiol.2005;94:516---23.
19.vanDockumWG,BeekAM,tenCateFJ,etal.Earlyonsetand progressionofleftventricularremodelingafteralcoholseptal ablationinhypertrophicobstructivecardiomyopathy. Circula-tion.2005;111:2503---8.
20.Sitges M,Qin JX,LeverHM,et al. Evaluationofleft ventri-cularoutflowtractareaafterseptalreductioninobstructive hypertrophiccardiomyopathy:areal-time3-dimensional echo-cardiographicstudy.AmHeartJ.2005;150:852---8.
21.JaberWA,YangEH,NishimuraRA,etal.Immediate improve-mentincoronaryflowreserveafteralcoholseptalablationin patientswithhypertrophicobstructivecardiomyopathy.Heart. 2009;95:564---9.
22.Mazur W, Nagueh SF, Lakkis NM, et al. Regression of left ventricularhypertrophyafternonsurgicalseptalreduction ther-apyforhypertrophicobstructivecardiomyopathy.Circulation. 2001;103:1492---6.
23.NaguehSF,LakkisNM,MiddletonKJ,etal.Changesinleft ventri-cularfillingandleftatrialfunctionsixmonthsafternonsurgical septalreductiontherapyforhypertrophicobstructive cardiomy-opathy.JAmCollCardiol.1999;34:1123---8.
24.NaguehSF,LakkisNM,MiddletonKJ,etal.Changesinleft ven-tricular diastolic function 6 months after nonsurgical septal reductiontherapyforhypertrophicobstructivecardiomyopathy. Circulation.1999;99:344---7.
25.Sitges M, Shiota T, Lever HM, et al. Comparison of left ventricular diastolic function in obstructive hypertrophic cardiomyopathy in patients undergoing percutaneous septal alcoholablationversussurgicalmyotomy/myectomy.AmJ Car-diol.2003;91:817---21.
26.ChowdharyS,GaliwangoP,WooA,etal.Inferiorinfarction fol-lowingseptalablation:aconsequenceof‘‘collateraldamage’’? CathetCardiovascInterv.2007;69:236---42.
27.ParakhN,BhargavaB.Goldenjubileeofhypertrophic cardiomy-opathy:isalcoholseptalablationthegoldstandard?Cardiovasc RevascMed:IncludingMolInterv.2009;10:172---8.
28.KwonDH,KapadiaSR,TuzcuEM,etal.Long-termoutcomesin high-risksymptomaticpatientswithhypertrophic cardiomyopa-thyundergoingalcoholseptalablation.JAmCollCardiolInterv. 2008;1:432---8.
29.Olivotto I, Ommen SR, Maron MS,et al. Surgical myectomy versusalcoholseptalablationforobstructivehypertrophic car-diomyopathy.Willthereeverbearandomizedtrial?JAmColl Cardiol.2007;50:831---4.
30.Alam M, Dokainish H, Lakkis N. Hypertrophic obstructive cardiomyopathy --- alcohol septal ablation vs. myectomy: a meta-analysis.EurHeartJ.2009;30:1080---7.
31.Agarwal S, Tuzcu EM, Desai M, et al. Updated meta-analysis of septal alcohol ablation versus myectomy for hypertrophic cardiomyopathy. J Am Coll Cardiol. 2010;55: 823---34.
32.MaronBJ,SpiritoP,ShenWK,etal.Implantable cardioverter-defibrillators and prevention of sudden cardiac death in hypertrophiccardiomyopathy.JAMA.2007;298:405---12.
33.tenCateFJ,SolimanOI,MichelsM,etal.Long-termoutcome ofalcoholseptalablationinpatientswithobstructive hyper-trophic cardiomyopathy: a wordof caution. Circ HeartFail. 2010;3:362---9.
34.CuocoFA, Spencer3rdWH,FernandesVL,etal.Implantable cardioverter-defibrillator therapy for primary prevention of suddendeathafteralcoholseptalablationofhypertrophic car-diomyopathy.JAmCollCardiol.2008;52:1718---23.
35.SorajjaP,OmmenSR,HolmesJrDR,etal.Survivalafteralcohol septalablation for obstructivehypertrophic cardiomyopathy. Circulation.2012;126:2374---80.
36.Kuhn H,LawrenzT, LiederF,et al.Survivalafter transcoro-naryablationofseptalhypertrophyinhypertrophicobstructive
cardiomyopathy(TASH):a10yearexperience.ClinResCardiol. 2008;97:234---43.
37.Spirito P,BelloneP,HarrisKM,et al. Magnitudeofleft ven-tricularhypertrophyandriskofsuddendeathinhypertrophic cardiomyopathy.NEnglJMed.2000;342:1778---85.
38.Leonardi RA, Kransdorf EP, Simel DL, et al. Meta-analyses of septal reduction therapies for obstructive hypertrophic cardiomyopathy: comparative rates of overall mortalityand suddencardiacdeathaftertreatment.CircCardiovascInterv. 2010;3:97---104.